
Abstract
Membranes or skin dressing are common treatments for skin wound injuries, collagen being one the most effective materials for their manufacturing. Many different sources of collagen with diverse methods of extraction and processing have been used, with evidence of positive effects on the stimulation of skin wound healing. In spite of these factors, there is still limited understanding of the interaction between collagen membranes and biological tissues, especially due to the series of different types of collagen origin. In this context, this study aimed to conduct a systematic review of the available literature examining the effect of various collagen membranes for accelerating skin wound healing in experimental animal models and clinical trials. The present review was performed from March to May of 2020 searching in two databases (PubMed and Scopus). The following Medical Subject Headings (MeSH) descriptors were used: “collagen”, “dressing”, “membranes”, “skin” and “wound”. After the eligibility assessment, 16 studies were included and analyzed. The studies demonstrated that collagen was obtained predominantly from bovine and porcine sources, by acetic acid and/or enzyme dissolution. Additionally, most of the studies demonstrated that the membranes were processed mainly by freeze-drying or lyophilization methods. All the in vivo and clinical trial studies evidenced positive outcomes in the wound healing process, thus confirming that collagen membranes are one of the most efficient treatment for skin wounds, highlighting the enormous potential of this biomaterial to be used for skin tissue engineering purposes.
Introduction
Skin wounds are very common injuries, caused by many different reasons, including physicochemical or thermal damage and metabolic diseases such as diabetes. They result in functional imbalance, increased level of pain, disability or even death. 1 , 2 It is estimated that approximately 5.7 million people in US are affected by wound lesions, with the treatment cost exceeding USD 50 billion dollars annually. 3
Skin wounds can be divided into acute and chronic wounds. Acute wounds, in general, heal by themselves in a smooth and efficient way. 4 Conversely, in the presence of some specific situations such as bad nutrition, associated diseases, age or extensive wound extension, the process of skin regeneration may be impaired, resulting in chronic or non-healed wounds. 5 , 6
Many treatments for chronic skin injuries have been proposed such as surgery, pharmacological interventions, use of growth factors and stem cells, and wound dressing with or without membranes.
6
,
7
Acute wounds normally heal in an orderly and effi- cient manner. They progress smoothly through the four distinct, but overlapping phases of wound healing: hemostasis, inflammation, proliferation and remod- elling Acute wounds normally heal in an orderly and effi- cient manner. They progress smoothly through the four distinct, but overlapping phases of wound healing: hemostasis, inflammation, proliferation and remod- elliAcute wounds normally heal in an orderly and effi- cient manner. They progress smoothly through the four distinct, but overlapping phases of wound healing: hemostasis, inflammation, proliferation and remod- elling
Membranes are one of the most efficient treatments for skin injuries, serving as protection from infection, reducing the level of pain, and stimulating and supporting cell migration and proliferation. 8 , 9 It is important to emphasize that many different biomaterials serve as raw material to be used for membrane manufacturing such as auto-grafts, 10 synthetic materials (artificial polymers), and natural materials like chitosan and collagen. 8 , 11
Collagen (formed by a triple-stranded helix of proline and glycine polypeptide chains) is the most abundant protein in vertebrates and is involved in the structural integrity of many tissues such as ligaments, tendons and bones.12–15 As a biomaterial, collagen is biocompatible, bioactive and has low immunogenicity, making it extremely suitable for tissue engineering and regenerative medicine, or TERM, strategies for human health issues, including membranes for skin wounds.16–19
In this context, it has been demonstrated that collagen membranes are resorbable (with an absorption rate matching tissue ingrowth), bioactive, have porosity and are able to support cell growth. 17 , 20 For this reason, they have been frequently used for treating skin wounds.18–20 Many different sources of collagen for membrane manufacturing have been explored, including bovine and porcine bone and skin, marine species such as fish skin, marine sponges and jellyfishes. 21 Collagen membranes, manufactured based on different methods, have demonstrated positive outcomes for stimulating tissue healing.16–18, 22 Table 1 shows some examples of collagen membranes commercially available used for skin wound healing.
Collagen membranes/wound dressing commercially available.
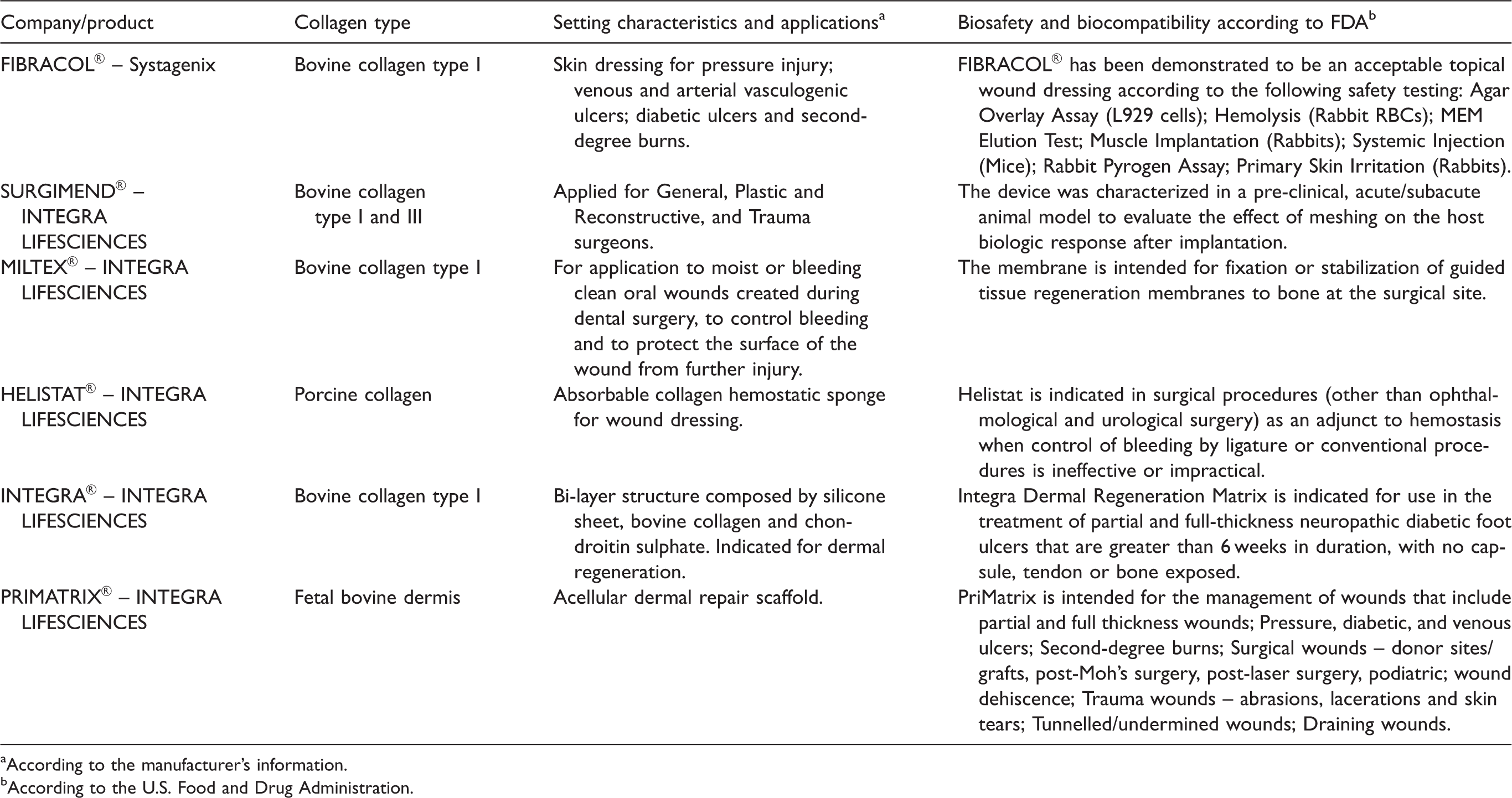
aAccording to the manufacturer's information.
bAccording to the U.S. Food and Drug Administration.
Although the evidence points towards positive effects of collagen membranes on skin wound healing, the wide range of collagen sources and the lack of standard protocols for membrane manufacturing (with many different extraction methods, chemical fixation agents, etc.) make it difficult to directly compare the published results. Also, the mechanisms by which collagen membranes interact with skin wounds are still controversial, and for many, their use as a treatment modality remains highly-debated. 12 Therefore, it is important to closely analyze the available data from the literature in order to improve the understanding of the effects of this therapeutic intervention on skin healing under different experimental conditions, to determine its safety and efficacy.
In this context, the purpose of this study was to perform a systematic review of the literature of studies investigating the effects of collagen membranes (from different origins) on improving skin wound healing in in vivo experimental models and clinical trials.
Methodology
Review protocol
This systematic review was performed according to the Systematic Review Center for Laboratory Animal Experimentation (SYRCLE) guidelines. 23 The search was conducted from March to May 2020 using the PubMed and Scopus databases. The search was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. The following descriptors of the Medical Subject Headings (MeSH) were used: “collagen”, “dressing”, “membranes”, “skin” and “wound”. In addition, several synonyms in the titles and abstracts were searched for each component.
Study selection
Two reviewers (ACMR and TAA) analyzed independently the title and the abstract of the selected works and identified the potential studies using the inclusion and exclusion criteria. The two reviewers had access to the selected studies to verify eligibility. Disaccords were solved by discussion. The selected studies were further reviewed during the full-text screening. Those that did not follow the eligibility criteria were excluded.
Inclusion criteria
In vivo experiments with animal models and clinical trials with patients with skin injuries or burns treated with collagen membranes. Type of intervention: use of collagen membrane as treatment for skin wound healing. In addition, articles were included by active search in bibliographic reference list of the selected articles and search in personal archives. Articles must be written in the English language and published in the last 30 years.
Exclusion criteria
Studies of characterization of the membrane, in vitro studies, in situ studies, reviews, and case reports. Studies without skin wounds, burns or injuries. Lack of description of the skin wounds, burns or injuries, methodology or outcomes. Animal models or clinical trials with systemic diseases (such as diabetic rats).
Data extraction
The variable analyzed to determine the quality of evidence was based on the histological analysis of the in vivo studies. In addition, the species/strain, animal sex, age, weight, origin of membrane, skin wound type, wound size, implantation period, ways of treatment, collagen extraction protocol, membrane manufacturing technique/crosslinking method, physical and morphological characteristics, collagen origin, analysis performed in the in vivo studies, outcome measures, analysis performed in the clinical trials, results and histological outcomes were also included in our analysis.
Types of reported results
Due to the heterogeneity of the primary studies, it was not possible to perform a meta-analysis. In order to compare the effect size (ES) of both techniques, we calculated the normalized average difference considering the values before and after the intervention. They were further classified as small (<0.20), moderate (about 0.50), or large (>0.80), according to Cohen criteria.
Quality of the evidence was determined using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach, which analyzes the following domains: trial design limitations due to risk of bias, inconsistency of results, indirectness, imprecision of results, and publication bias.
Results
The flow diagram demonstrates the search strategy used in the present study (Figure 1). A total of 49 articles was retrieved from the databases (31 from PubMed and 18 from Scopus). Duplicated records were excluded (n = 21). The remaining 28 full-text articles were assessed for eligibility and from those eight were excluded. Additionally, four studies were excluded for other reasons. There were 16 studies finally included and analyzed in this systematic review.
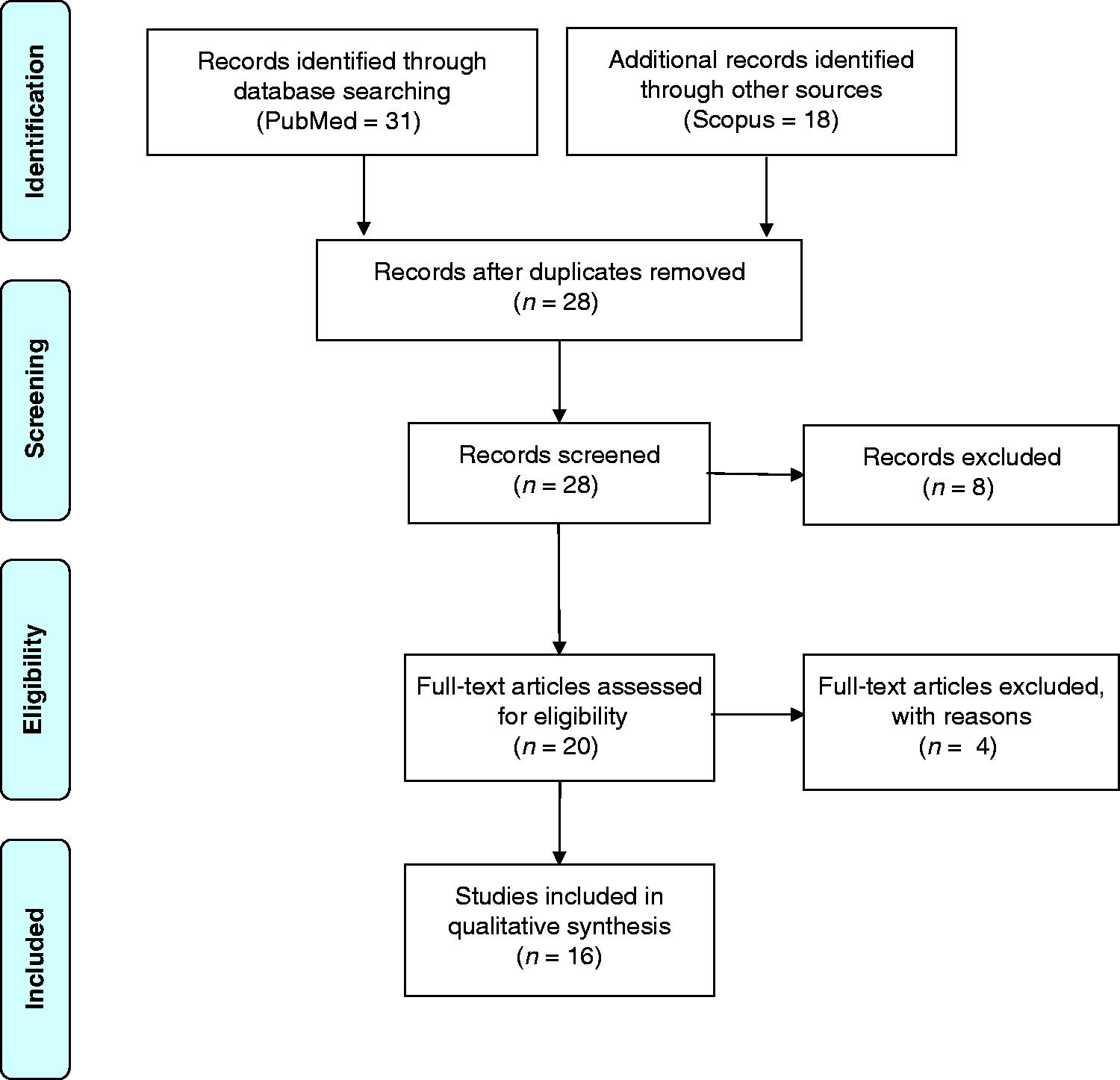
PRISMA flow diagram of search strategy.
Table 2 shows the characteristics of all included studies, such as author, species/strain, animal sex, age, weight, origin of membrane, skin wound size, implantation period (days) and way of treatment. Among the articles analyzed, seven studies used rats as the experimental model, such as Wistar rats24–27 and Sprague-Drawley rats.28–30 Two studies used rabbits, 31 , 32 one study used dogs and cats, 22 one used guinea pigs, 33 one used mices 20 and one minipigs. 34 The clinical trials included evaluated the effects of the membrane on the process of skin wound healing. 29 ,35–37
Characteristics of the studies.
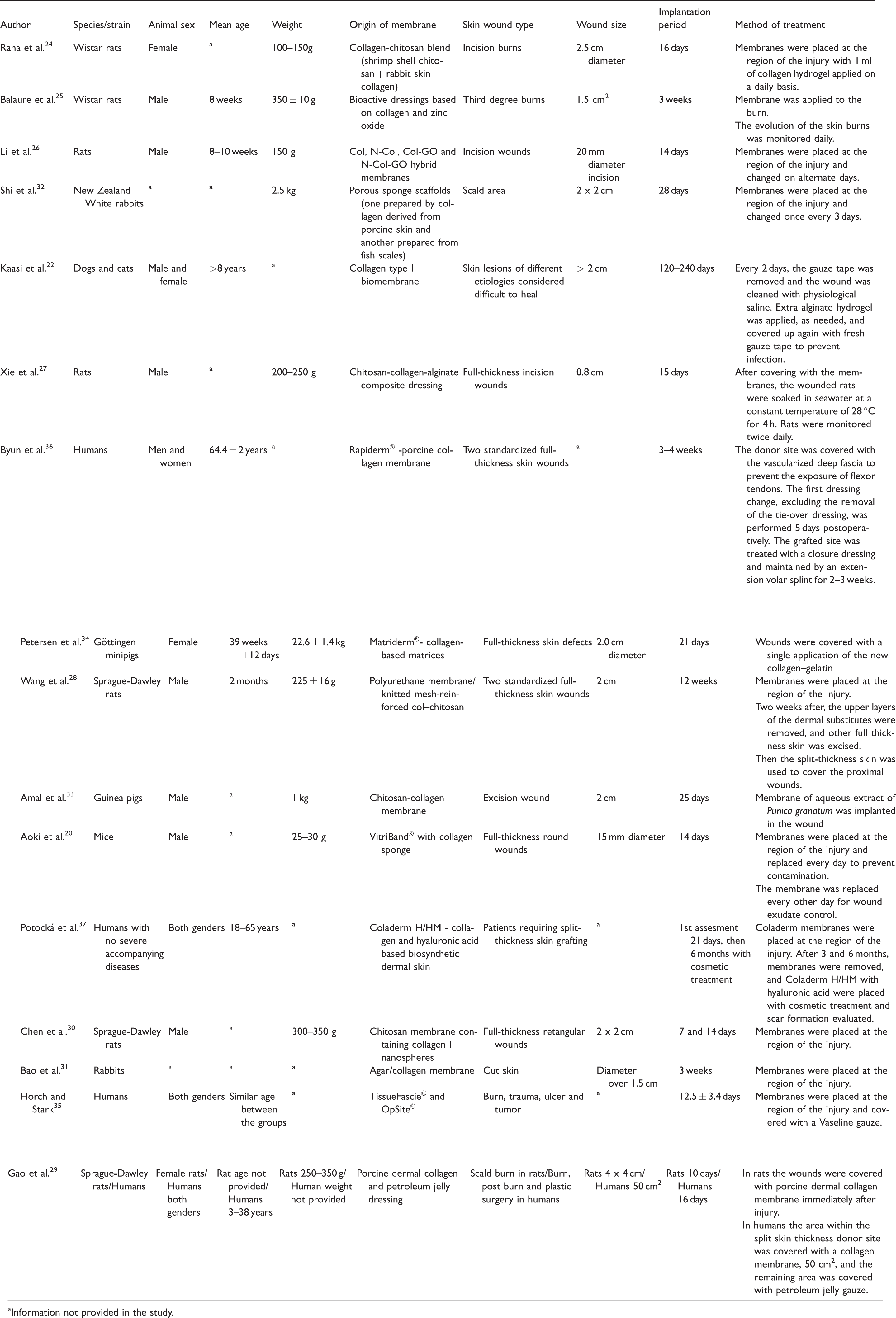
aInformation not provided in the study.
Table 2 also shows that half of the studies analyzed in this review applied the membrane directly to the wound, without dressing changes. 27 ,29–31,33–35 Seven studies performed more than two changes of membranes during experimental period 20 , 22 , 24 , 26 , 28 , 32 , 36 , 37 and one also included the use of cosmetics in association with the membrane. 37 Different wound sizes were used ranging from 15 mm2 to 50 cm2. 29 In addition, different timepoints were analyzed with a minimum experimental period of 7 days 30 and a maximum experimental period of 240 days. 22
A summary of collagen extraction protocols, membrane manufacturing processes as well as some of the physical and morphological properties of collagen membranes are listed in Table 3. We found that in nine studies, commercially available collagen was used (one from tendons of rats, four from bovine tissues, one from porcine tissue and for the others, the origin was not provided), 22 ,25–27, 31 ,34–37 while five studies extracted collagen from bovine bone, 26 , 28 , 34 , 35 , 37 four studies used porcine-collagen, 20 , 29 , 32 , 36 and two studies used collagen from marine fish. 32 , 33 Interestingly, Kaasi et al. used collagen from rat tail tendon 22 and Rana et al. used collagen extracted from rabbit skin. 24 Four studies did not provide data on the origin of the collagen. 25 , 27 , 30 , 31 The protocols for collagen extraction varied; three studies used an acetic acid and pepsin enzymatic method, 24 , 28 , 32 two studies employed an acetic acid method, 20 , 33 one used a tris-HCl buffer with acetic acid-pepsin extraction methodology, 29 and one utilized collagen produced from a high voltage electrostatic field system. 30
Collagen extraction and membrane protocols.
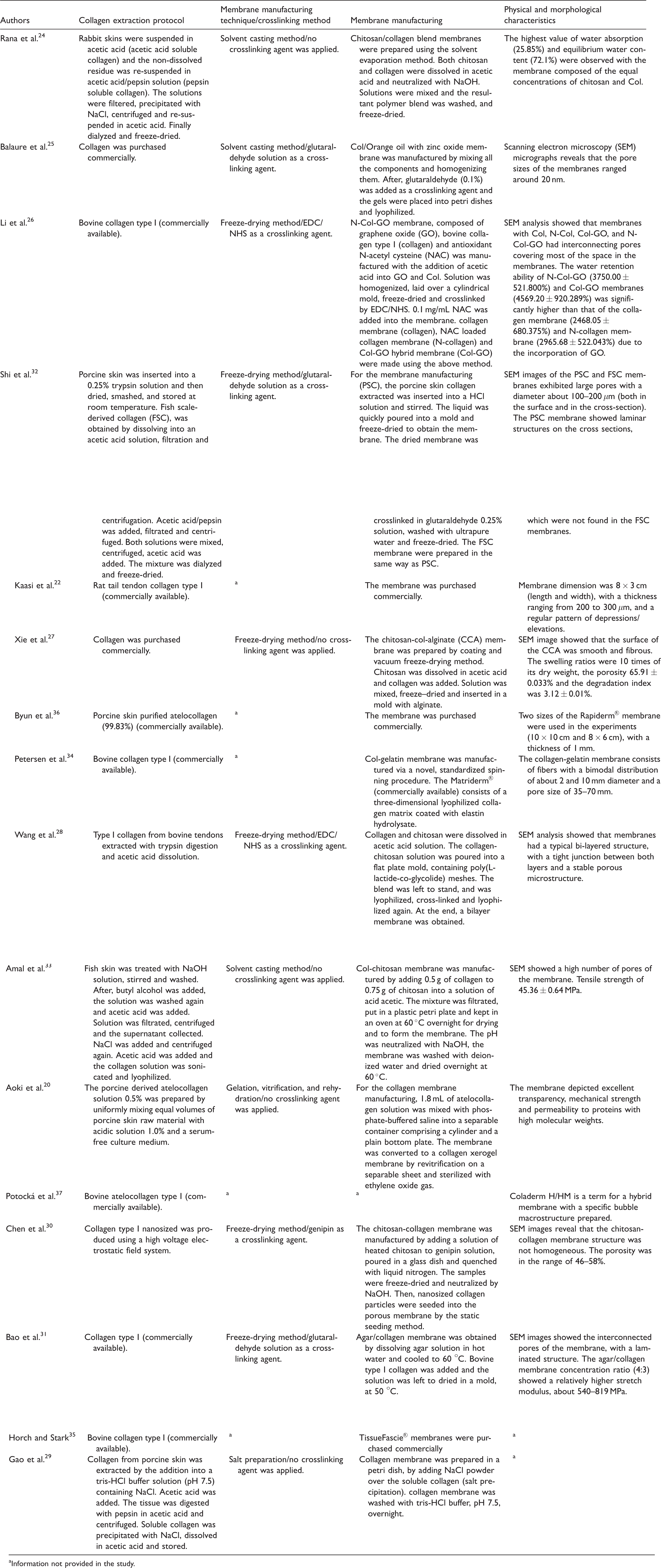
aInformation not provided in the study.
Three studies used commercially available collagen membrane in their experiments, 22 , 35 , 36 another three used chitosan/collagen blends, 24 , 28 , 33 one a chitosan/collagen/starch blend, 27 one a chitosan-collagen-alginate blend and one chitosan-genipin enriched with collagen nanoparticles. 30
For manufacturing of the membranes, most of the authors dissolved the raw materials in acid acetic, followed by freeze-drying or lyophilization.24–28, 32 , 33 Three studies used glutaraldehyde solution as a crosslinking agent in the manufacturing process. 25 , 31 , 32 Some authors used some specific protocols such as described: Aoki et al. employed a gelation, vitrification and rehydration methodology, 20 Gao et al. used a salt precipitation method, 29 and Petersen et al. developed a novel spinning procedure. 34 Five studies that used commercially available membranes did not present information about the manufacturing process. 22 ,34–37
A wide range of physical and morphological membrane characteristics can be observed. Scanning electron microscopy was used in seven studies to show the porosity and surface structure of the membranes. 25 , 27 , 28 ,30–33 One evaluated the water absorption and equilibrium water content of the membranes, 24 one analyzed membrane thickness (ranging from 200 to 300 μm), 22 one evaluated water retention ability, 26 and one swelling ratios (10 times of its dry weight). 27 Six studies did not show detailed information about the membranes (commercially available products). 22 , 29 ,34–37
Table 4 demonstrates the results and outcomes of the in vivo experiments. All 13 studies performed a macroscopic evaluation through images from the area of the wound after treatment with collagen membranes. 20 , 22 ,24–28, 30 ,32–34 For all studies, treated animals had a decreased wound area after the experiment and one reported subsequent reduced scarring. 33 Histological analysis demonstrated a faster reepithelization process, 20 , 22 , 25 , 27 , 29 , 32 , 34 reduced inflammatory reaction, 30 reduced scar formation20,25,30 and a faster rate of tissue healing.26,28,30–32 Four studies performed immunohistochemistry analysis and results are as described: Li et al. 26 and Wang et al. 28 observed an increase of cluster of differentiation 31 (CD31) immunostaining. Xie et al. 27 observed enhanced immunostaining of epidermal growth factor (EGF), CD 31, and transformation and growth factor (TGF) while Aoki et al. 20 observed a decrease of connective tissue growth factor (CTGF) and anti-a-smooth muscle actin (α-SMA) immunostaining after 7 days, and a decrease of cluster of differentiation 45 (CD45), macrophage F4/80 receptor (F4/80) and proliferating cell nuclear antigen (PCNA) immunostaining after 14 days. Wang et al. 28 also performed the immunofluorescence analysis and observed an increase of CD31 expression. Additionally, they performed a mechanical test and observed a gradual increase of tensile strength after 12 days.
Results and outcomes of the in vivo experiments.
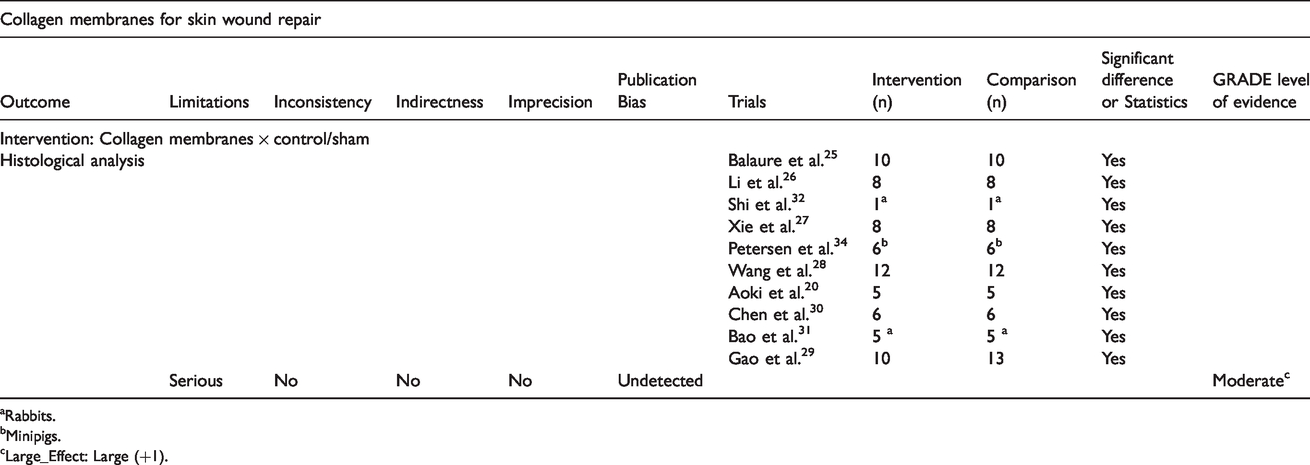
Table 5 shows the results and outcomes of the clinical trials included in the present study. The type of wound most reported were burn wounds 29 , 36 , 37 and only one study included ulcers, tumors and traumas. 35 The methodology applied in those studies included a split thickness skin from a donor site to use with the membrane to heal the wounds. 29 ,35–37
Results and outcomes of the clinical trials.
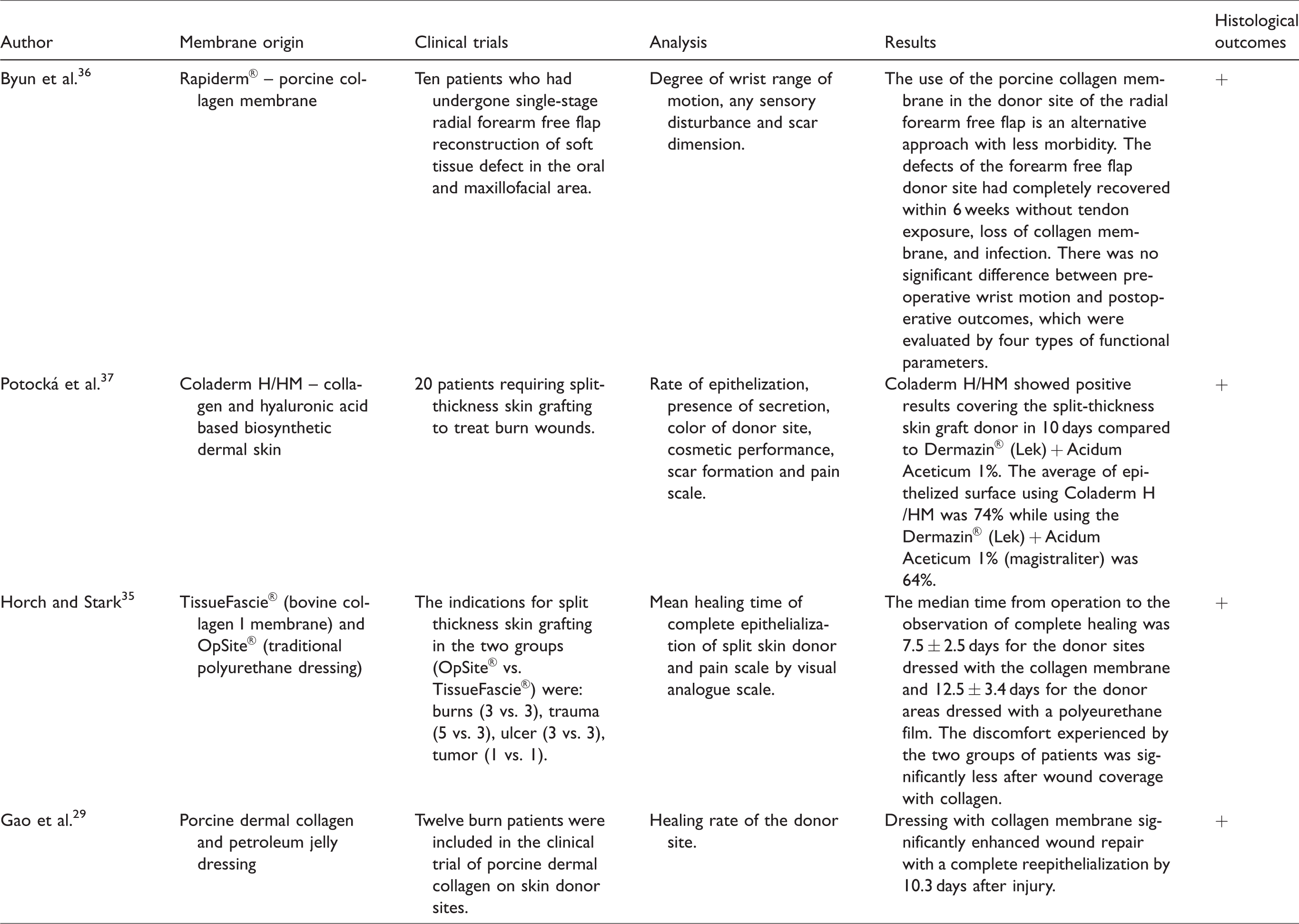
Three of the studies used commercially available membranes.35–37 Rapiderm® is a collagen membrane from porcine source, 36 Coladerm® is a membrane fabricated with collagen and hyaluronic acid, 37 and TissueFascie® is a bovine collagen I membrane. 35 Only one study fabricated a novel biomembrane manufactured from porcine dermal collagen and petroleum jelly dressing. 29
It is important to emphasize that all clinical trials showed positive results in the process of skin wound healing after covering the injury with collagen membranes, with a reduction in the time of healing in all studies compared to when a traditional membrane was used in the control group. Moreover, all the authors observed a complete healing process with the membrane treatment. 29 ,35–37
Table 6 shows the quality of evidence for the use of collagen membranes for skin wound repair according to the GRADE approach. The table shows the degree of evidence of the studies evaluating the effects of the collagen membranes on skin wounds in the animal studies. After the analysis, it was observed that there is moderate evidence (considering the variable “histological analysis”) showing the efficiency of collagen membranes on skin wound healing.
Summary of findings: Collagen membranes sources versus control/sham.
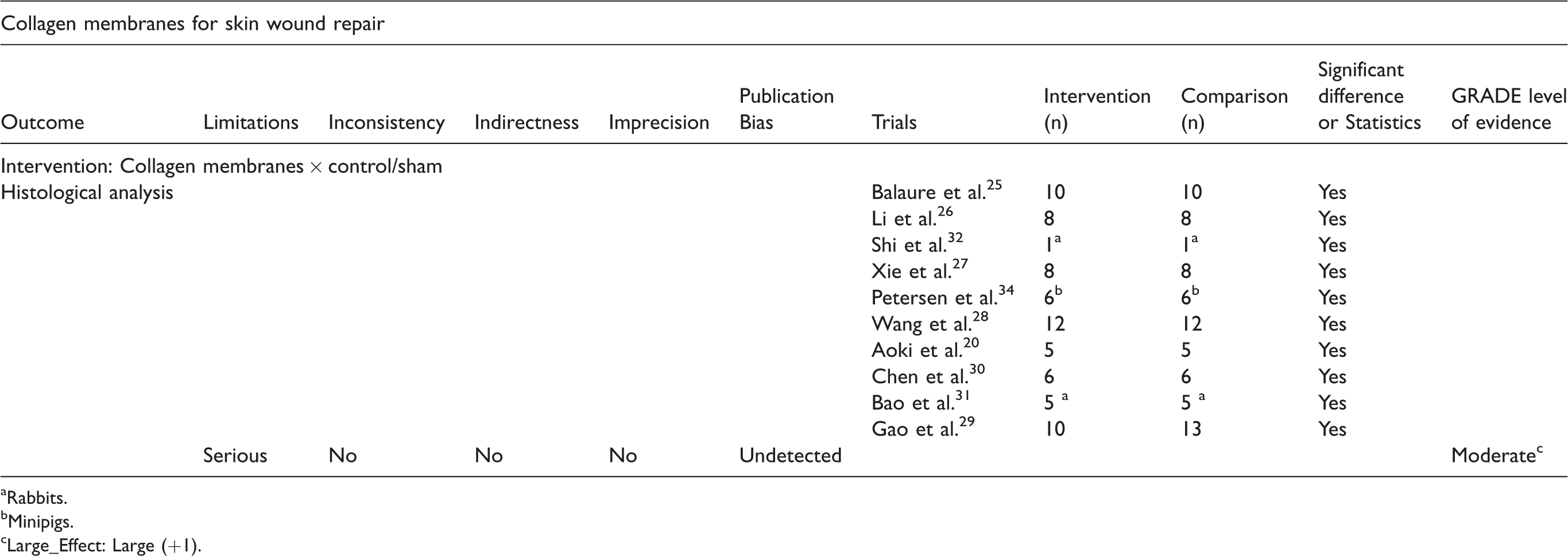
aRabbits.
bMinipigs.
cLarge_Effect: Large (+1).
Discussion
The present study evaluated the effects of different kinds of collagen membranes (used alone or in combination with other materials) on the process of healing in skin wounds in animal models and clinical trials. The results related to the biological data demonstrated that collagen membranes were able to accelerate skin wound healing, decreasing the time of wound resolution in both in vivo studies and clinical trials. Our systematic review also found that for the in vivo experiments, many different skin wound sizes and types (ranging from 15 mm2 to 50 cm2) as well as different timepoints of evaluation (ranging from 7 to 240 days) were used. 20 , 28 Acetic acid and pepsin enzymatic methods were used for collagen extraction. For membrane manufacturing, dissolution of the materials in acetic acid, followed by freeze-drying or lyophilization methods were applied. Different sources of collagen (porcine, bovine and fish) were used for membrane manufacturing. In addition, both commercially available collagen and lab-made membranes were employed.
The most commonly used raw materials to extract collagen were bovine 26 , 28 , 34 , 35 , 37 and porcine tissues. 20 , 29 , 32 , 36 These sources produce type I collagen, which is the main protein of the mammalian extracellular matrix, thereby providing structural stability, strength and constituting an appropriate material for manufacturing skin membranes. 38 However, its usage is sometimes limited due to religious constraints related to avoidance of animal products and for the prevention of transmission of diseases such as bovine spongiform encephalopathy. 11 In this context, alternatives have been explored such as collagen from marine origin (e.g. fishes, marine sponges, jellyfishes). 11 , 21 Some authors have recently discovered that fish skin represents an excellent source for obtaining collagen and has been used as an alternative for mammalian collagen in many different applications such as cosmetics, tissue engineering and pharmaceutical uses. 39 We noted that collagen was frequently blended with other materials such as chitosan, 24 ,26–28, 30 , 33 graphene oxide, 16 alginate, 27 , 30 polyurethane, 28 , 35 zinc oxide, 25 and hyaluronic acid. 37 This is a common strategy used to optimize some characteristics of the membranes such as mechanical strength and bioactivity. 25
We observed that the studies included in this review used different protocols for collagen extraction and most of them involved dissolution in acetic acid and/or enzymes (such as pepsin and papain). 20 , 24 , 28 , 29 , 32 , 33 The literature describes a wide variety of collagen extraction processes from different sources, but emphasizes the importance of optimizing extraction conditions to achieve a higher collagen yield. 39 , 40 For example, to obtain collagen from marine sponges, protocols involve the use of EDTA, 40 trypsin digestion and water acidified with CO2. 41 In addition, trypsin and acetic acid have been widely used for collagen extraction from skin, bones and tendons of rats, bovine and porcine as they are able to digest proteins without causing significant damage to collagen fibers, thereby guaranteeing high extractability rate. 17 ,42–44 However, it is important to stress that there is a continuous need to develop optimized protocols for collagen extraction, focusing on obtaining a faster, less expensive and more efficient process. 17 In addition, special attention needs to be paid to the use of “green” chemical products, as there is high demand to reduce the use of hazardous substances for the extraction of natural materials. 45
The manufacturing process of the membranes used in this review mainly involved dissolving the materials in acetic acid, followed by freeze-drying or lyophilization. Freeze-drying have been used by many authors to create matrices, membranes and scaffolds with structures containing interconnected pores that resulted from nucleation and crystallization of ice, which are excluded and distributed into reticulations.46–48 Some authors used crosslinking agents in the manufacturing process. 25 , 32 It is known that collagen based biomaterials are susceptible to mechanical failure during handling which limits their applicability as biomaterials. 44 Consequently, one of the strategies for improving the thermal stability and tensile strength of collagen samples is the inclusion of crosslinking agents. 49
Most of the authors demonstrated, by SEM, that the membranes present porosity. Some authors used commercially available collagen and membranes and did not present morphological data. 22 , 29 ,34–37
Additionally, according to both the in vivo studies and clinical trials, it was demonstrated that there were positive outcomes on the process of wound healing after the treatment with collagen membranes. Data from the in vivo experiments demonstrated that all of the collagen membrane treated animals presented faster wound skin healing, with a smaller injury area, higher deposition of granulation tissue, and stimulation of reepithelialization and neoangiogenesis. These findings are in agreement with theories saying that collagen membranes applied to the site of the wound serve as protection against infections and attractants of fibroblast cells. 50 , 51 Bohn et al. stated that one of the mechanisms of action of collagen membranes on the process of tissue healing is that collagen is capable of reducing the levels of metalloproteinases, acting as a sacrificial substrate for excessive proteases in a chronic wound. 52 Also, Aoki et al. demonstrated that a collagen membrane promoted epithelization and modulated the inflammatory process in an experimental model of burns in rats. 20 The same positive outcomes were observed in the clinical trials, where there was faster healing in wounds treated with the membranes. It is also worthwhile pointing out that different skin wound models were studied by the different authors but the majority looked at burns or skin incisions. This highlights the effectiveness and flexibility of the collagen membranes to be used in skin wounds with different morphologies.
The outcomes of this review confirmed our initial hypothesis that collagen membranes (from diverse origins or blended with another materials) are able to accelerate the process of skin healing in different types of wounds. Consequently, this therapeutic intervention constitutes a promising treatment for burns and skin incisions, including their use in the clinical setting. However, some limitations of the present review needed to be highlighted. For example, in view of the differences in skin metabolism in healthy compared to compromised conditions (e.g. diabetes mellitus), the biological performance of collagen membranes might be different. This aspect has not been analyzed in this review. Additionally, some membranes present issues such as the need of dressing changes, which may cause discomfort or pain.
In conclusion, this review demonstrates that the different types of collagen membranes (manufactured only with collagen or in association with another material) were biocompatible and interacted well with skin tissue. The membranes offer protection to the wound and stimulate tissue growth both in in vivo studies and clinical trials, representing an efficient treatment for skin wounds. There is huge potential for this biomaterial to be used for skin tissue engineering purposes. Further research is required to evaluate the biological performance of collagen membranes in compromised situations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.