
Abstract
This article examines the association between mental health disorders and being identified as a bully among children between the ages of 6 and 17 years. Data from the 2007 National Survey of Children’s Health were examined. A total of 63,997 children had data for both parental reported mental health and bullying status. Bivariate analysis and logistic regression was performed to assess the association between mental health status and being identified as a bully with an age-stratified analysis and sub-analysis by type of mental health disorder. In 2007, 15.2% of U.S. children ages 6 to 17 years were identified as bullies by their parent or guardian. Children with a diagnosis of depression, anxiety, or depression had a threefold increased odds of being a bully. The diagnosis of depression is associated with a 3.31 increased odds (95% CI = [2.7, 4.07]) of being identified as a bully. Children with anxiety and attention deficit and hyperactivity disorder (ADHD) had similar odds. The diagnosis of a mental health disorder is strongly associated with being identified as a bully. In particular, depression, anxiety, and ADHD are strongly associated with being identified as a bully. These findings emphasize the importance of providing psychological support to not only victims of bullying but bullies as well. Understanding the risk profile of childhood bullies is essential in gaining a better grasp of this public health problem and in creating useful and appropriate resources and interventions to decrease bullying.
Introduction
Bullying is a specific form of youth violence that is defined as a repetitive, intentional form of aggression that involves a disparity of power between the victim and perpetrators (Olweus, 1993). Bullying among school-aged youth has increasingly been recognized as a major problem with a great impact on the health and well-being of our youth (Nansel et al., 2001; J. Srabstein & Piazza, 2008). Bullying is a widespread problem in the United States that can result in physical injury, social and emotional distress, and even death from suicide. In a 2011 nationwide survey, just over 20% of high school students reported being bullied on school property in the 12 months preceding the survey (Centers for Disease Control and Prevention, 2012). Given the large prevalence of bullying and its impact on children’s health, it has been identified as a major public health problem (J. C. Srabstein & Leventhal, 2010).
Few studies have focused on those who do the bullying; in particular, not much is known about the relationship between mental health and bullying. Prior studies of both bullies and victims of bullying have found an association between bullying and mental health disorders (Kaltiala-Heino, Rimpela, Marttunen, Rimpela, & Rantanen, 1999; Kaltiala-Heino, Rimpela, Rantanen, & Rimpela, 2000; Kumpulainen, Rasanen, & Henttonen, 1999; Kumpulainen et al., 1998); however, the majority of research on bullying and mental health has been conducted in Europe and Australia. To our knowledge no study has examined the prevalence of bullying among children with mental health disorders in the United States using national survey data. This study attempted to further understand the relationship between mental health problems such as depression, anxiety, and attention deficit disorder (ADD)/attention deficit and hyperactivity disorder (ADHD) on being a bully. Furthermore, this study is unique because it examines children across multiple age groups while most studies focus on bullying among middle school students and early adolescence. This broad age range analysis is important to assess as bullying has been reported to peak in middle school and occur at every grade level (Robers, Zhang, & Truman, 2010). The study hypothesis was as follows:
Method
Data Set
Data from the 2007 National Survey of Children’s Health (NSCH) were analyzed. The NSCH uses the State and Local Area Integrated Telephone Survey method to conduct a random digit-dialing telephone survey designed and directed by the Health Resources and Services Administration’s Maternal and Child Health Bureau. The survey was conducted by the Centers for Disease Control and Prevention’s National Center for Health Statistics (Blumberg et al., 2012). A total of 91,642 interviews were completed in households with children of ages birth to 17 years between April 2007 and July 2008. The survey was administered for one randomly selected child in each household that had an age-eligible child. The parent or guardian who knew the most about the health and care of the selected child was the interview respondent. Analysis was restricted to children between the ages of 6 and 17 years of age, as bullying status was only assessed in this age group. Analyses also excluded children if the respondent refused to answer questions pertaining to mental health or bullying status, if the respondent replied “don’t know” to a mental health or bully survey question, or if there was any missing data for any variable.
Bully Status
Children who bully others were identified by the interviewees’ response to “How often your child bullies or is cruel or mean to others. Would you say never, rarely, sometimes, usually, or always?” A dichotomous variable to identify those who bully others was created. Those subjects who responded never or rarely to the above question were placed in the “No” bully category, and those who responded sometimes, usually, or always were placed in the “Yes” bully category.
Mental Health Status
Mental health illness as defined by this study was the diagnosis of one or more of the following illnesses: depression, anxiety, and/or ADD/ADHD. The presence of a mental health illness was assessed by the respondent’s report to the following questions: “Has a doctor or other health care provider ever told you that your child had (a) depression, (b) ADD/ADHD, (c) anxiety?” A dichotomous variable was created whereby a “yes” response to any of the above questions was used to identify subjects with a history of mental health problems and a “no” response to each question was used to identify those without a history of mental health problems.
Demographics and Characteristics of the Study Population
The NSCH provides information on a large array of demographic characteristics as well information on health and behavior, family function, neighborhood and community characteristics, and type of schooling. For the purpose of this study, race and ethnicity were reported as separate variables with racial categories consisting of White, Black, Multiracial, and Other. Ethnicity was reported as Hispanic or non-Hispanic. Three age categories were created according to school age where 6 to 10 years represented elementary school, 11 to 14 years represented middle school, and 15 to 17 years represented high school. The capability of schools to provide emotional support to students largely depends on the available resources, which may vary by type of school. Therefore, type of schooling identified as public, private, or home schooling was considered a potential confounder as it has been shown that children identify schools as an important place to receive emotional support (Kidger, Donovan, Biddle, Campbell, & Gunnell, 2009). Furthermore, perceived neighborhood and community safety was defined as unsafe or safe. Neighborhood safety was assessed by the answer to the following question, “How often do you feel your child is safe in your community or neighborhood?” A dichotomous variable was created whereby those who responded never or sometimes were placed in “Unsafe” category and parents who responded usually or always were placed in the “Safe” category. Parental and child communication was used to determine parent−child relationship and was defined as poor versus good and was assessed by the response to the following question “How well can you and your child share ideas or talk about things that really matter?” Replies of “very well” and “somewhat well” were placed in the good category and those who replied “not very well” and “not very well at all” were placed in poor communication category.
Statistical Analysis
STATA version 11.1 (College Station, TX) was used for all statistical analyses with survey commands to account for the complex survey design. Thus, all percents are weighted to be nationally representative (Blumberg et al., 2012). Bivariate analysis using chi-square statistics was performed to compare demographic characteristics of children between the ages of 6 and 17 years by mental health status. The independent association between the diagnosis of a mental health disorder and being identified as a bully was determined using logistic regression. For model selection, bullying status was the dependent variable and mental health status was the independent variable. Children without a diagnosed mental health disorder were the reference group. Race, ethnicity, age, sex, neighborhood safety, and parent−child communication were included in the adjusted model as covariates. The adjusted model included all relevant demographic variables that were statistically significantly different by mental health status and were previously identified as risk factors for bullying (Cook, Williams, Guerra, Kim, & Sadek, 2010; Nansel et al., 2001). A sub-analysis by type of mental health disorder was also performed with the reference group being children without that specific disorder. Both bivariate and logistic regression analyses were performed to establish the association between type of mental health disorder and being identified as a bully.
Results
A total of 63,816 children had valid data for both mental health and bullying status. The percentage of age-eligible children missing information was 0.12%. In 2007, 15.2% of U.S. children between the ages of 6 and 17 years were identified as bullies and 14.9% carried a diagnosis of at least one mental health disorder. Table 1 compares demographic and behavior characteristics of children between the ages of 6 and 17 years by mental health status. There were significant differences between those with mental health disorders and those without mental health disorders by race, ethnicity, sex, age, neighborhood safety, parent−child communication, and bullying status. Of the children with a diagnosis of a mental health disorder, the majority (63.6%) were males. Children with a mental health diagnosis were older than those without a mental health diagnosis. Of those with mental health disorders just over 16% perceived their neighborhood as unsafe compared with 13% of those with no mental health problems (p = .002). The proportion of respondents who reported poor parent−child communication was greater among those with mental health disorders versus those without a diagnosis of a mental health disorder (8.3% and 2.2%, respectively, p < .001). The percentage of age-eligible children missing information for race was 5.8%, for ethnicity 0.97%, for sex 0.14%, for perceived neighborhood safety 1.1%, for parent child communication 0.2%, and for type of school 0.36%.
Characteristics of U.S. Children Between Ages 6 and 17 Years by Mental Health Status.
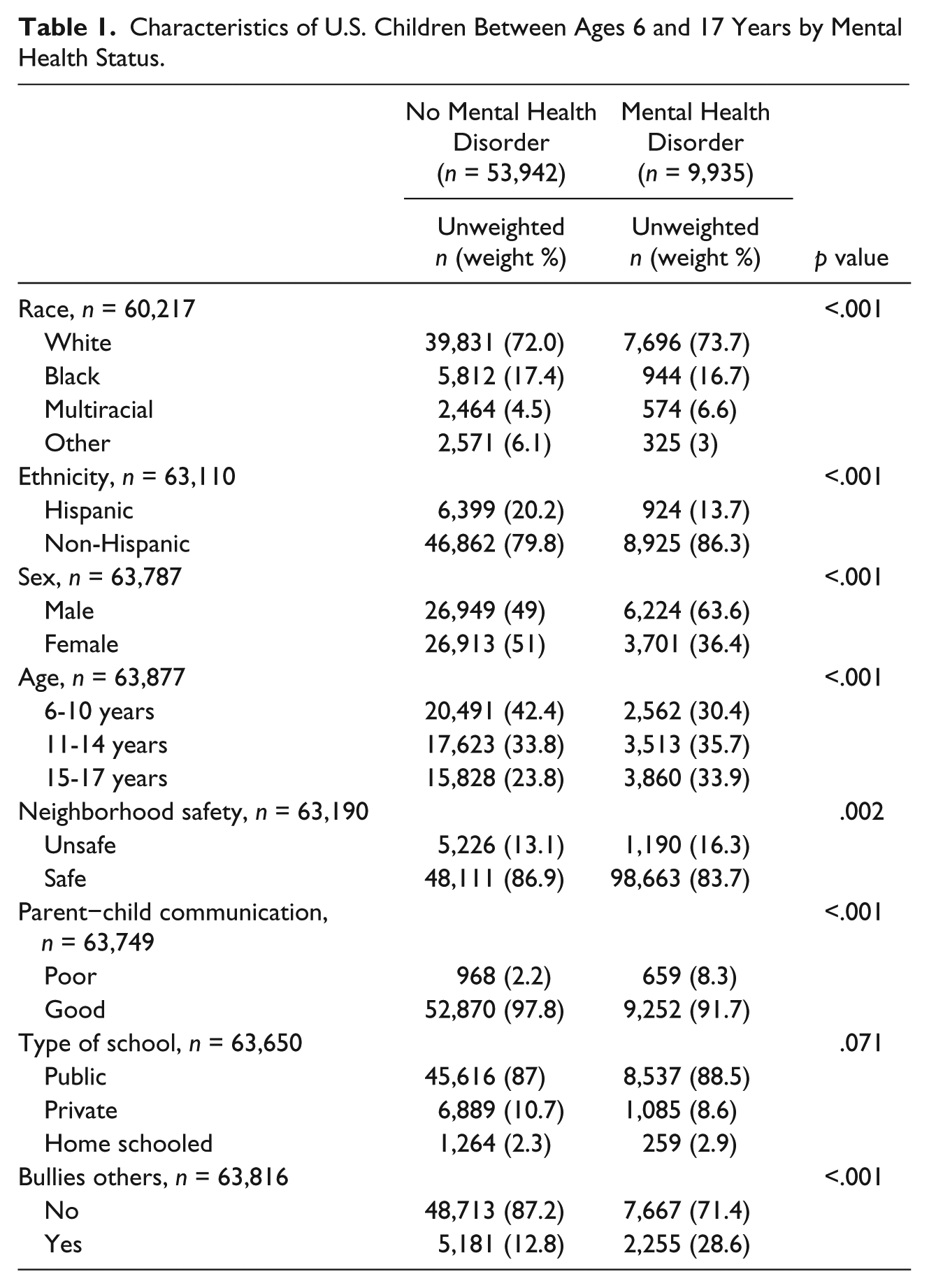
Children with mental health disorders were more likely to be identified as a bully compared with those with no mental health disorders. Of children with no mental health problems, 13% were identified as bullies compared with nearly 30% of children with mental health disorders (p < .001). Table 2 presents the crude and adjusted odds ratios (AOR) of mental health disorders by bully status. Children without a diagnosed mental health disorder were the reference group and the adjusted model controls for demographically relevant variables along with neighborhood safety and parent−child communication, which were both identified as confounders. Those with a diagnosis of a mental health disorder had nearly 3 times the odds of being identified as a bully compared with those without a mental health disorder (AOR = 2.81; 95% CI = [2.46, 3.22]).
Crude and Adjusted Odds for Bullying Among Children Between Ages 6 and 17 Years.
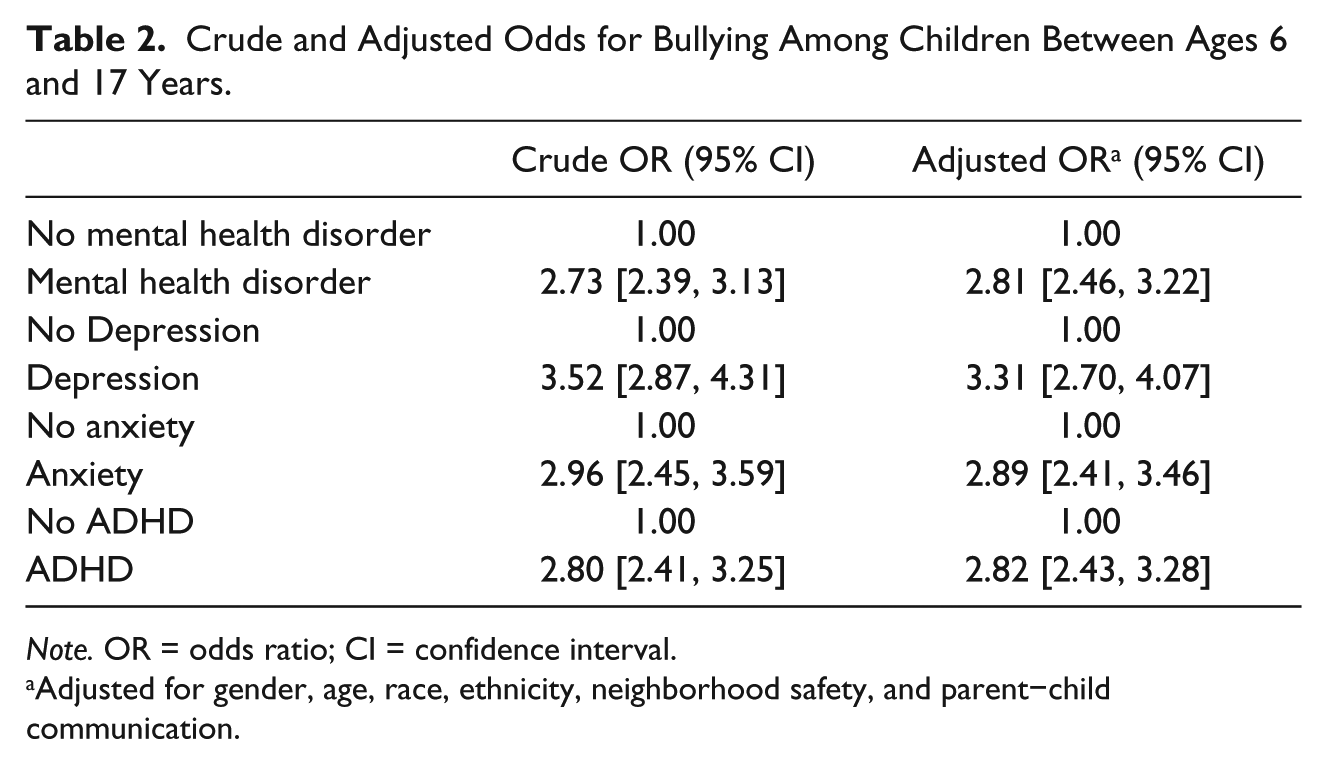
Note. OR = odds ratio; CI = confidence interval.
Adjusted for gender, age, race, ethnicity, neighborhood safety, and parent−child communication.
Table 3 compares demographic and behavior characteristics of children in the study sample by type of mental health disorder (depression vs. no depression, anxiety vs. no anxiety, and ADHD vs. no ADHD). This sub-analysis by type of mental health disorder revealed there were significant differences across each type of mental health disorder for race, perceived neighborhood safety, parent−child communication, and bully status. A sub-analysis by type of mental health disorder found that children diagnosed with depression, anxiety, and ADHD each had a threefold or nearly threefold increased odds of being a bully (Table 2).
Characteristics of U.S. Children Between the Ages of 6 and 17 Years by Type of Mental Health Disorder.
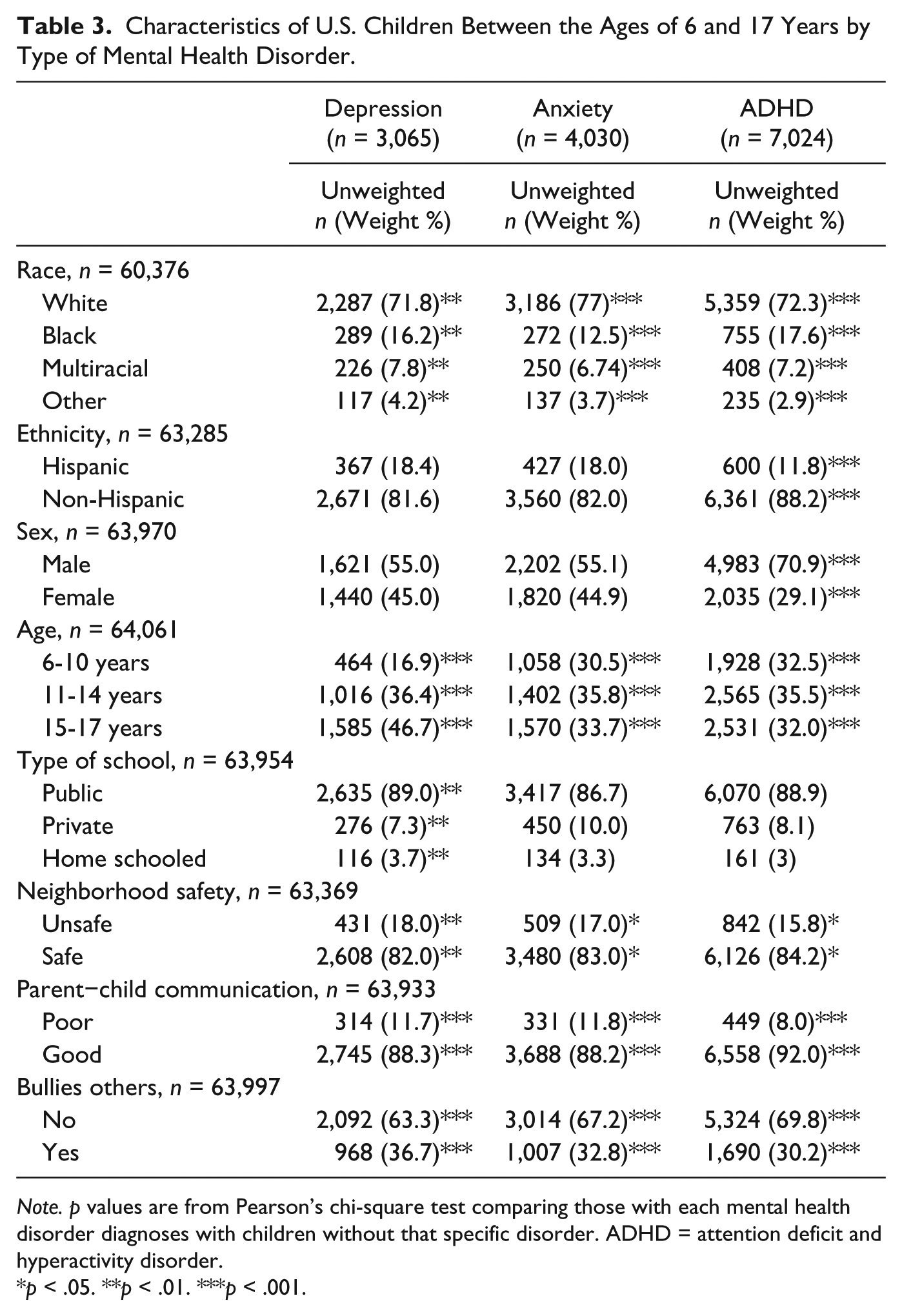
Note. p values are from Pearson’s chi-square test comparing those with each mental health disorder diagnoses with children without that specific disorder. ADHD = attention deficit and hyperactivity disorder.
p < .05. **p < .01. ***p < .001.
Discussion
While victims of bullying are most commonly associated with mental health disorders, this study demonstrated that the diagnosis of a mental health disorder is strongly associated with being identified as a bully. Furthermore, a sub-analysis by type of mental health disorder demonstrates that this strong association persists among children diagnosed with the individual diagnoses of depression, anxiety, and ADHD. These findings emphasize the importance of gaining a better understanding of the relationship between mental health disorders and bullying behavior to develop effective prevention and intervention programs.
Victims of bullying are at increased risk for mental health problems such as depression and anxiety, psychosomatic complaints such as headaches, and poor school performance (Kaltiala-Heino et al., 2000; Smokowski & Holland Kopasz, 2005). Conversely, youth who bully others are at increased risk for substance abuse, academic problems, and are more likely to become perpetrators of other forms of violence later in adolescence and adulthood (Smokowski & Holland Kopasz, 2005). Meanwhile youth who are identified as bully-victims, those who are both bullies and victims, suffer the most serious consequences and are at greater risk for both mental health and behavior problems (Kumpulainen & Rasanen, 2000; Nansel et al., 2001; Smokowski & Holland Kopasz, 2005). Although some studies have shown a relationship between mental health disorders and bullying (Kaltiala-Heino et al., 1999; Kaltiala-Heino et al., 2000; Kumpulainen et al., 1999; Kumpulainen et al., 1998), these studies primarily focus on victims and/or bully-victims. In addition, few studies have examined this association across multiple age groups. To our knowledge, no prior study has used national survey data to determine the prevalence of bullying among those with mental health disorders. Therefore, this study provides the most recent and comprehensive information about mental health illnesses and bullying.
In addition to finding strong associations between mental health disorders and bullying behavior, this study found similar prevalence rates for bullying and mental health disorders when compared with previous studies. Approximately, 15% of U.S. children were identified by their parents or guardians as bullies. This finding is consistent with a nationwide survey in which 13.4% to 24.4% (median: 19.4%) of students self-report being bullied on school property across different states (Eaton et al., 2010). Similarly, this study found that 16.2% of U.S. children have mental health disorders. This finding is similar to previous studies that have reported that 13% to 20% of U.S. children have mental health disorders (Merikangas, He, Brody, et al., 2010; Merikangas, He, Burstein, et al., 2010). Meanwhile, approximately 30% of those with mental health disorders were identified as bullies. A sub-analysis by type of mental health disorder found that the percent identified as bullies varied very little across depression, anxiety, and ADHD (all about 30%).
Although this study found that mental health disorders are associated with being a bully, the mechanism of this relationship is not well understood. Children with mental health disorders may be more likely to display bullying behavior or bullying others may cause psychosocial stress leading to the development of mental health disorders. However, the relationship between mental health disorders and bullies is most likely multifactorial in nature whereby family structure and socioenvironmental factors such as exposure to other forms of violence play a role in the development of mental health disorders and bullying behavior. Therefore, more studies are needed to better understand the mechanism by which mental health illnesses make it more likely for a child to display bullying behavior. While longitudinal studies may clarify this relationship, regardless of the mechanism children who are identified as bullies should be provided with mental health resources and children with mental health disorders should be screened for bullying behavior. While previous studies have shown the importance of providing mental health services to victims of bullying and bully-victims, this study demonstrates the need to provide mental health services to those who demonstrate bullying behavior as well. Providing appropriate mental health services may act as a form of bullying prevention but will also ensure the health and safety of the bullies, victims, and bully-victims.
This study has several limitations. First, NSCH is based on parental report. In addition to problems with recall bias that is inherent with survey-based studies, parents are probably less likely to identify or label their child as a bully. As a result this may have lead to a misclassification of children into the non-bully category instead of the bully category. This may have lead to an underestimation of bullying prevalence and may have biased the results toward the null. Nevertheless, in a study using 6- to 11-year-old children using National Longitudinal Survey of Youth, maternal report that their child “bullies or is cruel or mean to others” had validity as compared with a validated externalizing problems behavior scale (antisocial score was 1.3 standard deviations higher for maternally reported bullies than non-bullies, p < .001; Zimmerman, Glew, Christakis, & Katon, 2005). However, there is a lack of evidence to support that parental report of bullying coincides with adolescent self-report. In addition, the diagnosis of a mental health disorder may have been under-reported due to the stigma associated with a mental health diagnosis or lack of parental understanding of the diagnosis. However, regardless of this bias, a strong association between bullying and mental health was identified. Second, the NSCH did not ask parents if their child was a victim of bullying, and as a result, we were unable to control for this in our model. This is an important factor to take into consideration given that several studies have found that youth who are identified as bully-victims are at the greatest risk for both mental health and behavior problems (Brunstein Klomek, Marrocco, Kleinman, Schonfeld, & Gould, 2007; Kaltiala-Heino et al., 1999; Kumpulainen et al., 1999; Kumpulainen et al., 1998). Third, some children are underrepresented in this survey, including those from families who are homeless, those without landline telephones, and those children who are institutionalized. As a result, the survey data may be missing an important and high-risk population with mental health illnesses. Last, as mentioned previously this is a cross-sectional study therefore limiting the ability to evaluate for a causal relationship between bullying behavior and mental health disorders. However, no matter the causal relationship, bullies should be given mental health resources and children with mental health disorders should be screening for bullying behavior. Studies that assess the impact mental health services have on bullying behavior and the effect bully prevention programs have on children with mental health disorders may shed further light on this relationship.
In recent years, bullying has received a considerable amount of attention by the media, school officials, law enforcement, and communities nationwide, partly in response to several suicides among bullied children. As a result, many schools have rushed to implement anti-bullying campaigns and programs. In addition, anti-bullying legislation has been passed in 49 states over the past 12 years in support of schools’ efforts against bullying. This highlights the immense impact bullying has had on our society and our children’s mental health. The importance of providing psychological support to not only the victims of bullying but bullies as well cannot be overemphasized. Understanding the risk profile of childhood bullies is essential in gaining a better understanding of this public health problem and in creating useful and appropriate resources and interventions. To create more effective prevention programs, more information needs to be gathered on those who do the bullying. As our society works together to prevent bullying, further studies are needed to clarify the effect mental health disorders have on being a bully. Studies that evaluate the effectiveness of mental health services on bullying behavior would be most valuable in creating bullying prevention programs.
Footnotes
Acknowledgements
We gratefully acknowledge Dr. Siraj Amanullah and Dr. James Linakis for their thoughtful remarks and contributions when writing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.