
Abstract
People aging with HIV (PAWH) experience greater impairment in physical and pulmonary function than individuals aging without HIV. We examined whether baseline physical function was associated with subsequent pulmonary impairments. Associations of frailty and physical function (gait speed [m/s], grip strength [kg]) with pulmonary function (<80% predicted diffusing capacity for carbon monoxide [DLCO] and forced expiratory volume [FEV1]) 3 years later were modeled; age, HIV status, and smoking were assessed as effect modifiers. Among 1,024 men (54% PAWH, 10% frail, 51% prefrail), mean (SD) age = 53 (12) years, cumulative smoking = 12 (19) pack-years, gait speed = 1.1 (0.2) m/s, and grip strength = 36.6 (9.2) kg. Frailty, prefrailty, and weak grip strength were associated with higher odds of subsequent impaired DLCO and FEV1. Slow gait speed was associated with higher odds of DLCO impairment but not FEV1. No statistically significant modifications were found. Interventions to improve physical function may help preserve pulmonary function.
The life expectancy for people aging with HIV (PAWH) has increased due to effective antiretroviral therapy. 1 PAWH are at higher risk of developing earlier frailty and physical function impairments with greater severity.2,3 Frailty and pulmonary disease may co-occur due to shared risk factors and pathophysiological mechanisms, and a bidirectional association has been shown in the general population. 4 In our prior study, we showed that pulmonary impairment is associated with increased subsequent frailty risk, decreased gait speed, and weaker grip strength among men with and without HIV. 5 Building on our prior study, we hypothesize that frailty and physical function impairments are associated with subsequent impaired pulmonary function and that associations would be greater among PAWH, older adults, and smokers.
The Multicenter AIDS Cohort Study (MACS), now part of the Multicenter AIDS Cohort Study/Women’s Interagency HIV Combined Cohort Study (MWCCS), 6 began in 1984 and enrolled men with or at risk of HIV at four study centers (Baltimore/Washington DC, Chicago, Pittsburgh/Columbus, and Los Angeles) and three enrollment cohorts (before 1995, between 2001 and 2009, and 2010 and later). Institutional review board approval was obtained at each site. MACS details have been published elsewhere; in brief, participants completed semiannual visits for demographic, clinical, and laboratory assessments. 7 Pulmonary function tests (PFTs) were conducted from 2017 to 2019. Participants were invited to undergo PFTs; those who consented, completed PFTs, and had measurements that passed quality control standards were included here.8,9 Participants performed spirometry before and after inhaling 360 µg of albuterol via metered-dose inhaler, followed by single-breath DLCO testing (ndd EasyOne Pro, Zurich/Switzerland). Spirometry and DLCO tests underwent central quality control, and only acceptable-quality tests were included (Grades A, B, or C). 10 Predicted values were calculated using National Health and Nutrition Examination Survey (NHANES) equations for spirometry 11 and DLCO 12 accounting for factors such as age, sex, race, and height. Percent predicted DLCO and postbronchodilator percent predicted FEV1 in 1 s (FEV1) were categorized with <80% indicating impairment, except for models with an age interaction where absolute continuous DLCO and FEV1 were utilized (since percent predicted values are already adjusted for age). DLCO was corrected for hemoglobin (Hb) and carboxyhemoglobin. 13 The visit 3 years prior to PFTs was considered baseline for frailty, gait, and grip assessments, and if missing, then the next visit (up to 1 year prior to PFTs) was used. Participants who seroconverted during follow-up were excluded (n = 13).
Age, HIV serostatus, and cumulative pack-years of smoking were examined as potential effect modifiers on the associations of frailty and physical function with pulmonary function.
Baseline HIV serostatus, enrollment center, race, age, cumulative pack-years of smoking, and enrollment cohort were included in all models. In models examining interactions of age with DLCO or FEV1 (using absolute measurement), height (in cm) was also included. Potential confounders included education level, weight, body mass index, cardiovascular risk (Framingham coronary heart disease 10-year risk score %), diabetes defined as HbA1c ≥6.5% or fasting glucose ≥126 mg/dL or self-reported diagnosis of diabetes with medication use, use of cholesterol lowering medication, treatment for depression, current or prior confirmed diagnosis of kidney disease, hepatitis C seropositivity, hepatitis B (surface antigen positive or resolved vs. negative), and any use since last visit of alcohol, marijuana, cocaine, and/or heroin. Potential confounders were included in the model if their addition resulted in a ≥10% change in the primary exposure coefficient and excluded otherwise.14,15 Statistically significant precision variables that did not meet the confounder definition were also included in the final model.
Statistical analyses utilized SAS v9.4 (Cary, NC). Logistic regression models determined associations of frailty and physical function with pulmonary function. Exploratory analyses examined if frailty components other than gait speed or grip strength (i.e., weight loss, exhaustion, or low physical activity) were associated with pulmonary function impairment.
Interaction terms between frailty or physical function with age, HIV serostatus, or smoking were considered separately. A minimal clinically important difference was determined based on the literature and/or clinical expertise (Supplementary Data).
Of 1,133 men with PFTs, 1,024 and 1,007 met inclusion criteria for DLCO and FEV1 analyses, respectively. Overall, 54% and 55% of the DLCO and FEV1 participants, respectively, were PAWH. Cohort characteristics are reported in Table 1. Briefly, 16 and 14 participants with DLCO and FEV1 measures, respectively, were missing frailty measurement. On average, participants had 2.7 years (SD = 0.5) of follow-up between frailty and PFT measurements.
Baseline Characteristics of the Cohort (Diffusing Capacity for Carbon Monoxide and Forced Expiratory Volume)
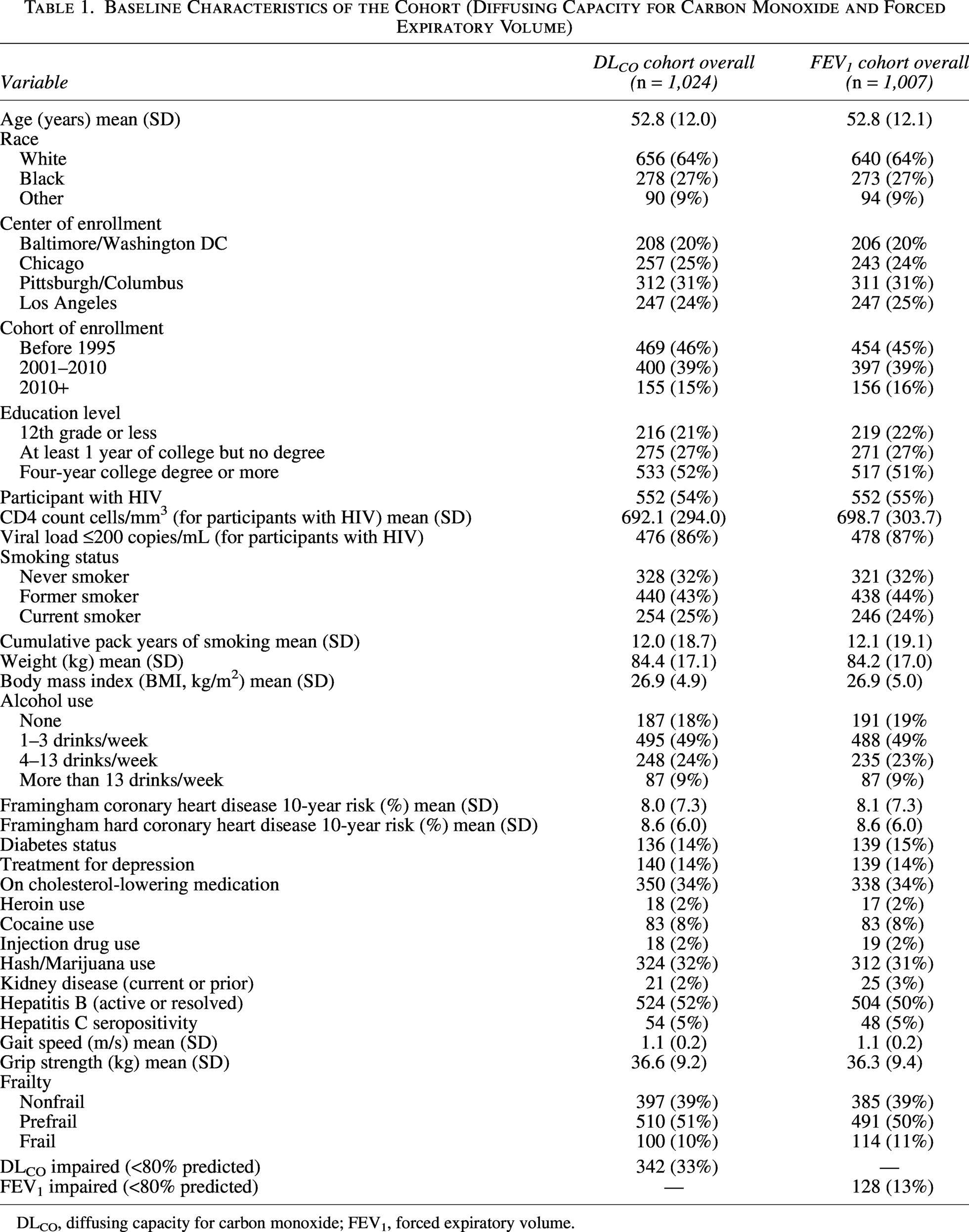
DLCO, diffusing capacity for carbon monoxide; FEV1, forced expiratory volume.
Compared to nonfrail participants, the odds of impaired DLCO (<80% predicted) were 1.94 [(95% CI: 1.42, 2.65); p < .001] times higher for prefrail participants and 2.53 [(1.54, 4.15); p < .001] times higher for frail participants (Fig. 1 and Supplementary Table S1a). Similarly, compared with nonfrail participants, the odds of impaired FEV1 were 1.44 times higher for prefrail participants and 2.32 times higher for frail participants compared with nonfrail ([95% CI 0.90, 2.32]; p = .13; [95% CI: 1.24, 4.32]; p = .008, respectively, Fig. 1 and Supplementary Table S1b). Every 0.05 m/s decrease in gait speed was associated with greater odds of DLCO impairment (OR = 1.07 [95% CI: 1.03, 1.12]; p < .001, Supplementary Fig. S2 and Table S2a) but not with FEV1 impairment (OR = 0.99 [95% CI: 0.94, 1.05]; p = .82, Supplementary Fig. S2 and Table S2b). Every 4 kg decrease in grip strength was associated with greater odds of both DLCO (OR = 1.25 [95% CI: 1.16, 1.34]; p < .001, Supplementary Fig. S2 and Table S3a) and FEV1 impairment (OR = 1.21 [95% CI: 1.10, 1.33]; p < .001, Supplementary Fig. S2 and Table S3b).
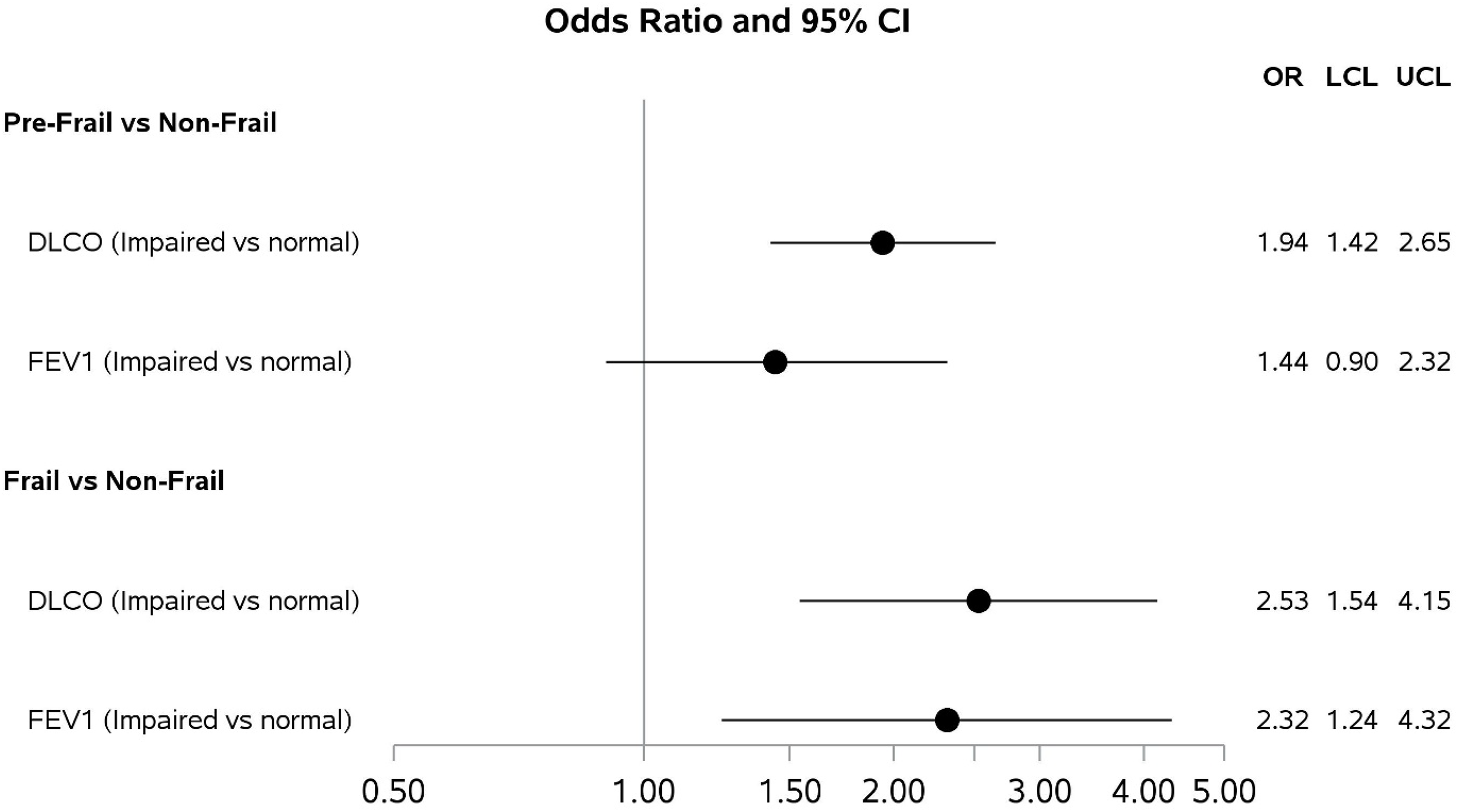
Odds ratios and 95% confidence intervals from adjusted logistic regression models for the association of frailty with subsequent impairment in DLCO* and FEV1**.*DLCO models adjusted for age, cohort of enrollment, center of enrollment, race, HIV serostatus, and cumulative pack-years of smoking** FEV1 models adjusted for age, cohort of enrollment, center of enrollment, race, HIV serostatus, cumulative pack-years of smoking, and Framingham hard coronary 10-year risk score.
Inconclusive results were found when exploring age, HIV status, or smoking modification of frailty on DLCO and FEV1 and age modification of grip strength on FEV1 (Supplementary Tables S4, S5, S6, S7, S8, S9, S10, S11, and S12). Therefore, primary results were presented without these interactions.
Neither age, HIV, nor smoking modified associations between gait speed or grip strength and DLCO or between gait speed and FEV1 (Supplementary Tables S13, S14, S15, S16, S17, S18, S19, S20, and S21). Neither HIV nor smoking modified the association between grip strength and FEV1 (Supplementary Tables S22, and S23).
In exploratory analyses, participants reporting low physical activity had higher odds of DLCO and FEV1 impairment compared with participants not reporting low physical activity (OR = 1.76 [95% CI: 1.32, 2.34]; p < .01, OR = 1.66 [95% CI: 1.07, 2.57]; p = .02, respectively, Supplementary Fig. S3). Unintentional weight loss and exhaustion were not significantly associated with subsequent pulmonary function (Supplementary Fig. S3).
Our results expand on the literature by showing associations between frailty and subsequent pulmonary function across multiple measures. Surprisingly, associations between frailty, gait speed, and grip strength with DLCO and FEV1 were generally similar regardless of age, HIV serostatus, and smoking history. Considering this and our previous study, 5 we propose a bidirectional association between pulmonary function and physical function impairment or frailty, as has been suggested in the general population. 4
We found no differences in associations between physical function or frailty and pulmonary function by HIV serostatus or age. We did observe a higher nonsignificant percentage of PAWH with impaired DLCO (36% vs. 31%) and frailty (10.3% vs. 9.4%). The lack of modification by HIV serostatus could result from the majority of the PAWH having limited disease progression, with 86% having a viral load ≤200 copies/mL and 74% having a CD4+ count >500 cells/mm3. The lack of modification by age could be due to one-time pulmonary function testing or a relatively narrow age range.
This study has several strengths. It is a multicenter study with a large sample size including men with and without HIV. We used well-validated objective physical function measures of gait speed and grip strength and lung function. The extensive demographic and health-related data allowed us to adjust for numerous covariates. This study also has limitations. Although the MACS has more recently combined with the Women’s Interagency HIV Study (comparable data not yet available), this study only included U.S. men, >90% of whom were White or Black, and study results may not be generalizable to women, other racial/ethnic groups, or non-U.S. populations. We looked at single measurements for both physical function/frailty and pulmonary function (at different time points); so, we could not examine changes over time. We acknowledge that participants with impaired pulmonary function at the 3-year follow-up may have had pre-existing impairments, and thus, there remains uncertainty about the directionality of the association. Future longitudinal studies are needed to confirm. Our interpretation of pulmonary function relied on percent-predicted values calculated using NHANES/NHANES III reference equations. Because these equations were developed from general-population samples, they may not fully capture normative lung function in the MACS cohort and could lead to some misclassification of impairment, thereby limiting generalizability.
In conclusion, our findings support a bidirectional association between pulmonary function and physical function and frailty. A better understanding of mechanistic pathways underlying both frailty and pulmonary functions is needed to develop improved treatments to reduce declines in physical and pulmonary function and improve overall quality of life.
Authors’ Contributions
M.A.: Conceptualization, methodology, software, formal analysis, writing—original draft, and visualization. K.M.K., A.M., D.C., G.D., K.C., and V.S.: Writing: review and editing. M.A.-M., C.D., T.T.B., and S.M.: Conceptualization, visualization, data analysis and interpretation, writing: review and editing. S.M.: Conceptualization, visualization, data analysis and interpretation, validation, supervision, and writing—review and editing. K.M.E.: Conceptualization, visualization, data analysis and interpretation, supervision, and writing—review and editing.
Footnotes
Acknowledgments
Data in this article were collected by the MACS/WIHS Combined Cohort Study (MWCCS). The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (Kathryn Anastos, David Hanna, and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D’Souza, Stephen Gange, and Elizabeth Topper), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen, Audrey French, and Ryan Ross), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky, Frank Palella, and Valentina Stosor), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels and Matthew Mimiaga), U01-HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Margaret Fischl, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf, James B. Brock, and Deborah Konkle-Parker), U01-HL146192; and UNC CRS (M. Bradley Drummond and Michelle Floris-Moore), U01-HL146194. The MWCCS is funded primarily by the
The authors gratefully acknowledge the contributions of the study participants and dedication of the staff at the MWCCS sites.
Author Disclosure Statement
The authors have no conflicts of interest to declare for this specific study.
Funding Information
M.A. was supported by the Integrative Physiology of Aging Training Grant
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.