
Abstract
Purpose:
To examine whether retrospectively assessed sports participation (SP) and competitive sports (CS) at the age of 12 years is associated with mental health and health behavior in young adulthood among males.
Design:
A cross-sectional study using self-administered questionnaires.
Setting:
Conducted prior to compulsory military refresher training course in Finland allowing geographically representative sample of Finnish young men.
Participants:
Six hundred eighty males aged between 20 and 35 years.
Measures:
Mental well-being was measured with the short version of Warwick-Edinburgh Mental Well-Being Scale and mental distress with 5 items of The Short Form Helalth Survey (SF-36) scale.
Analysis:
Binary logistic regression models.
Results:
Sports participation at the age of 12 was associated with better mental health in young adulthood, with both mental well-being (odds ratio [OR] = 1.86, 95% confidence interval 1.11-3.11) and mental distress (OR = 0.61, 0.41-0.90). Age, years of education, and current physical activity were controlled. Higher level of intensity of SP and the level of CS in childhood were associated with lower level of mental distress in adulthood. No association was found between the level of CS in childhood and mental well-being in adulthood. Further, youth SP seemed to be a risk factor for increased alcohol consumption and use of snuff in adulthood.
Conclusions:
Despite negative outcomes related to health behavior, the findings provide support for the association between youth SP and positive mental health outcomes in adulthood among males.
Keywords
Purpose
Mental health problems account for a large and growing share of ill health in high-income countries measured in disability-adjusted life years. 1,2 According to estimations from the Organisation for Economic Co-operation and Development, around 5% of the working-age population has a severe mental health condition and a further 15% is affected by a more common mental health condition causing significant socioeconomic cost. 3 The authors of the World Happiness Report 4 found that mental illness was the strongest predictor of misery in 3 rich countries, even stronger than poverty. However, mental health is more than the absence of mental disorder. Positive mental health is based on an assumption that focusing only on mental disorders does not give the whole picture of the state of mental health. Positive mental health is a human resource that can be used and strengthened in order to protect against mental health problems. 5,6 Identifying protective factors that prevent mental health problems is necessary to widen the knowledge of how to develop optimal preventive interventions.
There is a growing body of evidence that higher level of physical activity is associated with better mental well-being 7 –12 and that physical activity among children and young people is favorably associated with physical, psychological, social, and cognitive health indicators. 13 –21 Several prospective studies have provided evidence on the association between physical activity and mental well-being, indicating that low physical activity during adolescence is a risk factor for poor mental health in adulthood. 22 –27 There is also a growing body of evidence that physical activity interventions have beneficial effects across several physical and mental-health outcomes. 28–29 A recent systematic review based on longitudinal studies by Mammen and Faulkner 30 pointed out that physical activity could be preventive in the onset of depression. Despite growing number of studies reporting positive effects of physical activity and sports participation (SP), some studies report negative outcomes indicating SP to be related to higher level of alcohol consumption. 21,31 –36
Besides the association between the level of physical activity and mental well-being, the role of involvement in organized sport activities in childhood, on the state of well-being later in life, is an important topic of health-related research. In Finland, sport club activities play a dominant role in the leisure time activities of young people. Among children aged 7 to 14 years, 49% of girls and 61% of boys participate in sport club activities at least once a week. 37 Organized sport activities offer opportunities to young people to become involved with peers in a prosocial context, which promotes their social skills. Further, in organized sport activities, children have the possibility to interact with adult role models and receive social support. 38 The benefits of organized youth sport activities are well-known. 12,13,17,23,26,27,35 However, very little is known about the relationships between youth competitive sports (CS) and mental health in adulthood.
The aim of the present study was to examine whether (1) regularly participating in a sports clubs at the age of 12 years is associated with mental health (positive mental health as well as mental distress) in young adulthood, (2) experience of CS in childhood has an association with mental health in young adulthood, and (3) regular participation in sports in childhood (retrospectively assessed) is associated with health behavior in adulthood.
In this study, SP is understood as any type of organized physical activity, both competitive and noncompetitive by nature. Competitive sport is understood as taking part in organized physical activities that are competitive by nature, including also recreational sport if this includes competition. The competitive level and commitment of participant can, logically, vary.
Methods
The study sample consisted of young adult Finnish men who were called up to military refresher training. They voluntarily participated in the study prior to their military refresher training course organized around Finland in 2015. Of the 1106 invited reservists, 823 participated in the courses and 792 in the study. One hundred twelve were excluded from the analysis of the present study: 15 of them were females and 97 were over 35 years old. Thus, the study sample consisted of 680 men, age between 20 and 35 years (mean ± standard deviations [SD] age 26 ± [4] years).
The reservists were informed about the study in the call-up letter to the refresher course. All examinations were performed and the data were gathered at the beginning of the refresher course. Written informed consent was received from all study participants. The ethical approval for the study was granted by the Central Finland Health Care District, and the Headquarters of the Finnish Defence Forces gave a permission to conduct the present study. Health behavior and psychosocial well-being were measured with a self-administered questionnaire.
Mental well-being was measured with the short version of Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS). 39,40 The SWEMWBS includes 7 positively phrased items indicating positive mental health. Respondents rate their feelings over the previous 2 weeks from 1 (none of the time) to 5 (all of the time) on the following questions: “I’ve been feeling optimistic about the future,” “I’ve been feeling useful,” “I’ve been feeling relaxed,” “I’ve been dealing with problems well,” “I’ve been thinking clearly,” “I’ve been feeling close to other people,” and “I’ve been able to make up my own mind about things.” Weighted sum score was calculated higher score indicating better mental well-being. The scale was used in 4 refresher training courses only, and therefore, the sample size related to analysis with SWEMWBS was 362. In all other measures, the sample size was 680.
Mental distress was measured with the following 5 items of The Short Form Helalth Survey (SF-36) scale 41 : How much of the time during the last 4 weeks (1) have you been a very nervous person, (2) have you felt so down that nothing could cheer you up, (3) have you felt downhearted and blue, (4) have you felt worn out, and (5) did you feel tired. The response scale was 1 = all of the time, 2 = most of the time, 3 = a good bit of the time, 4 = some of the time, 5 = a little of the time, and 6 = none of the time. A sum score was calculated lower score indicating higher rate of mental distress.
Sports participation in the childhood was measured with the question “How often did you participate in training or other structured sports activity at the age of 12?” The responses were 1 = not at all, 2 = once a month, 3 = 2 to 3 times a month, 4 = 1 to 2 times a week, 5 = 3 to 4 times a week, and 6 = 5 times a week or more. For the analysis, the responses 2 and 3 were combined.
Competitive sports in childhood were measured with the question “If you participated in CS in childhood, at which level did you compete?” The responses were 1 = I didn’t participate in CS, 2 = school, 3 = sports club, 4 = district, 5 = national, and 6 = international. For the analysis, responses 2, 3 and 5, 6 were combined. In addition, dichotomized variable was recoded (1 = participated in CS, 0 = did not participate in CS).
Self-reported leisure time physical activity (LTPA) was determined from responses to a single question “Which of the following definitions best describe your LTPA habits? (Think of the last 3 months and consider all LTPA that lasted at least 20 minutes per session)” with 6 response categories: 1 = less than once a week, 2 = no vigorous activities, but light or moderate physical activity at least once a week, 3 = brisk physical activity once a week, 4 = vigorous activity twice a week, 5 = vigorous activity 3 times a week, and 6 = vigorous activity at least 4 times a week. For further analysis, a dichotomized variable was computed (1 = at least 3 times a week brisk physical activity, 0 = less physical activity a week).
Health behavior of study participants was determined with the following variable: smoking (yes/no), using snuff (yes/no), and binge drinking (at least once a week more than 6 units of alcohol at once, yes/no).
Statistical Analysis
Data were analyzed with IBM SPSS Statistics 24 software. Means and SD of mental health variable were calculated in different response categories related to participating in a sports club/CS at the age of 12. The association between mental well-being/mental distress and sports activity in childhood was tested using Kruskal Wallis and Mann Whitney U tests. The association between sports activity in the childhood and health behavior in young adulthood was tested using dichotomized variables in χ2 tests. Binary logistic regression models were calculated (method: enter) to explain the impact of other background variables in the relationship between high positive mental health and high mental distress with childhood sports activity. Organized by quartiles, groups of high positive mental health (SWEMWBS score more than 25,03) and high mental distress (sum score more than 27) were formed for these models. Age, years of education (9 years of less, 10-12 years, 13-15 years, 16 years or more), and present LTPA (no brisk physical activity, activity 1 to 2 times a week, activity at least 3 times a week) were used as covariates. The level of significance was set at .05.
Results
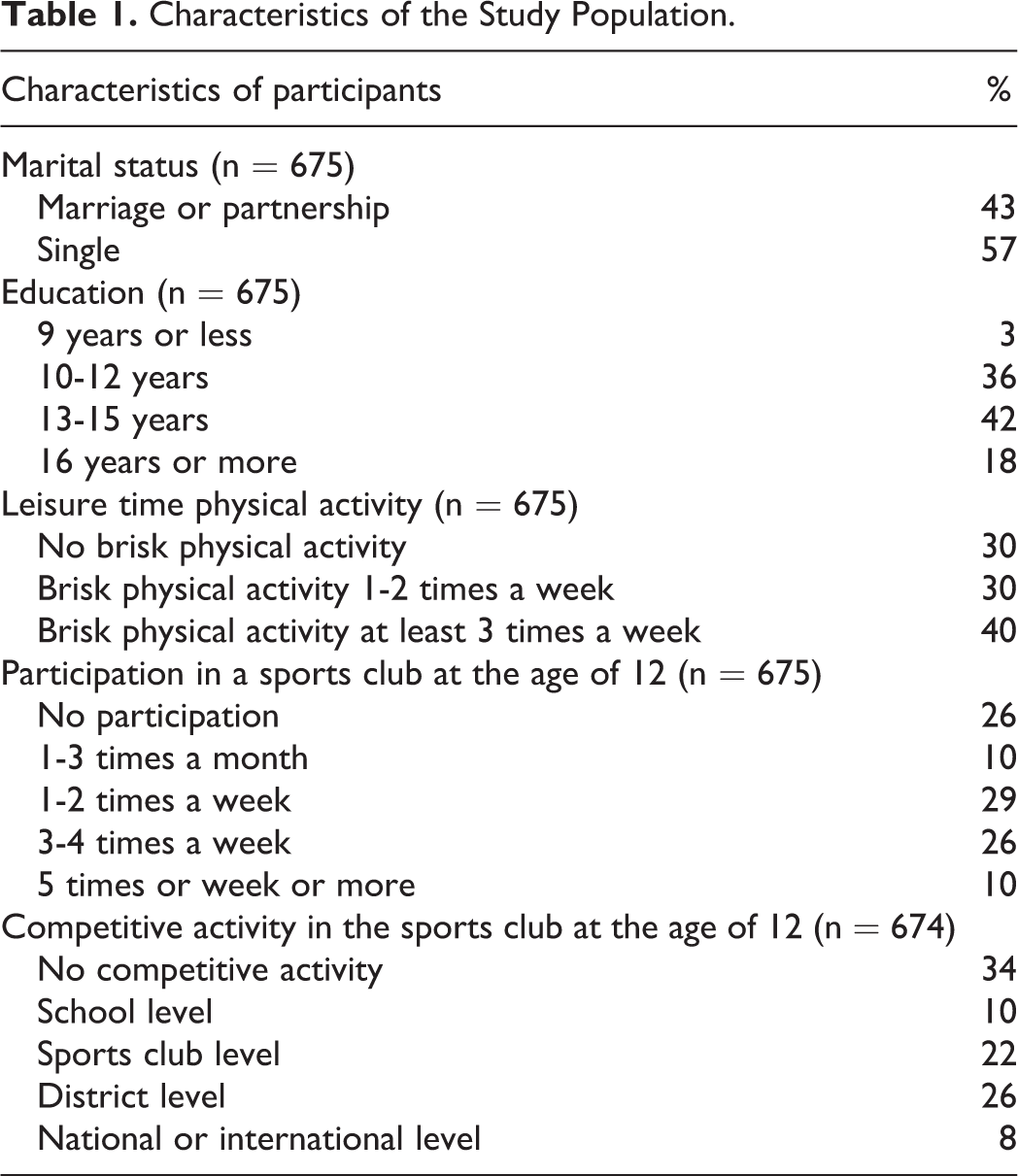
Of the study participants, 3 (74%) of 4 reported participation in a sports club at the age of 12. Among one-third (36%) of respondents, the participation had been quite intense with at least 3 to 4 times a week. Two-thirds (66%) reported to have experiences with CS at the age of 12. One-third (34%) had competed at least at district, national, or international level (Table 1).
Characteristics of the Study Population.
Sports participation in childhood was positively correlated with higher mental well-being in young adulthood (Table 2, F = 0.446, P < .05, df = 360). However, the level of intensity of participation did not seem to play a role. Further, no significant association was found between CS in childhood and mental well-being in adulthood. However, sport participation in the childhood seemed to positively associate with mental health when it comes to mental distress. Mental distress was lower among those who had participated in a sports club at the age of 12 years (Z = −2.391, P < .05) and among those who had experiences with CS (Z = −2.792, P < .01). The higher the level of intensity of SP (P < .001, χ2 = 25.857, df = 4) or the level of CS (χ2 = 8.592, P < .05, df = 3), the lower the experiences with mental distress in adulthood.
Association Between Sports Activity at the Age of 12 and Mental Well-Being/Mental Distress in Young Adulthood.
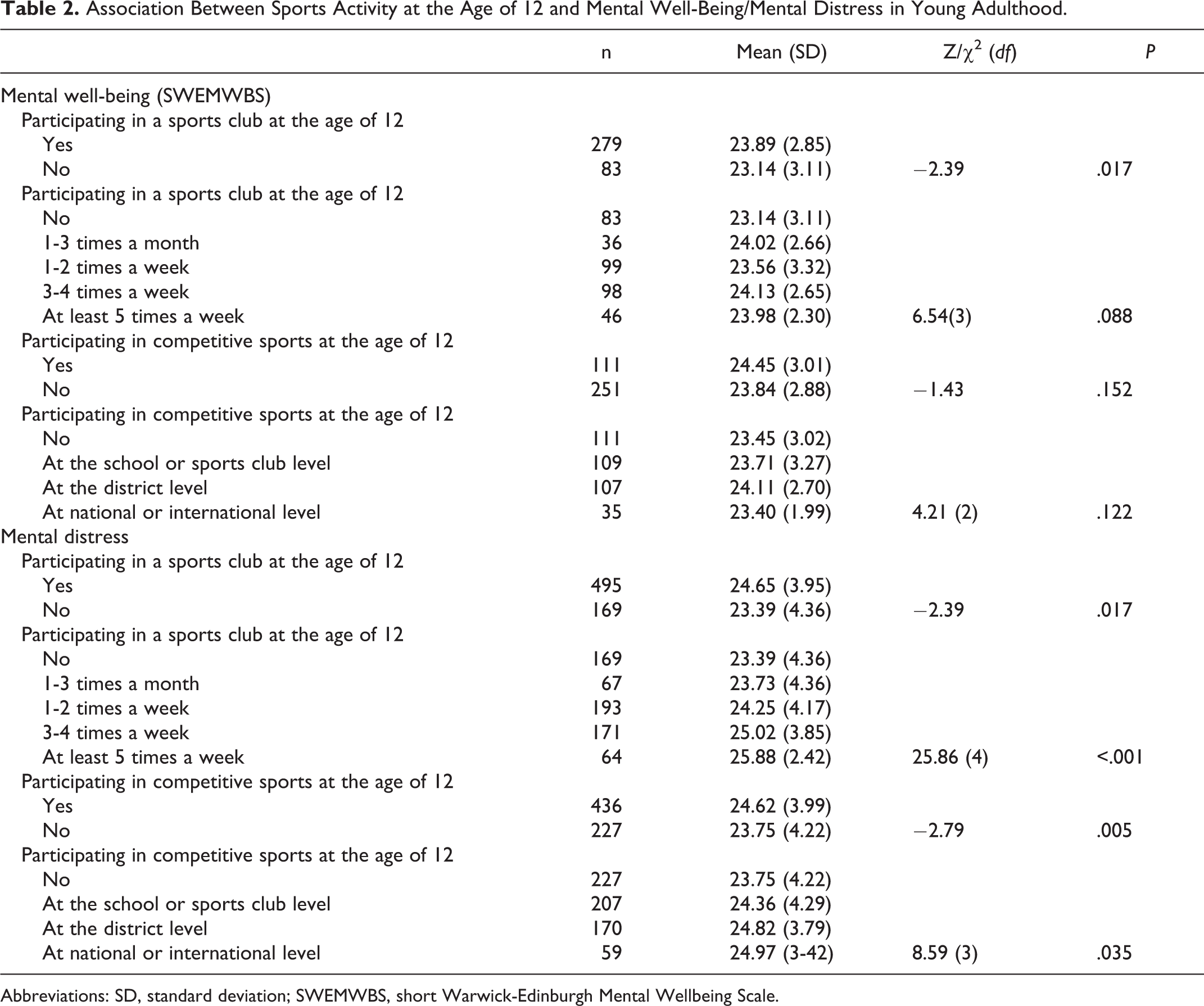
Abbreviations: SD, standard deviation; SWEMWBS, short Warwick-Edinburgh Mental Wellbeing Scale.
Binary logistic regression was performed to detect the association between childhood SP/childhood CS and current positive mental health/mental distress. Age, education, and the present LTPA were included in the model (Table 3). Positive mental well-being was positively associated with age, education, and childhood SP, but not with childhood CS or present LTPA. Mental distress was negatively associated with childhood SP or CS in the childhood as well as present physical inactivity, but not by age or years of education.
Binary Logistic Regression Models for High Positive Mental Health and High Mental Distress.

Abbreviations: CI, confidence interval.
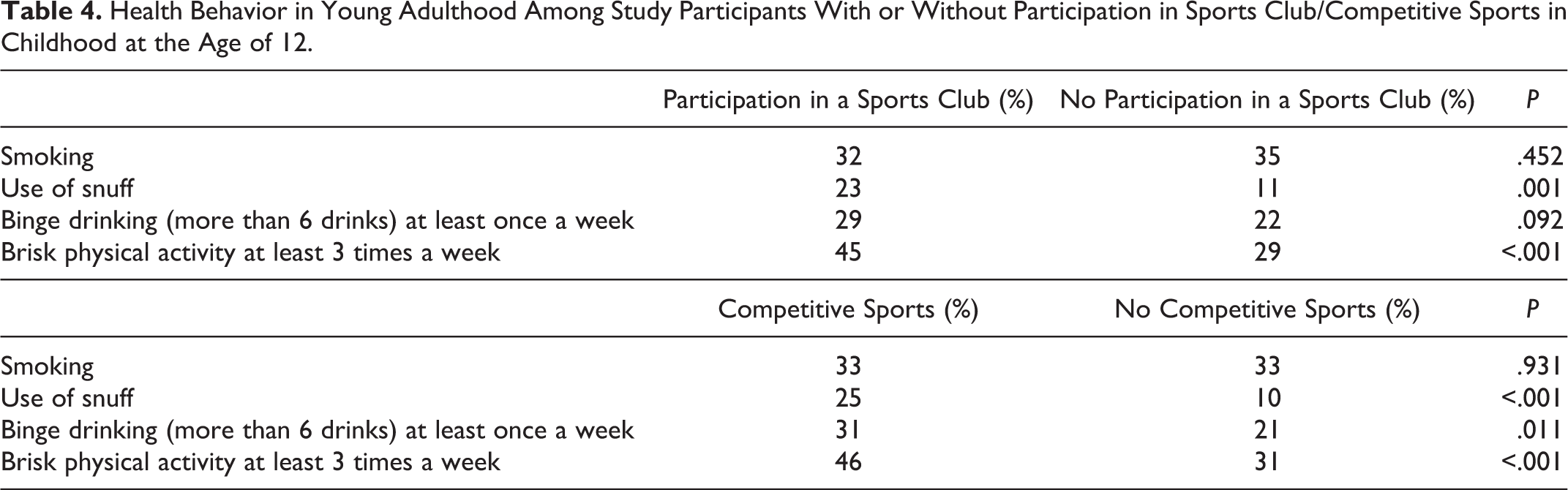
The use of snuff (P = .001) and brisk physical activity at least 3 times a week (P < .001) were more common among those who participated in a sports club at the age of 12 years (Table 4). Competitive sports in childhood was associated with the use of snuff (P < .001), binge drinking (P = .011), and physical activity in the adulthood (P < .001). Those with CS experiences at the age of 12 reported more commonly brisk physical activity at least 3 times a week. However, they were more likely to use snuff and have experiences with binge drinking (more than 6 units of alcohol) at least once a week in adulthood.
Health Behavior in Young Adulthood Among Study Participants With or Without Participation in Sports Club/Competitive Sports in Childhood at the Age of 12.
Discussion
The results of the present study indicated that SP at the age of 12 years is associated with better mental health in young adulthood among males, with both positive mental health and mental distress. This was also the case when controlling the impact of age, education, and present LTPA. These findings are in line with previous research, 42 –44 even though partly contradictory results related to the genders have been reported. Some studies have found an association only among females, 22 whereas the studies by Sagatun et al 44 and Flotnes et al 43 indicated that the level of physical activity has more influence on the development of mental health among boys compared with girls. Besides mental health benefits, previous research provides evidence that physical activity in childhood has the potential to improve self-regulation, life skills, and prosocial behavior, 31 as well as educational achievement and cognitive function. 38
The level of intensity of SPs in childhood did not seem to affect the state of mental health in later life from the perspective of positive mental health. This finding was somewhat unpredictable as the large European study by Richards et al 9 found a dose–response association between physical activity volume and happiness. The findings of the present study suggest that childhood SP, despite the intensity, could be a protective factor for mental health in later life. This may be related to the possibilities provided by youth SP for sense of social inclusion, possibilities to form peer relations, and possibilities to learn social skills.
Here, the higher level of intensity of SP in childhood was associated with lower level of mental distress in adulthood. This finding is supported by several studies, 12,23,26,27,42,44,45 indicating association between higher level of physical activity in childhood and lower level of mental health problems in later life.
An interesting finding was the association between the level of CS in childhood and mental health in young adulthood. The higher the level of CS in childhood, the lower was the level of mental distress in adulthood among study participants. This finding may be explained by the experience that CS teaches children valuable life skills and this may prepare them to handle challenges and pressures of daily life. Sports provide an opportunity for developing friendships and learning developmental skills across all domains. 18 Competitive athletes learn goal setting, bringing their best effort and to use coping strategies to handle with nervousness and anxiety involved with competitions, teaching commitment, and building self-esteem which is beneficial for mental health in later life. This finding is also supported by the study of Pyle et al 46 on university students, indicating that competitive athletes report fewer mental health problems compared with recreational athletes.
Those young men who had experiences with CS in childhood reported higher consumption of alcohol and snuff compared with those without CS in childhood. This finding draws support from several studies indicating that youth sport participation can protect against the use of illicit drugs but presents a higher risk of increased alcohol consumption. 21,31 –36 The authors of a systematic review of longitudinal studies by Kwan et al 32 pointed out that this risk effect of SP may be related to peer-group interaction and/or a culture of drinking that is associated with many sport events. Alcohol consumption is seen to be a socially acceptable form of celebration especially in team sports. Sports participation in childhood did not seem to affect smoking in young adulthood. However, it had an association with physical activity in later life. The findings showed that physical activity in adulthood was higher among those with SP in childhood.
Besides alcohol-related negative outcomes reported in some studies, the multiple health benefits for children who participate in organized physical activity are well documented. The findings of the present study provide initial support for the association between youth participation in CS and mental health outcomes in adulthood.
Limitations
Some methodological issues regarding the present study should be considered. First, with a cross-sectional design, this study provided data on childhood SP retrospectively only with 1 time point. However, there is a high dropout rate in SP during adolescence, especially at the age of 14 to 15 years. According to a Finnish report by Myllyniemi and Berg, 37 61% of boys at their age of 7 to 9 years participate in sport club activities at least once a week. This percentage drops to 32% in the age group of 15 to 19 years. Longitudinal data would be needed to detect changes in physical activity or SP over time.
Second, it would have been interesting to gather more specific data on involvement in sport activity in childhood including unorganized sport activity and overall health-related physical activity in childhood. Furthermore, SP was assessed by a number of times in a week, not by hours of physical activity.
Third, SWEMWBS is an established measure for mental well-being. 47,48 However, the sum score indicating mental distress using items of SF-36 has not been validated in previous research. Furthermore, despite statistically significant results, it is difficult to estimate the clinical significance of the findings.
Fourth, data on childhood living conditions and socioeconomic background of the parents would have been necessary to detect important confounding variables that affect mental health not only in the childhood but also in later life.
Despite the limitations noted, the study provides important data on the relationship between childhood SP and mental well-being in later life among young males, a group commonly difficult to reach in surveys related to mental health. Finland has compulsory military service, and the reservists who were invited to participate in the study can be seen as a geographically representative sample of Finnish young men, although northern and southern Finland were slightly overrepresented. Furthermore, one notable strength of the study was that mental health was measured from the perspective of mental well-being as well as from the perspective of mental health problems.
Conclusions
The results indicated that SP at the age of 12 years is associated with better mental health in young adulthood in males, with respect to both positive mental health and mental distress. According to the findings, the higher the level of CS in childhood, the lower was the level of mental distress in the adulthood among study participants. No association was found between the level of CS in childhood and positive mental health in adulthood. Furthermore, the study showed that youth SP can present a higher risk of increased alcohol consumption and use of snuff in adulthood.
Despites these negative outcomes related to health behavior, the present findings provide support for the association between youth SP and mental health outcomes in adulthood. Promotion of policies to increase participation in organized sports activities may be of benefit to a public health strategy to promote not just physical health but also mental health. It is important that all children are provided with same opportunities to take part in structured sports activities. This may be particularly important for children with greater psychosocial needs. It is important to address the change in habits of SP during adolescence to promote mental well-being in later life. Many adolescents stop being physically active after the age of 15 years, and thus, the dropout rate in SP in this age group is high. With regard to negative outcomes related to health behavior, sports clubs and coaches need to invest more time and effort to promote healthy lifestyle among participants.
Implications for Future Studies
Due to methodological limitations in the present study, it is not possible to conclusively state that youth sport participation carries clear positive effects on mental health later in life in males. Longitudinal study design testing causality and data on variable causing potential bias would be needed to understand the causal relationships between youth sport participation and mental health in adulthood. Furthermore, the impact and role of sports coaches in promotion of well-being and positive development would be an interesting topic for future studies.
So What?
Sports participation and competitive sports at the age of 12 is associated with better mental health in young adulthood among males.
youth sports participation presents a higher risk of increased alcohol consumption and use of snuff in young adulthood.
All children should be provided with opportunities to take part in structured sports activities.
Sports clubs need to invest more time and effort to promote healthy lifestyle among participants.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.