
Abstract
Purpose:
The purpose of this study was to explore the likelihood of meeting the physical activity guidelines in veterans who are obese by disability status.
Design:
We used data from the 2017 Behavioral Risk Factor Surveillance System, a cross-sectional telephone survey. The mean response rate was 44.9%.
Setting:
Respondents came from all 50 states, District of Columbia, and 3 US territories.
Patients:
Respondents included veterans self-reporting being obese (N = 13 798).
Measures:
We created a mutually exclusive disability variable: no disability, multiple disability, and limitations only with hearing, vision, cognitive, mobility, Activities of Daily Living, or Instrumental Activities of Daily Living. Physical activity guidelines were defined as 150 minutes/week of aerobic activity and 2 days/week of strength activities.
Analysis:
Prevalence ratios (PRs) were calculated by performing separate log-binomial regression models for meeting strength and aerobic recommendations on veterans who were obese.
Results:
Obese veterans with mobility limitations only or multiple disabilities were significantly less likely to meet the aerobic (PR = 0.74, P = .002 and PR = .62, P = .021, respectively) or strength (PR = .76, P < .001 and PR = 0.74, P < .001, respectively) recommendations, compared to not having a disability (n = 7964).
Conclusions:
Inactivity could be explained by a lack of inclusive weight loss programs for veterans with disabilities and barriers to physical activity encountered by people with disabilities. Two primary limitations of this study are self-report of obesity and physical activity and exclusion of adults in institutional settings.
Introduction
Obesity is associated with numerous health risks, including elevated blood pressure, type 2 diabetes, stroke, coronary heart disease, dyslipidemia, and depression. 1 -5 More than a third of all adults (37.7%) in the United States are obese and has been steadily increasing. 6 A greater proportion of adults with functional disabilities (such as serious difficulty walking or climbing stairs, and concentrating or remembering) are obese than people without a functional disability (45.0% vs 28.6%, respectively). 7 Similarly, the high prevalence of obesity in veterans is currently over 40%. 8,9 Obesity in veterans was most common in black women (51%), women with schizophrenia (56%), both female and male veterans with diabetes (68% and 56% respectively), and over 40% of veterans with any service connected disability. 8
Regular physical activity can reduce obesity and, independent of weight change, has positive impacts on obesity-related diseases. 10,11 According to the 2008 Physical Activity Guidelines for Americans, regardless of disability status, adults should engage in at least 150 minutes per week of moderate aerobic activity or 75 minutes per week of vigorous activity (or an equivalent combination thereof) and at least 2 days per week of strength activity. 12 Adults who were obese and over 50 years old, regardless of veteran status, were significantly less likely to be physically active. 13
In 2 separate studies using nationally representative samples, veterans engaged in more physical activity than nonveterans. 14,15 However, veterans were less likely to meet the physical activity guidelines than active duty personnel, with obese veterans being even less likely to meet the guidelines than over/normal weight veterans. 16 A limitation of these studies are that they did not account for the disability status of the veterans. This is important because a significantly greater percentage of adults with disabilities, regardless of veteran status, are inactive than adults without disabilities (47.1% compared to 26.1%, respectively). 7 One survey of veterans found that having a functional impairment was associated with decreased physical activity. However, this study was limited in that it was a small sample of veterans from the Seattle area. 17 To our knowledge, there has yet to be a study that has explored the physical activity habits of veterans by their disability status using a representative sample.
Purpose
Therefore, the purpose of this study is to explore the likelihood of meeting the physical activity guidelines in nationally, representative sample of veterans who are obese by disability status.
Methods
Design
The University of Florida Institutional Review Board approved this study as exempt (IRB201802692). The Behavioral Risk Factor and Surveillance System (BRFSS) is an annual, random-digit-dial telephone survey that collects data from all 50 states, District of Columbia, and 3 US territories. This study used the 2017 BRFSS core data set, which are a set of questions asked of everyone. 18 All BRFSS data are self-reported.
Sample
The study’s sample was from all respondents who self-reported being a veteran and obese (N = 13 798). Respondents were categorized as being a veteran, if they reported that they had ever served on active duty in the US Armed Forced (either in the regular military, national guard, or military reserve). Body mass index (BMI, kg/m2) was calculated based on the respondent’s self-reported height and weight. Respondents were categorized as obese if their BMI was 30.0 or higher.
Measures
Demographics
Behavioral Risk Factor and Surveillance System calculated an imputed age variable, with 6 categories (18-24, 25-34, 35-44, 45-54, 55-64, 65+). We collapsed these 6 categories into 3 mutually exclusive categories: 18 to 34 years old, 35 to 54 years old, and 55 years old or older. Race was collapsed into white non-Hispanic and other. Education was categorized into 3 mutually exclusive categories: graduated high school or less, attended some college or technical school, and graduated college or technical school. Income was categorized into 3 mutually exclusive categories: less than $25 000, $25 000 to less than $50 000, and $50 000, or more.
Disability
BRFSS asked respondents whether they have difficulty with hearing, seeing, concentrating or remembering, walking or climbing stairs, dressing or bathing, and doing errands. Respondents were able to select multiple disabilities. We therefore created a mutually exclusive disability variable with the following categories: no disability, hearing limitation only, vision limitation only, cognitive limitation only, mobility limitation only, Activities of Daily Living limitation only, Instrumental Activities of Daily Living (IADL) limitation only, and multiple disabilities.
Meeting physical activity recommendations
For the purposes of this study, meeting the physical activity recommendation is based on the 2008 physical activity guidelines. 12 BRFSS includes questions about physical activity that asks about the kind and frequency of aerobic and strength activities. Respondents were coded as meeting the aerobic guideline if they had at least 150 minutes of physical activity or 75 minutes of vigorous activity (or an equivalent combination). Respondents were coded as meeting the strength recommendation if they reported doing strength activities at least 2 days per week. 19
Analysis
We used variables with imputed responses whenever possible. Supplemental file 2 provides weighted prevalence estimates of “Don’t know/Not sure/Refused/Missing” for all covariates prior to analysis. We excluded respondents with “Don’t know/Not sure/Refused/Missing” data on covariates.
Stata version 14.1 was used for all analyses. 20 All analyses included veterans who were obese. Weighted, descriptive prevalence estimates (%) and 95% confidence intervals (CIs) were calculated for all veterans who were obese. The χ2 analyses were performed to identify differences in meeting aerobic and strength guidelines by disability status. Prevalence ratios (PR) were calculated by performing separate log-binomial regression models predicting the likelihood of meeting the strength or aerobic recommendations with sex, age, race, education, and income as covariates. 21 The comparison group is obese veterans without disabilities. The SUBPOP statement was added to the SVY Stata syntax, when exploring veterans who are obese.
Results
Table 1 presents the prevalence estimates (%) and 95% CIs of veterans who are obese (N = 13 798). The majority of obese, veterans were male (91.2%), white, non-Hispanic (74.2%), 55 or older (58.1%), and had an income greater than $50 000 (56.4%). Over a third (39.3%) of all veterans who were obese reported having at least 1 disability, with over a fifth (20.3%) reporting having multiple disabilities followed by mobility limitation only (8.9%).
Demographics of Obese Veterans.a
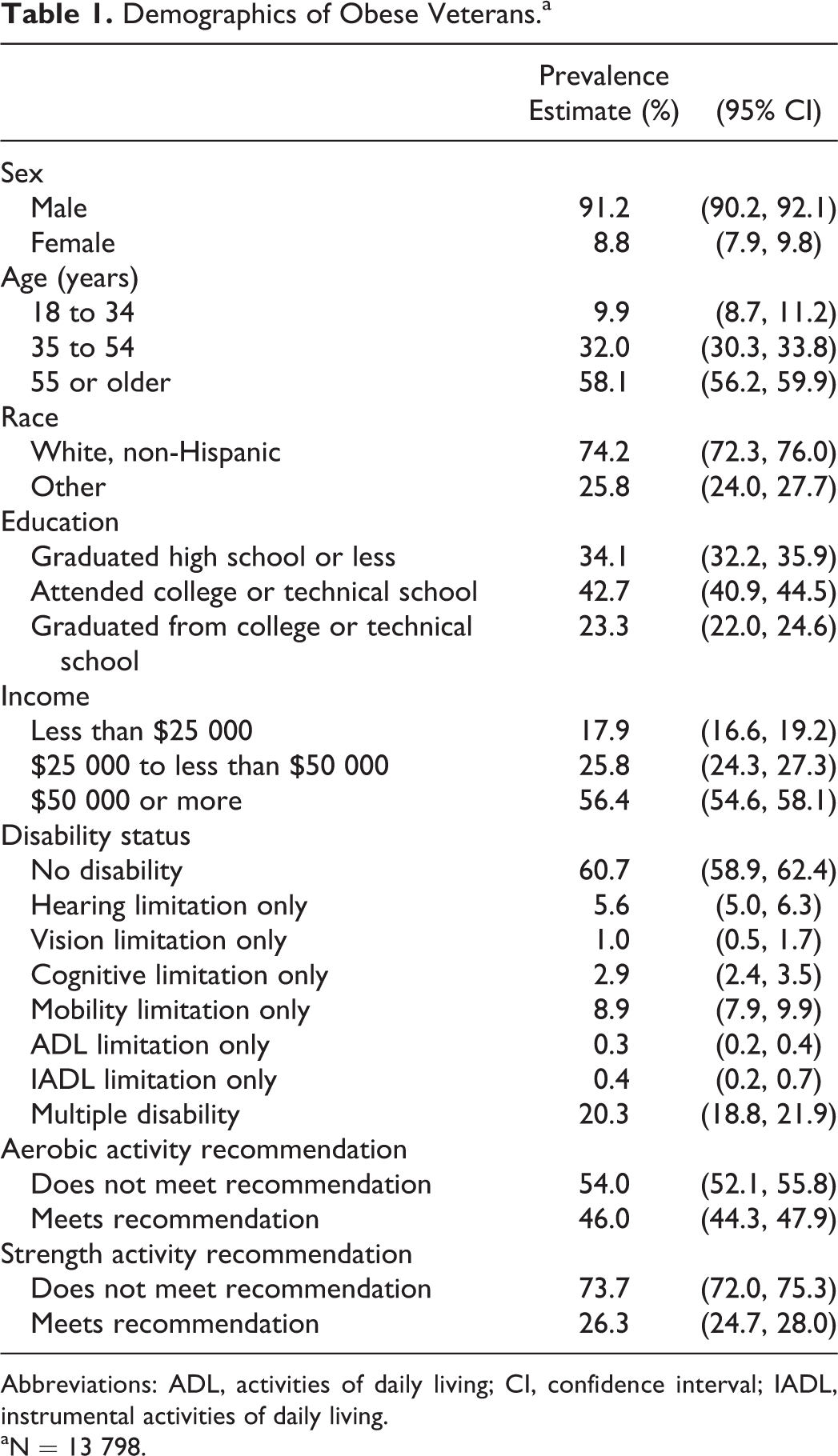
Abbreviations: ADL, activities of daily living; CI, confidence interval; IADL, instrumental activities of daily living.
aN = 13 798.
A significantly lower percentage of veterans who were obese with any disability met the aerobic activity recommendation when compared to veterans who were obese without a disability (38.0% vs 51.3%, respectively, χ2 = 231.8, P < .001). Likewise, a significantly lower percentage of veterans with any disability who were obese met the strength activity recommendation when compared to veterans without a disability who were obese (20.4% vs 30.1% respectively, χ2 = 160.8; P < .001). When controlling for covariates (Table 2), veterans who were obese and had a mobility limitation only or multiple disabilities were significantly less likely to meet the aerobic recommendation (PR = 0.74, CI: 0.64-0.86; P = .002 and PR = 0.62, CI: 0.54-0.70; P = .021, respectively) or strength recommendation (PR = 0.76, CI: 0.60-0.96; P < .001 and PR = 0.74, CI: 0.62-0.89; P < .001), when compared to not having a disability.
Likelihood of Meeting the Physical Activity Guidelines Among Veterans Who Are Obese by Disability Status.
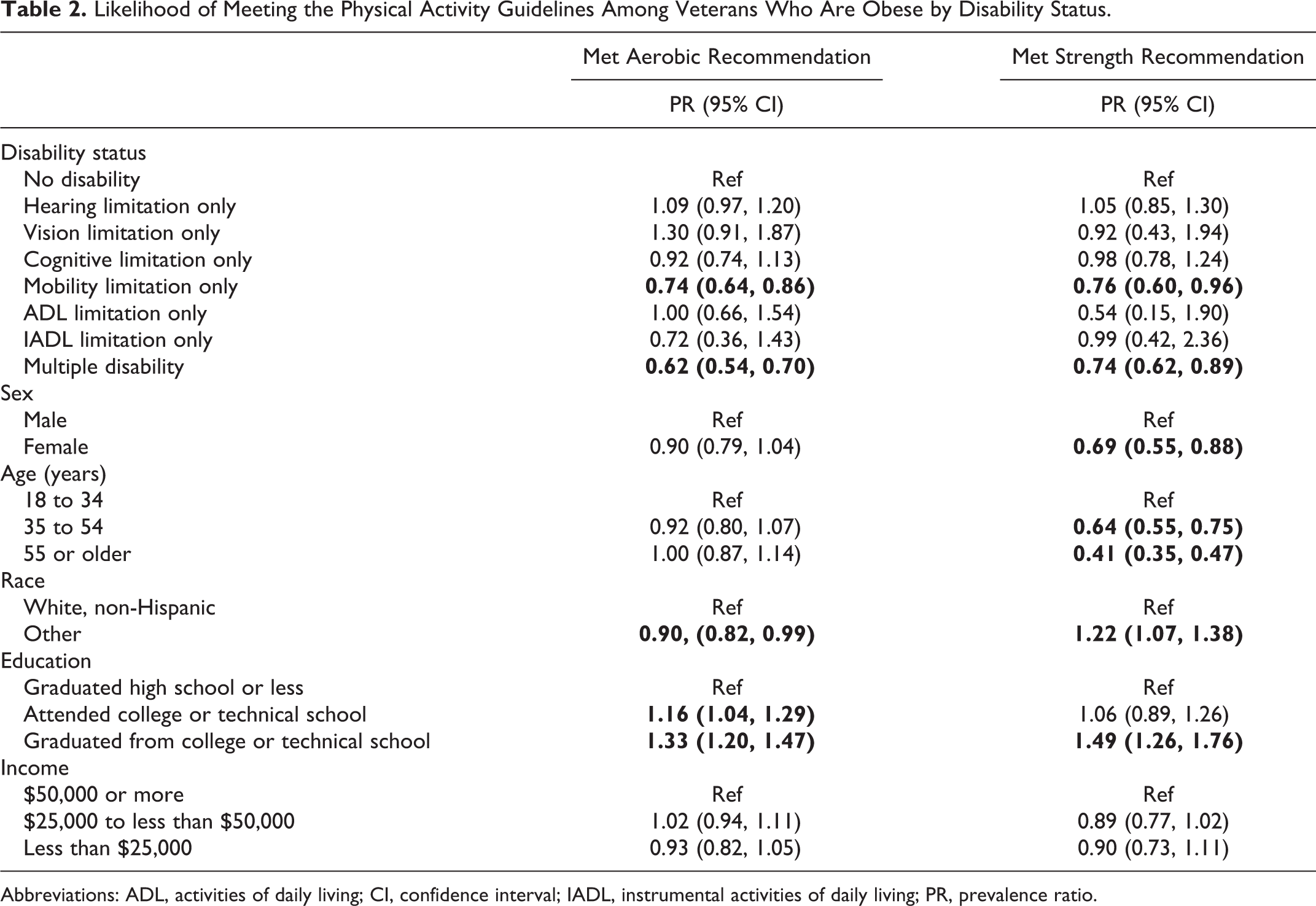
Abbreviations: ADL, activities of daily living; CI, confidence interval; IADL, instrumental activities of daily living; PR, prevalence ratio.
Discussion
To our knowledge, this study is the first to establish that obese veterans with a disability were less likely to meet the aerobic or strength physical activity recommendations than veterans who are obese without a disability. This finding is supported by other research which showed that disability status was significantly associated with decreased physical activity for people with disability. 7 Because disability and obesity status are highly correlated, programs should take disability status into account while promoting physical activity.
The VA has different programs to increase physical activity. The MOVE! Weight Management Program (MOVE!) and TeleMOVE! are national weight management programs developed for veterans to help them lose weight through physical activity and healthy eating. Studies have shown that MOVE! and TeleMOVE! have differing levels of success at achieving weight reduction. 22 -26 Other VA programs aimed to increase physical activity promotion include: MOVE! UP, Be Active and MOVE!, Physical Activity and Community Engagement, and Stay Strong. However, these programs do not examine the physical activity of veterans by their disability status. By understanding how physical activity changes for obese, veterans with disabilities, the VA could better tailor their programs to address barriers they face while trying to be active.
A possible reason that obese veterans with disabilities are significantly less likely, than obese veterans without disabilities, to meet the physical activity guidelines are that they encounter barriers limiting their ability to be active. The Social Ecological Model identifies 4 domains of influence of behavior (personal, social, organizational, and environmental). 27 -30 People with disabilities, regardless of veteran status, encounter barriers to physical activity across each of these domains. Personal domain barriers that were identified by veterans with disabilities included: pain (such as poorly fitted prosthetics or phantom limb pain), cost of adaptive equipment and sports, and lack of knowledge on where and how to exercise. Veterans with disabilities stated that not having family/friends to exercise with, changes in their relationship status (eg, divorce), and unsupportive clinicians were social barriers. 31 Organizational barriers include: inaccessibility of fitness centers (such as exercise equipment which are not accessible and staff who did not have disability training) and programmatic barriers in VA weight management programs including: travel distance to the nearest MOVE! program, scheduling conflicts, and a lack of a supportive, invested physician champion. 25,32 -35 Finally environmental barriers included environments that were not accessible to people with disabilities (eg, inaccessible sidewalks or fear of crime) and community design that which inhibit physical activity such as a lack of transportation forcing people with disabilities to use cars. 36 By understanding the effects of the multidimensional barriers, the VA could tailor their programs for veterans with disabilities.
Finally, the study findings are based on the 2008 physical activity guidelines, and in November 2018, the US Department of Health and Human Services released the second edition of the physical activity guidelines which stated that all activity counts toward the recommendation. 37,38 Future studies should explore the effects of this change in the physical activity guidelines, as it would enable more adults to potentially meet the physical activity guidelines.
This study is subject to 4 limitations. First, because BRFSS data are self-reported, respondents might provide socially desirable responses by inaccurately reporting their levels of physical activity or weight. This might lead to underreporting of weight and overreporting of physical activity. We expect this bias to be non-differential by disability status, that is, similar across all respondents regardless of disability, in which case our point estimates could be conservative. Second, BRFSS does not include adults living in institutional settings or group homes, which predominantly house people with disabilities. Because the VA provides nursing home and home health services, the prevalence of veterans with disabilities might be underestimated in the BRFSS sample, and the experiences of veterans who are obese and live in institutional care settings may not be represented by the results of this study. Thirdly, we cannot determine causality because BRFSS is cross-sectional. Finally, we are limited on covariates to include in our models because BRFSS is limited in the number of questions they can include in the survey or are available in the public domain. For example, while BRFSS offers an urban/rural variable, it is only asked of landline respondents. Future studies could explore using restricted data to identify urban/rural respondents for model inclusion.
Having a disability has been associated with many negative health behaviors, including inactivity. Having information about physical activity and disability status will better enable the VA to tailor their programs to accommodate veterans who are both obese and have a functional disability.
So What?
What is already known on this topic?
While veterans are generally more active than civilians, adults with disabilities are less likely to be active.
What does this article add?
This study explored the likelihood of meeting the physical activity guidelines for obese, veterans by their disability status. Veterans who are obese and have a disability were significantly less likely to meet the aerobic or strength physical activity guidelines than veterans who are obese without a disability.
What are the implications for health promotion practice or research?
The VA and other physical activity entities like fitness centers could better tailor their programs and facilities to accommodate veterans with disabilities. Additionally, researchers should explore how recent changes in physical activity guidelines effect these results.
Supplemental Material
Supplemental_File_1 - Likelihood of Meeting Physical Activity Guidelines of Veterans Who Are Obese by Disability Status
Supplemental_File_1 for Likelihood of Meeting Physical Activity Guidelines of Veterans Who Are Obese by Disability Status by Vijay Vasudevan, Erin Bouldin, Shannon Bloodworth and Linda Rocafort in American Journal of Health Promotion
Supplemental Material
Supplemental_File_2 - Likelihood of Meeting Physical Activity Guidelines of Veterans Who Are Obese by Disability Status
Supplemental_File_2 for Likelihood of Meeting Physical Activity Guidelines of Veterans Who Are Obese by Disability Status by Vijay Vasudevan, Erin Bouldin, Shannon Bloodworth and Linda Rocafort in American Journal of Health Promotion
Footnotes
Acknowledgments
This research was conducted when Vijay Vasudevan was a Postdoctoral Fellow at the Center of Innovation on Disability and Rehabilitation Research at the NF/SG Veterans Health System. Vijay’s time was supported by a NF/SG Veterans Health System, Health Services Research and Development postdoctoral fellowship. Shannon Bloodworth and Linda Rocafort are paid employees of the NF/SG Veterans Health System. This study did not receive any other financial support from grants or other means. The authors have no other conflicts of interests to report. The research presented in this paper is that of the authors and does not represent the views of the US Department of Veterans Affairs or the United States Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.