
Abstract
Purpose
To examine associations between past-year mental illness (MI) diagnoses and e-cigarette use status.
Design
Data were obtained from the National College Health Assessment, a nationally recognized cross-sectional survey of university students.
Setting
Participants were recruited from 2-year and 4-year public and private universities across the United States from 2017-2019.
Subjects
The analytic sample included 277 291 university students.
Measures
Self-reported past-year MI diagnosis, binarily coded, served as the primary predictor. The outcome was e-cigarette use status (never, noncurrent, and current user).
Analysis
Multinomial logistic regression models were used to estimate relative risk ratios (RRR) of e-cigarette use, as predicted by past-year MI diagnoses, age, race/ethnicity, sex and gender, sexual identity, geographic region, and other combustible tobacco, alcohol, and marijuana use.
Results
Compared to those who had never received any MI diagnosis in the past year, those who did had a 16% higher relative risk (RRR = 1.16, 95% CI: 1.11, 1.20) of being a noncurrent e-cigarette user and a 33% higher relative risk (RRR = 1.33, 95% CI: 1.28, 1.38) of being a current e-cigarette user. Schizophrenia, substance use or addiction, bipolar disorder, and attention deficit and hyperactivity disorder (ADHD) diagnoses demonstrated the strongest associations with noncurrent and current e-cigarette use.
Conclusion
Results suggest the need to screen young adults for e-cigarette use and mental health indicators to facilitate early detection and timely intervention for at-risk university students.
Purpose
Mental health is a growing area of concern in the United States (US), especially among young adults. In 2021, young adults (aged 18-25 years) had the highest prevalence of mental illness (MI), when compared to older adults (aged 26-49 years). 1 Nearly half (48%) of young adults (aged 18-25 years) have reported experiencing symptoms of depression or anxiety over the past year. 2
This is concerning, given that there are higher reported rates of nicotine use among young adults with MI, when compared to those without MI. 3 Young adults with MI may use nicotine to mitigate symptoms of MI or to counteract negative side effects from psychotropic medications (e.g., self-medication).4,5 However, nicotine use may increase the risk of cognitive and psychiatric disorders, 6 while also interfering with the development of adaptive coping skills – especially during adolescence. 7 Furthermore, long-term brain changes resulting from continued nicotine use can lead to addiction, the experience of withdrawal symptoms, and increased difficulty quitting. 8
Individuals with MI are generally more likely to try e-cigarettes, be current users of e-cigarettes, and be susceptible to e-cigarette use in the future. 9 E-cigarettes are currently the most commonly used nicotine containing product among youth and young adults 10 and there is a growing literature demonstrating associations between MI symptoms of anxiety and depression and e-cigarette use among young adults.9,11-20 Specifically, higher anxiety and depression symptoms are associated with current e-cigarette use. 16 Former and current e-cigarette users have higher odds of reporting a clinical diagnosis of depression, when compared to never users, according to a cross-sectional study using data from the Behavioral Risk Factor Surveillance System (BRFSS) from 2016 to 2017. The same study demonstrates a dose-response relationship between increasing frequency of e-cigarette use and greater likelihood of depression. 21 Further, depression has been associated with the escalation of e-cigarette use, in terms of the number of reported days used, while anxiety was associated with a decreased rate among a sample of high school students. 22 Another study has demonstrated a bidirectional relationship, such that higher baseline depressive symptoms predicted subsequent e-cigarette use and that sustained e-cigarette use was associated with a greater rate of increase in depressive symptoms. 23
Yet, few studies examine the association between e-cigarette use and MI symptoms beyond depression and anxiety. For example, a 2019 study of undergraduate and graduate students (n = 195 443, aged 18-39 years) found that e-cigarette use was significantly associated with higher levels of attention deficit and hyperactivity disorder (ADHD) symptoms. In addition, respondents with a history of ADHD were 1.72 times more likely to use e-cigarettes, compared to those without ADHD. 24 Sleep disorders, such as insomnia or sleep deprivation, were also associated with e-cigarette use among young adults. Another study using pooled, cross-sectional data from the 2017 and 2018 BRFSS (n = 19 701 respondents, aged 18 to 24 years), found that former e-cigarette users were 1.17 times more likely to report sleep deprivation, compared to never users. 25
Despite growing evidence for associations between symptoms of MI and e-cigarette use, few studies consider differences across e-cigarette use status (e.g., never user, noncurrent user, current user). Additionally, many of these studies primarily focus on depression, anxiety, or composite scores of MI symptoms.26-31 Thus, the current study expands upon the existing literature by examining associations between prior MI diagnoses and current e-cigarette use among a sample of young people.
Methods
Design
Data was obtained from the American College Health Association’s National College Health Assessment (ACHA-NCHA), a nationally recognized survey that has provided data on college students’ health habits, behaviors, and perceptions since 2000. Convenience samples of students at voluntarily participating 2-year and 4-year public and private universities across the United States are surveyed on physical health, mental health, use and dependence on alcohol, tobacco, or drugs, sex behavior and contraceptive practices, weight, nutrition, and exercise along with demographic information. 32 The ACHA-NCHA II data reflects survey responses from 1 440 197 individuals across 1532 colleges and universities from 2008 to 2019. 33
Sample
The analytic sample for this study included 277 291 individuals who were surveyed between Spring 2017 and Spring 2019. Permissions for conducting the research at each study site is granted by individual university institutional review boards. Consent from students is implied by their participation in the survey, as they are given the right to refuse to participate. This secondary analysis was approved as exempt from full review by Advarra Institutional Review Board.
Measures
The outcome of interest was e-cigarette use status. E-cigarette use status was measured using the following question: “Within the last 30 days, on how many days did you use e-cigarettes?” Responses were categorized into never used, former or noncurrent user (i.e., used previously, but not in the last 30 days), and current user (i.e., used in the past 30 days).
Past-year MI diagnosis was the primary predictor, measured using: “Within the last 12 months, have you been diagnosed or treated by a professional for any of the following?” The mental health illness categories included: anorexia, anxiety, ADHD, bipolar disorder, bulimia, depression, insomnia, other sleep disorder, obsessive compulsive disorder (OCD), panic attacks, phobia, schizophrenia, substance abuse or addiction (alcohol or other drugs), other addiction (e.g., gambling, internet, sexual), or other mental health condition. Responses were binarily coded (e.g., no vs yes). Treatment for MI diagnosis was categorized as: no MI diagnosis; diagnosed with MI, but not treated; diagnosed with MI and treated (inclusive of yes, treated with medication; yes, treated with psychotherapy; yes, treated with medication and psychotherapy; yes, other treatment).
Additional covariates included age (18-20, 21-24, 25+ years), race/ethnicity (Non-Hispanic White, Non-Hispanic Black, Hispanic/Latino, Non-Hispanic Asian American, Native Hawaiian, or Pacific Islander, Non-Hispanic American Indian or Alaskan Native, and another race/ethnicity, including multiracial), sex and gender (female, male, nonbinary), sexual identity (asexual, bisexual, gay, lesbian, pansexual, queer, questioning, same-gender loving, straight/heterosexual, another identity), and region (Northeast, Midwest, South, West).
Analysis
Descriptive statistics are provided for sample characteristics. The prevalence of e-cigarette use status by semester (e.g., Spring 2017 to Spring 2019) is presented, separated by any MI diagnosis (yes vs no MI diagnosis). Relative risk ratios (RRR) and 95% confidence intervals (CI) for e-cigarette use status are estimated using multinomial logistic regression models that include the effects of past 12-month mental health illness diagnoses and covariates.
Results
Sample Characteristics (National College Health Assessment, 2017-2019).
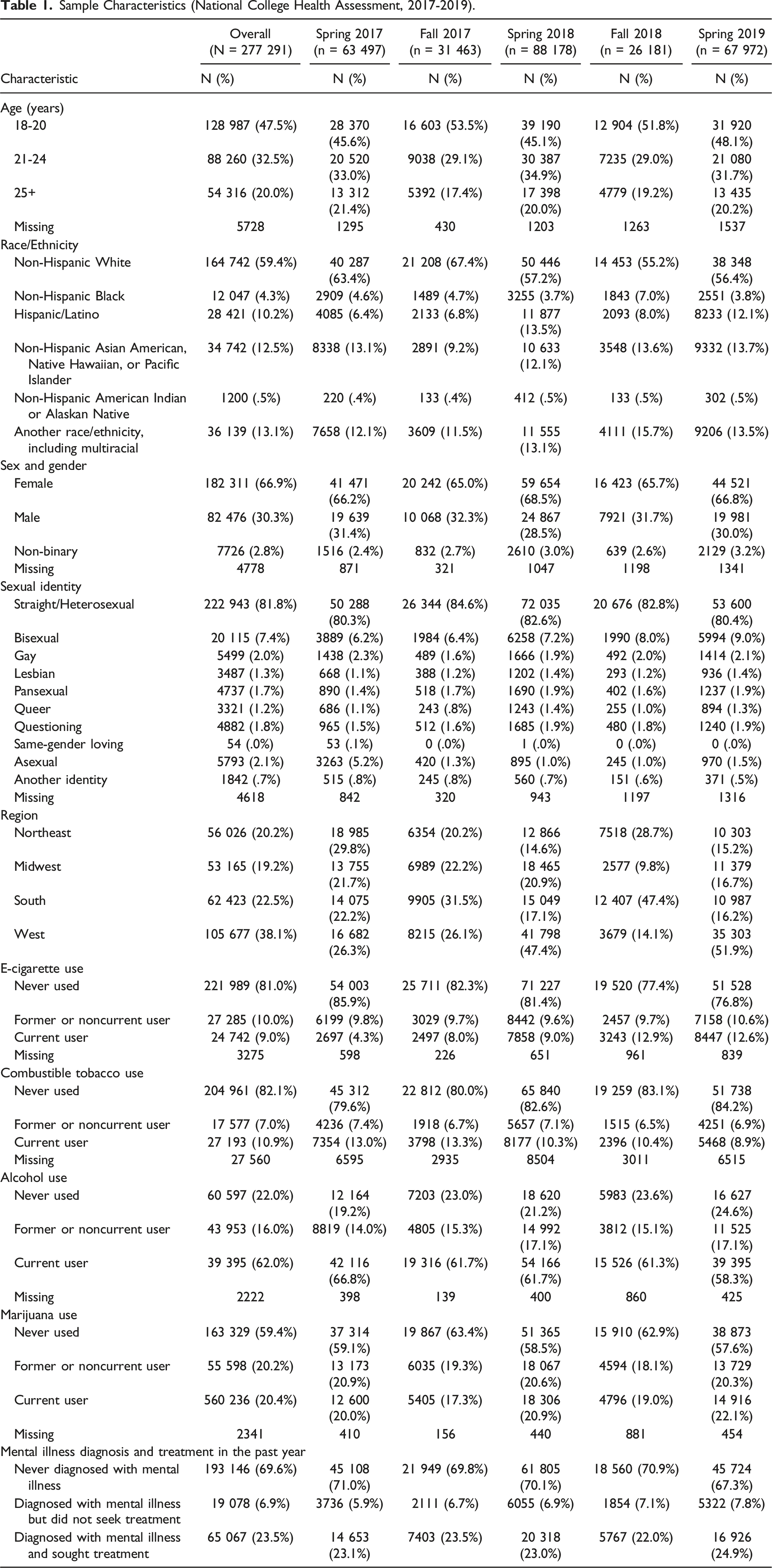
Figure 1 displays the proportions of respondents with or without MI diagnosis in the past 12 months reporting current e-cigarette use from Spring 2017 to Spring 2019. Greater proportions of respondents with any MI diagnosis reported current e-cigarette use, relative to those without any MI diagnosis. The largest difference in proportions was observed in Fall 2018, with 17.2% of respondents with any MI diagnosis and 11.0% of respondents without any MI diagnosis indicating current e-cigarette use. Current E-cigarette use by past-year mental illness diagnosis (National college health assessment, 2017-2019). Note. MI = mental illness.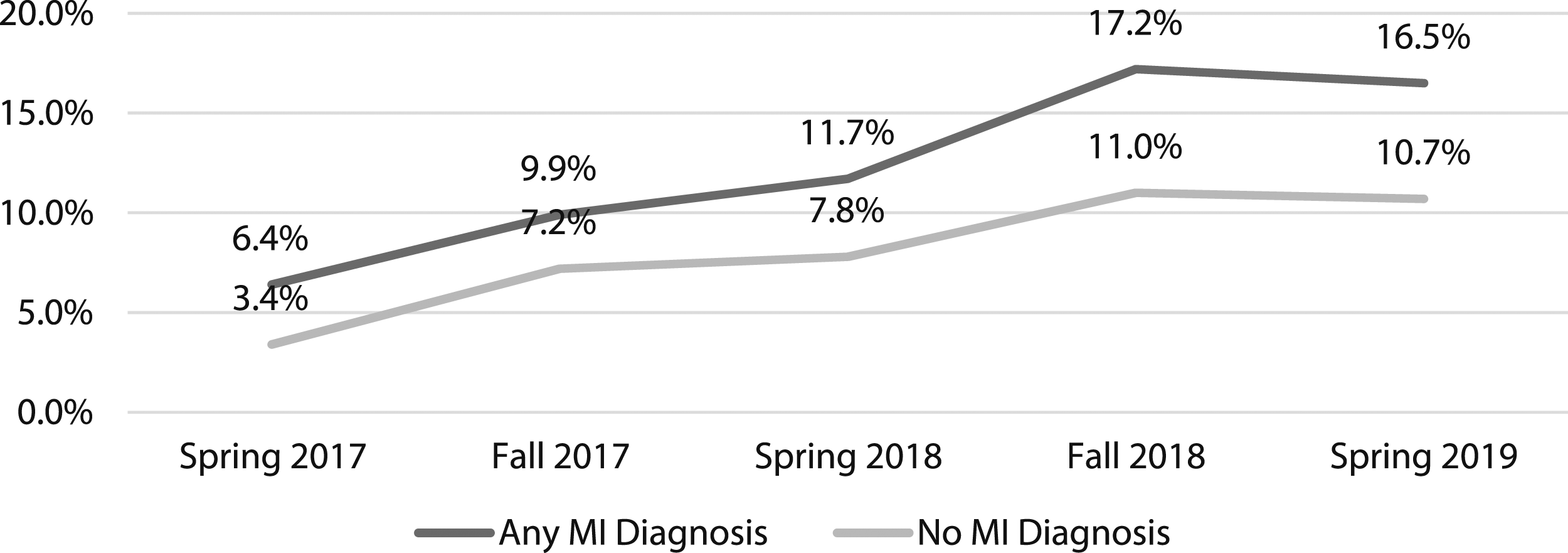
Relative Risk Ratio Estimate Comparisons Between Never, Former/Noncurrent, and Current E-cigarette Users.
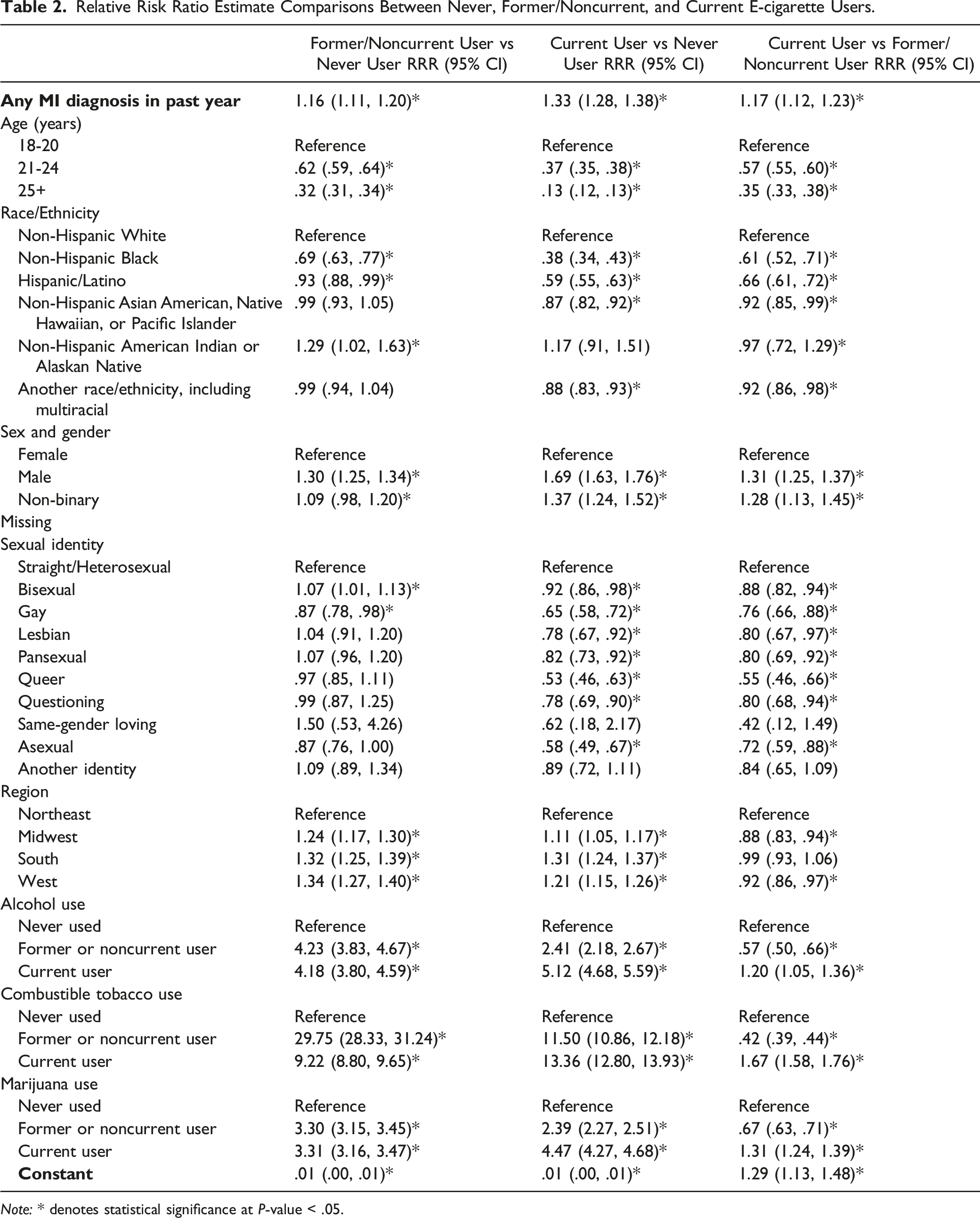
Note: * denotes statistical significance at P-value < .05.
Model Results for Past-Year Mental Illness Diagnoses Predicting E-cigarette Status, Adjusted for by Covariates.
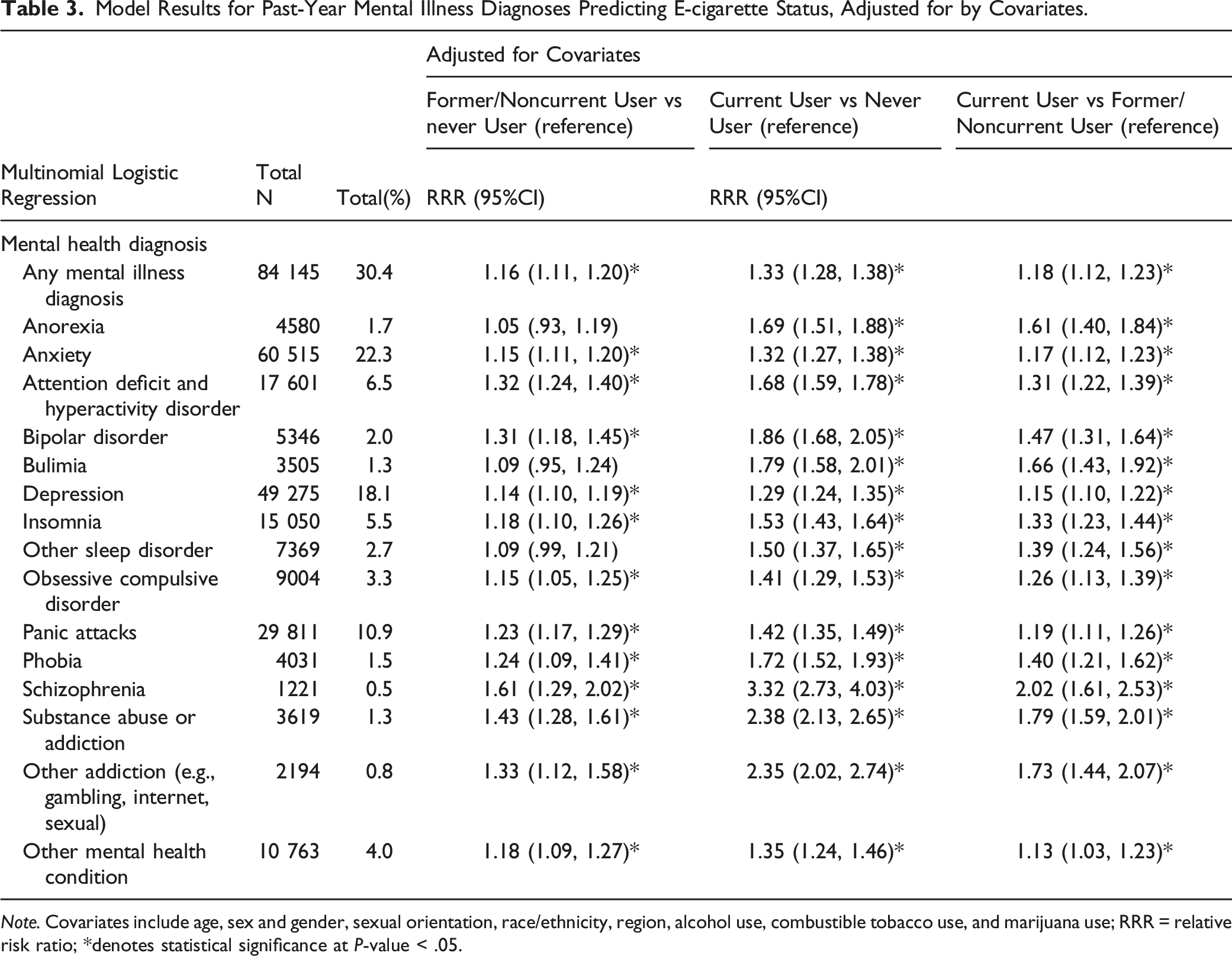
Note. Covariates include age, sex and gender, sexual orientation, race/ethnicity, region, alcohol use, combustible tobacco use, and marijuana use; RRR = relative risk ratio; *denotes statistical significance at P-value < .05.
Discussion
This study sought to expand upon the current literature by examining e-cigarette use status across MI diagnoses. The most prevalent past-year MI diagnoses among this sample were anxiety, depression, and panic attacks – which may be unsurprising, given that the sample is drawn from college/university students. Overall, respondents with any MI diagnosis were more likely to be current or noncurrent e-cigarette users than those without – a finding supported by the existing literature.11,12,19,34 Although all MI diagnoses included in the study were associated with a greater likelihood of e-cigarette use, respondents reporting past-year diagnosis of substance abuse or addiction, bipolar disorder, or ADHD were most likely to be former/noncurrent or current e-cigarette users, relative to those who had not reported past-year diagnoses.
Findings are supported by evidence that e-cigarette use prevalence varies across MI diagnostic group. 35 In general, substance use disorders occur at high prevalence with mental disorders, such as depression, bipolar disorder, and ADHD. Furthermore, substance use is highly prevalent among youth and young adults who use e-cigarettes. 36 Schizophrenia, substance use or addiction, and other addiction were the strongest predictors of former and current e-cigarette use, compared to all other MI diagnostic groups in the current study. Bipolar disorder, bulimia, and ADHD were the next strongest predictors; though, evidence from prior studies are limited and mixed.18,30,37 More research is needed to understand how specific psychiatric symptoms, symptom severity, and level of disability are related to e-cigarette use, as other studies have determined that increased frequency of e-cigarette use was associated with higher depressive symptoms.27,29
Additionally, increased relative risk estimates were found among current e-cigarette users, relative to former/noncurrent e-cigarette users. Although further study is needed to determine explanations for this finding, it may reflect individual decisions to start, continue, or stop e-cigarette use, in response to mental health challenges and symptomatology. Future research will also need to consider how sociodemographic factors, such as biological sex, race/ethnicity, sexual identity, age, and geographic region may moderate associations between past-year MI diagnosis and e-cigarette use status.
There are a few limitations to this study. First, MI diagnosis and e-cigarette use were based on self-report, which may be subject to social desirability bias. Second, this study utilizes data that is aggregated from cross-sectional surveys of college and university studies which may limit generalizability. Third, the large difference in the time frame between the main exposure (past-year MI diagnosis) and outcome (e-cigarette use status) may increase the likelihood of finding spurious correlations. Longitudinal studies are needed to validate these findings and confirm the directionality of effects. To date, there are only a handful of longitudinal studies examining MI and substance use, with overall findings suggesting that MI predicts substance use.38,39 Additional longitudinal research is needed to determine how e-cigarette consumption may influence symptom severity and level of disability over time. This information could help researchers and health professionals better understand and treat young people who either have been diagnosed with MI or reported current use of e-cigarettes. Future studies should also investigate how individuals receiving treatment for MI diagnoses might differ in e-cigarette use from those who are diagnosed with a MI but not yet receiving treatment.
Conclusion
Past-year diagnosis of any MI was associated with e-cigarette use status. Results have the potential to inform intervention efforts, as it suggest that efforts to improve mental health among young people could help to curb e-cigarette use. Future research is needed to further elucidate explanatory mechanisms for the association between MI and e-cigarette use across young people, to advance this growing area of research.
• Young adults who use e-cigarettes are more likely to report symptoms of depression and anxiety. • Few studies examine associations between e-cigarette use and symptoms of MI beyond depression and anxiety.
• Past-year diagnosis of schizophrenia, substance abuse or addiction, bipolar disorder, bulimia, or ADHD were most likely to be former/noncurrent or current e-cigarette users, relative to those who had not reported past-year diagnoses.
• More research is needed to understand how specific symptoms of MI are related to e-cigarette use. • This information can help researchers and health professionals better understand and treat young people who have been diagnosed with MI or reported current e-cigarette use.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Acknowledgments
The authors of this study would like to thank the participants of the American College Health Association’s National College Health Assessment Surveys for contributing their data to this work.
Author Contribution
EKD: conceptualization, methodology, analysis, writing – original draft, writing – review and editing; KA: writing – original draft; writing – review and editing; GP: writing – original draft; writing – review and editing; ECH: conceptualization, methodology, analysis, writing – original draft; writing – review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
Permissions for conducting the research at each study site is granted by individual university institutional review boards. Consent from students is implied by their participation in the survey, as they are given the right to refuse to participate. This secondary analysis was approved as exempt from full review by Advarra Institutional Review Board.
Data Availability Statement
The data that support the findings of this study are available from the National College Health Assessment (NCHA), which is sponsored and distributed by the American College Health Association (ACHA) ![]() . Restrictions apply to the availability of these data, which were used under license for this study.
. Restrictions apply to the availability of these data, which were used under license for this study.