
Abstract
Background:
Kramer et al’s PROBIT (Promotion of Breastfeeding Intervention Trial) research in Belarus studied effects of the Baby-Friendly Hospital Initiative (BFHI) training on breastfeeding duration, exclusivity, and health outcomes.
Aims:
To critique inclusion criteria, context, approaches to data analysis, and health outcome results.
Method:
Twenty-two articles were retrieved from PubMed and the PROBIT Website for 2001-2010; 6 were excluded as not focusing on breastfeeding and health outcomes.
Results:
PROBIT data from the cluster randomized hospital comparisons included only breastfed babies since all non-breastfed babies were excluded from the research. Context may affect outcomes, knowing that Belarus has good basic health services, 3-year maternity leaves with little use of daycare, 95% breastfeeding initiation rate, and a well-educated population. PROBIT data were analyzed in 2 ways: (a) intent-to-treat analyses of breastfeeding and health differences by cluster randomized intervention and control site mother/baby pairs; and (b) as an observational cohort study of health outcomes for all mother/baby pairs, analyzed by various breastfeeding categorizations and controlling for biases. PROBIT demonstrated links between BFHI and longer breastfeeding duration (19.7% vs 11.4% at 12 months, P < .001) and exclusivity (43.3% vs 6.4% at 3 months, P < .001), reductions in gastrointestinal episodes and rashes, higher verbal IQ scores, and longer exclusive breastfeeding rates for subsequent children but no statistically significant differences in the child’s body mass index, blood pressure, or dental health.
Conclusion:
PROBIT provides foundational evidence for BFHI policy and follow-up care. Knowing that non-breastfed babies were excluded, caution must be exercised for health comparisons.
Keywords
Background
When Dr Michael Kramer and his team of scientists first published the PROBIT (Promotion of Breastfeeding Intervention Trial) research findings from the Republic of Belarus, 1 breastfeeding researchers and clinicians alike realized the importance of this. The randomized design was the gold standard of research in terms of looking at the efficacy of the Baby-Friendly Hospital Initiative (BFHI) and its effects on duration and exclusivity of breastfeeding. It was the necessary “proof” in terms of epidemiological rigor. The purpose of this review is to examine the research design, the context of Belarus, various approaches to analyses, and the health outcome results of the PROBIT studies. A review of the original research design and the various ways in which the data were analyzed may help the reader to understand the context and the findings of these studies and be aware of both the strengths and limitations of the results related to health outcomes.
Methods
All published articles for PROBIT studies were retrieved for years 2001 to 2010, using a search of the PROBIT Website listing at the University of Bristol, UK: http://www.epi.bris.ac.uk/probit3/PROBIT%20III%20Publications.htm.
In total, 22 publications were found. This was supplemented through a PubMed search of the lead investigator’s name and the study name (Kramer MS AND PROBIT), where the 10 articles identified were duplicated in the first search. All articles were read in their entirety, and 15 were related to the relationships of BFHI site allocation, or breastfeeding exclusivity/duration, with subsequent health outcomes. One of the 7 excluded articles was referenced in this publication for purposes of illustration.
Results: The Importance of Understanding the PROBIT Research Design and Setting
In the results sections of this article, aspects of the PROBIT research are described and discussed as to the implications these may have on understanding and critiquing the health outcomes results.
A Cluster Randomization Design
It is seldom possible in the realm of breastfeeding research to do a randomized controlled trial since babies could never be ethically randomly assigned to be or not be breastfed. However, in the case of the original PROBIT research trial, 1 BFHI policy itself was randomly assigned through “cluster” randomization (ie, an entire hospital site and its associated polyclinic was exposed to either receiving or not receiving the intervention). These clusters were matched prior to randomization by geography, urban/rural status, number of births, and breastfeeding initiation rates (within 5%). The intervention consisted of the 18-hour BFHI lactation management training course for the leaders (organized by the European Regional Office of the World Health Organization), followed by 12 to 16 months of training for all midwives, nurses, and physicians providing care both within the hospitals and the polyclinics as well as ongoing monitoring of policies and procedures for BFHI compliance. 1 The polyclinic follow-up was designed to approximate the support group follow-up of the 10th step in the Ten Steps to Successful Breastfeeding, because no breastfeeding support groups existed in Belarus at that time. Following the PROBIT research, the control sites did receive BFHI training similar to the original intervention sites.
The Setting of Belarus
Understanding the context of Belarus is very important in understanding the study results. The authors state that this country’s maternity practices were similar to those in North America 20 to 30 years ago, which maximized the differences between intervention and control sites. As well, Belarus has good basic health services (with many maternity hospitals in both rural and urban settings) and good public health services, including clean water monitoring. Kramer et al 1 state that the norm in Belarus was prolonged (3 years) maternity leave, with very little use of daycare centers for infants. In addition, 67.5% of the intervention group mothers and 60.1% of the control group mothers had advanced education beyond high school completion. Cesarean section rates were low (12.6%, intervention; 10.5%, control groups), as were smoking rates during pregnancy (2.8%, intervention; 1.8%, control), but 3-month Belarus breastfeeding discontinuation rates were 50%.
The authors also remark on the highly centralized system that helped implement the BFHI intervention in a very brief period. This may differ from the experience of a less centralized system, where resistance to maternity hospital policy change may delay the adoption of the policies and practices.1,2 Discharge practices from maternity hospitals may also affect the generalizability of these results—6 to 7 day stays were common, in contrast to much shorter stays being the norm in most industrialized countries. Finally, the breastfeeding initiation rate in Belarus, even before the PROBIT research, was at least 95%. 2
Inclusion Criteria, Study Size, and Follow-Up
Although the original intent of the research was to include women who intended to breastfeed, the original protocol was slightly altered so that women were actually enrolled in the postpartum ward (clarified in correspondence with Dr. Michael Kramer (August, 2011). So the women eligible for the research were those who initiated breastfeeding after birth and were healthy, along with their healthy newborn, who was of at least 37 weeks’ gestation, was at least 2500 g, and had an Apgar score of at least 5 at 5 minutes. Moreover, because of necessary efficiencies of doing the research, enrollment of mothers was limited to those who were going to be followed up at one chosen specific polyclinic associated with each hospital (therefore not all mothers were followed from each hospital). Although other publications have measured the impact of BFHI on initiation, 3 Kramer’s research did not set out to examine the relationship between BFHI and breastfeeding initiation but rather the effect of BFHI on breastfeeding duration and exclusivity once breastfeeding was initiated.
PROBIT had a large number of enrolled participants, with 17 046 mother-infant pairs enrolled at 16 intervention and 15 control sites—1 site was excluded due to falsification of data at the polyclinic. 1 Very few mothers (around 3%) were lost to follow-up at a year, and the researchers validated the information by doing both chart reviews and maternal interviews. The analyses reported in all publications are adjusted for the effect of clustering, that is, for people being within the same hospital setting. The authors did further statistical analyses for some of the health outcomes by including known confounders such as previous breastfeeding history of the mother, family size, type of delivery, infant demographics, maternal smoking, and family history of disease.
Results: The Breastfeeding and Health Benefits of PROBIT
Effect on Breastfeeding Duration and Exclusivity
In the PROBIT research, 100% of mothers in both the intervention and control site samples initiated breastfeeding. The results of the BFHI intervention on breastfeeding duration rates do show statistically significant differences (Table 1)—at 6 months, 49.8% of the intervention group mothers and 36.1% of the control group mothers were still breastfeeding (adjusted odds ratio [aOR] = 0.52; 95% confidence interval [CI], 0.39-0.71 for weaning); at 12 months, the difference was 19.7% versus 11.4% (aOR = 0.47; 95% CI, 0.32-0.69 for weaning). 1 The largest effect was seen on exclusivity of breastfeeding—at 3 months, 43.3% of the intervention mothers compared with only 6.4% of control mothers (P < .001) were exclusively breastfeeding; at 6 months, the difference was 10.6% versus 1.6% (P = .003). In the long-term follow-up data collection of the mothers who were in the original study, the researchers also examined the breastfeeding patterns for subsequent children. The mothers who were in the original BFHI sites experienced longer breastfeeding and exclusive breastfeeding duration of their subsequent child compared with mothers in the original control sites 4 (Table 1).
Selected Health Outcomes From the PROBIT (Promotion of Breastfeeding Intervention Trial) Research, Comparing Cluster Randomization Intervention with Control Group Children
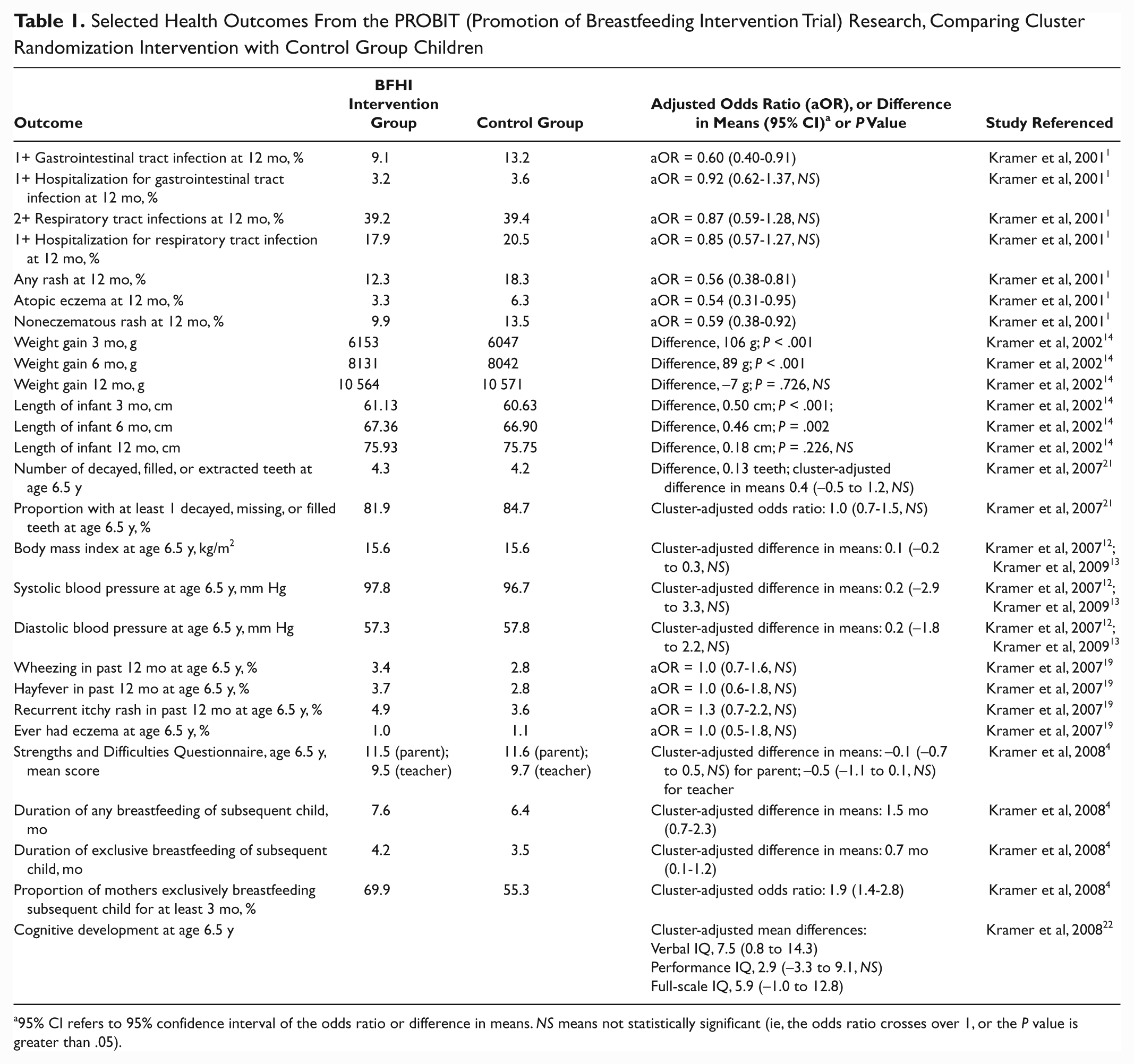
95% CI refers to 95% confidence interval of the odds ratio or difference in means. NS means not statistically significant (ie, the odds ratio crosses over 1, or the P value is greater than .05).
Effect on Health Outcomes
Many publications have documented the health outcome results from the PROBIT research, including a recent summary article. 5 Table 1 summarizes key publication results comparing health outcomes for the intervention and control groups.
The BFHI intervention group represents a group that has slightly longer overall duration of breastfeeding but substantial increases in exclusivity of breastfeeding. The majority of women in both groups were still breastfeeding at 3 months (72.7% intervention, 60.0% control group—a difference of 12.7%). Absolute differences in duration rates were between 12% and 13% for most of the first year and down to 8% by the end of the first year. The large difference between groups was in the degree of exclusive breastfeeding, especially at 3 months (43.3% vs 6.4% at 3 months; 7.9% vs 0.6% at 6 months). For a breastfed baby born in a BFHI site, in contrast to a non-BFHI site, the health benefits included increased cognitive development and academic performance, reductions in gastrointestinal infections and rashes, and increases in weight and length (but the differences were no longer present at 12 months). However, long-term follow-up of the 2 groups showed no statistically significant differences in body mass index (BMI) and related obesity measures, blood pressure, dental health, or Strengths and Difficulties Scores at age 6.5 years (Table 1).
A cautionary note is appropriate when examining the effects of BFHI (and, indirectly, exclusivity of breastfeeding) on obesity. Patel et al 6 studied the relationship between socioeconomic position and adiposity based on the results of the PROBIT data collection. Using paternal education, maternal education, and highest household occupation as measures of socioeconomic status, all 3 measures demonstrated that the higher the socioeconomic status, the more likely that the child at age 6.5 years was in the 90th percentile or greater (even after adjusting for many other factors). This needs to be examined for its effects on any of the findings of the relationship between obesity and breastfeeding when basing results on the PROBIT studies since the relationship is exactly the inverse of what has been found in many other places, such as North America (ie, obesity is normally associated with the lower socioeconomic groups in North America). 7 Moreover, Belarus at the time of these studies had a much lower percentage of obesity in childhood than did North America, with BMIs at the 85th percentile or greater at 13% for Belarus and 33.6% for the United States (children 2-19 years old, 2003-2004). 8 Note also that Belarus has a very low degree of income inequality (Gini index 29.7), similar to Sweden (25.0), which is one of the lowest in the world, in contrast with the United States (Gini index 40.8), which has one of the highest inequality ratings. 9
Breastfeeding has been shown to influence the upper tail end of the BMI distribution, but this is difficult to detect if the analyses are limited to overall average BMI scores rather than percentages in the overweight or obese category.10,11 Kramer et al12,13 did analyze both the mean BMI score and the percentage in various upper tail categories and found no differences in mean BMI or on the tails (85th or 95th percentiles) by randomized grouping.
Observational Studies Nested within the Randomized Study
Although the data used in various publications were all derived from the original randomized PROBIT trial and follow-up data collection 6.5 years later, researchers have analyzed these data in 2 distinct ways. The first way was to use the data as originally collected, using the randomized allocation groups of BFHI sites versus non-BFHI sites to compare various health outcomes (including breastfeeding duration and exclusivity outcomes). For example, the study by Kramer et al, 14 which looked at infant growth patterns, did the comparison this way. The second way in which the data were analyzed was as one data set, taking all mother-child results no matter what the original allocation to intervention or control hospital and analyzing the whole cohort to see the effects of breastfeeding exclusivity or duration on the various health outcomes. This type of analysis treated all enrolled participants as if they were part of a large observational cohort study. The downside of an observational study is possible biases, since mothers who may choose to breastfeed exclusively may be different from those who do not in unmeasured ways that could also affect health outcomes. So the researchers who used the data in this way made a concerted effort to control for these potential biases as much as possible through multivariate analyses techniques. Table 2 summarizes the findings from the observational approach to the PROBIT data.
Using PROBIT (Promotion of Breastfeeding Intervention Trial) Enrollees as an Observational Cohort Study: Selected Health Outcomes a
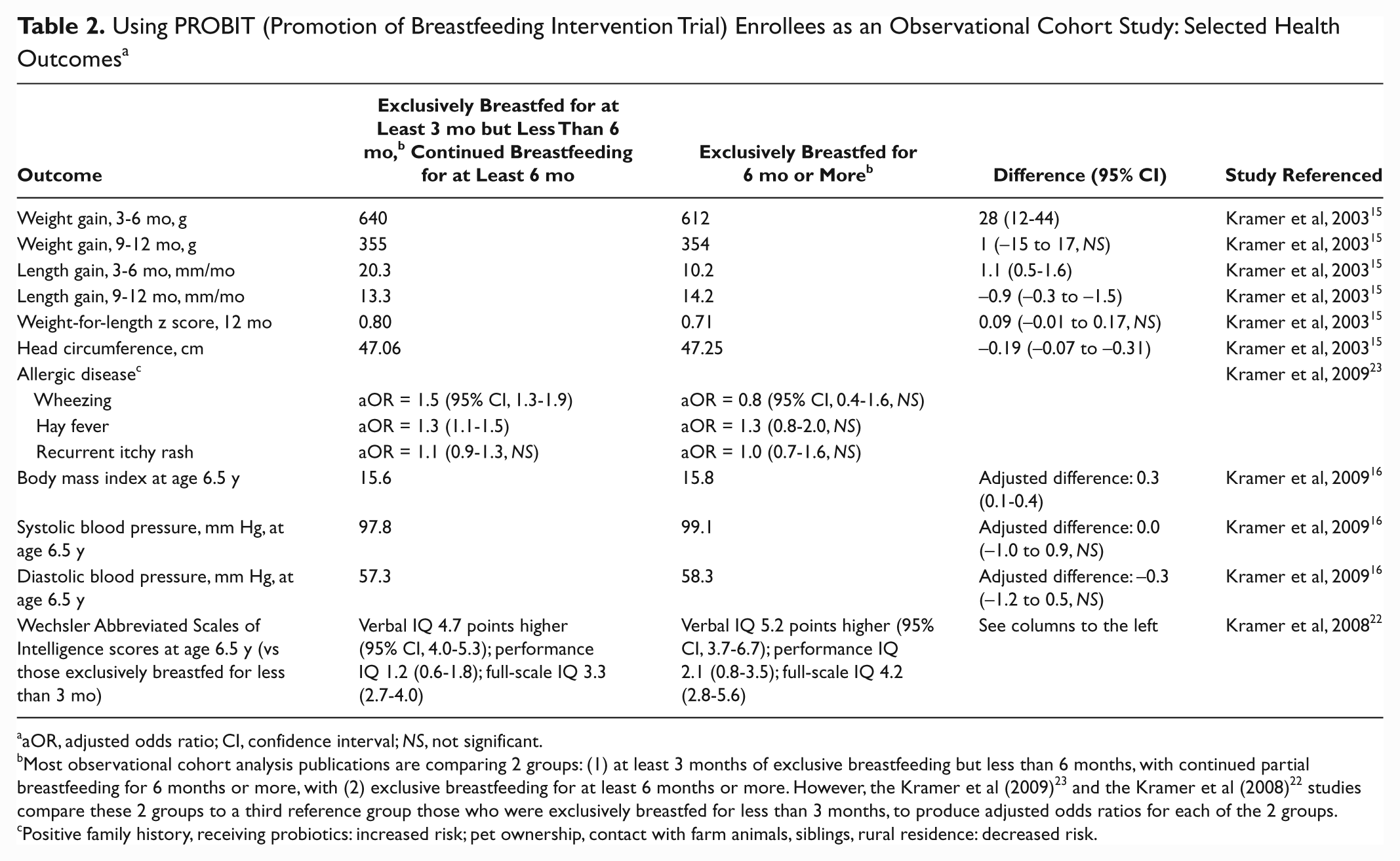
aOR, adjusted odds ratio; CI, confidence interval; NS, not significant.
Most observational cohort analysis publications are comparing 2 groups: (1) at least 3 months of exclusive breastfeeding but less than 6 months, with continued partial breastfeeding for 6 months or more, with (2) exclusive breastfeeding for at least 6 months or more. However, the Kramer et al (2009) 23 and the Kramer et al (2008) 22 studies compare these 2 groups to a third reference group those who were exclusively breastfed for less than 3 months, to produce adjusted odds ratios for each of the 2 groups.cPositive family history, receiving probiotics: increased risk; pet ownership, contact with farm animals, siblings, rural residence: decreased risk.
The 2003 publication by Kramer et al 15 is one example of using the PROBIT data as an observational cohort, analyzing by categories of exclusive breastfeeding, which did not follow the original randomized group assignment of the PROBIT research. The authors looked at infants who had been exclusively or partially breastfed for at least 6 months and chose 2 subgroups of infants to compare—2862 infants who were exclusively breastfed for at least 3 months but less than 6 months (often referred to in the various publications as the 3-month group) compared with 621 infants who were exclusively breastfed for at least 6 months (often referred to as the 6-month group). The definition was based on cross-sectional data at 1, 2, 3, and 6 months, with exclusive defined as no liquid or solid foods other than breast milk being administered to the infant. Note that the 3-month group could have been breastfed for almost 6 months since no cross-sectional observation was done between the 3-month and the 6-month interview. This could result in dilution of effect differences, because the group of exclusively breastfed for at least 3 months but less than 6 months could include babies who were exclusively breastfed for the majority of that time (even up to a few days before 6 months).
The observational cohort study analyses controlled for as many confounding effects as possible (geographic region, urban or rural, hospital of birth, maternal education, number of siblings, birth weight and length, and weight/length gain from birth to 3 months). These confounding effects would be expected to be randomly distributed in a randomized study (the original design), but in dealing with the group as an observational cohort study, biases would need to be accounted for through statistical modeling.
Despite several limitations, the PROBIT analyses that used the observational cohort type of approach have contributed important findings to current debates. There was no difference in weight, length, weight-for-age, or length-for-age comparing the 3-month group with the 6-month group of exclusively breastfed infants. 15 There did appear to be a benefit of lower gastrointestinal infection rates for the 6-month group compared with the 3-month group, as well as a larger head circumference at 12 months for those exclusively breastfed for at least 6 months. 15 Hence, the PROBIT observational cohort contributed to the World Health Organization (WHO) revised infant feeding recommendations to encourage exclusive breastfeeding for the first 6 months of life (rather than former recommendations for only 4 months) and provided some evidence of protection for gastrointestinal infections.
In a 2009 article, 16 the data were again analyzed as an observational cohort study, once again comparing the 3-month and 6-month groups as previously described. Using measurements at 6.5 years, the researchers collected information on 53 different outcomes, including BMI, systolic and diastolic blood pressure, atopic symptoms, allergen skin-prick tests, and dental caries, and adjusted for the clustering of results within clinics where the children were measured. The only statistically significant differences were in BMI, triceps skinfold thickness, and hip circumference, all very slightly higher in the group exclusively breastfed for 6+ months. However, these were all done at the 95% confidence interval, with no adjustment for the number of tests done. If you assume the null hypothesis (ie, there will be no observed differences between breastfeeding groups), you could be making a type I error 5% of the time when you use P < .05 as your statistical cutoff (ie, finding a significant effect merely by chance, so making the conclusion of difference even though there was no real difference at the population level). So if you do 53 tests, you would assume that 2.7 findings (ie, 5% of 57), or somewhere around 3 results, would show up as statistically significant by chance alone. Interestingly, that is exactly what was found, with 3 outcomes showing slightly higher results. Therefore, caution should be exercised.
Many subsequent studies derived from PROBIT data have not focused on breastfeeding and its relationship to health but rather the interrelationship between diseases. For example, one study found that prior infection was not protective against subsequent atopic eczema or recurrent wheezing in the first year of life. 17 These types of publications were excluded in this review of PROBIT.
Implied vs Actual Comparison Groups for Health Outcomes of PROBIT
Discussions of the various health outcomes from the PROBIT studies have mistakenly interpreted the findings as the relative health benefits (or risks) of breastfeeding versus formula feeding, whereas the reality is a comparison of longer and more exclusive breastfeeding versus shorter and less exclusive breastfeeding. This is a critical distinction since even a short duration of breastfeeding could be protective against certain diseases or adverse outcomes, if compared with no breastfeeding at all. For example, the Pima studies on type 2 diabetes demonstrated that infants experiencing at least 2 months of total and partial breastfeeding had around half the risk of adult-onset type 2 diabetes when compared with infants who were not breastfed at all. 18
Kramer et al have worded their conclusions very carefully in their publications. For example, in the 2007 BMJ article, the section called “What This Study Adds” states that “prolonged and exclusive breast feeding had no protective effect on allergic symptoms and diagnoses or on positive skin prick tests” (emphasis added).19(p815) In contrast, however, was the reporting of this study in a national Canadian newspaper, The Globe and Mail. Helen Branswell’s article on September 13, 2007, was titled, “Breastfeeding Does Not Avert Allergies,” and the lead sentence was, “The first-ever randomized trial to look at the much debated question of whether breastfeeding protects an infant from developing asthma and allergies has found that breastfed babies are not at a lower risk of developing these conditions.” 20 The media often recognize that breastfeeding is the topic area of the PROBIT studies but miss the fact that no non-breastfed babies were enrolled in the research.
Discussion
The PROBIT analyses have taken 2 approaches—that of analyzing the results by the randomly assigned birth hospital (BFHI vs not) on health outcomes and that of analyzing the entire sample of mothers/children as a prospective study to look at effects of duration and exclusivity of breastfeeding on health outcomes. The analyses by randomized site investigated the effects of the BFHI intervention on the health outcomes, with the assumption that this intervention was in turn associated with higher exclusive breastfeeding rates and hence possible health outcome differences due to this. Knowing the ethical impossibility of actually randomizing children to various categories of feeding (exclusive or not), the researchers derived an indirect way of measuring health benefits or risks. But this analysis does not directly measure the effects of duration or exclusivity of breastfeeding on health outcomes and certainly does not answer the question of breastfeeding versus no breastfeeding, given the fact that only children initiating breastfeeding were enrolled in the study.
This review article is not comparing the randomized analyses to the observational cohort analyses. A direct comparison of findings from analysis of the randomization trial versus an observational cohort approach is almost meaningless, given the fact that the randomization itself was not a random assignment by breastfeeding category but rather a randomization to a particular BFHI policy and protocol. So any health benefits of infants being born in a BFHI hospital site may be indirectly related to the fact that these infants were more likely to be exclusively breastfed or breastfed slightly longer overall. This is very different than analyzing the data by actual breastfeeding categories, as was done in the observational cohort analyses. Given that proviso, it is interesting to note that many of the health outcomes’ results are similar in the 2 types of analyses, comparing Tables 1 and 2. For example, the cognitive development scores indicate that the BFHI intervention site children had higher verbal IQ and higher, but not statistically significant, full-scale IQ scores compared with the non-BFHI control sites. A cohort analysis by duration of exclusive breastfeeding showed that the longer the exclusive breastfeeding, the higher the verbal and the full-scale IQ scores. There was no difference in allergic reactions such as wheezing, hay fever, rashes, and eczema between the BFHI intervention and control groups at age 6.5 years, similar to the cohort finding that exclusive breastfeeding for at least 6 months was not associated with any differences in allergic reactions compared with a reference group of babies exclusively breastfed for less than 3 months.
Given the extensive nature of the PROBIT trial and the many publications that have resulted and will continue to result from this program of research, it is extremely important that certain aspects of the research are well understood. In the original cluster randomized research to measure the efficacy of BFHI policy, it is important to note that the PROBIT research also included training and monitoring of an associated polyclinic for follow-up postnatal care and not just the hospital intervention. Thus, any institution that expects to see similar effects on duration and exclusivity of breastfeeding following implementation of BFHI will require the additional effort be placed into follow-up care by trained and knowledgeable health care providers.
When discussing any health outcome of the PROBIT studies, it is critical to understand that the research only included women who initiated breastfeeding after giving birth and excluded all non-breastfed infants. Given this exclusion, it is important to take into account the fact that the health effects in the PROBIT research are referring to the effects of slightly longer duration of breastfeeding, as well as much higher exclusive breastfeeding, but not comparing any breastfeeding to totally non-breastfed infants. Secondary reporting of results, such as media articles, often implies that the comparison of health outcomes is for breastfed versus non-breastfed infants. A careful read of the original publication will be necessary to check on which comparison groups were used and thus what interpretation should be placed on the findings.
Finally, the context of the PROBIT studies also needs careful consideration when evaluating the health benefits (or the findings of “no health benefits”). In Belarus, mothers were at home with their children for an average of 3 years, with little use of daycare. This may have an influence on the rates of certain communicable disease transmission, such as respiratory infections, possibly lowering rates in all children to the point where it may be difficult to assess the effect of breastfeeding duration or exclusivity on these infections.
Conclusion
The PROBIT publications are critical, in terms of both the effects of BFHI policy and health outcomes. However, an understanding of who was enrolled, the context of Belarus, and the type of analysis that was done is required. Careful interpretation is particularly essential when reading the PROBIT studies, knowing that non-breastfed babies were excluded from the research.
Despite these cautionary notes, the PROBIT randomized study results have pointed out causal links between BFHI and health benefits of babies who were breastfed initially, including longer duration and more exclusive breastfeeding, reductions in gastrointestinal episodes and rashes, higher verbal IQ scores, and a greater probability that the mother’s subsequent children had a longer duration of exclusive breastfeeding. And thanks to Kramer and his PROBIT research team, we have a solid foundation of evidence in which to institute BFHI policy and follow-up care.
Footnotes
Acknowledgements
Dr. Martens acknowledges support of the Canadian Institutes of Health Research (CIHR) and the Public Health Agency of Canada (PHAC) for her CIHR/PHAC Applied Public Health Chair. Thanks to Jessica Jarmasz, research assistant at the Manitoba Centre for Health Policy, for helping with document searches.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received financial support through her CIHR/PHAC Applied Public Health Chair funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.