
Abstract
Background:
Strategies that promote higher exclusive breastfeeding rate and duration are highly recommended. To date, no study has tested the feasibility of Web-based monitoring among breastfeeding mothers.
Goals:
To develop an interactive Web-based breastfeeding monitoring system (LACTOR) and examine its feasibility, usability, and acceptability among breastfeeding mothers.
Methods:
A prospective, descriptive, mixed-methods study was conducted. Mothers who met the study inclusion criteria were recruited from mother infant units in 2 Midwestern hospitals in the United States. Mothers were asked to enter their breastfeeding data daily through the system for 30 days and then submit an online exit survey. This survey consisted of a system usability scale and mothers’ perceptions form. Twenty-six mother/infant dyads completed the study.
Results:
The Feasibility of LACTOR was established by mothers’ compliance in entering their breastfeeding data. The mean was 8.87 (SD = 1.21) daily entries, and the range was 6-13 times per day. Usability scale total mean score was 3.35 (SD = 0.33; scale range 0-4). Ninety-two percent of the mothers thought that they did not need to learn many skills before they started to use LACTOR and did not need any technical support. Mothers reported that the monitoring was beneficial and gave them the chance to track their infants’ feeding patterns and detect any problems early.
Conclusions:
This study demonstrated the feasibility of LACTOR, and it was user-friendly and acceptable among mothers. Further studies to test its effect on breastfeeding outcomes are needed.
Well Established
Although previous studies have shown that post-discharge lactation support and follow-up such as home visits, education, and telephone calls improve breastfeeding outcomes, those interventions did not provide continuous monitoring, which is necessary for early detection and resolution of breastfeeding problems immediately after hospital discharge.
Newly Expressed
In this study, Web-based breastfeeding monitoring proved to be feasible, usable, and user friendly, with features that help mothers navigate and recognize breastfeeding problems. Mothers expressed the usefulness of the system in recognizing infant feeding patterns and appreciated the interactive features.
Background
Several evidence-based systematic reviews and meta-analyses have confirmed the long-term positive effects of breastfeeding for mother and baby. Breastfeeding provides protection against obesity and type 2 diabetes1-5 and promotes the infant’s cognitive development.6,7 According to the Institute of Medicine, encouraging and promoting breastfeeding is a critical step in preventing childhood obesity.8,9 The surgeon general has called for action to promote, support, and encourage breastfeeding with more postpartum and post-hospital discharge interventions to improve the rate and duration of exclusive breastfeeding. 10
Postpartum interventions that promote breastfeeding have been found effective in improving breastfeeding exclusivity and duration.11-13 One of these interventions is a paper-and-pencil breastfeeding journal, which has increased mothers’ breastfeeding self-regulation and the duration and exclusivity of breastfeeding. 14 Currently, we are witnessing an increase in the use of online diaries and Web-based monitoring in clinical practice. Studies have examined their effectiveness in chronic diseases such as asthma, diabetes, and migraine headache and found them feasible and effective.15,16 Electronic diaries have also been associated with higher rates of compliance with medication among children, and they have been found to provide more accurate recordings than the traditional paper-and-pencil diary. 17 Furthermore, electronic diaries have been associated with greater compliance rates and effectiveness in pain management among adults with chronic pain. 18 Internet-based interventions that facilitate monitoring and behavioral coaching among patients with chronic illness are becoming common and are improving knowledge and changing behavior. 19 Web-based interventions also improve patient-provider communication and adherence among patients with chronic illnesses through promoting self-awareness and self-regulation.20,21 Despite all these advantages, to date, online diaries have not been used to improve breastfeeding outcomes.
Interventions that lead to higher breastfeeding rates and longer duration of breastfeeding are needed nationally and internationally. Although studies have shown that post-discharge lactation support and follow-up such as home visits, education, and telephone calls improve breastfeeding outcomes,11,22 these interventions do not provide continuous monitoring, which is necessary for early detection and resolution of breastfeeding problems. This study therefore developed and tested the feasibility, usability, and acceptability of an interactive Web-based breastfeeding monitoring system.
Development of the Web-Based Breastfeeding Monitoring System
Our research team developed the breastfeeding monitoring system LACTOR based on a breastfeeding diary developed and tested by the main author, who is a lactation consultant. The system has 2 main components: (1) the Mothers’ Portal, where mothers enter their breastfeeding data and receive notifications (Figure 1); and (2) the Lactation Consultants’ Portal where the lactation consultant can monitor mothers’ data, send the system evaluation survey, and download the data into a spreadsheet for further analysis. Both portals are password protected. The system was developed to recognize patterns of mothers’ responses that indicate breastfeeding problems such as difficulty with latching, sleepy infants, jaundice, maternal breast engorgement, sore nipples, and inadequate breastfeeding entries. As soon as a breastfeeding problem is detected based on the rules that we have defined, LACTOR sends immediate feedback to the mothers along with suggestions for solving that problem; at the same time, the system alerts the lactation consultant.23
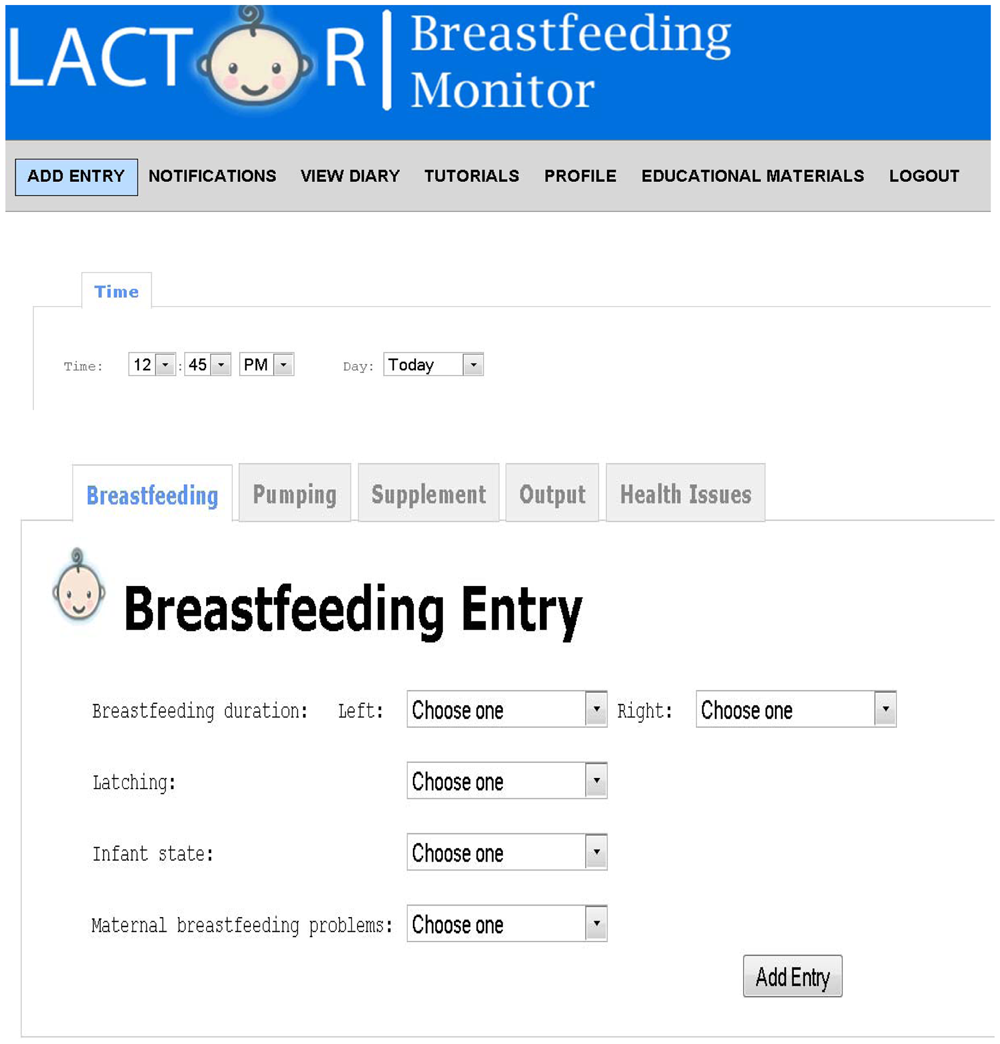
A screenshot of LACTOR breastfeeding data entry interface. The mother can enter her data by clicking the dropdown box.
Methods
Design
A prospective, descriptive, mixed-method study was conducted to test the feasibility, usability, and acceptability of LACTOR, which was developed by the authors and is accessible through http://www.lactor.org/.
Sample and Settings
A convenience sample of 50 mothers was invited to use the system before hospital discharge from mother/baby units in 2 Midwestern hospitals, St. Vincent Women’s Hospital in Indianapolis, Indiana and St. Elizabeth East Hospital in Lafayette, Indiana. Inclusion criteria for mothers included singleton birth, ability to read and speak English, age 18 years or above, willingness to continue breastfeeding after discharge, no problems that would interfere with breastfeeding, having basic knowledge of how to use the Internet, and access to electronic mail, phone, and Internet either through a standard PC or a smart phone. Mothers of infants who were born between 34 and 38 gestational weeks were included in the study. We should note that we initially targeted late preterm infants (34-36 weeks). However, we found out that early breastfeeding cessation rates were high, hence we included early term infants (37-38 weeks). Mothers were excluded if they had any condition that could significantly interfere with breastfeeding, such as a serious illness, an infant with a congenital anomaly, or an infant who was critically ill or stayed in the neonatal intensive care unit more than 1 week.
Process of Data Collection
The study was approved by the Institutional Review Boards of Purdue University, St. Vincent Women’s Hospital, and St. Elizabeth East Hospital. Eligible mothers were approached about the study by the lactation consultant immediately after birth. Once a mother agreed to participate in the study and agreed to be contacted, she signed the consent form. Then the lactation consultant or author invited her to access LACTOR. The mothers were given a folder that included a pamphlet with instructions on how to use LACTOR and educational materials explaining the terms used in the system such correct latching, infants’ states, and signs of correct latching along with the research team contacts. A welcome message from the research team was also sent by e-mail to welcome the mothers to the study. Mothers were encouraged to watch a video tutorial that explains how to enter data and use LACTOR. The tutorial was embedded in the system and was also available through YouTube for easier access. Mothers were asked to enter their daily breastfeeding data, infant output data, pumping data, and any health problem in the system. The 2 main authors trained the lactation consultants and research team to use LACTOR.
To ease the burden of data entry, we asked mothers to either write down their data and enter it at a convenient time or enter their data immediately after the breastfeeding sessions. Husbands, partners, or significant others were encouraged to help mothers with data entry. A mobile version of the system was also available for smart phones for mothers’ convenience. Seven mothers used the mobile version through their own smart phones. Trained research team members monitored the mothers’ data and contacted mothers by phone when data entry was missing for 24 hours or insufficient data were entered (< 6 infant feeding sessions /day). The research team members also monitored mothers’ notifications to make sure that the mothers read them. We asked the mothers to enter their data for 30 days, and then we issued an online system feedback survey through LACTOR. Mothers who completed the monitoring for 3 or more weeks were considered to have met the protocol criteria. When they completed data entry and submitted the online survey, mothers received a thank you letter with a compensation of $50 for mothers who completed 30 days and $30 for those who completed 3 weeks.
Instruments
Breastfeeding Diary
The breastfeeding diary was developed by the author to monitor breastfeeding progress. The diary includes times, frequency, and duration of breastfeeding sessions; number of dirty and wet diapers, with the color of the output; latching problems; supplementation types, amount, and method; pumping frequency and amount pumped; the infant’s alertness state; and maternal breastfeeding problems. Content validity was established by a panel of 2 lactation consultants, 2 maternal/child nurses, and 2 pediatric nurses. Face validity (whether the instrument “looks valid” to the examinees who take it) was tested through interviews with 5 lactating mothers. The diary was formatted for use on the Internet to collect daily breastfeeding progress post-discharge.
System Usability Scale (SUS)
The SUS was developed and used by computer science experts to evaluate usability of Web-based applications. We adapted it to LACTOR to evaluate its user-friendliness and mothers’ satisfaction. The scale was composed of 10 items that used a Likert response format on a 5-point scale. The scale includes 5 positive and 5 negative items. The negative items were reverse scored. Scores ranged from 0-4 points for each item, with 0 strongly disagree and 4 strongly agree. The SUS has been found valid and reliable with a Cronbach α of 0.91.24,25
Perception Survey
The survey included open-ended questions, such as: How did the system help you? Was the data entry time consuming, a burden for you, or overwhelming? Do you have any suggestions? How did the Web-based monitoring help in overcoming your baby’s health problems? How was your experience with this Web-based monitoring? Would you recommend this Web-based monitoring to a friend? Mothers submitted their responses though LACTOR in a narrative note after completing their data entry period.
Data Analysis
Quantitative Data:
We used descriptive statistics to examine the sample and analyze the feasibility and usability data. Means and standard deviations were calculated for continuous variables and frequencies and percentages for categorical variables. Fisher exact tests were used to assess differences between groups of mothers who completed the study and those who did not. Data were analyzed using SPSS (version 18). A 2-tailed level of significance at P < .05 was used for analysis of secondary outcomes such as differences between groups in mothers’ and infants’ demographics.
Qualitative Data:
Mothers’ responses to the Perception Survey were downloaded, and data were organized for each question. Using qualitative content analysis consisting of several stages, 26 as described by Granehem and Lundman, 27 the comments were read several times, and codes were identified to describe mothers’ experience with the Web-based monitoring and then combined to form categories and themes explaining similarities and variances in data. The main author, with help from undergraduate students and a qualitative data consultant, examined the data line by line to identify themes and patterns. The students downloaded the data from the Web site and classified mothers’ responses for each question, and then the main author and the consultant performed the content analysis.
Results
Participants
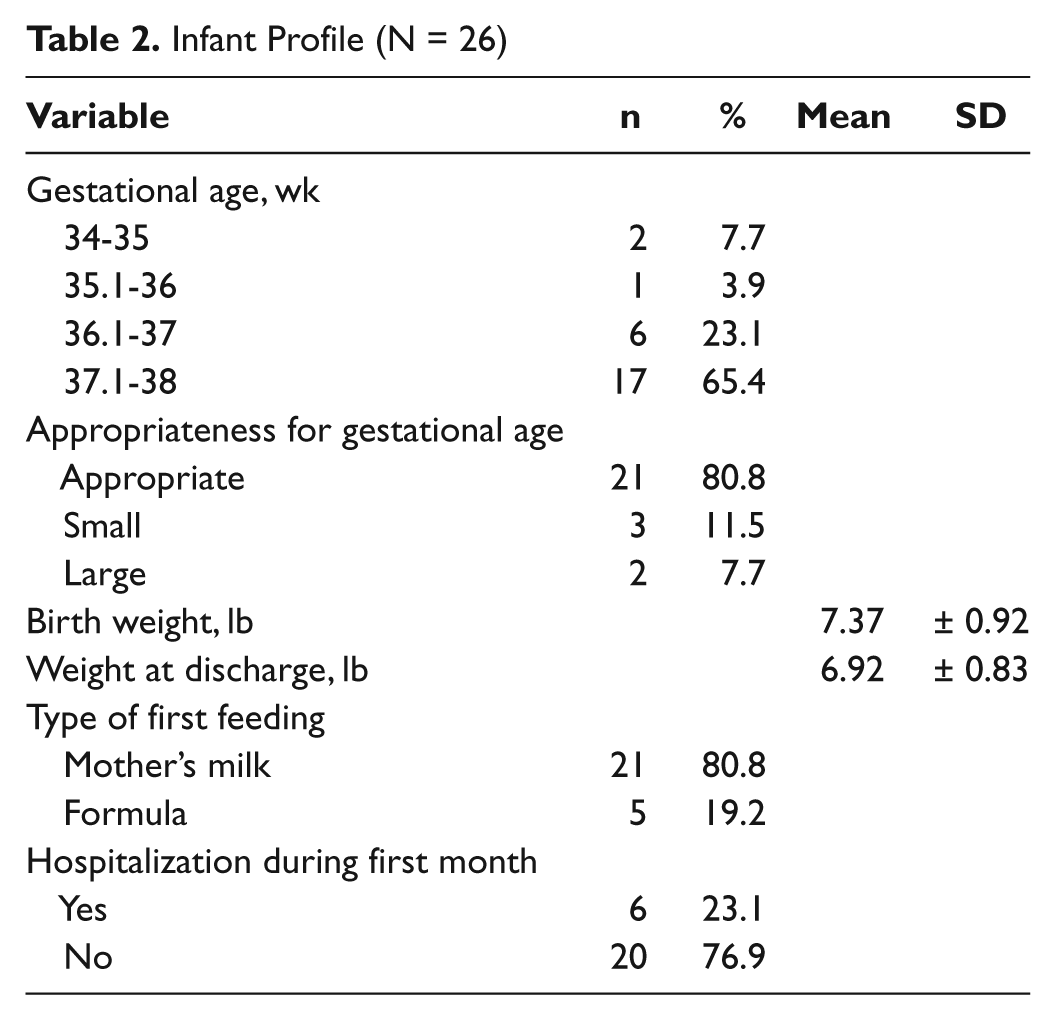
Mothers’ ages ranged from 20-39 years, with a mean of 29.88 (SD = 5.08). Most mothers were white (78.93%), which reflects the nature of the state population, and 50% worked as professionals. Table 1 describes more of the mothers’ demographics. The Fisher exact test revealed no significant differences between the mothers who completed the study and those who did not in age, education, race, household income, parity, and mode of delivery (Table 1). Mothers who completed the study had a significantly longer previous breastfeeding experience than those who did not ( p = .02). Infants’ gestational age ranged from 34-38 weeks, with a mean of 37.42 weeks (SD = 1.52). The majority of infants were appropriate for gestational age, with a mean birth weight of 7.37 lb (SD = 0.92) and a weight of 6.92 lb (SD = 0.83) at discharge (Table 2). Twenty-four mothers completed data entry for 1 month and 2 mothers completed entry for 3 weeks. One of them had stopped breastfeeding by the third week. Ten mothers accessed the system but did not complete the study for various reasons such as mother’s postpartum complications, infant hospitalization, visitors and family, and Internet problem (Figure 2). The attrition rate was 27.7% based on the mothers who accessed the system.
Demographics and Perinatal History for Mothers Who Completed and Did Not Complete the Study
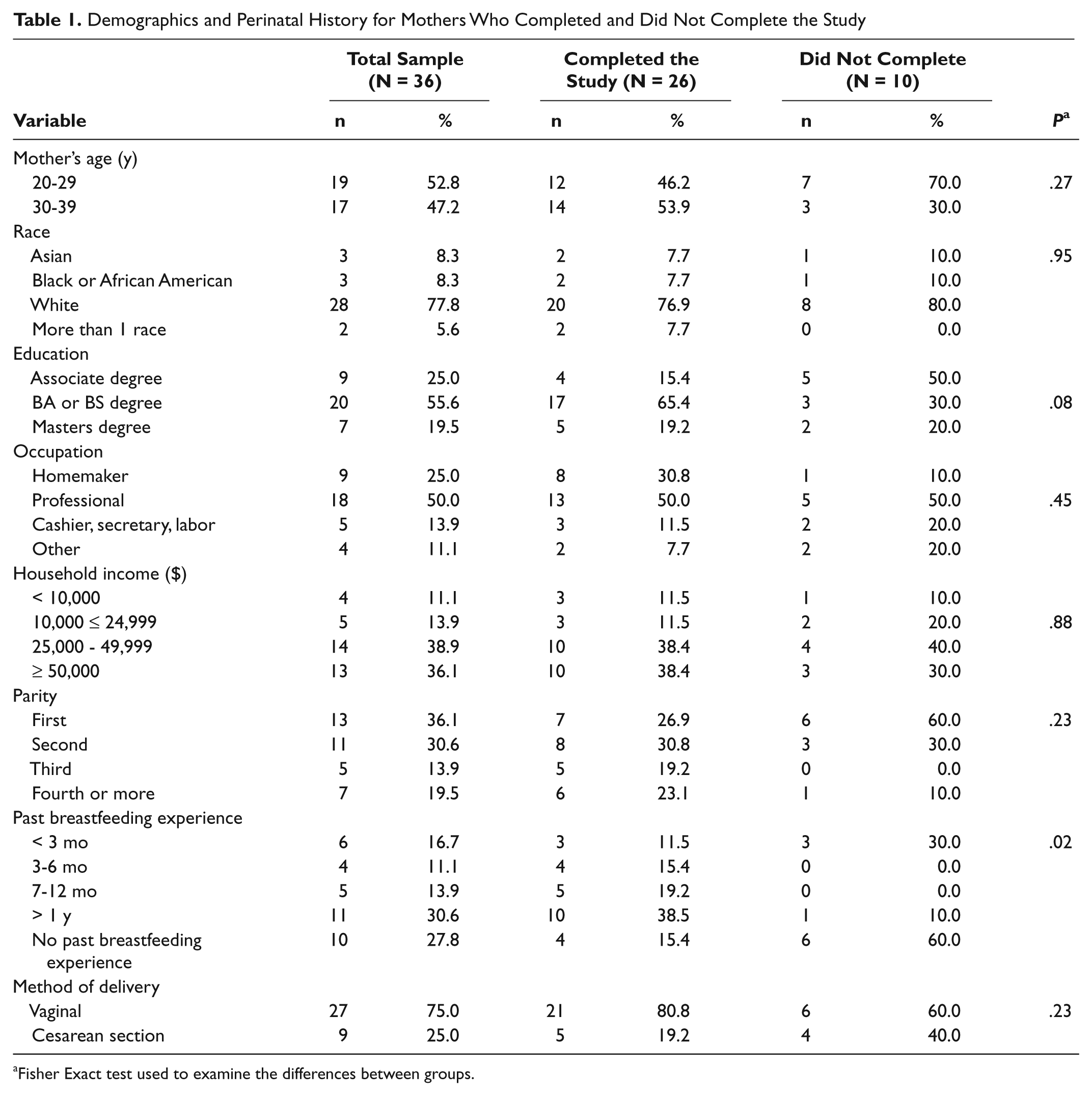
Fisher Exact test used to examine the differences between groups.
Infant Profile (N = 26)
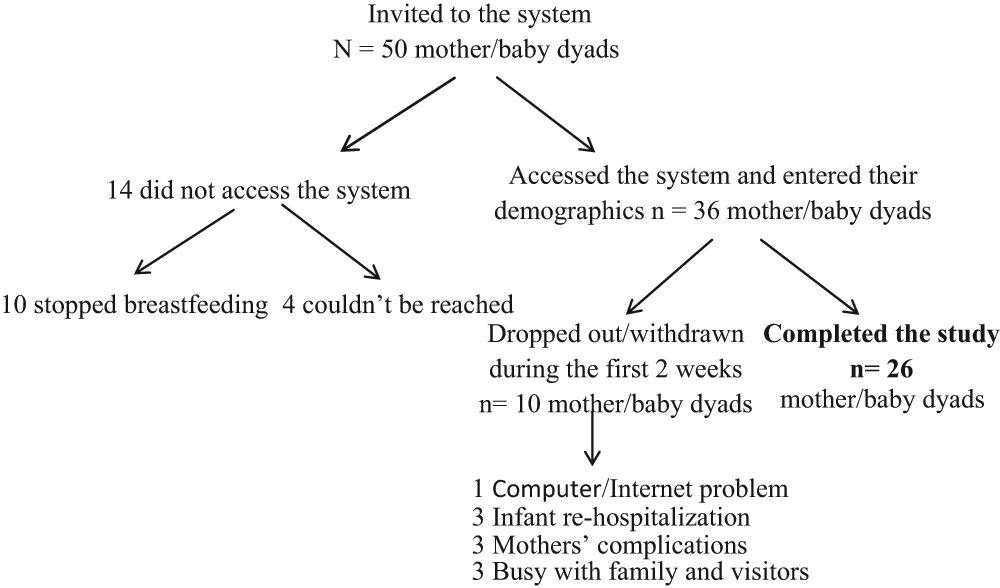
Recruitment and completion information
Feasibility
The feasibility of LACTOR was measured by number of mothers’ data entries per day, including breastfeeding entries and reading of notifications. The mean daily data feeding entries for the sample was 8.87 (SD = 1.21) entries per day, with a range of 6-13 times per day. More than 90% of the 26 mothers who completed the study read their notifications and entered their infants’ output data. Mothers were allowed to enter their infants’ data with each breastfeeding session or to give the total numbers of wet and dirty diapers per 24 hours. Three mothers missed 2 days of data entry because of traveling and computer problems.
Usability
The SUS measured the user friendliness of LACTOR. Scale response scores ranged from 0-4 points. The total mean score for the scale was 3.35 (SD = 0.33). Ninety-two percent of the mothers thought that they did not need to learn many skills before they started to use LACTOR (mean 3.68 [SD = 0.55]) and did not need any technical support to use LACTOR (mean 3.68 [SD = 0.55]). Eighty-five percent reported that the system was easy to use (mean 3.4 [SD = 0.70]) and that it was not complex (mean 3.4 [SD = 0.82]). No mother reported any difficulty in data entry or logistical access problem.
Acceptability
In general, mothers were very positive about the user friendliness of LACTOR and thought that it was easy to navigate. All of the mothers agreed on the usefulness of the monitoring and appreciated the interactive feature of the system and the notifications. More than 70% of the mothers reported that the data entry was not time consuming, and 77% reported that it was not a burden to complete. One mother said it was a burden when she started working outside the home. Another parent said that it was time consuming in the beginning, but the system got easier and faster when she became used to it. One mother said it became easier when she started to use the mobile phone version. Two mothers, however, expressed that it was a burden. Both had older children and suggested using the system until breastfeeding is well established: “It did become overwhelming because I have a 2-year-old, and with feeding and trying to take care of his needs, it was difficult to get to the computer to enter. I would suggest that this is a great tool until breastfeeding is established or problems are solved, but after that it might not be as useful.” Mothers reported that they enjoyed their experience with the system and described it as “very good,” “interesting,” “nice,” “great idea,” and “helpful.” However, the mothers said that the monitoring did not replace the face-to-face consultation with a lactation consultant. Based on the open-ended responses, the following themes were identified:
Recognizing infant feeding patterns and problems
Most of the mothers reported that the monitoring was very helpful in recognizing feeding patterns. A mother said, “It made me realize how often he was eating and that maybe he was getting enough.” Another mother said, “I felt it was helpful. It helped me to recognize his feeding pattern.” Mothers also reported that the monitoring helped them to identifying feeding problems. One said, “It helped me pay more attention when my baby was sleepy during breastfeeding. It also helped me track better how good or bad my baby was breastfeeding.”
Mothers also thought that the system helped them manage common breastfeeding issues. One mother said, “I was monitoring my baby’s feeding, which is something I would not have done. This monitoring allowed me to see that he ate more often in the mornings and evenings, and I was able to try for longer, fuller feedings at these times. Also, I had a problem with being engorged, which was in part due to only feeding my baby every 3-4 hours. I increased the feedings to every 2 hours and the problem went away.”
Mothers reported that the monitoring helped them prepare for their pediatrician visit. One reported that “I was able to look at the data from my diary entries and take any questions I had to my child’s pediatrician.” Another mother regrets not using the system from the beginning, during the first week after birth. This mother started data entry during the second week after her child’s re-hospitalization: “We had health problems very early on (hospitalization at day 5), so at that point I was not familiar enough with using the system and was so overwhelmed with my baby’s issues and being a new parent that I didn’t use the system for several days. Perhaps if I had been used to making entries sooner, it would have helped more.”
2. Usefulness of the notifications in minimizing and preventing problems
Most of the mothers noted the usefulness of the notifications. One said, “It helped me deal. I really liked that it had notifications with suggestions on how to fix the problem.” Another reported the benefits of waking a sleepy baby: “I also felt that the notifications were helpful and gave me good information to keep my child awake while feeding him.” Another mothers said, “It helped me when my baby was sleeping too much and didn’t wake up for feeding. The system alerted me, and I would wake him up every 3 hours.”
Mothers also thought that the suggested interventions helped them manage their breast problems. One mother said, “I had problems with sore nipples. With my last child, this lasted for a long time, but I was able to take care of it in a week by pumping. With my last child I was given the advice but I didn’t follow through as much, but seeing it constantly telling me to pump made me continue to do it.” Another one said, “It was nice to get some feedback on some potential problems he might be experiencing while breastfeeding and what I can do better to make feeding time easier and more efficient.” Mothers also mentioned that with the suggestions helped to prevent infants’ health problems: “It helped me identify the issues of sleepiness that my baby had during breastfeeding which could have resulted in health problems.”
3. Mobile version made data entry convenient
Several mothers got the chance to use the mobile version of LACTOR. All of the mothers reported that data entry was easier and more convenient than on the regular computer. One said, “I mostly did entries on my iPhone, and it was simple and quick to log entries. Little time required. I completed on the computer a couple times and found the Web site very user friendly.” Mothers also gave suggestions on how to improve the system: “The mobile LACTOR helped a lot. I would have liked to see the mobile LACTOR have a function that you can look at the diary or at least the last entered times.”
Most of the mothers said that the monitoring was beneficial and encouraged them to continue breastfeeding. One mother commented, “I think it does help with the overall process. You are tired and it does mean 1 more thing to do, but I think if you just take the 15 min 2x’s a day, it is easier and really helps if you are frustrated. I am actually still breastfeeding and since it went so well am going to try to continue through his first year.” Another said that, “Any caring mom will like this monitoring, because it is like a record for you that you can keep you and your baby’s performance saved, and return to it any time, and not just that, you will have solutions for many of the problems that you may not be aware of.”
One mother summarized the whole benefits of LACTOR: “It kept my baby on the right track, because by entering the data, the system told me if there was any problem and it would give me some solutions to do, and I tried these solutions, and guess what? It worked!!!!! Thanks to you!”
Discussion
This study evaluated LACTOR, an interactive, Web-based breastfeeding monitoring tool, and found LACTOR to be feasible, usable, and acceptable to the breastfeeding mothers who completed this study. Mothers showed high compliance rates in feeding data entry. More than 77% reported infant feedings ≥ 8 times per day. Mothers also read the notifications they received in case of breastfeeding problems and entered their babies’ output. Some mothers reported that the data entry was overwhelming if they had other children and when they went back to work. More than 70% of the mothers who accessed the system completed the study, with an attrition rate of only 27.7%. This attrition rate is normal for Web-based studies, and the reasons for mothers’ withdrawal from the study were acceptable and unrelated to the intervention (eg, infant re-hospitalization, mothers’ postpartum complications). 28
This was the first study to test the feasibility and usability of an interactive, Web-based breastfeeding monitoring system. The results of the study are consistent with other studies, which have found that mobile Web-based monitoring and coaching was feasible among patients with migraine headache, asthma, congestive heart disease, and diabetes.28-31 Although the situation of mothers who have just given birth differs from that of patients with chronic illnesses, and data entry could be overwhelming for mothers at this time, these mothers entered their data on a regular basis. In addition, fathers were encouraged to help with data entry and a mobile phone version was available for more flexibility.
Mothers’ responses to the usability scale indicated that the system was user friendly. The mean usability score was more than 83% of the total score (3.35 out of 4). The LACTOR system’s user friendliness was reflected in the ease of entering data and that there was no need to learn any new skills or obtain any technical help to use the system. Similarly, Tasi found that a mobile phone system of real-time monitoring of caloric balance was user friendly. 32 Nijland et al noted that innovation in health care will diffuse rapidly when technology is simple and has interactive components. 33 The LACTOR system has interactive features that help mothers recognize breastfeeding problems and offer some interventions to help with the problems. The LACTOR system is a promising method for assessing breastfeeding patterns and identifying breastfeeding problems early, while maintaining communication between mothers and lactation consultants. Breastfeeding mothers need motivation to continue breastfeeding. We posit that self-monitoring through LACTOR can help the mothers develop self-awareness and be motivated to continue breastfeeding through daily monitoring of their breastfeeding pattern and early identification of any problems. 14
The results of this study, however, must be considered in the context of its limitations, including the attrition rate and missing data. Fifty mothers were invited to use the system and signed consent forms; however, 14 mothers did not access the system. In the study protocol, mothers were to be asked to enter their demographic data online when they accessed LACTOR the first time. For this reason, we did not have demographic data on those mothers who never accessed the system. The second limitation is that although we recruited our sample from 2 hospitals that provide services for a diverse population, Hispanics were not represented in the sample, which may reflect that the system was developed in English and additional funds would be needed for a Spanish version. Also, mothers who completed the study were highly educated, and they came mostly from middle socioeconomic status, which is consistent with Pollard and reflective of breastfeeding mothers in the United States. 14 Heck et al found that women with high family incomes, high educational levels, and professional or executive occupations were more likely to breastfeed than their counterparts. 34 The findings also represent those who use the Internet for health purposes. 35 Thus, it appears that although this system has promise for implementation on a wide scale, less-educated mothers may be less likely to use the intervention, and strategies to promote the use of Web-based monitoring among less-educated mothers are needed.
Conclusion
In this study, LACTOR proved to be feasible, usable, and acceptable with features that help mothers navigate and recognize their breastfeeding problems. The mothers were able to enter their breastfeeding data and interact with LACTOR by reading notifications in case of breastfeeding problems. The researcher was able to monitor their data and make sure that the mothers read their notifications. Mothers also expressed their appreciation of the interactive features of LACTOR. Further studies are needed to identify the effect of LACTOR on duration and exclusivity as well as decreasing neonatal morbidities.
Footnotes
Acknowledgements
The authors would like to thank Elizabeth Moore, research scientist, and Vicki Wasy, research team at St. Vincent Women’s hospital, Indianapolis, Indiana and Glenda Clossin, Lactation Consultant at St. Elizabeth East Hospital, Lafayette, Indiana for helping in mothers recruitment and Karen Foli, PhD, RN, the Purdue University School of Nursing for qualitative analysis consultation. ![]() is hosted on hardware provided by the Cyber Center, Purdue University
is hosted on hardware provided by the Cyber Center, Purdue University
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this study was funded by a grant from the International Lactation Consultants Association (ILCA).