
Abstract
Background:
Changes in health care access and birthing practices may pose barriers to optimal breastfeeding in modernizing rural populations.
Objectives:
We evaluated temporal and maternal age-related trends in birth and breastfeeding in a modernizing Maya agriculturalist community. We tested 2 hypotheses: (1) home births would be associated with better breastfeeding outcomes than hospital births, and (2) vaginal births would be associated with better breastfeeding outcomes than cesarean births.
Methods:
We interviewed 58 Maya mothers (ages 21-85) regarding their births and breastfeeding practices. General linear models were used to evaluate trends in birthing practices and breastfeeding outcomes (timing of breastfeeding initiation, use of infant formula, age of introduction of complementary feeding, and breastfeeding duration). We then compared breastfeeding outcomes by location (home or hospital) and mode of birth (vaginal or cesarean).
Results:
Timing of breastfeeding initiation and the rate of formula feeding both increased significantly over time. Younger mothers introduced complementary foods earlier, breastfed for shorter durations, and formula fed more than older mothers. Vaginal hospital births were associated with earlier breastfeeding initiation and longer breastfeeding durations than home births. Cesarean births were associated with later breastfeeding initiation, shorter breastfeeding durations, and more formula feeding than vaginal hospital births.
Conclusion:
We have observed temporal and maternal age-related trends toward suboptimal breastfeeding patterns in the Maya community. Contrary to our first hypothesis, hospital births per se were not associated with negative breastfeeding outcomes. In support of our second hypothesis, cesarean versus vaginal births were associated with negative breastfeeding outcomes.
Well Established
Breastfeeding supports optimal infant health, and its benefits are particularly salient in remote and economically deprived settings. Despite rigorous international health promotion efforts, impoverished mothers face barriers to breastfeeding in many modernizing rural regions throughout the developing world.
Newly Expressed
Maya birthing practices are in transition. Hospital births are increasingly common and cesareans now make up nearly 30% of births. Vaginal hospital births were associated with better breastfeeding outcomes than home births. Cesareans were associated with worse breastfeeding outcomes than vaginal births. Young mothers have adopted formula feeding, early complementary feeding, and shortened breastfeeding durations.
Background
Breastfeeding supports optimal infant health, and its benefits have been extensively documented.1-13 Due to its indisputable benefits, the World Health Organization (WHO) recommends early breastfeeding initiation (within 1 hour of birth), 6 months of exclusive breastfeeding, and continued breastfeeding (in conjunction with appropriate complementary foods) for 2 years and beyond.14-16 Promotion of these WHO-recommended practices is a major international public health goal.16,17
World Health Organization breastfeeding recommendations are largely concordant with the traditional breastfeeding patterns of many nonindustrialized populations in the developing world. 18 In rural and impoverished environments, prolonged and intensive breastfeeding is the only economical, hygienic, and nutritionally adequate infant feeding option.18-21 However, modernization and urbanization can pose novel economic and social barriers to the initiation and maintenance of breastfeeding in these populations.22-33 Many modernizing communities experience changes that can affect breastfeeding behaviors such as maternal employment,30,34-37 aggressive marketing of breast milk substitutes, 38 the sexualization of breasts,39,40 and the medicalization of birth.41-45
Although these changes inevitably influence maternal–infant interactions and breastfeeding, the susceptibility (or resilience) of traditional breastfeeding patterns to encroaching modernization has been documented in only a handful of remote societies. These studies show that modernization has variable effects on the breastfeeding patterns of traditional populations, but they do not focus on the role of changing birth dynamics. For example, shorter breastfeeding durations and increased formula feeding were documented in a Yucatec Maya community following exposures to modern medicine and mainstream belief systems. 22 In contrast, modernization was associated with increased breastfeeding intensity in an Amazonian population, likely due to improvements in maternal education and nutritional conditions. 46 The diversity of environmental conditions, historical and cultural factors, and women’s work activities in remote settings make it challenging to predict how modernization might influence traditional breastfeeding patterns. It is nonetheless important to identify and mitigate novel barriers to breastfeeding in remote communities, because nearly half of the world’s population and 70% of the world’s poor live in rural areas. 47
In Mexico, the rural poverty rate is 63.6%, and indigenous peoples make up the vast majority of the rural poor.47,48 To address this problem, Mexico has provided government assistance programs (Progresa, 1997, reinstated in 2002 as Oportunidades) that are dedicated to “breaking the generational cycle of poverty” through health care, nutritional supplementation, educational incentives, and cash stipends. Currently, approximately 30% of Mexican families, predominantly rural and indigenous, are beneficiaries of Oportunidades. 49 The program has yielded well-documented improvements in child growth, health, and development. 50 At the same time, some potentially negative trends have recently been reported. For example, breastfeeding initiation rates and breastfeeding durations have decreased markedly in indigenous populations since the inception of these programs (1999-2006). 51 Furthermore, Mexico’s national rate of cesarean births rapidly increased (from 24.2% in 1994 to 44.8% in 2010), even among the rural poor. 52
Many rural indigenous Mexican populations have until very recently maintained traditional birthing and breastfeeding practices.53-55 We suspected that a recent and abrupt shift to hospital birthing practices, and particularly a rise in cesarean births, might contribute to the erosion of their traditional breastfeeding patterns. No study, to our knowledge, had assessed the relationship between changing birthing practices and breastfeeding outcomes in a remote population that has only recently had access to medical care. Still, ample evidence from industrialized settings suggests that intrapartum medical interventions, and particularly cesarean births, can pose barriers to breastfeeding.45,56-59 Indigenous Mexican mothers are particularly disempowered in the hospital environment due to their impoverished status and linguistic barriers. Under these circumstances, we expected that hospital birthing practices, and cesarean births in particular, may be especially detrimental to their breastfeeding success.
To investigate the relationships between modernization, changing birth dynamics, and breastfeeding patterns, we conducted a cross-sectional study in a small community of Maya subsistence agriculturalists in Campeche, Mexico. This community provided an ideal population in which to conduct the study. It is geographically isolated, and traditional birthing and breastfeeding patterns predominated until very recently. Only in the past 20 years have villagers had access to modern medical care, followed by a rise in hospital and cesarean births. Mothers maintain prolonged breastfeeding durations (2.60-year median, 2007-2011) 60 ; however, we suspected that breastfeeding patterns, like birthing practices, are in transition.
The goal of this article is to examine whether hospital birthing practices, and particularly cesareans, are detrimental to traditional breastfeeding patterns in a rural indigenous population. We conducted this study with 2 broad aims: First, we evaluated changes in birthing practices and breastfeeding beliefs and behaviors over time. Second, we identified barriers to breastfeeding, with a focus on the birth experience. We specifically hypothesized that (1) mothers who gave birth at home would have better breastfeeding outcomes, and (2) mothers who had vaginal births would have better breastfeeding outcomes. We operationalized “breastfeeding outcomes” using the following 4 variables: timing of breastfeeding initiation, the use of infant formula, age of introduction of complementary feeding, and breastfeeding duration.
Methods
Study Setting
The Maya of Xculoc are traditionally subsistence maize agriculturalists who reside in the humid and hilly Puuc region of the Yucatan Peninsula. Their economic structure, subsistence strategy, household organization, and demographic characteristics have been extensively studied for the past 20 years. 61 In 1992, villagers (population = 316) participated minimally in the labor–market economy. Their diet consisted primarily of maize and the village had no running water, electricity, or motorized transportation. 62 Men, women, and children participated in agricultural labor and grew most of the food they consumed. Medical care was not locally available. Most women gave birth at home and had no access to prenatal care or contraceptives. Fertility was high (7-8 births on average per woman), and women spent their reproductive career in a cycle of pregnancy and lactation. 63
The community is now experiencing rapid changes in diet, health, and economy. The population has increased to more than 500 people. Recent road improvements (2001) and the introduction of mechanized agriculture in the past several years have increased market sales and contributed to the consumption of market foods. A clinic was established in 1997 but did not operate regularly until around 2001. Minor illnesses and injuries can now be treated there. A local health promoter and a physician who visits once or twice monthly oversee it.
Fertility is now in transition in this Maya community. Although some women are having even larger families than before, contraceptives are now available, and other women express a desire to have small families. Since 2007, major changes in the health surveillance of mothers and young children have occurred with the instigation of the Oportunidades program. For example, the village health promoter now monitors growth and morbidity in children monthly from birth to 5 years.
Prenatal care is also now widely available, and most young women now choose to have hospital births. However, a midwife lives in the village and some women still choose to give birth at home. Midwives tend to promote prolonged and intensive breastfeeding. In hospital settings, the execution and efficacy of breastfeeding promotion varies by facility and by individual health care practitioner. Although Mexican doctors and nurses are required to promote breastfeeding, there is little oversight of actual promotion practices.
Data Collection and Analysis
From May to June 2014, we interviewed a cross-sectional sample of 58 Maya mothers (ages 21-85) regarding their birth histories and breastfeeding beliefs and practices. The 58 women represent approximately 60% of all mothers (in that age range) who currently live in Xculoc. Their youngest children ranged in age from 2 months to 53 years. Mothers were recruited at village clinic meetings and in informal household visits.
The sample was stratified into 5 age categories (20-30, n = 12; 30-40, n = 12; 40-50, n = 11; 50-60, n = 12; 60-85, n = 11) to capture maternal age-related trends. Young mothers were interviewed in Spanish, and older mothers were interviewed in Maya with assistance from a local Maya–Spanish translator. Interviews lasted on average for 45 minutes, with substantial variation among mothers. Reported maternal and child ages and maternal parity were cross-checked with demographic data and reproductive histories collected at regular intervals since 1992. Consent was obtained from community leaders and individual participants upon initiating research activities in the community. Research protocols were approved by the University of Utah’s institutional review board.
Mothers were asked how many times they had given birth and whether these were home births or hospital births. Home births refer to any birth that took place in Xculoc or another town or village in a private home or in the home of a midwife. Hospital births refer to any birth that took place in a medical facility with at least 1 medical doctor or nurse attending. Hospital births were then divided into vaginal and cesarean deliveries. Because mothers gave birth in a variety of hospitals and clinics, some of which no longer exist, we cannot state whether they were designated Baby-Friendly Hospital Initiative facilities.
Mothers were then asked open-ended questions about their beliefs regarding colostrum, preferred types of infant foods, and optimal breastfeeding durations. Another set of questions focused specifically on the birth of the mother’s youngest child. Mothers were asked how much time elapsed between the birth and the initiation of breastfeeding, if they practiced formula feeding, at what age complementary feeding began, and at what age the child was weaned (breastfeeding duration). Qualitative data were also collected regarding maternal perceptions of the birthing process and their interactions with medical personnel. These data are presented for the purposes of description and to contextualize our quantitative results.
To evaluate temporal and maternal age-related trends in hospital and cesarean births and breastfeeding outcomes (timing of breastfeeding initiation, presence/absence of formula, timing of complementary food introduction, and breastfeeding duration), we used generalized linear models. Timing of breastfeeding initiation, age of introduction of complementary feeding, and breastfeeding duration were non-normally distributed. They were treated as discrete variables (hours or months) and models assume an underlying Poisson distribution with a log link. Formula feeding is a binary variable and was modeled using a logistic regression.
Nonparametric correlations were used to assess relationships between timing of breastfeeding initiation, complementary food introduction, and breastfeeding duration. We also performed analysis of variance (ANOVA) comparisons of timing of breastfeeding initiation, complementary food introduction, and breastfeeding duration in formula-fed and non-formula-fed infants. Hypotheses were tested using generalized linear models, as described above. Initial models were adjusted for the year a birth occurred, maternal age at the time of interview, total number of births per mother, and potential interactions between year of infant birth and maternal age, and between maternal age and number of births. Models with the lowest Akaike information criteion (AIC) are reported here. Data were analyzed using SPSS, version 21.
Results
Sample Characteristics
Descriptive statistics for maternal birth history and reported breastfeeding practices are presented in Table 1. Of the 58 mothers, 72% (n = 42) were not at risk of conception, 55% (n = 23) were postmenopausal, and 45% (n = 19) had undergone tubal ligation. Of the remaining 16 mothers, only 1 woman (6%; n = 1) was currently pregnant, and 50% (n = 8) were still breastfeeding their youngest child. Lactating mothers were excluded from subsequent analyses pertaining to breastfeeding duration.
Descriptive Statistics for 58 Maya Women in Our Sample, with Summary of Interview Results.
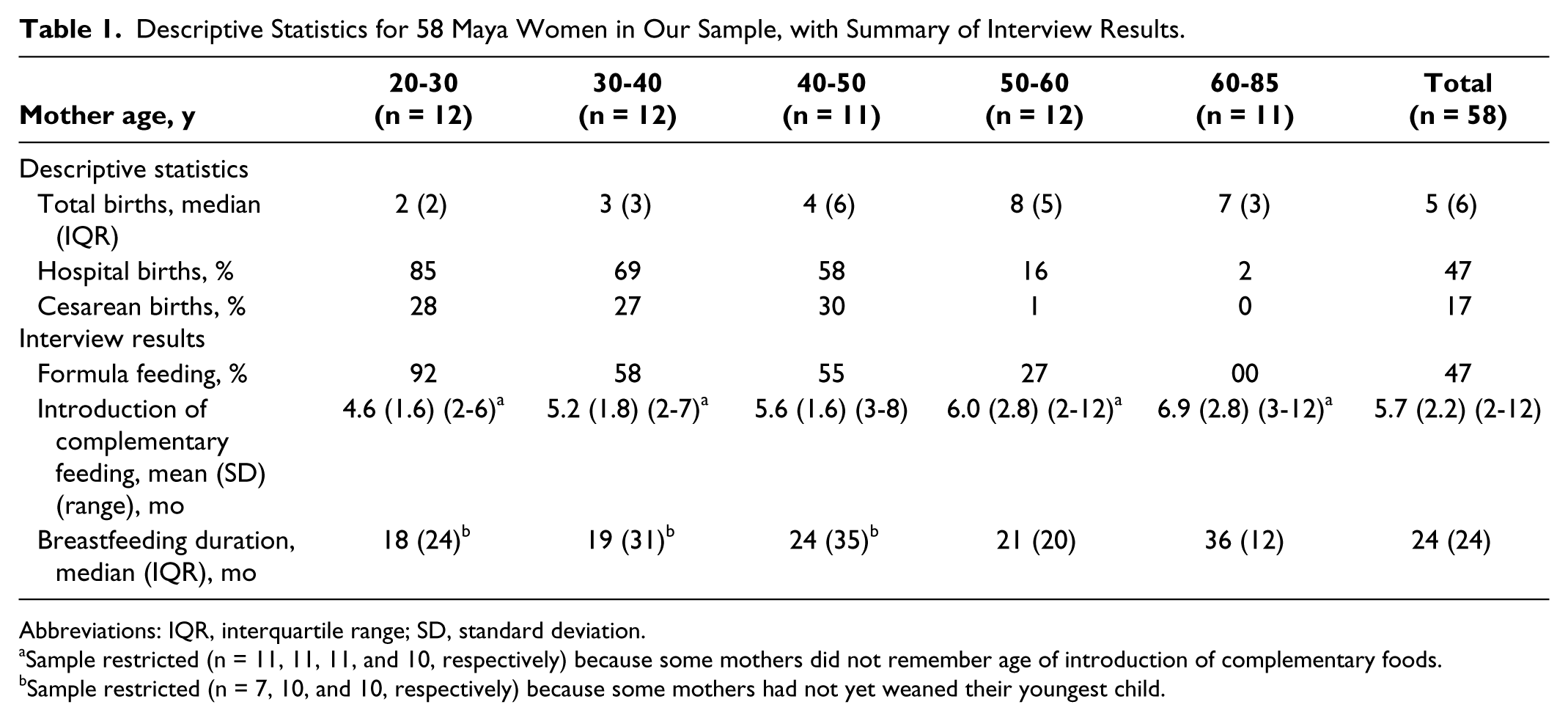
Abbreviations: IQR, interquartile range; SD, standard deviation.
Sample restricted (n = 11, 11, 11, and 10, respectively) because some mothers did not remember age of introduction of complementary foods.
Sample restricted (n = 7, 10, and 10, respectively) because some mothers had not yet weaned their youngest child.
Birth in Transition
Total births to mothers in our sample (290 total, n = 58 mothers) spanned a 66-year period (1948-2014). For women who had their last birth between 1948 and 2002, < 3% (n = 4) of 144 total births occurred in a hospital setting, and 50% (n = 2) of the 4 hospital births were cesarean deliveries. For women who had their last birth between 2002 and 2014, nearly 48% (n = 70) of 146 total births occurred in a hospital setting and 30% (n = 21) of hospital births were cesarean deliveries.
The mothers in our sample had a variety of birth experiences: 29% (n = 17) had only home births attended by designated midwives, 36% (n = 21) had only hospital births, and 34% (n = 20) had given birth both at home and in hospitals. The majority of mothers had given birth only vaginally (71%, n = 41), whereas 19% (n = 11) had experienced 1 cesarean delivery and 10% (n = 6) had experienced 2 cesarean deliveries. All mothers expressed a preference for vaginal over cesarean births, because cesareans have a much longer recovery period. Several mothers complained that they could not work for several months following a cesarean birth, to the detriment of their families.
Breastfeeding Trends over Time
Breastfeeding beliefs and behaviors are based on mothers’ reports for their last-born children only (58 children). These last births spanned a 53-year period (1961-2014). In our sample, 33% (n = 19) of last-borns were born at home, whereas 67% (n = 39) were born in hospitals. The majority of last-births were vaginal (81%, n = 47), with cesarean deliveries composing 28% (n = 11) of hospital births.
The majority of mothers (98%) believed that breast milk is the best food for infants. Only 1 mother believed that breast milk and breast milk substitutes were equally adequate infant foods. All of the mothers recognized the benefits of colostrum, although older and younger mothers tended to have different reasons for this belief. Young women often reported having learned about colostrum’s benefits from medical practitioners, and many compared it to a vaccination. In contrast, older mothers tended to believe that feeding colostrum helps the milk “mature” and reported that they learned this from their midwives and female kin.
All of the mothers in the sample initiated breastfeeding, and most did so within 1 hour of birth (71%, n = 41). However, 22% (n = 13) initiated breastfeeding between 1 and 24 hours following birth, and 5% (n = 3) initiated breastfeeding 1 to 3 days postpartum due to medical complications or insufficient milk. In an extreme case, 1 mother (< 2%) initiated breastfeeding at 30 days postpartum due to excessive postnatal complications. This outlier was excluded from subsequent analyses. In ordinary least squares regressions, timing of breastfeeding initiation (in hours) increased significantly each year [exp(β) = 1.02; 95% confidence interval (CI), 1.01-1.03; n = 57], but not with maternal age [exp(β) = 1.00; 95% CI, 0.99-1.00; n = 57].
No child born to the 14 mothers whose last birth occurred between 1961 and 1991 was formula fed. Of 11 mothers whose last birth occurred between 1992 and 2002, 36% (n = 4) formula fed their youngest child. Of 33 mothers whose last birth occurred between 2003 and 2014, 70% (n = 23) formula fed their youngest child. In a simple logistic regression model, formula feeding increased significantly each year [exp(β) = 1.15; 95% CI, 1.03-1.29; n = 44] from 1992 to 2014. In a simple logistic regression model, formula feeding decreased significantly with maternal age [exp(β) = 1.08; 95% CI, 1.01-1.15; n = 44]. Interactions between year of birth and maternal age were not significant.
Mothers described a variety of introductory complementary foods. The most common were boiled vegetables such as carrots, potatoes, and squash; tortillas; pureed beans; crackers; atole; and boiled chicken. Preferred infant foods did not vary substantially across age groups, or over time, except for 2 young mothers who used applesauce and store-bought infant food. In ordinary least squares regressions, the timing of the introduction of complementary feeding (in months) did not change significantly over time [exp(β) = 0.99; 95% CI, 0.99-1.00; n = 53] but did increase with maternal age [exp(β) = 1.01; 95% CI, 1.01-1.02; n = 53].
Mothers reported a range of breastfeeding durations from 1 to 72 months. Only 2 mothers breastfed for very short durations (≤ 2 months), and both weaned early due to medical complications. In ordinary least squares regressions, breastfeeding duration (in months) did not change significantly over time [exp(β) = 1.00; 95% CI, 0.99-1.00; n = 50] but did increase significantly with maternal age [exp(β) = 1.01; 95% CI, 1.01-1.01; n = 50].
When asked how long infants should breastfeed (optimal breastfeeding duration), maternal responses varied (Table 2). Nearly half of mothers did not provide an optimal duration because they believed that infants should be breastfed as long as possible (until the child self-weans or a new baby is born). Other mothers reported optimal breastfeeding duration of 6 to 12 months, or 13 to 48 months, whereas some reported that they did not know the optimal breastfeeding duration.
Reported Optimal Breastfeeding Duration in 58 Maya Mothers.
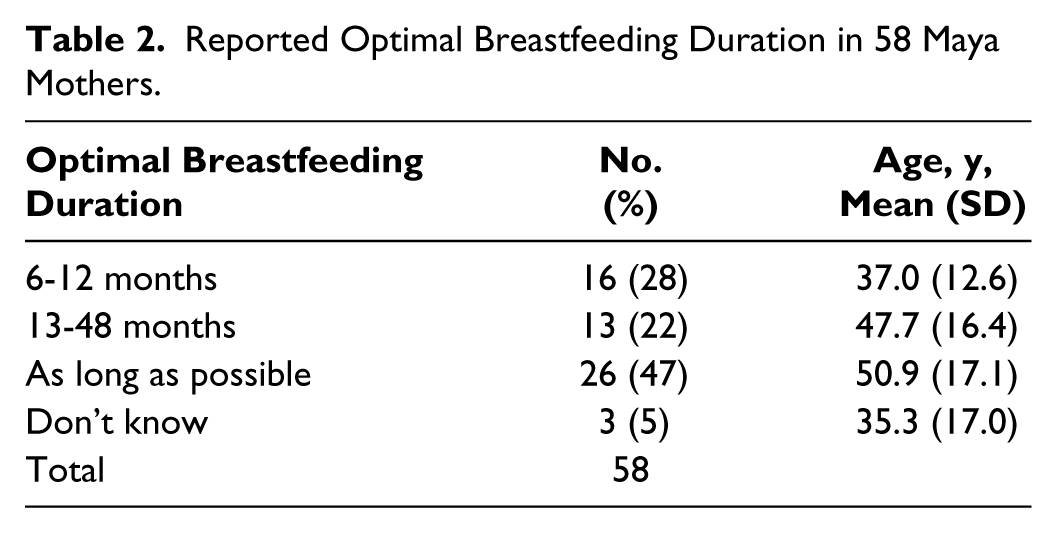
Mothers who reported an optimal breastfeeding duration of 6 to 12 months often claimed that this was the recommendation they had received from a doctor or health care worker. They were also significantly younger than mothers who favored breastfeeding as long as possible in between-group comparisons (mean difference = −13.82, P = .02). Differences in age were not significant between the groups reporting 6–12- and 13–48-month optimal breastfeeding durations (mean difference = −10.61, P = .23) or between the group reporting a 13–48-month optimal breastfeeding duration and the group who favored breastfeeding for as long as possible (mean difference = 3.20, P = 1.00).
Relationships between Breastfeeding Outcomes
Table 3 summarizes the nonparametric correlations between timing of breastfeeding initiation, timing of complementary feeding onset, and breastfeeding duration. There was a significant and positive correlation between breastfeeding duration and timing of onset of complementary feeding. There was a significant inverse correlation between timing of breastfeeding initiation and breastfeeding duration. There was no significant correlation between timing of breastfeeding initiation and the timing of introduction of complementary feeding. ANOVA comparisons of formula-fed infants with infants who were not formula-fed yielded significant differences in other breastfeeding outcomes: formula feeding was associated with later timing of breastfeeding initiation (F = 4.93, P = .03), earlier onset of complementary feeding (F = 4.30, P = .04), and shorter breastfeeding durations (F = 4.15, P = .05).
Spearman’s (Nonparametric) Correlation Matrix for 3 Outcome Variables (Each Reported in Months).
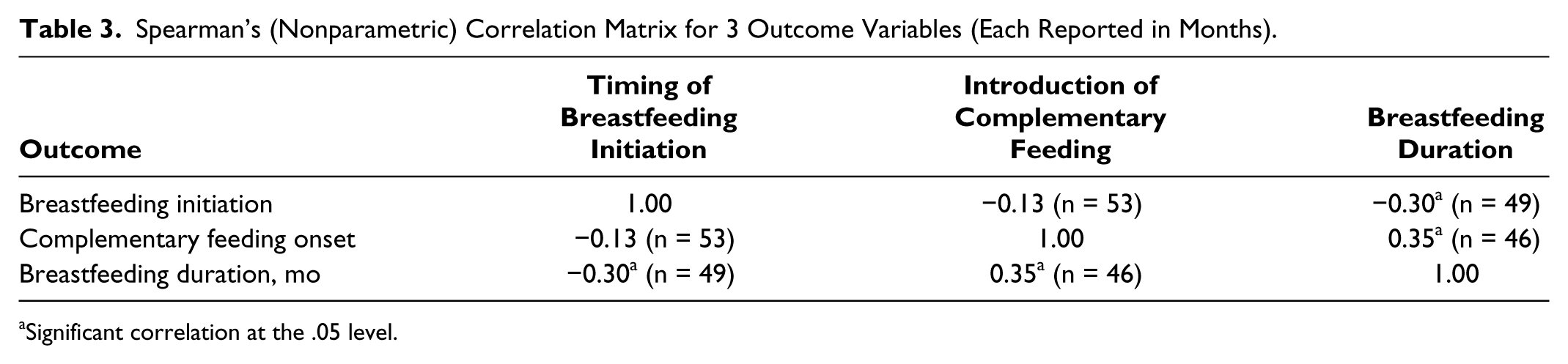
Significant correlation at the .05 level.
Birthing Practices and Timing of Breastfeeding Initiation
Timing of breastfeeding initiation did not differ significantly between home births and hospital births after adjusting for maternal age and year of birth [exp(β) = 1.21; 95% CI, 0.88-1.68; n = 57]. All mothers who gave birth at home had immediate skin-to-skin contact and attempted to breastfeed shortly after parturition. In hospital settings, most mothers initiated breastfeeding approximately 1 hour following birth (when there were no complications).
Among vaginal births, hospital births were significantly associated with earlier breastfeeding initiation than were home births [exp(β) = 0.28; 95% CI, 0.18-0.42; n = 45]. This effect is largely due to 1 mother who had a home birth and delayed breastfeeding initiation for 3 days due to insufficient milk. Although an outlier among home births, we retained this individual in our analysis. We do not assume that breastfeeding complications are limited to the hospital setting.
Among hospital deliveries, cesarean births were associated with delayed breastfeeding initiation [exp(β) = 6.90; 95% CI, 5.03-9.47; n = 37]. We combined these results into 1 model comparing timing of breastfeeding initiation in home births, vaginal hospital births, and cesarean births (Table 4). Vaginal hospital births were associated with the earliest breastfeeding initiation, and cesarean births were associated with the latest breastfeeding initiation. The best-fit model controls for maternal age, maternal age squared, and year of birth.
Timing of Breastfeeding Initiation by Location and Mode of Birth in 57 Maya Mothers, Assuming a Poisson Distribution with Log Link (AIC = 833.98).
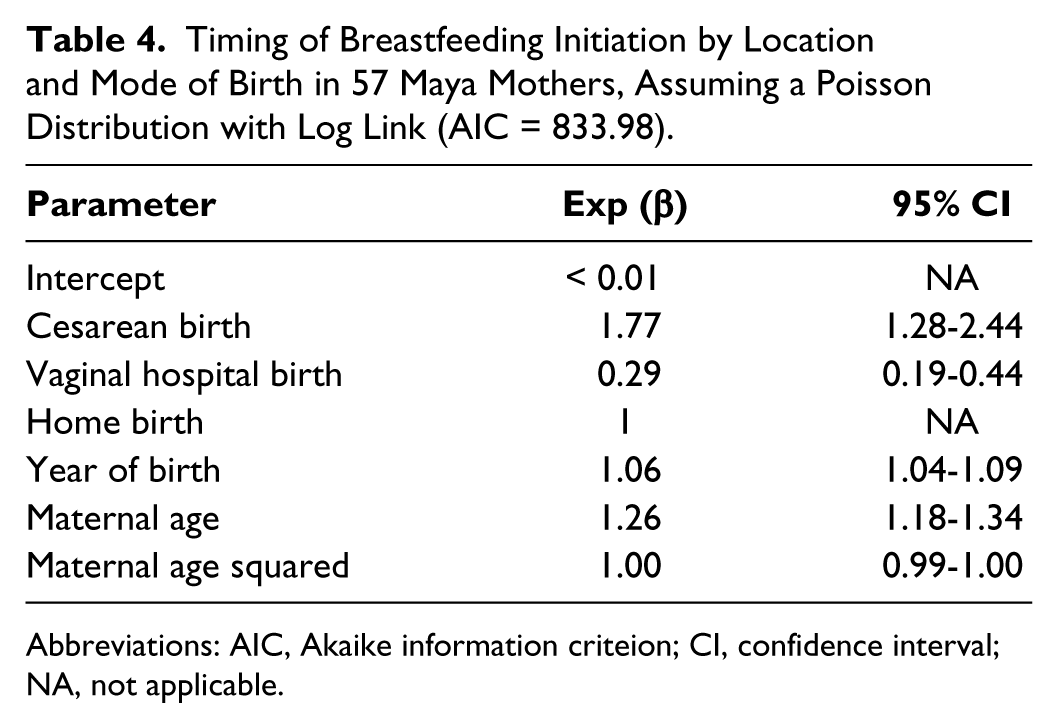
Abbreviations: AIC, Akaike information criteion; CI, confidence interval; NA, not applicable.
Birthing Practice and Formula Feeding
Birth location and mode of birth were not associated with probability of formula feeding after controlling for the year in which the birth occurred [exp(β) = 0.75; 95% CI, 0.12-4.84; n = 58]. However, when the analysis was limited to hospital births, cesarean births tended to be associated with increased formula feeding after controlling for year of birth [exp(β) = 9.89; 95% CI, 0.96-1.02; n = 38]. Many mothers who fed their infants formula did so upon recommendation by a medical doctor, often to replace breast milk when breastfeeding initiation was delayed. Even when breastfeeding initiation was timely and successful, doctors recommended formula to augment breast milk. Many mothers complained that formula was expensive and reported that their infants preferred breast milk.
Birthing Practice and Timing of Introduction of Complementary Foods
Birth location was not a significant predictor of complementary feeding onset after controlling for maternal age [exp(β) = −0.17; 95% CI, 0.58-1.10] or other potential confounders. Mode of birth was not a significant predictor of complementary feeding onset after controlling for maternal age [exp(β) = 1.00; 95% CI, 0.74-1.35] or other potential confounders.
Birthing Practice and Breastfeeding Duration
Among mothers who had weaned their last child, breastfeeding duration was longer for hospital births than for home births after adjusting for maternal age and year of birth [exp(β) = 1.23; 95% CI, 1.06-1.44; n = 50]. Among vaginal births, hospital births were associated with longer breastfeeding durations than were homebirths [exp(β) = 0.71; 95% CI, 0.60-0.83; n = 40] after adjusting for maternal age and year of birth.
Among hospital births, cesarean deliveries were associated with shorter breastfeeding durations [exp(β) = 0.81; 95% CI, 0.69-0.95; n = 31] than vaginal deliveries. We combined these results in a model comparing breastfeeding duration in home births, vaginal hospital births, and cesarean births (Table 5). Vaginal hospital births were associated with the longest breastfeeding durations. Cesarean births and home births had roughly equal breastfeeding durations. The best-fit model controls for maternal age and year of birth.
Breastfeeding Duration by Location and Mode of Birth in 50 Maya Mothers Who Had Weaned Their Youngest Child (AIC = 657.90).
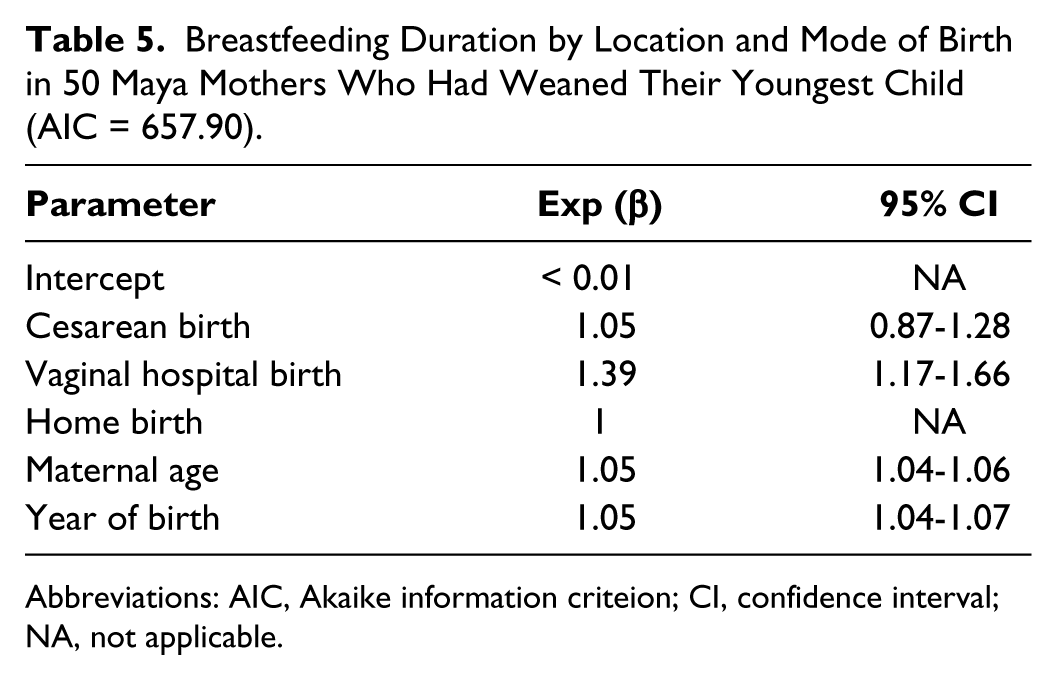
Abbreviations: AIC, Akaike information criteion; CI, confidence interval; NA, not applicable.
Discussion
Maya mothers maintain favorable attitudes toward breastfeeding and reported intensive breastfeeding patterns over the past 53 years. Their breastfeeding patterns are largely concordant with many nonindustrialized populations and with WHO recommendations.18,64 This is likely because many common economic and social barriers to breastfeeding are absent in this community. Breastfeeding mothers rarely engage in wage labor, and women’s subsistence and household tasks are compatible with breastfeeding. 63 Prolonged, intensive breastfeeding is still the cultural norm, and no taboos prohibiting public breastfeeding exist.
Despite these beneficial aspects of Maya breastfeeding culture, our analyses suggest potentially detrimental temporal and maternal age-related trends in several breastfeeding outcomes, such as decreases in breastfeeding duration and the onset of formula feeding (summarized in Table 6). This is particularly concerning because the Maya continue to live under conditions of poverty and poor sanitation. Suboptimal infant feeding practices are especially detrimental to infant health in such epidemiologically challenging environments.
Summary of Results.
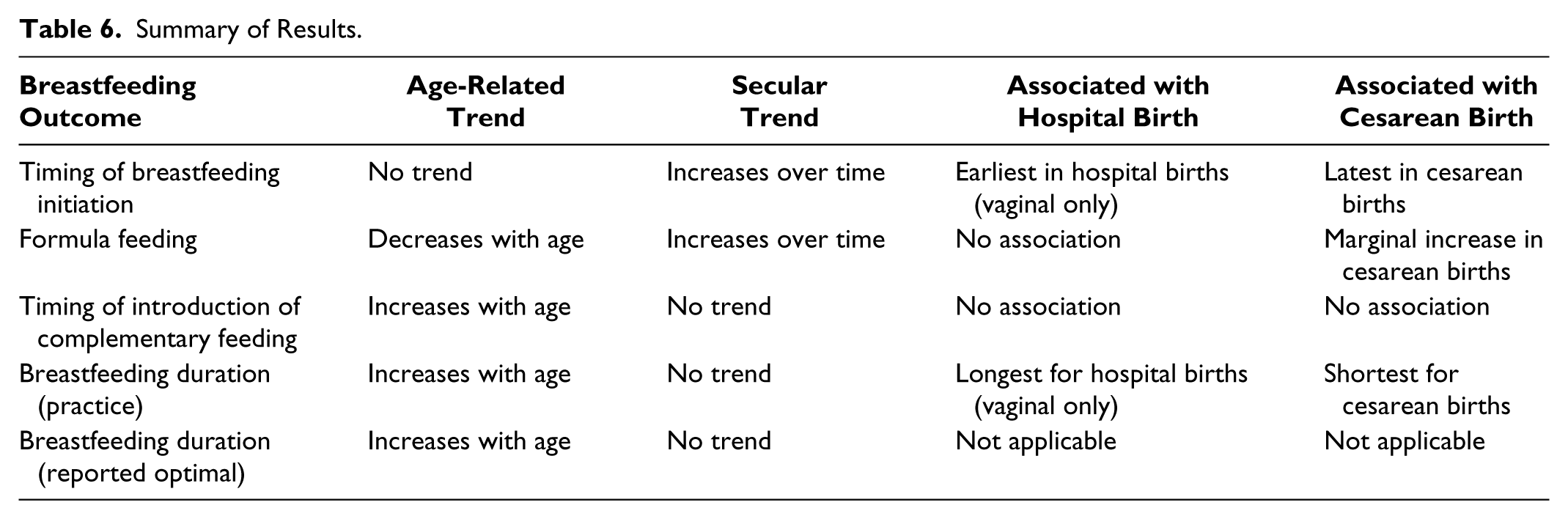
Maya birthing practices are also in transition. Hospital births are increasingly common and the cesarean rate is nearly 30%. Contrary to our hypothesis, hospital births per se were not associated with negative breastfeeding outcomes. In fact, vaginal hospital births had the best breastfeeding outcomes. However, in the case of cesarean births, breastfeeding initiation was inevitably delayed. As hypothesized, several negative breastfeeding outcomes were associated with cesarean births (Table 6).
Maternal Age-Related Trends in Breastfeeding
Several changes in breastfeeding patterns appear to be age related. Maternal age was a strong predictor of formula feeding, age of complementary feeding onset, breastfeeding duration, and even perceived optimal breastfeeding duration. Maternal age-related changes are not surprising, given the many recent changes associated with modernization. Younger mothers tend to be more acculturated. Compared to older mothers, they have higher levels of formalized education, travel more often to larger towns, and are more exposed to mainstream Mexican values and popular culture. Young Maya also have access to modern medicine, prenatal care, and birth control, whereas the oldest mothers did not. Future research is needed to determine if and how these differences underlie maternal age-related declines in breastfeeding.
We suspect that, in particular, medical care access may play a role. For example, young mothers are exposed to the recommendations of health providers, who sometimes promote detrimental practices such as formula feeding and short breastfeeding durations. Furthermore, medical interventions such as vaccines and antibiotics may mitigate some of the negative health effects of suboptimal infant feeding. Young mothers may therefore perceive that prolonged and intensive breastfeeding is no longer necessary to maximize infant health and survival. 22
Temporal Trends in Breastfeeding
Timing of breastfeeding initiation and formula feeding rates each increased over time. These temporal trends were each independent of the effect of maternal age. These transitions seem to be associated with medical access and hospital birthing practices—mainly those associated with cesarean births. Because early breastfeeding is associated with lower neonatal mortality 65 (and with longer breastfeeding durations in this population), care should be taken to encourage prompt breastfeeding initiation in all but dire medical emergencies. Future research should explore the infant and longer term child health consequences of formula feeding in this population.
The Medicalization of Birth
In contrast to our first hypothesis, vaginal hospital births were associated with earlier breastfeeding initiation and longer breastfeeding durations than home births and cesarean births. In hospital settings, mothers generally reported being permitted to breastfeed shortly after birth (in the absence of cesareans and other complications). The longer breastfeeding durations reported for vaginal, hospital births were not expected and warrant further investigation.
We propose 2 potential mechanisms to explain this phenomenon. First, successful early breastfeeding initiation may generally contribute to a cascade of successful breastfeeding outcomes. Second, fertility differences may underlie variation in breastfeeding durations. Until very recently, the study community was a natural-fertility population with no access to hormonal birth control. Under these conditions, breastfeeding duration is tightly linked to birth spacing. As an illustration, many older mothers in our sample habitually breastfed their children partway into a subsequent pregnancy. They spent their reproductive careers in a cycle of gestation and lactation, and their fertility was modulated mainly by nutritional conditions. Now, hormonal contraceptives are available and mothers can choose to prolong their birth spacing. In particular, some mothers may opt for postnatal hormonal birth control following a hospital birth. This should allow them extra time to breastfeed longer.
Postnatal complications often contribute to delayed breastfeeding initiation following a cesarean birth, and mothers may need time to recover from anesthesia. In the Maya study community, cesarean births were associated with delayed breastfeeding initiation, as well as marginal increases in formula feeding and shorter breastfeeding durations than vaginal births. Interruptions in postnatal maternal–infant contact can be detrimental to a variety of breastfeeding outcomes.66-68 For example, the provisioning of prelacteal formula can interfere with the establishment of lactation. The mechanism linking cesarean births to shorter breastfeeding durations is unclear, but this pattern is concordant with the findings of several other studies.66-68
Although cesarean births are sometimes a medically necessary, life-saving procedure, much debate surrounds their use and overuse in Mexico and throughout the world.69-78 For example, elective cesarean births have increased among wealthy Mexican women who perceive the procedure as safe and convenient. 78 In contrast, the mothers in our study population prefer vaginal to cesarean births. They are particularly concerned about the prolonged postcesarean recovery period and how their lost labor affects their families.
We suspect that there may be additional negative consequences of increasing cesarean rates in remote and impoverished communities. For example, cesarean births are associated with increased rates of offspring obesity in childhood and adulthood,79-81 possibly due to differences in the establishment of inflammatory profiles. 81 Obesity is already an epidemic and a major public health crisis in Mexico. 82 Although obesity rates are currently highest in nonindigenous Mexicans, 83 indigenous populations are particularly susceptible to its negative health effects as they navigate nutritional and epidemiologic transitions.84,85
Limitations
Our study is limited by its small sample size and reliance on maternal reports. It is therefore possible that our results are subject to recall bias, particularly in interviews of older mothers. We are also limited in having no medical records regarding the births.
Conclusion
Indigenous Mexicans and other remote populations are susceptible to poverty-related health challenges. In resource-scarce, pathogenic environments, prolonged and intensive breastfeeding is crucial to protect infants from infectious disease and from encroaching diseases associated with modernization. The Maya women have generally maintained intensive breastfeeding practices, but some novel and detrimental practices have emerged and increased over time. Suboptimal breastfeeding patterns are particularly common in young mothers.
There seems to be a need to educate physicians in the area, particularly with respect to the dangers of formula feeding and shortened breastfeeding durations in impoverished settings. More oversight is needed to ensure that physicians and other medical personnel are promoting WHO-recommended breastfeeding practices. Medical care providers must also responsibly consider the short- and long-term detrimental effects of cesarean deliveries on maternal and infant health, particularly when working with vulnerable and impoverished populations. Future research efforts should focus on modernizing influences that may create novel breastfeeding barriers in rural communities throughout the developing world.
Footnotes
Acknowledgements
The authors thank the Maya women who participated in the research. The authors also thank Russell Greaves, Maxmilano Moo Moo, Rogelia and Mirna Moo Tzec, and Vitaliano Canul Pat.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Science Foundation, grant numbers 0349963 and 0964031.