
Abstract
Background:
Although Hispanic mothers in the United States have slightly higher rates of breastfeeding initiation than the national average, they are more likely to supplement with formula.
Objectives:
To describe infant feeding decisions in a sample of 72 urban Hispanic mothers and assess whether demographic and personal factors influence exclusive breastfeeding (EBF) status at 4 months postpartum.
Methods:
The study was longitudinal and included assessments during pregnancy, in the hospital following childbirth, and monthly up to 4 months following birth.
Results:
Nearly all of the 72 mothers were breastfeeding at discharge after the birth of their infant (94%); half of these were EBF. By 2 months postpartum, the rate of EBF had declined to 26%, dropping to 22% by 4 months. Significant predictors of EBF status at 4 months included the baseline indicator for mother’s partner as the most important person in life (adjusted odds ratio [AOR], 5.42; 95% confidence interval [CI], 1.03-28.66) and breastfeeding self-efficacy score at 1 month (AOR, 1.20; 95% CI, 1.07-1.34).
Conclusion:
These findings have particular relevance in this population, given the high rate of breastfeeding initiation coupled with breastfeeding self-efficacy being a modifiable factor. Support during pregnancy and postpartum, including consultation with a lactation consultant, may increase the self-efficacy of EBF in this low-income population, leading to higher rates of extended EBF among Hispanics.
Well Established
Hispanic mothers in the United States have slightly higher rates of breastfeeding initiation than the national average; nevertheless, they are more likely to supplement with formula. Early supplementation with formula decreases not only the rate of exclusive breastfeeding but also the duration of breastfeeding.
Newly Expressed
Hispanic mothers with a high level of breastfeeding self-efficacy at 1 month were more likely to exclusive breastfeed at 4 months. The quality of relationship with the partner was a more significant predictor of exclusive breastfeeding at 4 months than living with the partner.
Background
According to the 2010 Census, the Hispanic population accounted for most of the nation’s growth—namely, 56%—from 2000 to 2010. 1 In 2011, Hispanics comprised 16.7% (51.9 million) of the total population in the United States, an increase of 48% since 2000. Fertility in the same year was 7.7% for Hispanics compared with 6.4% of African Americans and 6.0% of whites. 2 Of all Hispanics residing in the United States, 49% are female; of these, 43% are of childbearing age, and half are immigrants. 2
Healthy People 2020 set objectives to combat the barriers to breastfeeding across all populations in the United States to reduce the proportion of breastfed newborns who receive formula supplementation within the first 2 days of life and increase the proportion who are exclusively breastfed at 6 months of age. 3 Hispanic mothers in the United States have slightly higher rates of breastfeeding initiation than the national average (80.6% vs 75.0%, respectively) 4 ; nevertheless, they are more likely to supplement with formula in the first 2 days of life compared with black and white US mothers (Hispanic, 33%; black, 28%; white, 22%). 5 Early supplementation with formula decreases the rate of breastfeeding duration and exclusivity.6-8 Exclusive breastfeeding (EBF) for the first 6 months of an infant’s life offers additional health benefits, including an increase in receptive language and verbal and nonverbal intelligence and lower risk of type 1 and type 2 diabetes, celiac disease, and sudden infant death syndrome.9-11 There is also evidence that racial/ethnic disparities in childhood obesity (ie, higher prevalence of overweight and obesity among Hispanic children) may be reduced by increasing the prevalence of EBF for 6 months and delaying the introduction of solid food.12-16
A study about decision making among low-income Hispanics reported that mothers want to breastfeed but at the same time provide formula as a way to give their babies the best of both. 17 For immigrant and low-income Hispanic women, mixed feeding is considered acceptable, desirable, and not harmful.18-20 A study analyzing the attitudes about nonexclusive breastfeeding in Hispanic mothers in an area serving a large Dominican population reported that the most common reasons for introducing formula were mother’s perception of insufficient milk production, keeping the baby fuller longer, and planning for return to work. 18
Review of literature on breastfeeding worldwide describes 3 key modifiable factors that are positively associated with breastfeeding duration: (a) mother’s breastfeeding intention, (b) her breastfeeding self-efficacy, and (c) her social support. 21 Although investigators have described factors influencing breastfeeding among Hispanic mothers, there is limited research about EBF, and none has addressed the importance of breastfeeding self-efficacy or the 3 key modifiable factors simultaneously on duration and EBF in the Hispanic population. The purposes of this study were to (1) describe infant feeding decisions in a sample of urban Hispanic mothers in Kentucky who were followed during pregnancy and for 4 months postpartum; (2) assess whether breastfeeding self-efficacy, measured in mothers who were EBF at 1 month, differs between those who were still EBF at 4 months and those who had switched to another type of feeding by that time; and (3) examine the demographic and personal factors, including the quality of the primary intimate relationship, infant feeding intentions, and breastfeeding self-efficacy, which influence EBF status at 4 months postpartum.
Methods
Design and Sample
The study design was longitudinal and included assessments during pregnancy, the hospital stay following the birth of the child, and monthly assessments up to 4 months after hospital discharge. One hundred women were enrolled in the study, and 72 completed the 4-month assessment (72% retention). While the sample size of the full study was planned so that there would be at least 80% power to detect a multiple regression R2 of at least 0.15 with an α level of .05 and up to 10 predictors, the current study is focused on only those with known infant feeding status at 4 months and uses a different analytic strategy. The largest percentage of the mothers who dropped out did so by the 1-month assessment (47%). Reasons for attrition were inability to reach (n = 26) and death of the infant (n = 2).
Procedure
The Medical Institutional Review Board of the University of Kentucky approved the study. To ensure privacy and to protect participants’ sensitive information on immigration status and/or mistrust in sharing their personal information, a Certificate of Confidentiality was obtained from the National Institutes of Health. Participants were recruited from a primary health care clinic that provides prenatal care to Hispanic women. Women were approached in a waiting area reserved exclusively for pregnant patients by bilingual and bicultural trained research personnel who explained the objectives of the study, checked for eligibility, and invited them to participate in the study. Women who agreed to participate and met the inclusion criteria signed a written informed consent and Health Insurance Portability and Accountability Act forms. Inclusion criteria were as follows: (1) self-identified as Hispanic, (2) age 16 years or older, (3) an apparently healthy pregnancy at or beyond 20 weeks of gestation, (4) planning to give birth in a local birthing hospital, and (5) intending to remain in central Kentucky for at least 4 months after the birth. In this study, we included pregnant women between 16 and 17 years old who met the state laws for emancipated minors. 22
The recruitment, informed consent documents, and interviews were administered in Spanish because most participants (98.6%) were immigrants, and all spoke Spanish as their primary language. Data were collected 6 times: prenatal survey (in person), chart review during hospital stay, perinatal survey during the first month (in-person), and postpartum phone calls at 2, 3, and 4 months. In-person interviews were scheduled at a time and place convenient to the participant. Mothers were compensated for participation with a $25 gift card during the prenatal survey, a baby gift package during the perinatal survey, and a $30 gift card at the last postpartum follow-up.
Measures
Demographic and personal characteristics
At the baseline prenatal interview, participants were asked to indicate their age, place of birth, and highest level of education. Responses to the education item were classified into 2 categories: less than high school diploma and high school diploma or higher. Mothers were asked to indicate whether they lived with their partner (yes or no). Also in the prenatal survey, mothers were asked, “Who is the most important person in your life?” and the open-ended responses were categorized as partner (ie, spouse, boyfriend) or other (ie, mother, other family member, and friend). This question was included as the opening prompt for the assessment of the quality of the primary intimate relationship. Determination of mode of delivery and the number of pregnancies (parity) was obtained by chart review.
Quality of primary intimate relationship was assessed during the prenatal survey using the Autonomy and Relatedness Inventory, Spanish version (ARI), a 32-item scale.23,24 The scale includes items that measure both the positive and negative aspects of the primary intimate relationship with the most important person in the respondent’s life, as indicated in the initial open-ended item. Each item was scored on a 5-point scale, with response options ranging from 1 = not at all like to 5 = very much like. To calculate a total score, negative items were reversed, all ratings were summed, and then 32 was subtracted from the sum so that the cumulative score ranged from 0 to 128. Higher scores indicate a more positive assessment of the relationship. Cronbach’s α for this sample was 0.92.
Breastfeeding plan and breastfeeding goal were assessed during the prenatal survey using the Infant Feeding Intentions, Spanish version (IFI).25,26 This scale has 5 items, with response options ranging from 0 = very much disagree to 4 = very much agree. The total score was obtained by averaging the first 2 items (which include planning about giving breastfeeding a try and another item that is reverse-coded as it is an endorsement of planning to use formula) and adding the remaining 3 items to this mean. The range of scores was from 0 to 16, with higher scores indicating a stronger intention to EBF until 6 months. Cronbach’s α for this study was 0.78.
Breastfeeding Self-Efficacy Scale, Spanish version (BSES)27,28 was used to measure maternal confidence to breastfeed at 1 month postpartum. This instrument consists of 33 items, each with a response set ranging from 1 = not at all confident to 5 = very confident. The summary score was created by adding the 33 items in the scale, with scores ranging from 33 to 165; higher scores indicated greater self-efficacy for breastfeeding. Cronbach’s α for this sample was 0.90.
Infant feeding status was measured starting with discharge from the hospital immediately following birth and continuing at each month postdischarge, with possible options of EBF, exclusive formula feeding (FF), or combination feeding (BOTH). EBF was defined as infant feeding with only breast milk, without any additional food or drink, and might include drops of medicine or vitamins/minerals; FF, when the infant was feeding only with formula; and BOTH, when the infant was feeding with breast milk and supplemented with formula or other food or drink.29,30 Infant feeding status at discharge was determined from reports via the infant’s chart review and compared for accuracy with the mother’s chart notes from the physician, lactation consultant, nurse, or other clinician. In cases where there was conflicting documentation and EBF and FF were documented, the abstractor selected BOTH. During 1 to 4 months postpartum, mothers were asked, “How do you feed your baby?” Mothers who indicated they were only breastfeeding were also asked, as a confirmation of EBF, “Does your baby receive water, juice, or any solids?”
Data Analysis
The comparisons of those who completed the study versus those who dropped out prior to 4 months postpartum were accomplished using the 2-sample t test or the χ2 test of association. All study variables were summarized descriptively using frequency distributions or means and standard deviations. Descriptive analysis was used to summarize the percentage of mothers in each infant feeding category starting at discharge from the hospital and continuing each month up to 4 months postpartum. A 2-sample t test was used to determine whether the level of breastfeeding self-efficacy among mothers who were EBF at 1 month differed between those who were still EBF at 4 months and those who had switched to another type of feeding by that time. Predictors of 4-month EBF status were determined by using binary logistic regression. Variance inflation factors were used to test this model for multicollinearity, and the goodness of fit of the logistic regression was assessed using the Hosmer-Lemeshow χ2 test. Data analysis was conducted using SAS version 9.3 (SAS Institute, Cary, NC, USA); an α level of .05 was used throughout.
Results
There were no differences between those who dropped out and those who completed the study on age, education, living situation (living with partner vs not), parity status, mode of delivery, or EBF status at discharge. Table 1 shows the demographic and reproductive characteristics among women included in the analysis. At baseline, participants generally rated their primary intimate relationship positively; the mean (SD) quality of the primary intimate relationship score was 107.1 (15.3) of a maximum possible of 128. Infant feeding intention scores had a mean (SD) of 11.8 (4.2) compared with the maximum possible score of 16. Finally, among the 61 mothers who were breastfeeding at 1 month (whether supplementing with formula or EBF), the mean (SD) score on the BSES at that time was 146.6 (14.7) compared with the maximum possible score of 165. This suggests that mothers in the study who were still doing any breastfeeding at 1 month were generally committed to continuing breastfeeding (Table 2).
Summary of Maternal Descriptive and Reproductive Characteristics (N = 72).
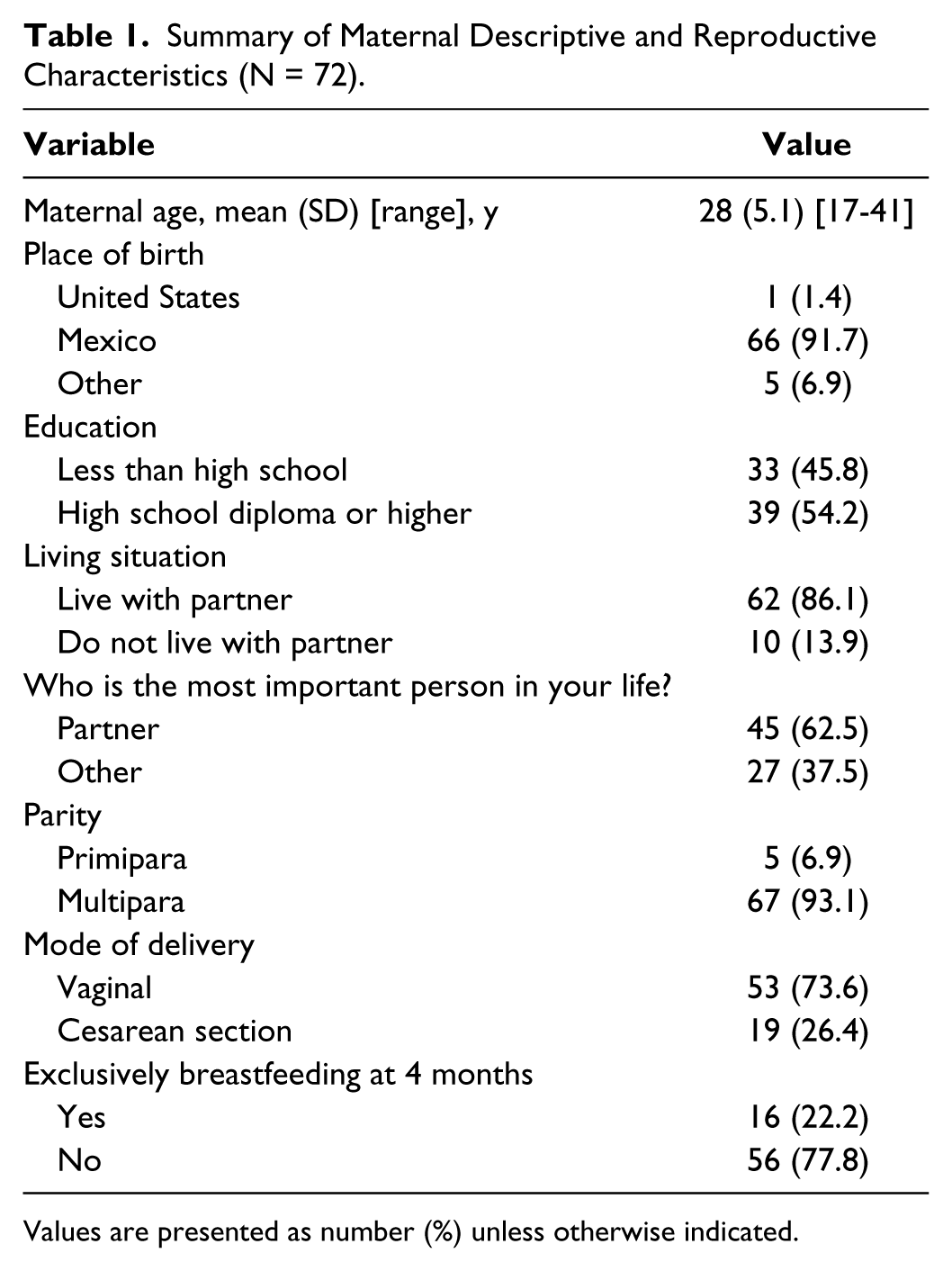
Values are presented as number (%) unless otherwise indicated.
Descriptive Summary of Maternal Scores with the Autonomy and Related Inventory, Infant Feeding Intention, and Breastfeeding Self-Efficacy Scale.
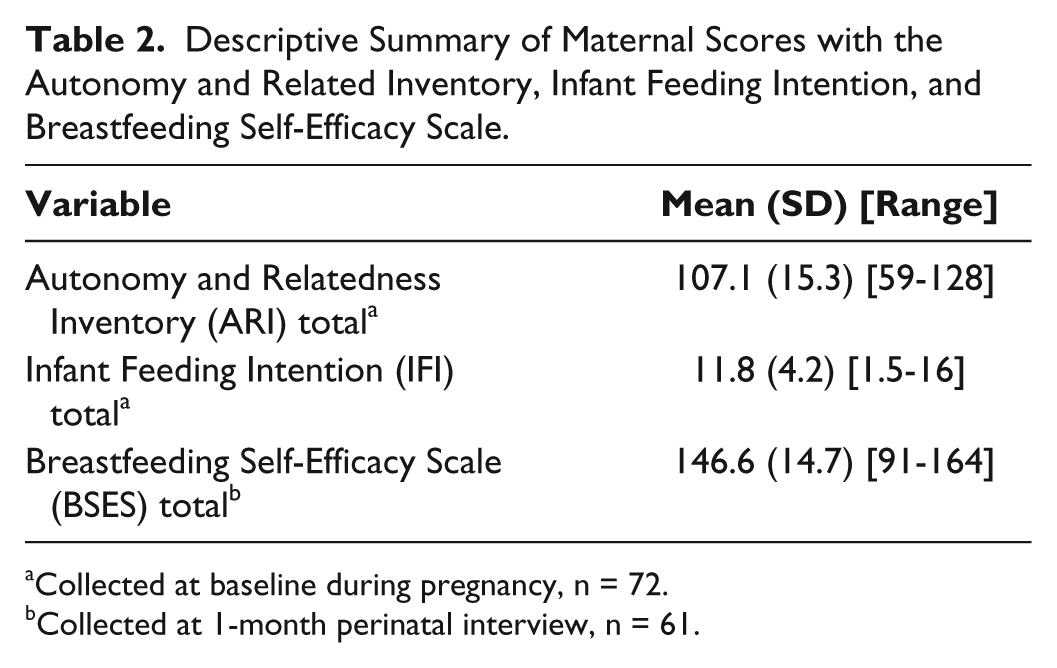
Collected at baseline during pregnancy, n = 72.
Collected at 1-month perinatal interview, n = 61.
Trajectory of Infant Feeding Decisions
As shown in the Figure 1, most of the mothers were breastfeeding at discharge, whether EBF (50%) or combining breastfeeding and formula (44%). At 1 month postpartum, 61 mothers were breastfeeding, including 26 who were EBF (36%) and 35 who were BOTH (49%). The increasing use of formula over time is apparent at both 2 and 3 months: in both assessments, 19 mothers were EBF (26%), and the number of mothers feeding BOTH also declined to 31 (43%) at 2 months and 28 (39%) at 3 months. At the conclusion of the study, 16 mothers continued to EBF (22%), 29 (38%) were using BOTH, and 27 (38%) were FF. The most common reasons among mothers who were EBF at discharge from hospital stay but introduced formula during the study were perception of low milk production (45%), followed by having to work (31%). Less common reasons included experiencing pain with breastfeeding (11%), embarrassment about breastfeeding in public (7%), pediatrician prescribed formula for low birth weight infant (3%), and mother taking medication (3%).
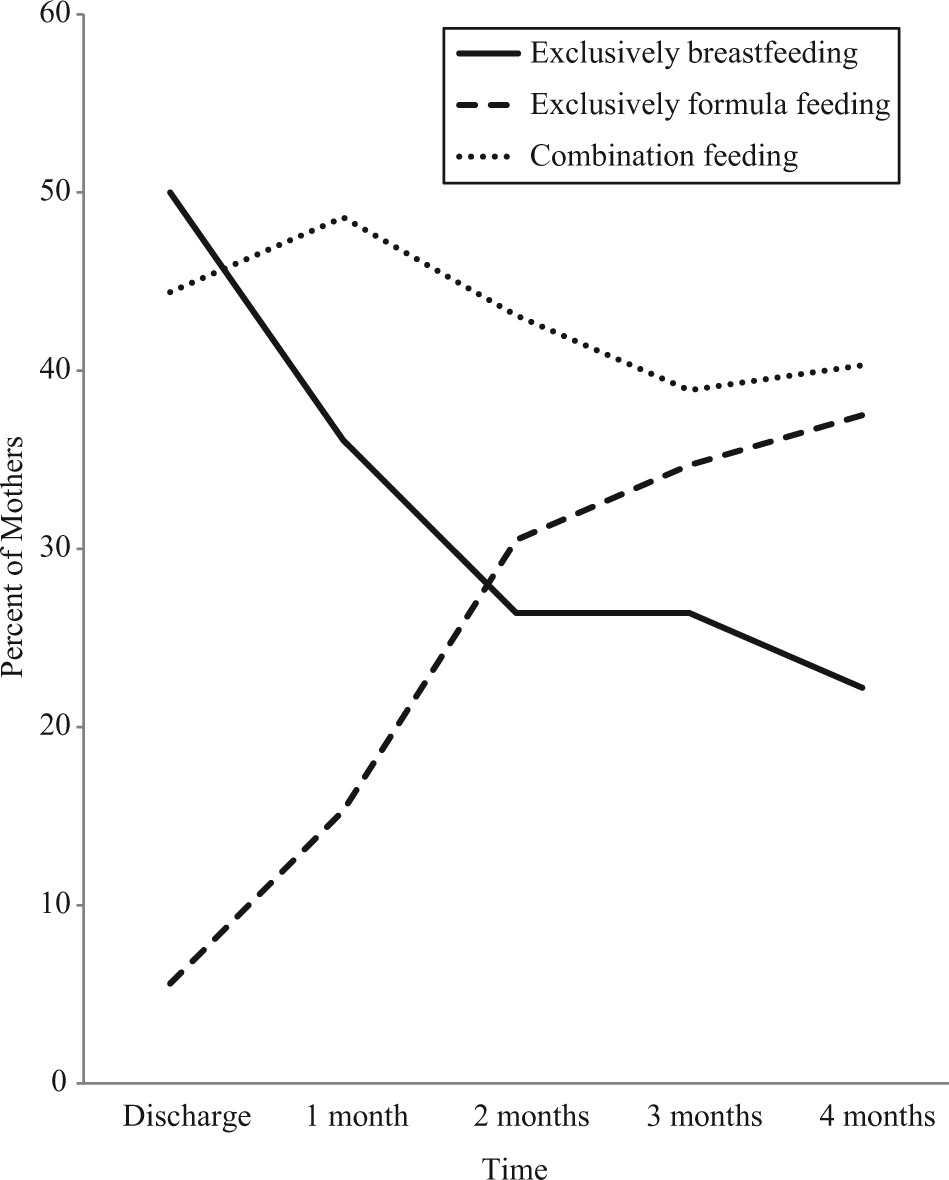
Percent of Mothers in Each Feeding Decision Category over Time (n = 72).
Breastfeeding Self-Efficacy and Continued Exclusive Breastfeeding
Among the 61 mothers who were breastfeeding at 1 month postpartum and completed the BSES at that time, 26 were EBF. Of this latter group of participants, half were EBF at 4 months and the other half were using either FF or BOTH methods of feeding. The mean (SD) BSES score for those who were continuing to EBF at 4 months was 157.6 (7.3) compared with 150.7 (11.7) for those who had switched to another type of feeding. Although the t test comparison of these 2 groups is not significant (t = 1.8, P = .083), this finding suggests that EBF mothers with lower BSES scores at 1 month postpartum may be at risk for changing their infants’ diet to include formula by 4 months postpartum.
Predictors of Exclusive Breastfeeding at 4 Months
The potential predictors included in the logistic regression to determine factors that influence EBF at 4 months were age, education, whether their partner is the most important person in their life, the quality of the intimate relationship ARI score, IFI score, and BSES score. Living status (ie, living with partner or not) was not included in this regression because it was significantly associated with the indicator for whether the partner is the most important person (χ2 = 5.2, P = .02), and also the association between “living with partner” and EBF at 4 months was weaker (χ2 = .03, P = .9) than the association between “partner is the most important person” and EBF at 4 months (χ2 = 3.1, P = .07). Similarly, given no association between EBF at 4 months and either parity status (χ2 < .1, P = .9) or mode of delivery (χ2 < .1, P = .9), these variables were not included in the regression. The final consideration for excluding these 3 variables was that they would have caused the model to exceed the goal of having at least 10 observations per predictor. 31
The overall logistic regression model was significant (χ2 = 25.0, P < .001), and the data fit the model well (Hosmer-Lemeshow χ2 = 4.8, P = .78). The model variance inflation factors were all less than 1.2, so multicollinearity is very unlikely to have distorted the regression parameters. The significant predictors of EBF status at 4 months included the indicator for whether the partner is the most important person and the breastfeeding self-efficacy score. Mothers who listed their partner as the most important person during the prenatal assessment had 5.4 the odds of being EBF as of the 4-month survey. For every point increase in BSES score, the odds that the mother was EBF at 4 months increased by 1.20 (Table 3). Given the 165-point range of scores possible for BSES, a 5-point difference may be more clinically meaningful; for every 5-unit increase in BSES as of the 1-month survey, mothers had 2.5 the odds of being EBF at 4 months postpartum (adjusted odds ratio, 2.47; 95% confidence interval [CI], 1.42-4.30). Likelihood of EBF at 4 months was not related to age, education, the quality of the primary intimate relationship, or infant feeding intentions assessed at baseline (during pregnancy).
Logistic Regression to Assess Predictors of Exclusively Breastfeeding at 4 Months Postpartum (n = 61). a
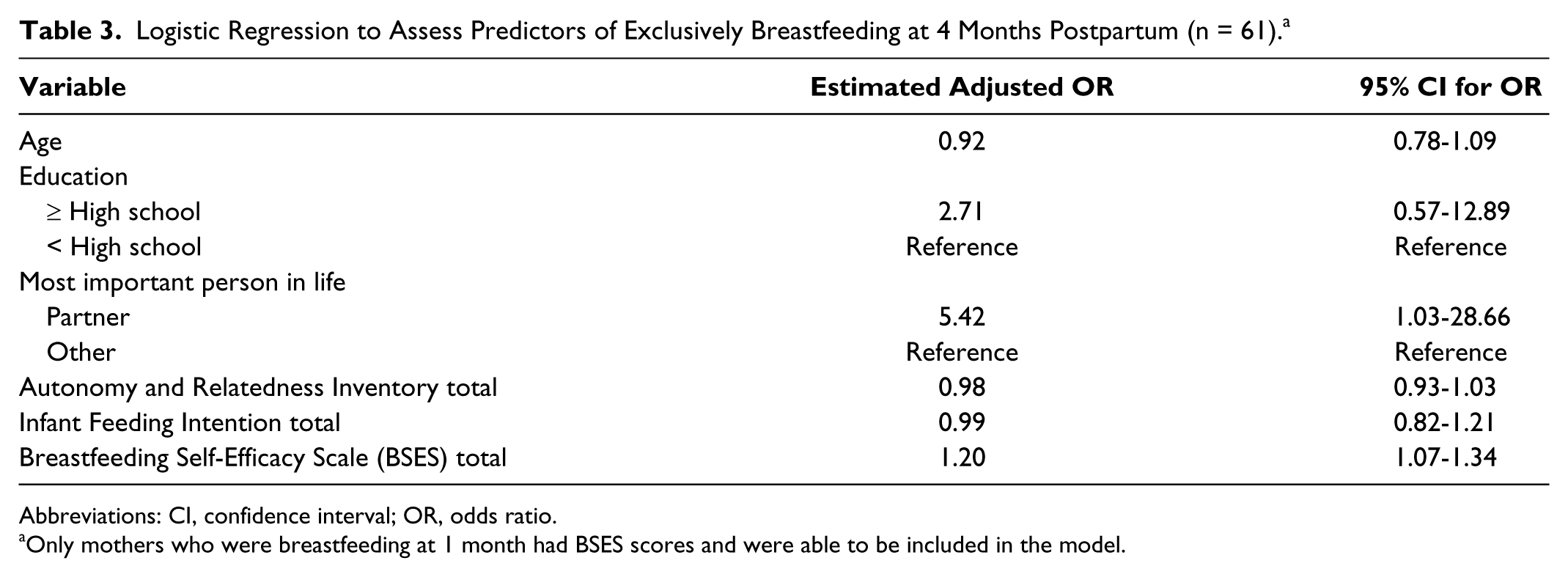
Abbreviations: CI, confidence interval; OR, odds ratio.
Only mothers who were breastfeeding at 1 month had BSES scores and were able to be included in the model.
Discussion
Hispanic mothers in this study were fairly homogeneous in demographic characteristics. The majority were Spanish-speaking Mexican immigrants living with a partner. Nearly all of the 72 mothers in this study were breastfeeding at discharge following the birth of their infant (94%), and half of these participants were EBF. This finding supports a Centers for Disease Control and Prevention (CDC) report that depicts Hispanic mothers as more likely to initiate breastfeeding compared with other ethnic groups. 4 However, by 2 months postpartum, the rate of EBF had dropped to 26% (from 50% at discharge), which is even lower than that reported from the CDC. 4 Furthermore, smaller declines occurred between 2 and 4 months among study participants (22%).
We found an inconsistency between the intention to EBF and the actual rate of EBF in these participants; when we asked about their intention to breastfeed during pregnancy, most obtained a high score on the IFI scale, which suggested their commitment to EBF their infants until 6 months of age.25,26 A higher IFI score was significantly associated with EBF at discharge and at 1 month and has been described extensively in our previous publication. 32 However, the relationship between IFI score and EBF status at 4 months was not significant. Perception of low milk supply was the most common reason to justify the introduction of formula among mothers who were EBF at discharge but introduced formula during the first 4 months. This study finding is consistent with previous reports that Hispanic women are likely to breastfeed their infants, but at the same time, they want to supplement with formula as they see formula as a good solution to breastfeeding difficulties.17,18,33-36
Among mothers who were EBF at 1 month, half were still EBF at 4 months, and the remainder were using at least some formula. While the comparison was not significant, there is preliminary evidence to suggest that breastfeeding self-efficacy at 1 month postpartum may be associated with successful continuation of EBF to 4 months postpartum, since mothers who continued to this time point had a higher BSES score than those who discontinued EBF between 1 and 4 months.
An important finding of this study was that among mothers who were breastfeeding at 1 month postpartum (whether EBF or combination feeding), the significant predictors of EBF at 4 months were whether their partner was the most important person and their BSES score at 1 month. One interesting finding was that when the partner was the most important person in the life of the mother, she was more likely to EBF; however, we did not get the same result if we substituted this variable with “living with partner.” This suggests that living with a partner may not be sufficient to support extended EBF; rather, it is the nature of the partner relationship that may be more of an influence. It has been described previously that Hispanic women, especially immigrants, have strong ties with family members, and the effect of close proximity and primary support may lead to consistently positive health outcomes. 37
Women with higher scores of BSES at 1 month were more likely to EBF at 4 months. This finding has particular relevance in this population, given the high rate of breastfeeding initiation coupled with the fact that breastfeeding self-efficacy is a modifiable factor. 21 This has important implications for interventions aimed at improving sustained EBF among Hispanic mothers. Interventions delivered worldwide that aim to increase self-efficacy are reported to be more effective than those that are limited to focusing on enhancing knowledge. 21 Another implication for practice is that Hispanic mothers who are breastfeeding at 1 month but who have lower scores on the BSES may have a higher risk of discontinuing EBF in the following months. This finding reinforces the recommendations for additional lactation support following discharge from the hospital since this may bolster the mothers’ confidence about their breastfeeding experience.38-42
Limitations of this study should be noted. First, not all potential factors that influence EBF were examined in our analyses; thus, our results may have residual confounding. Second, we used a convenience sample that limits the representativeness of the sample and thus the generalizability of results. We recommend caution in generalizing our findings beyond this area or to women who do not have similar characteristics. Finally, there is a limited sample size due to the omission of the 28 participants who were lost to follow-up by 4 months postpartum. The comparison of BSES scores between those who were still EBF at 4 months and those who had changed to another feeding type was based on only those who were EBF at 1 month. Further research in this area will benefit from a larger sample of mothers who are EBF at 1 month, as our study only had 26. In addition, we do have a significant logistic model that includes significant predictors. So while the power was lessened through the loss of dropouts, it remained at a high enough level to discern predictors of EBF at 4 months, including BSES.
Conclusion
In conclusion, our findings support that partner as the primary intimate relationship and breastfeeding self-efficacy at 1 month both influence EBF at 4 months in this group of Spanish-speaking Hispanic mothers. Support to Hispanic mothers during pregnancy and postpartum, including consultation with a lactation consultant, may increase the breastfeeding self-efficacy in this vulnerable population, leading to higher rates of extended EBF.
Footnotes
Acknowledgements
We thank Maria Gomez, DrPH, and Ana Machado, MPHc, for their valuable collaboration during the data collection process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Start Fund of the College of Nursing, University of Kentucky, and was awarded to Ana Maria Linares.