
Abstract
Background:
Implementing evidence-based practices and policies for breastfeeding support in community clinics is a promising, but challenging, approach to reducing disparities in breastfeeding rates.
Objective:
This study aimed to apply a policy process research framework to increase knowledge of factors that facilitate adoption and implementation of breastfeeding policy changes.
Methods:
In 2013, Washington State piloted a process to encourage 8 clinics to adopt and implement steps to become breastfeeding friendly. Evaluation data were collected through interviews, project reports, training evaluations, and pre– and post–self-assessments of achievement of the steps.
Results:
In 6 months, clinics increased the breastfeeding-friendly steps that they were implementing from a median (interquartile range) of 1.5 (0-3) to 6 (5-7). Improvements were most likely in the steps that required the fewest resources and administrative changes. Barriers to implementation included misperceptions about breastfeeding and breastfeeding support; lack of administrative “buy-in”; need for organizational changes to accommodate actions like monitoring breastfeeding rates and allowing providers training time; and the social-political climate of the clinic. Several factors, including actions taken by public health practitioners, enhanced the change process. These included fostering supportive relationships, targeting technical assistance, and providing resources for planning and training.
Conclusion:
This pilot project demonstrates that it is possible to make changes in breastfeeding support practices and policies in community clinics. Recommendations to enhance future work include framing and marketing breastfeeding support in ways that resonate with clinic decision makers and enhancing training, resources, and advocacy to build capacity for internal and external systems changes to support breastfeeding best practices.
Keywords
Well Established
Following recommended breastfeeding policies and practices in hospitals and clinics increases the number of women who choose to breastfeed and the length of time that women breastfeed. There are several barriers to implementing these policies and practices.
Newly Expressed
Applying the methods and frameworks of policy process research is a useful way to increase knowledge about the organizational, political, and systematic barriers and enhancers of adoption and implementation of recommended breastfeeding policies and practices in clinics.
Background
The mission of public health is to “assure conditions in which people can be healthy.” 1 For mothers and their infants, this includes assuring conditions in which mothers can initiate and sustain breastfeeding. Although breastfeeding initiation, duration, and exclusivity have increased over the past 20 years, there are still socioeconomic, racial, and ethnic disparities in breastfeeding rates. 2 Inequalities in access to and delivery of maternity care practices are associated with disparities in breastfeeding rates.3-10 A coordinated system of care through the preconception, pregnancy, and postpartum periods and policies that create supportive environments in birthing facilities, clinics, worksites, and child care settings could improve breastfeeding outcomes.11-18
Although evidence-based breastfeeding policies and practices are effective, they are not consistently adopted, implemented, or maintained.4,19 For example, supportive maternity care practices can eliminate racial and ethnic disparities in in-hospital rates of exclusive breastfeeding,5-10 but only 10.5% of babies in the United States are born in hospitals that are designated Baby-Friendly. 20 Many organizations have developed recommendations about optimal breastfeeding policies and practices,21-23 but there are challenges to meeting these recommendations. Lack of administrative buy-in, an unsupportive organizational culture, and lack of adequate human and financial resources interfere with best practices in hospitals.24,25 Gaps in provider education and training, unsupportive clinic culture, negative personal attitudes, perceived lack of time, and reliance on personal breastfeeding experiences rather than evidence-based protocols also interfere with effective breastfeeding care and services.26,27 Evidence-based breastfeeding policies are more likely to be implemented when there is strong commitment from management, funding, training, and ongoing monitoring of breastfeeding data.24,25,28,29 Most of what is currently known about adoption and implementation of breastfeeding policies and practices comes from studies in hospitals.
The Baby-Friendly Hospital Initiative 17 is well known for its global effect on hospital maternity services. Parallel programs have been initiated in community-based settings, including clinics that serve women before and after hospital discharge.30-32 Although Baby-Friendly approaches in clinics are associated with increased breastfeeding exclusivity and duration, 32 promoting policy and practice change in clinics has been challenging, and the adoption of Baby-Friendly community clinic policies has been relatively slow compared to Baby-Friendly hospital policies.30,31
The field of policy process research, the study of interactions among people and public policy, 33 offers tools and frameworks that can be applied to a comprehensive examination of the effect of factors that influence the implementation of recommended breastfeeding policies in many settings. The purpose of this article is to apply a policy process research framework to share what was learned about facilitating breastfeeding policy adoption and implementation in a pilot project led by state-level public health practitioners in partnership with 8 community clinics.
Methods
The Pilot Project
For 6 months in 2013, leaders from 8 community health clinics in Washington State, in the Pacific Northwest part of the United States, participated in the Breastfeeding-Friendly Community Health Centers pilot project. The initiative aimed to establish clinic environments that support breastfeeding by implementing research-based policies and practices identified for this project in the document, Ten Steps to Breastfeeding-Friendly Community Health Centers. 34 Although Washington State as a whole has high breastfeeding rates compared to the national average, 35 there are disparities in breastfeeding rates by race/ethnicity and income. 36 This initiative focused on clinics that serve populations that tend to have lower breastfeeding rates.
Through a competitive grant process, clinics applied to receive $30 000 in implementation funding, technical assistance, training, and resources to build local capacity to implement the evidence-based steps listed in Table 1. The 8 clinics chosen to receive funding were supported by a state-level team that included staff from the state health department and the state breastfeeding coalition. Clinic project teams participated in 3 training and networking meetings. Trainings were designed around learning objectives that included both affective (attitudes, values, motivation) and cognitive (knowledge, comprehension, application, analysis) learning domains. The primary goals of the first training were to introduce the project and its activities and review the evidence behind each of the 10 steps. The second meeting was focused on problem solving, networking, and billing for breastfeeding support services. The third meeting was open to all clinic staff and focused on building clinical skills for better breastfeeding support and management. State staff visited each clinic twice and provided ongoing technical assistance through phone calls and emails. Each clinic was provided with an implementation tool kit, provider pocket cards, and reference guides.
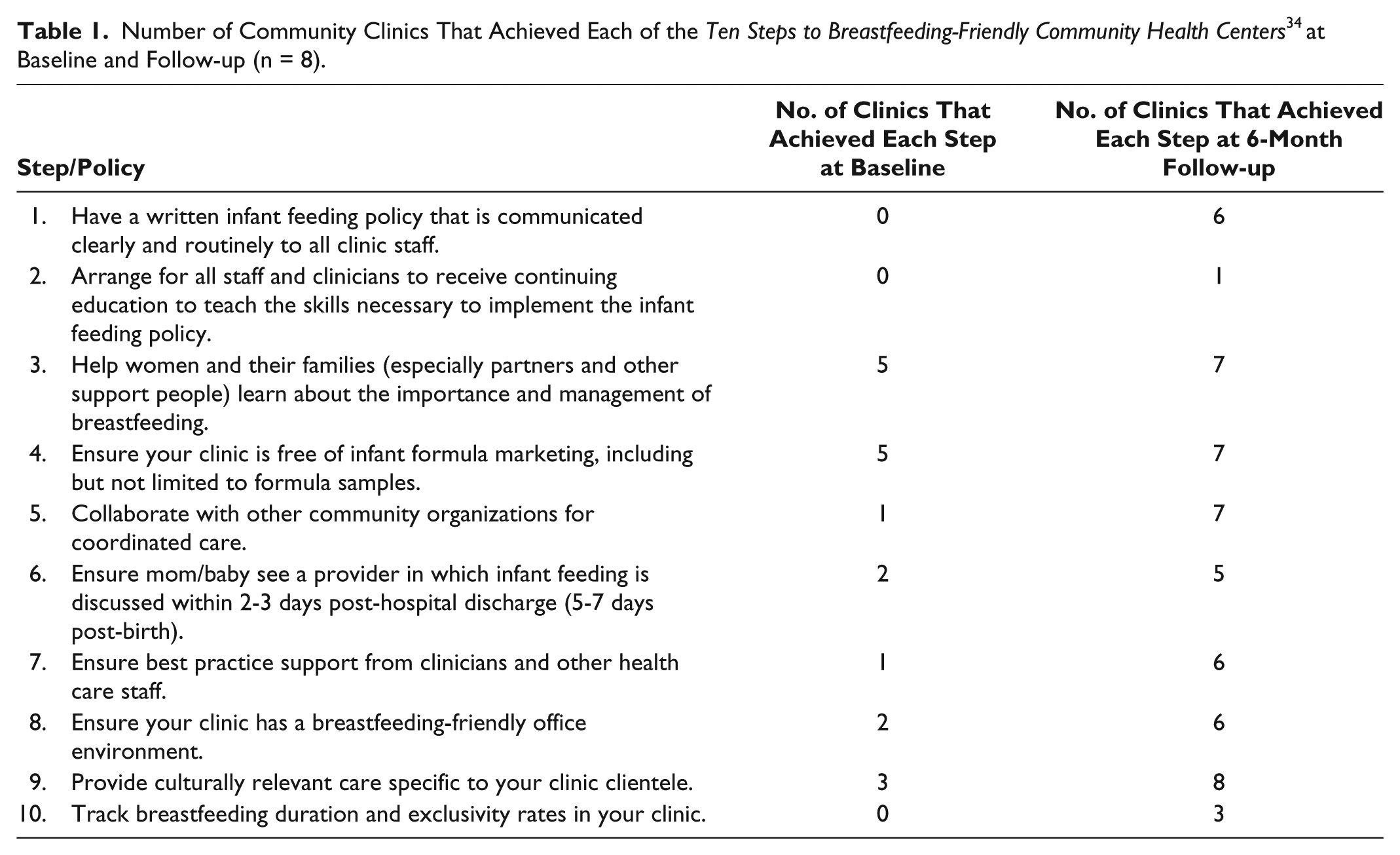
Number of Community Clinics That Achieved Each of the Ten Steps to Breastfeeding-Friendly Community Health Centers 34 at Baseline and Follow-up (n = 8).
The project’s short-term objectives were to increase clinic staff and provider knowledge, positive attitudes, and self-efficacy about breastfeeding management and the effect of clinic environments on breastfeeding success; the medium-term objective was to increase the adoption of best practices to build environments and practices to support breastfeeding in the clinics.
Data Collection and Analysis by the University Partner Evaluation Team
The purpose of the project evaluation was to build practice-based evidence for future efforts by the state-level team and others. Evaluation data included information obtained during 16 semistructured interviews with project leaders at each clinic (8 mid-project and 8 final), 16 project reports submitted by each clinic at 2 time points (mid-project and final), pre– and post–self-assessments of the status of the implementation of the Ten Steps to Breastfeeding-Friendly Community Health Centers, 34 and pre- and post-evaluations of training sessions.
The interviews were designed to capture information about the policy development process and outcomes and were completed, coded, and analyzed by 1 experienced university evaluation coordinator. Extensive notes were taken during each interview. A coding scheme was developed in concert with other experienced university research coordinators. Results were summarized by themes. The evaluation team augmented and triangulated thematic descriptors with information from reports and self-assessment documents.
The criteria for meeting each of the steps were developed by the state-level project implementation team and are described in detail elsewhere. 34 The self-assessment document and corresponding scoring system allowed clinics to assess their implementation of each step. The clinics completed the self-assessment on their own, and the implementation team assigned the score. 34 The scoring system was designed to make a simple pass/fail determination. For example, to achieve step 2, provider training, at least 80% of providers must have received at least 5 hours of continuing education in breastfeeding management within the previous 5 years; only providers who interact with mothers and/or infants are included in this calculation. To achieve step 5, community collaboration, the clinic had to identify at least 3 organizations with which they collaborate; organizations had to include “WIC” (the Special Supplemental Nutrition Program for Women, Infants, and Children) and a “local birthing hospital.”
For the in-depth training about breastfeeding, training evaluation was based on questions used in earlier studies about breastfeeding knowledge and attitudes.37-39 These were asked before and immediately after the training session. Six weeks following the training, participants were asked again to answer questions about actual changes that had been made to attitudes, practices, and policies.
Analytical Framework
Because the process of working with organizations to implement changes to policies and practices is dynamic and complex, evaluators applied an existing framework to guide the analysis. The framework developed by Greenhalgh et al, 40 Diffusion of Innovations in Service Organizations, is based on a systematic review of diffusion of innovation literature and incorporates widely cited diffusion of innovation theory. The framework has been used to analyze the implementation of policies for electronic health records, integrated care pathways, and telemedicine. 41 The application of this framework supports an analysis that considers the effect of 9 influences on adoption, implementation, and sustainability of policies and practices. In this case, the first model component, the “innovation” to be diffused, was the adoption of the Ten Steps to Breastfeeding-Friendly Community Health Centers. 34 A second component of the framework is the characteristics of the adopters including their needs, motivations, values, goals, skill levels, learning styles, and social networks. The third component involves the nature of communication and influence, such as messages conveyed about the innovation, communication networks, and the main agents of influence. Fourth, the framework accounts for a variety of system antecedents such as size, maturity, and level of decentralization. The framework separates the concepts of an organization’s readiness for innovation from its receptivity and defines system readiness as component 5. The sixth component, assimilation, addresses the aspects of the wider organizational context and processes and the degree they would need to adapt to accommodate the innovation. The seventh component, implementation, addresses the implementation and maintenance process in terms of planning, resources, and management. The eighth component, “outer” context, relates to the prevailing economic and political context, funding, and the influence of similar organizations. The framework proposes in the final, linkages component that the intersection and integration of these components are critical to success.
Using the criteria of the University of Washington Institutional Review Board, this study was exempt from institutional review board approval because data were collected as part of program evaluation and consisted of “fact collecting interviews of individuals where questions focused on things, products, or policies” rather than research subjects.
Results
Sample
Four of the 8 clinics are in the eastern part of the state, and 4 are in the western part; clinics serve both urban and rural areas. Four clinics are associated with Native American tribes and 4 serve primarily Hispanic families.
Training Outcomes
Tables 2 and 3 provide a comparison of quantitative pre- and post-training assessment results. Overall, higher proportions of participants reported positive attitudes and correct knowledge after the training than before. In addition to these quantitative data, in response to an open-ended post-training evaluation question, attendees provided a long list of positive changes that they planned to put in place in their interactions with individual patients after the training; none listed any changes they hoped to make to their clinic environments. In response to another open-ended question about the most valuable and interesting topics from the training, some attendees highlighted learning about the importance of having everyone who works at a clinic or hospital trained and engaged in breastfeeding support.
Pre- and Post-Training Assessment of Breastfeeding Attitudes, Values, and Knowledge of Providers and Staff from 8 Community Clinics.
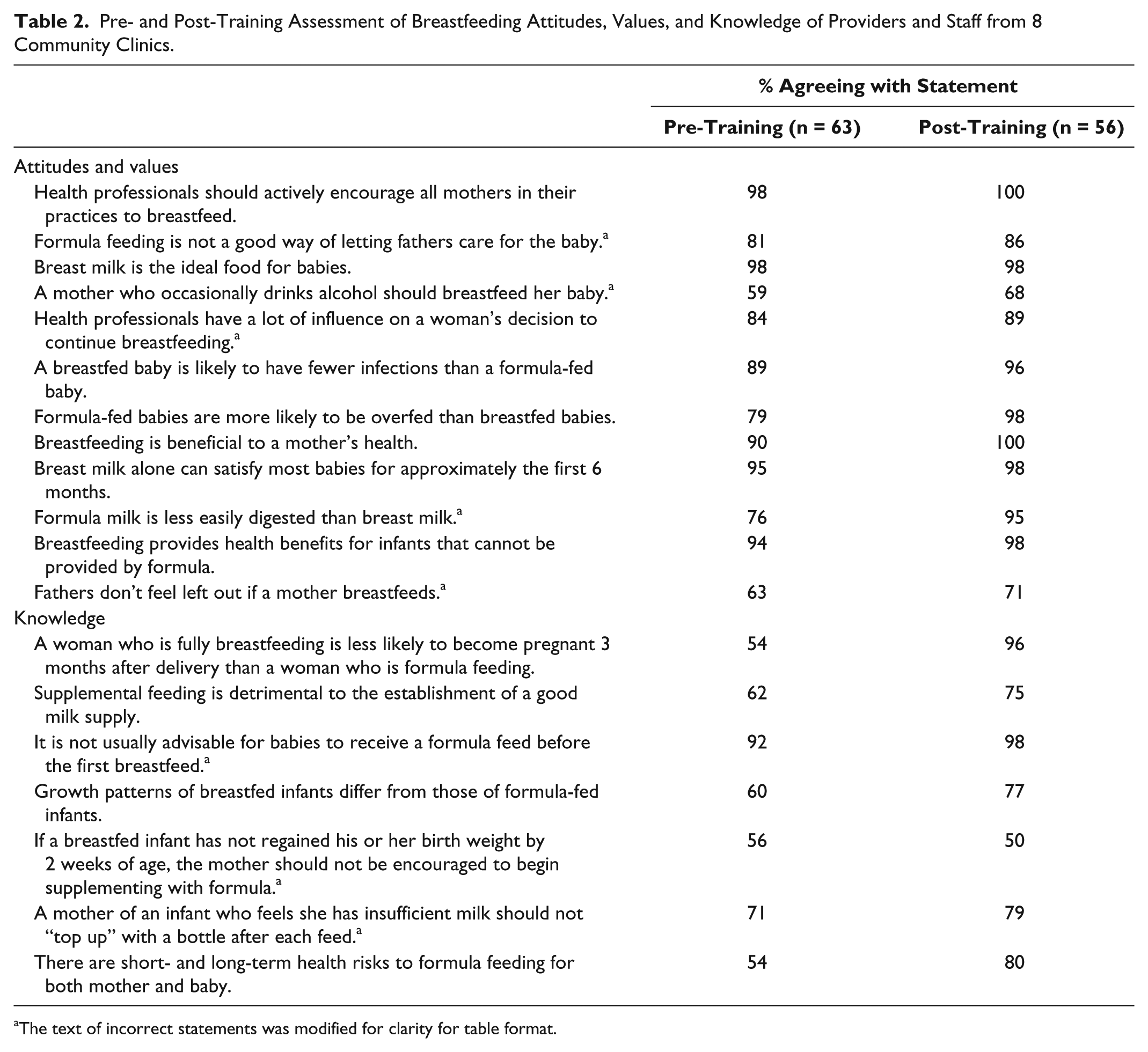
The text of incorrect statements was modified for clarity for table format.
Pre- and Post-Training Assessment of Breastfeeding Practices of Providers and Staff from 8 Community Clinics: Proportions of Respondents Who Indicate That They Are Following Recommended Practices to Support Breastfeeding.

Abbreviation: IBCLC, International Board Certified Lactation Consultant.
Recommended practice.
Policy Outcomes: Achievement of the Breastfeeding-Friendly Community Health Center
As Table 1 shows, the clinics achieved substantial changes in breastfeeding policies and practices. Clinics increased the number of steps they had in place from a median (interquartile range) of 1.5 (0-3) clinics per step to 6 (5-7). Whereas the clinics had variable experiences, most found that some environmental changes such as putting culturally appropriate posters in clinic spaces were easy to do, especially with the extra grant resources. The challenges came with the implementation of steps that required a commitment of time and resources from the clinics’ administrative systems. For example, most clinics were unable to accurately use existing clinic information systems to assess the proportion of postpartum women who were breastfeeding. Breastfeeding training for clinic staff and providers was hampered by challenges associated with busy clinic schedules and the lack of reimbursement for provider hours spent in training.
Barriers and Enhancers of the Project Process
Table 4 provides a short summary of the factors associated with each component of the Diffusion of Innovations in Service Organizations Framework. 41 There were general factors, as well as factors intrinsic to each clinic, that facilitated or slowed the process. The idea of changing policies and practices to support breastfeeding was challenging for some providers and staff who had limited experience with thinking about the importance of environmental change to supplement their usual clinical practice, but breastfeeding policy change was easier to accept when it was framed to align with the values and mission of the clinic and community. On an individual level, staff and providers were motivated to either oppose or champion the policy changes based on their personal experiences or perceptions of what was right for the clients. Organizational issues played a major role in policy implementation; strong favorable leadership, positive communication, and the institutionalization of the policies so that they would survive staff turnover contributed to the success of the initiative. Systems-level issues included resources, staffing patterns, and the perception that breastfeeding did not need to be a focus of clinical care since it was taken care of by staff from WIC. The sociopolitical context in the community outside the clinic and relationships with community providers and hospitals influenced the ability of the clinics to achieve some of the recommended policies and practices; some clinics were highly motivated by building a reputation as a breastfeeding-friendly facility and a good place to go for breastfeeding support.
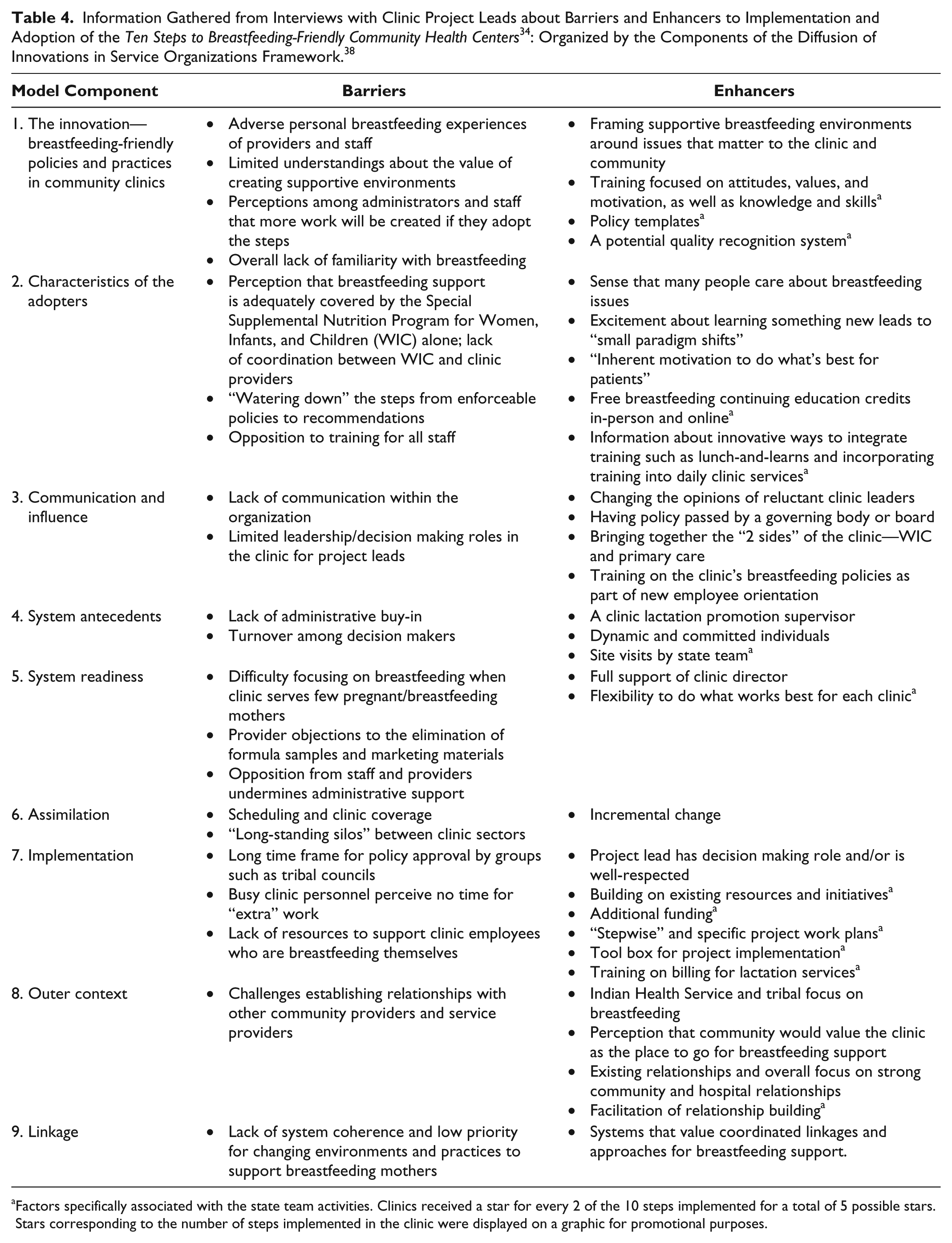
Factors specifically associated with the state team activities. Clinics received a star for every 2 of the 10 steps implemented for a total of 5 possible stars. Stars corresponding to the number of steps implemented in the clinic were displayed on a graphic for promotional purposes.
As shown in Table 4 in bold, clinic leaders were able to identify several actions taken by the state project team that enhanced the local process. These included training that integrated experiences designed to address values, attitudes, and beliefs; piloting a system that may eventually be used to promote clinics as breastfeeding friendly; providing materials, such as a tool kit for implementation strategies, policy templates, and clinical guides; and technical assistance.
Discussion
The Breastfeeding-Friendly Community Health Centers pilot project demonstrates that it is feasible to promote evidence-based best practices and policies for breastfeeding support in community clinics as a public health intervention. Given previous studies in hospital settings,5-10 public health practitioners could reasonably consider the promotion of breastfeeding-friendly community clinics as a promising approach to reducing breastfeeding disparities. In this evaluation, the barriers to policy change in community clinics were similar to those previously found in hospitals—limited support from administrators, issues associated with organizational culture, and too few resources.24,25 Enhancers of policy change were also similar. In both settings, it is clear that the support of leaders and administrators is crucial. 24 In clinic settings, the potential to market the clinic as breastfeeding friendly was motivating to many administrators; the situation in hospitals is unclear. 28 In hospitals, training of all staff is considered an important component of implementing changes in breastfeeding policies and practices. 24 In community clinics, training also appeared to be a necessary component, but training alone was insufficient to promote institutional policy change; a combination of approaches was required.
The Diffusion of Innovations in Service Organizations Framework 41 is a useful way to analyze the process of implementing changes to breastfeeding policies in community clinic settings and complements previous work that has applied a diffusion of innovation model to provider-level breastfeeding interventions in clinics. 27 Across the model components, the framework helps to identify opportunities for addressing important elements of policy adoption and implementation. For example, of the 10 potential steps that could have been implemented by each clinic, the steps most likely to be implemented were those that reflected the best fit with existing systems and values and an incremental approach, as well as those for which there were available resources.
The framework was also a useful way to analyze why and how the actions that were taken by the state-level team were perceived as helpful and to gauge how comprehensive the state team’s actions were. For example, training that addressed affective learning domains such as values and motivations helped to build positive perceptions that the “innovation” was in tune with the values of the clinics and the clinics’ missions to care for underserved families. Training about billing for breastfeeding services helped clinics to perceive some of the policies and practices as administratively feasible. In addition, staff and providers from the community clinics highly valued the work of the state team to create opportunities to network and discuss challenges, develop solutions, and share successes. It is likely that the same success would not have been achieved if each clinic had attempted to make these changes on its own.
In this pilot, some framework areas received more attention than others. For example, there was a great deal of emphasis on the actual implementation of the project and not as much emphasis on the effect of the outer context on institutional change. In future initiatives, it may be helpful to consider a greater focus on things like system readiness or the outer and/or organizational context for assimilation. This project was completed in a very short period of time in the clinics—less than 6 months. With a longer time for the policy process, care could be taken to assess the policy beliefs and values of the “policy actors” in each setting and base the initial project activities on the context of each unique clinic setting.
Limitations
This case study approach in a nonrepresentative sample of community clinics has limitations, and results are not necessarily generalizable. Within the small sample size, limited study time, and the complexity of service-level innovations, it is not possible to make quantitative connections between the actions taken by the state-level or local teams and specific achievements of “steps” at each clinic. There is value, however, in theory-driven evaluation and reflection and the practice-based evidence that can be derived from this experience. It is important to continue to build and share this evidence about what works.
Another limitation is that clinic compliance with the 10 steps was self-reported via the self-assessment tool. It is possible that clinics biased their responses in favor of their own performance.
Recommendations for Research
This pilot evaluation found that it is feasible to change some breastfeeding policies and practices in community clinics in a short period of time and identified several factors that appear to facilitate the process. Given that breastfeeding policy change in community clinics is effective, 32 but “not easy,” 30 policy process research methods could be applied across a larger set of clinics and other settings to further build knowledge about the process of implementing breastfeeding- friendly policies. These findings could then be applied to the design of an intervention/control study that could compare changes in policies, practices, and breastfeeding outcomes in community clinics that have an opportunity to collaborate with state teams and each other to implement clinic changes with control clinics that do not have access to these resources. The results of these studies could provide much needed evidence to support the work of public health practitioners who seek to assure conditions in which mothers can initiate and sustain breastfeeding.
Recommendations for Future Initiatives in Community Clinics
This analysis supports recommendations that fall into 2 broad categories: (1) to position and frame breastfeeding policies and practices as part of a holistic system to make it easier for the populations served by community clinics to adopt health-promoting choices; and (2) to build state-level public health agency capacity to support breastfeeding- friendly community clinics.
Breastfeeding policy change can be framed and marketed to key decision makers in ways that address the goals and values of the clinic and community. For example, community clinics have a mission to improve the health of the vulnerable populations they serve; increasing community breastfeeding rates is 1 way to reduce inequalities and improve population health. Frontline staff is important, but for sustainable breastfeeding policy change, it is essential to reach key decision makers–clinic administrators/managers, tribal and community leaders, physicians, and other providers.
Training is important, but training alone is not enough to sustainably change breastfeeding policies and practices. Systems changes are necessary at all levels to address issues like the technology needed to monitor breastfeeding rates, finding ways to pay for provider time for training, and assuring that breastfeeding is perceived as “a public health concern and not just a lifestyle choice.” 22 Incentive systems that clinics can use to highlight their breastfeeding-friendly status appear to be a promising practice.
At the state level, agencies should strategically plan and budget for activities needed to build and maintain long-term relationships across and between agencies and community clinics. For a medium-size state like Washington, this kind of challenging policy initiative across diverse community clinics and over a large geographic area could be best supported by 2 professional staff with public health training to plan, lead, and assure quality, plus additional resources to bring together breastfeeding experts and clinic staff for initial and ongoing training and technical assistance. Important components of such an initiative include descriptions of best practice steps, project tool kits for implementation strategies, and templates for work plans. Training that is facilitated by state agencies should focus not only on how to clinically support and troubleshoot breastfeeding but also on how and why to make breastfeeding policy changes. This training should be extended beyond individual clinic providers to administrators and other decision makers.
Conclusion
It is possible to make changes in breastfeeding practices and policies in community clinics that serve racially, ethnically, and economically diverse families. Public health practitioners can provide training, technical assistance, planning tools and resources, and opportunities to network so that community health clinics can continue to improve conditions that make it easier to breastfeed.
Footnotes
Acknowledgements
The authors wish to acknowledge the dedicated administrators, staff, and families of the community clinics who participated in this initiative and the foresight and leadership of the Washington State Breastfeeding Leadership Group and Breastfeeding Coalition of Washington.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by a cooperative agreement from the Centers for Disease Control and Prevention (CDC) RFA-DP08-8050501PPHF12. Its contents are solely the responsibility of the authors and do not necessarily reflect the official views of the CDC, the Department of Health and Human Services, or the federal government.