
Abstract
Background:
Lactating women in the United States have several options for what they do with excess breast milk, including donating to milk banks that serve medically fragile infants, sharing directly with families seeking milk, and selling to individuals or for-profit entities. The World Health Organization and the US Surgeon General have issued calls to increase access to pasteurized donor milk for medically fragile infants.
Objective:
To explore how lactating women with a surplus of breast milk come to the decision to share their milk with a peer rather than donate to a milk bank.
Methods:
A qualitative design using a grounded theory approach was employed. Semistructured telephone interviews were conducted with 27 women who had shared milk with a peer but not with a milk bank.
Results:
Five dominant themes were identified: a strong belief in the value of breast milk, unexpected versus planned donation, sources of information regarding milk exchange, concerns and knowledge gaps about milk banks, and helping and connecting.
Conclusions:
This research offers insights into potential strategies for promoting milk bank donation among peer-to-peer milk sharers, including developing donor education campaigns focused on knowledge gaps regarding milk banks and developing health care professional referral programs that can reduce barriers associated with the convenience of milk bank donation.
Well Established
Lactating women who share breast milk with a peer are motivated to do so because they place a high value on human milk, often have an unplanned excess of milk, and value helping others.
Newly Expressed
Peer-to-peer milk sharers in the United States learn about methods for exchanging milk through their social circles, not health care providers. Many misconceptions about milk bank costs are barriers for donating to a milk bank.
Background
While sharing human milk has been practiced for centuries, 1 the banking of human milk got its start in the early 20th century as technologies advanced to improve milk collection and storage.2,3 Today, women have choices for what they do with their excess milk, including sharing within their social circles, donating to nonprofit milk banks, 4 selling milk to individuals or for-profit entitites,5-7 and sharing milk via Internet-based communities that facilitate a connection between milk seekers and milk donors.8,9 In this article, terms will be used as follows: sharing refers to the commerce-free exchange of milk between individuals, donating refers to the commerce-free exchange of milk between an individual and an organization (eg, milk bank), selling refers to the compensated exchange of milk with an individual or an organization, and exchange is collectively used to describe methods of sharing, donating, and selling human milk.
Various organizations, including the World Health Organization, 10 the US Surgeon General, 11 and the American Academy of Pediatrics, 12 have issued calls for the safe use of donor milk with preterm infants; therefore, understanding the various channels of human milk exchange is important for creating strategies to support these initiatives. In 2010, over 500,000 infants were born prematurely in the United States, and 15 million children were born prematurely worldwide. 13 Mothers of preterm infants have been shown to have an increased risk of inadequate milk production compared with mothers of full-term infants.14,15 Donor human milk, which has been screened, pasteurized, and dispensed by milk banks, is critical for preterm infants when they do not have access to their mother’s milk, improving health outcomes and reducing costs.16,17 Recent studies in the United States have reported that less than half of neonatal intensive care units (NICUs) are using pasteurized donor milk (PDM).18,19 While donations to the Human Milk Banking Association of North America (HMBANA) milk banks have been steadily increasing, 20 these data suggest that significant growth must continue to provide PDM to all NICUs in the United States.
Awareness of milk exchange among lactating women in the United States appears to be widespread, with a 2014 study of 499 postpartum women in Ohio reporting that 77% were aware of milk exchange, 25% had considered participating in milk exchange, and 4% had exchanged milk with family, friends, or a milk bank. 21 The demographic characteristics of women who exchange breast milk have been explored in a few studies. In a large online survey of milk sharers in the United States, most women were married (94.7%), non-Hispanic white (90.8%), college-educated (71.1%), and employed (57.4%). 22 Osbaldiston and Mingle 23 found similar demographics in a study of donors to a nonprofit milk bank in Texas, suggesting that milk banks and peer-to-peer milk sharing networks draw from similar, privileged populations in the United States.
Research into the motivational factors and experiences of mothers who have shared or donated breast milk suggests that these women place a high value on breast milk for infant feeding.24-27 In Brazil, 28 France, 29 and the United States, 23 women who donated to a milk bank cited similar top reasons for donating: the desire to help others and having too much milk. Similarly, mothers who shared milk via online peer-to-peer websites described wanting to help and having excess expressed milk as top reasons for sharing their milk. 24 A survey administered to 737 Brazilian milk bank donors found that the encouragement of health care professionals (25.8%) and information they received in the hospital (49.9%) were top influencers for donating. 30 In contrast, a study of 87 milk bank donors in the United States found that only 14% learned about being a milk bank donor from health care professionals, and 3% received information from a health care facility. 23
A 2013 international study of women who shared milk in peer-to-peer arrangements facilitated by the Internet found the top reason women did not donate to a milk bank was because mothers believed they lacked the opportunity to do so, the most common explanation being the absence of a local milk bank. 31 In the United States, many HMBANA milk banks cover the costs of transporting milk from an out-of-town donor; therefore, women do not likely lack the opportunity to donate even in the absence of a local milk bank. Studies that have quantified the volume of milk shared in peer-to-peer arrangements have found that volumes are often in excess of 100 oz,22,31,32 which is the minimum requirement to be able to donate to many HMBANA milk banks. A survey of 661 peer-to-peer milk sharers found that 89.3% had never donated to a milk bank (unpublished results). In terms of milk supply, these data suggest that peer-to-peer donors may be a potential population that could help increase the supply of PDM milk available for medically fragile infants.
The primary purpose of this study is to explore how mothers in the United States with a milk surplus come to the decision to share their milk with a peer rather than donate to a milk bank. To this end, we examine peer-to-peer milk sharers’ beliefs about milk banks and milk bank donation, their knowledge of other exchange options, and sources of information regarding various forms of milk donation.
Methods
A qualitative design was used to explore the experiences of peer-to-peer milk sharers using a grounded theory approach. 33 The study population consisted of peer-to-peer milk sharers who had participated in a large, population-based online survey about milk-sharing practices and had volunteered to participate in follow-on interviews (N = 342). 22 The current study sample was purposively selected and stratified to provide variability in socioeconomic status, education level, and race/ethnicity where possible. Criteria for selection included that the participant had shared milk with a peer but never donated to a milk bank and that the participant resided in the United States. Invitations to participate in the study were sent via email to qualified participants in groups of approximately 10 participants per invitation, to ensure that interviews could be scheduled and completed in a timely manner. Over the course of the study, a total of 46 participants were invited to participate, and 28 women (60.9%) agreed to be interviewed.
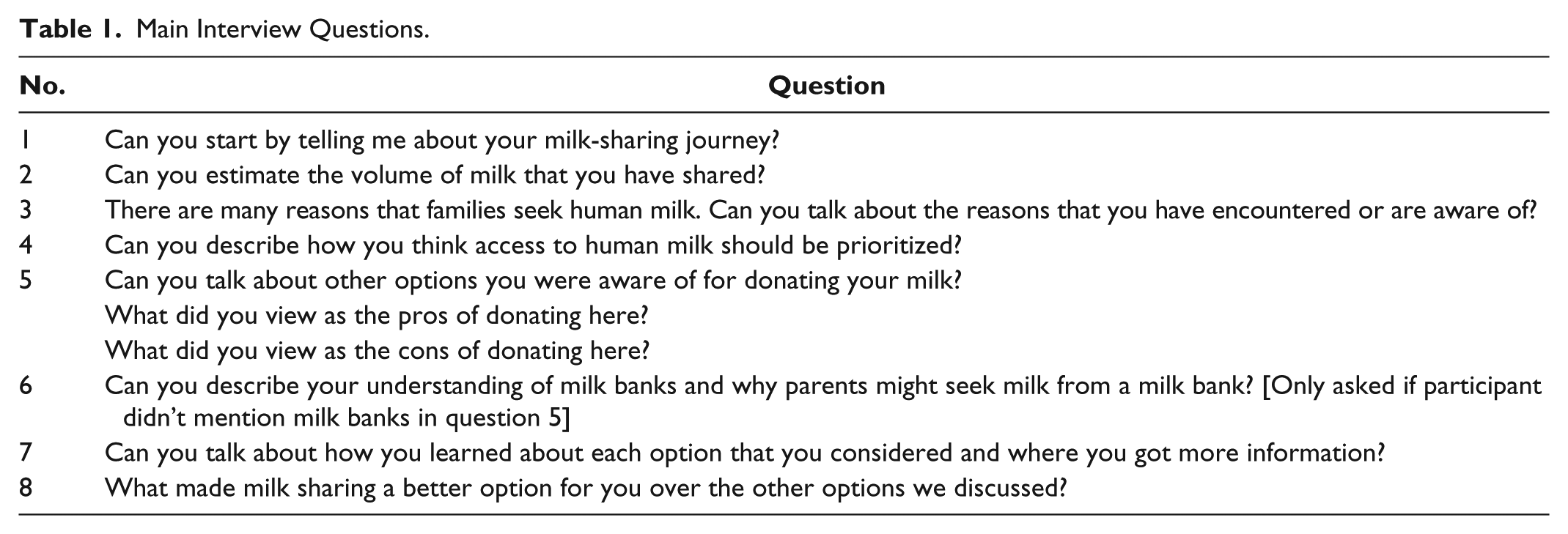
Semistructured telephone interviews were conducted between January and April 2014 by the first author, using the questions in Table 1 as a guide. Informed consent was obtained verbally at the start of each interview. Interviews lasted between 23 and 75 minutes (mean, 41.6 minutes; median, 41 minutes) and were digitally recorded for analysis. Audio files of the interviews were transcribed verbatim by 4 trained research assistants, and initial analysis was completed for each transcribed interview by the research assistant and the primary researcher to begin to identify emerging themes. Constant comparison of interviews was used throughout the process to guide both the evolution of the interview questions and the theoretical sampling strategy. 34 For example, after noting that social circles were described as a primary source of milk-sharing information, a new probe was added to the moderator guide at the ninth interview to explore the role of the health care providers as a source of milk-sharing information. Theoretical saturation was reached when no new themes emerged from the initial analysis. A retrospective review of the initial analysis themes suggested that saturation occurred at the 11th interview; therefore, further recruitment was stopped and the remaining scheduled interviews were conducted to compare and validate initial findings. One participant was excluded from our analysis because of poor audio quality, resulting in a final sample of 27 participants.
Main Interview Questions.
A preliminary coding manual was developed by the primary researcher and revised based on input from 2 of the research assistants who had participated in interview transcription and initial analysis. To test the coding manual, all 3 researchers performed independent line-by-line coding on a single transcript. The coding manual was further revised based on the research team’s consensus for the understanding and utilization of codes. All remaining transcripts were independently coded in duplicate; the primary researcher coded all transcripts, and 2 research assistants each coded half of the transcripts. Discrepancies were resolved via discussion and consensus. 34 Once coding of all transcripts was complete, the primary researcher analyzed the coded transcripts to identify dominant themes, which were reviewed and validated by other members of the research team.
Several steps were taken to increase the trustworthiness of this study 35 : member checks were done throughout the interview process, the research team included individuals with no prior experience in lactation and milk sharing to balance the primary researcher’s perspectives as a mother and a nutrition scientist who studies donor milk, and debriefing was completed throughout the project with qualitative researchers not involved in the data collection process. This study received ethical approval from the Elon University Institutional Review Board. All names in this manuscript have been changed to protect participants’ identities.
Results
Demographics and Milk-Sharing Activities
Overall, milk sharers included in this study were predominantly white, well-educated, middle-income, and married, which is similar to the characteristics of US mothers with higher breastfeeding rates. 36 Table 2 provides summary demographic data and milk-sharing characteristics. Participants shared their milk with a range of 1 to 8 recipients, and all participants shared a minimum of 100 oz of breast milk. Most participants (17/27) had shared their milk with someone they connected with on an Internet-based milk-sharing website, but participants reported a variety of other methods for sharing milk, including with friends (11/27) and with members in their moms’ groups (10/27).
Demographic and Milk-Sharing Activities (n = 27).
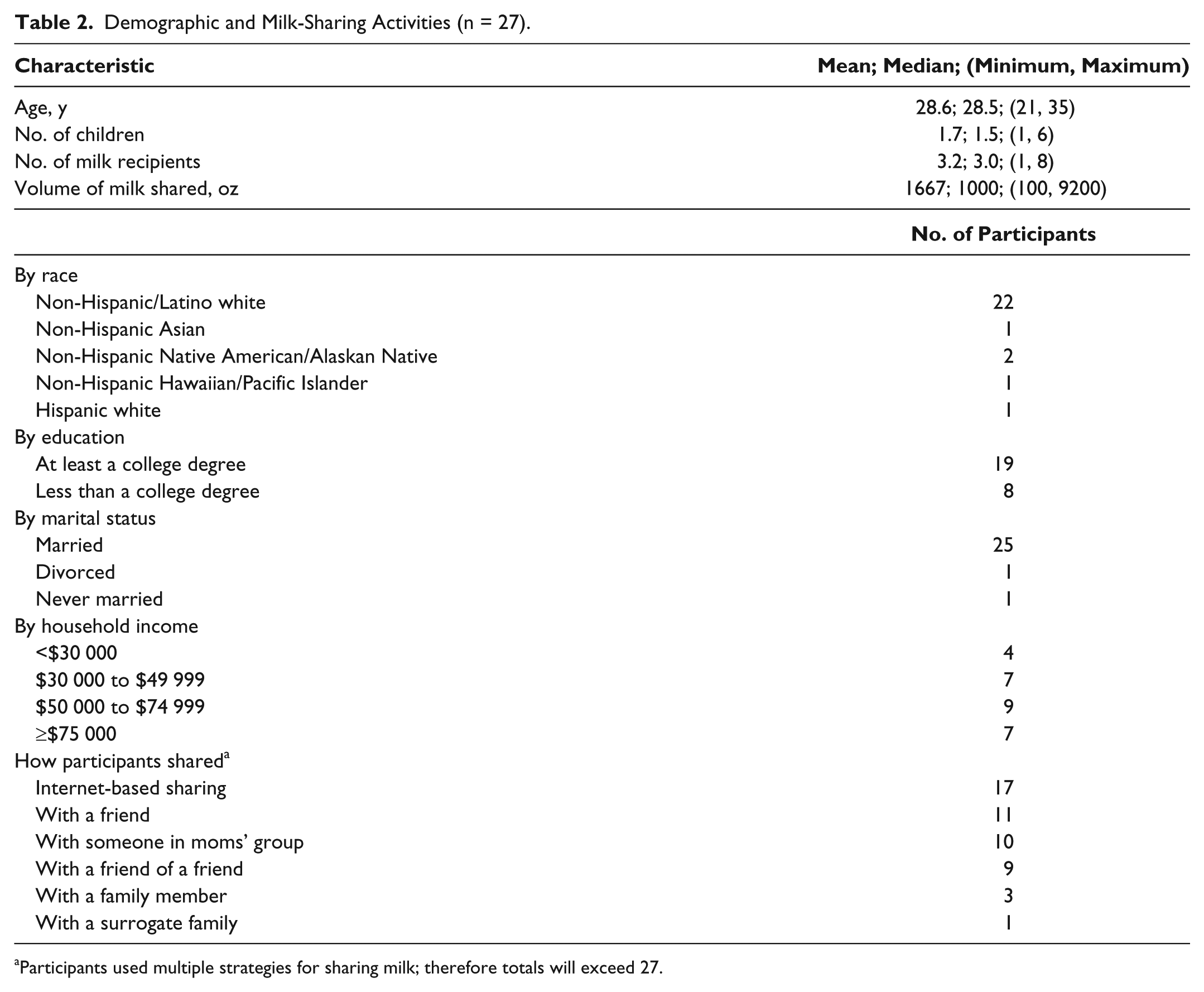
Participants used multiple strategies for sharing milk; therefore totals will exceed 27.
The Process of Becoming a Peer-to-Peer Milk Sharer
Five dominant themes emerged in participants’ stories of their peer-to-peer milk-sharing journeys: (1) a strong belief in the value of breast milk, (2) unexpected versus planned donation, (3) sources of information regarding milk exchange, (4) concerns and knowledge gaps about milk banks, and (5) helping and connecting. Table 3 provides representative comments that illustrate these themes.
Dominant Themes and Representative Comments. a
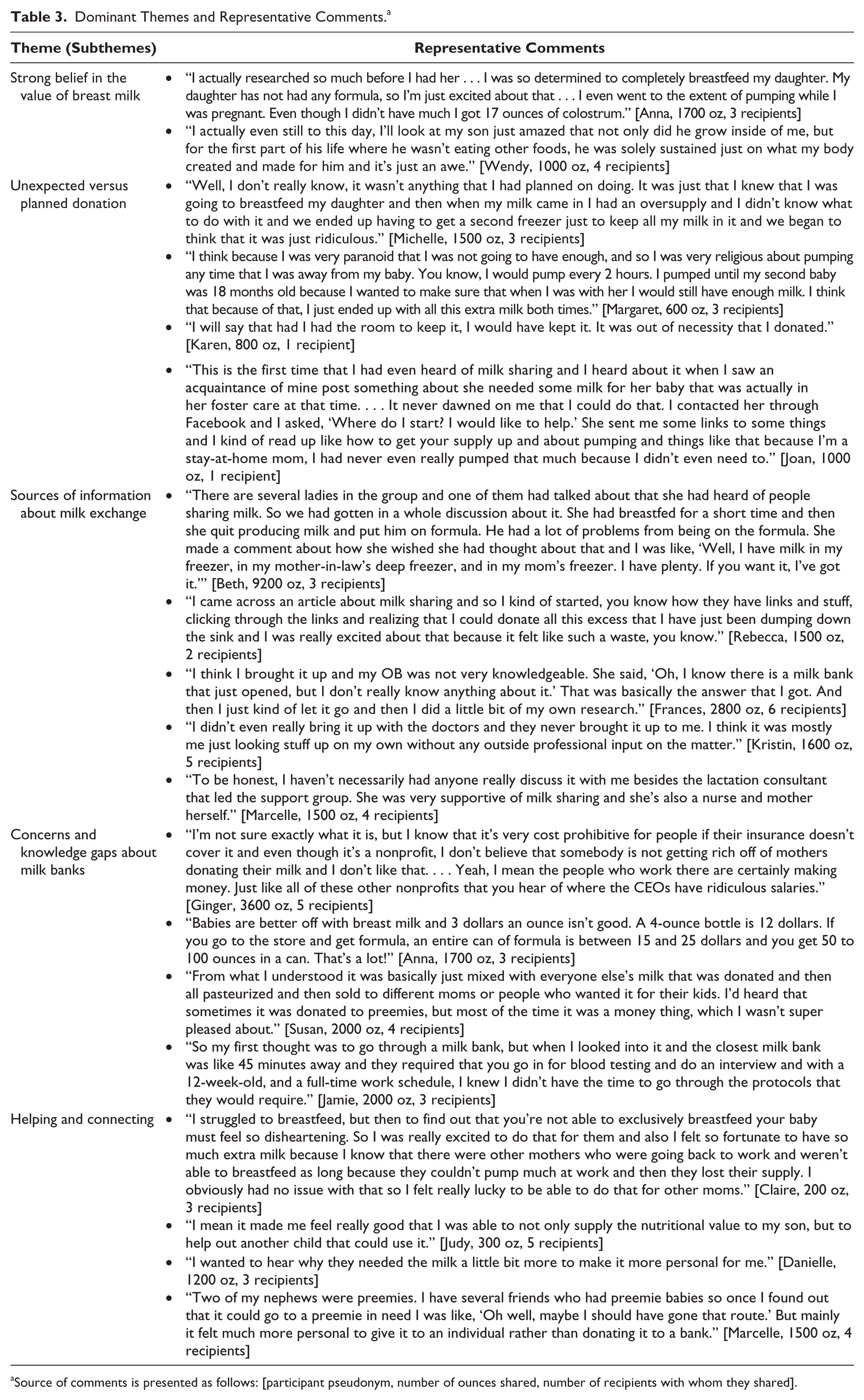
Source of comments is presented as follows: [participant pseudonym, number of ounces shared, number of recipients with whom they shared].
Strong belief in the value of breast milk
Peer-to-peer milk sharers verbalized a common belief in the value of breast milk that was illustrated by their actions, attitudes, and emotions. They described persevering through major breastfeeding challenges to continue to provide milk for their child, purchasing extra freezers so they would not have to throw away their milk, and devoting extensive time and energy to pumping milk. This act of valuing human milk provides a foundation for why women shared their milk with others.
Unexpected versus planned donation
Most participants did not set out intentionally to share their milk. Instead, a full freezer that resulted from regularly pumping their milk is what prompted many women to look into ways to give their milk away. Mothers described expressing milk for a variety of reasons, including employment, lactation problems, separation from child due to custody arrangements, and oversupply. For a few mothers, pumping was primarily motivated by a fear that they would not have enough milk. The ability to provide breast milk was a very important aspect of motherhood for these women, and expressing milk consumed significant physical and emotional time. The high value women placed on their milk made throwing the milk away an unacceptable alternative, and some even expressed reservation in sharing milk with others, lest they might need it in the future. A small number of participants began to pump their milk intentionally to share, either because they knew someone who was seeking milk or because they had been on the receiving end of milk donation for their own sick child and wanted to give back in a similar way.
Sources of information regarding milk exchange
Most participants learned about the various options for exchanging human milk from their social circles, including friends, family members, mother support groups based on common interests (eg, cloth diapering, baby-wearing, breastfeeding), and online resources. Participants described a wide variety of methods for exchanging human milk of which they were aware, including wet-nursing, for-profit and nonprofit milk banks, online milk-sharing websites, and websites for selling milk. Most participants reported that they received no information about milk exchange options and considerations from health care professionals. Sometimes this was because health care professionals were not knowledgeable when participants asked, and other times this was because participants chose not to share their questions and intentions with their health care professionals. Conversations about milk exchange that were initiated by health care professionals were rare, but when they did happen, it was most often initiated by a midwife, doula, or lactation consultant.
Concerns and knowledge gaps about milk banks
Knowledge about milk banks varied across participants, with some women familiar with the screening process to become a donor, as well as who milk banks primarily served, and other women having little information about these topics. The biggest source of concern about donating to a milk bank was the fact that milk banks charge for the screened and pasteurized milk. When probed further about their understanding of milk bank costs, beliefs varied and included the following: milk banks profit from the sale of milk, individual families bear the financial burden of obtaining PDM, and the cost of PDM is significantly greater than the cost of infant formula, which suggests the use of a “food for a healthy infant” framework to compare the cost structure of these 2 products. When probed about differences between nonprofit and for-profit milk banks, many participants were unaware that both nonprofit and for-profit milk banks exist. Danielle, who had received a flyer about breast milk donation to Milkin’ Mamas, a for-profit affiliated milk bank, said she was not aware of distinctions between for-profit and nonprofit milk banks, which may contribute to the concerns that organizations are profiting from milk donations. Several participants were also concerned with the work involved in becoming a milk bank donor (getting screened, adhering to milk-collecting protocols, shipping the milk) and the partial destruction of milk during pasteurization.
Helping and connecting
Milk sharing was viewed as a way of helping, with some participants focusing on the recipient infant and others focusing on the recipient mother. Women who described peer-to-peer sharing in the framework of helping other mothers often referenced their own personal struggles with breastfeeding as something that allowed them to relate to the situation of families seeking milk. Most participants expressed a belief that human milk was important for medically fragile infants, even if that is not with whom they shared their milk. Some participants valued connecting with the families that they were helping, which made the process more personal. They felt this personal connection would be lacking if they donated to a milk banks.
Discussion
This study provides new evidence regarding how women in the United States come to the decision to share expressed breast milk with a peer instead of donating to a milk bank. Major findings include the absence of health care providers as a source of information about milk exchange and misconceptions about milk bank costs that are major barriers for donating to a milk bank.
We found that women who share milk in peer-to-peer arrangements place a high value on human milk, which is well supported in the literature.24-27 Our study findings are consistent with previously published research in peer-to-peer milk-sharing communities, including an unexpected surplus often prompting peer-to-peer sharing, peer-to-peer sharers having concerns about milk bank costs and convenience, and peer-to-peer sharers valuing the personal experience of helping another family.24,31
This study provides additional insights into the understanding of donor milk costs, including the belief that milk banks profit from the milk that is donated, that PDM is often viewed in the framework of “food for a healthy term infant” and not as a medical product for a fragile infant, and the belief that parents bear the financial burden for the cost of PDM. The research by Gribble 31 also identified “object to parents having to pay for banked milk” as a top barrier to milk bank donation among peer-to-peer sharers. A 2013 survey of level 3 NICUs in the United States found that hospitals (85.5%) and insurance companies (25.0%) most frequently paid for PDM, compared with parents (11.8%), 18 suggesting that one of the major barriers to milk bank donation in the United States is based on misinformation regarding who typically bears the cost of PDM. Findings from our study can help shape strategies for communicating with potential milk bank donors, including campaigns to differentiate nonprofit milk banks from for-profit entities, as well as campaigns to reframe PDM ($80 to $100 per pint) in the context of other life-saving medical products such as screened blood ($225 to $240 per pint).
This is the first study to report on how peer-to-peer milk sharers learn about the options for exchanging human milk. A key finding from our research is that health care professionals are currently not a major source of information about milk exchange in the United States. This is in sharp contrast to Brazil, where information about milk donation is regularly provided to lactating mothers through the health care system. 30 In 2012, approximately 5% of women who gave birth in Brazil donated milk to a milk bank,13,37 compared with less than 0.1% of women in the United States,32,38 suggesting that referrals from health care professionals may be an important strategy for achieving the public health call to expand the supply of pasteurized donor milk. Health care professionals have the potential to influence patient behavior related to breastfeeding, as evidenced by studies that show improved breastfeeding initiation and duration with health care provider support.39,40 Providing information about milk donation prenatally could allow mothers to be screened during regular prenatal visits, thus potentially lowering the barriers that some mothers described regarding the work involved in being screened to become a milk bank donor. In addition, education that was provided early in the lactation process related to milk collection requirements could inform the way mothers who were interested in potentially becoming donors collected and stored their milk, thus increasing the amount of milk that was eligible for donation. A small pilot study with potential donors in Australia found that most women preferred to get milk bank information prenatally, although more research is needed regarding timing preferences and effectiveness. 41
Participants in our study viewed sharing their milk as a way to help an infant but also as a way to help a mother who was experiencing similar struggles to those that they had experienced with breastfeeding. This desire to help people based on shared experiences is one strategy that has been used to increase charitable giving in other industries, which may have practical applications in a campaign to attract new milk bank donors. 42 Other participants in our study, while aware of the benefit of human milk for preterm infants, said they preferred the personal connection that they felt when giving their milk directly to an individual. While not all peer-to-peer sharers are likely to be candidates for milk bank donation based on this desire for personal connection, milk banks can take this into account by highlighting the personal stories of the infants and families who have benefited from pasteurized donor milk.
Limitations
Participants were selected for this study from a convenience sample of women who had already voluntarily participated in an online survey about milk sharing; therefore, there is a selection bias toward women who have a strong interest in this topic, and results may not be generalizable to a broader peer-to-peer milk sharing population. Milk donation is an emotionally sensitive topic, and interviews may have encouraged socially desirable responses, especially if one donation option was perceived as superior to another. Attempts were made to reduce this bias by asking open-ended, nonjudgmental questions and validating participants’ responses.
Conclusions
Peer-to-peer milk sharing represents a de-medicalization of human milk that expands access beyond the NICU. 43 At the same time, there is also the need for hospitals to have easy access to a screened human milk product for the most fragile infants. Many participants in our study recognized that human milk access was important for this population. Our research suggests that some of the barriers related to milk bank donation in the United States among peer-to-peer milk sharers may be improved with education campaigns that focus on people, payers, profits, and products. This includes creating more personal connections to the people (infants and mothers) who benefit from donated milk, educating donors on who bears the burden of payment for PDM, differentiating nonprofit and for-profit milk banks, and reframing PDM as a medical product for fragile infants versus a food. Using health care professionals to disseminate information about milk donation warrants further research and consideration as a strategy for promoting milk donation and reducing barriers associated with donation convenience. Future research should focus on developing effective messaging to address donor barriers as well as designing education programs for a variety of different health care professionals who support lactating women, including obstetricians, pediatricians, nurses, and lactation consultants. There is little information available on the demographics, motivations, attitudes, and experience of women who sell their milk; therefore, this is also an important area for future research.
Footnotes
Acknowledgements
We thank the peer-to-peer milk sharers who generously gave their time to tell us their stories.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: April Fogleman serves on the Board of Directors for the Human Milk Banking Association of North America.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Elon University Faculty Research and Development Grant, North Carolina State University CALS Dean’s Enrichment Grant, and research gifts from Mothers’ Milk Bank of San Jose, Mothers’ Milk Bank of Denver, and the Northeast Mothers’ Milk Bank.