
Abstract
Background:
Displacement caused by the 2015 earthquake in Nepal exacerbated poor health and nutrition for thousands of women and children.
Research aim:
This study aimed to identify the perceptions of Nepalese mothers residing in earthquake relocation camps regarding barriers, facilitators, and situational factors influencing breastfeeding and family well-being.
Methods:
An exploratory, rapid ethnographic approach was used during two fieldwork phases. Phase 1 consisted of reconnaissance and observation, whereas Phase 2 consisted of observation and qualitative semistructured interviews with infant caretakers (N = 14).
Results:
We found evidence of human milk substitutes donated by various groups after the earthquake, despite Nepal’s media statement condemning these donations. Participants in this study expressed concerns about their milk supply. They also expressed concerns about the impending winter season combined with distress about the 2015 fuel crisis and the impact that this had on their infants and children. Furthermore, participants expressed choices about infant feeding that were influenced by traditional Nepalese practices. Specifically, homemade complementary foods and spices designed to boost lactation were identified as being used during daily infant feeding practices.
Conclusion:
Infant caretakers need culturally specific support for breastfeeding after disasters. These findings can directly influence future interventions concerning Nepalese mothers’ perceptions, infant care, and feeding practices in disaster scenarios.
Background
On April 25, 2015, a magnitude 7.8 earthquake killed nearly 9,000 people in Nepal and damaged almost half a million homes. On May 12, a powerful aftershock caused additional damage to structures that were already partially collapsed in the original earthquake. The combined earthquakes affected over 8 million people (Nepal Planning Commission, 2015). Natural disasters and catastrophic hazards can have adverse impacts on the health of families, especially maternal and child health (Brunson, 2017; Datar, Liu, Linnemayr, & Stecher, 2013). Despite advances in reducing malnutrition rates in Nepal, the country still faces challenges in ensuring that infants and young children are properly nourished (Karn, Devkota, Uddin, & Thow, 2017). Although there were media reports about mothers and children affected by the earthquake and fuel crisis, it was unclear how these events affected infant feeding. In addition, it was unclear if and how human milk substitutes were distributed following the earthquake.
Even in nonemergency scenarios, breastfeeding has several health benefits for both mothers and infants, including but not limited to reduced rates of respiratory infections, reduced rates of diabetes, and bolstered immunity against infections (Rollins et al., 2016; Salone, Vann, & Dee, 2013). The practice of breastfeeding in Nepal is particularly important because it may impact fertility, or more specific, family spacing (Tommaselli, Guida, Palomba, Barbato, & Nappi, 2000), known as the lactational amenorrhea method (Labbok et al., 1994). Child spacing and overall fertility rates can help developing regions achieve lower maternal and infant mortality, among many other health benefits (Ahmed et al., 2015).
Supporting breastfeeding after disasters and in low-resource settings can dramatically increase the chances of infants surviving and thriving as breastfeeding reduces vulnerability to infections and communicable diseases (Atari & Mkandawire, 2014; Binns et al., 2012; Carothers & Gribble, 2014; Gribble, McGrath, MacLaine, & Lhotska, 2011; Hargest-Slade & Gribble, 2015; Hipgrave, Assefa, Winoto, & Sukotjo, 2012; World Health Organization, 2014). Artificial feeding in emergency scenarios can be particularly dangerous because of the increased likelihood of bacterial infections through improperly sterilized feeding supplies and lack of clean water for infant formula preparation (Gribble, 2014, 2017). Although infant formula donation is not unusual after disasters (Gribble et al., 2011), there has been a lack of qualitative fieldwork on maternal perceptions and decision making regarding infant feeding in disaster-affected areas, with some exceptions (e.g., Dörnemann & Kelly, 2013).
Compared with the broader body of knowledge on infant feeding decision making, much less is known about the extent to which these decision-making factors intersect with major events such as disasters or humanitarian emergencies (Prudhon et al., 2016). Therefore, the topic of decision making for infant feeding in emergency contexts is important not only for bolstering the scholarly knowledge of maternal perceptions in emergencies but also because of the urgent public health implications of improper infant nutrition and unsafe infant feeding.
After the earthquake, the government of Nepal and the United Nations Nutrition Cluster implemented a country-wide intervention during the summer following the earthquake (Aguayo, Sharma, & Subedi, 2015). The intervention, which included more than 467,425 women and children in 14 districts, had several core components, including supporting pregnant and breastfeeding women, screening infants and children for malnutrition, and distributing supplements (e.g., vitamin A). However, there is a scarcity of research regarding the narratives and daily perceptions of mothers who survived the earthquake (Brunson, 2017).
Also, 5 days after the earthquake, a document was distributed through social media, released by the Government of Nepal; the Child Health Division, Ministry of Health and Population of UNICEF; and the Nutrition Cluster (2015), with guidelines for aid workers and the general public about distribution of human milk substitutes (infant formula). This document listed common myths about breastfeeding and lactation after disasters (e.g., stress causing lactation to cease or to be greatly reduced) and also indicated that distribution of human milk substitutes (infant formula) should be prohibited and that Nepal should “refuse any unsolicited donations of these products” (p. 1). The local nonprofits and large international nongovernmental organizations (INGOs) focused on rescue, relief, and recovery immediately after the earthquake (Penta, DeYoung, Yoder-Bontrager, & Suji, 2016), but infant feeding protocols vary among the groups.
Key Messages
This study fills a gap in research on the social and cultural aspects of infant feeding in emergencies in Nepal.
Displaced Nepalese women in this study had perceptions of low milk supply and were concerned about their infants’ physical needs (shelter, warmth, and medical needs). It is probable that infant formula was distributed after the 2015 earthquake without assessment and lactation support.
Infant feeding support for mothers and families is important during emergencies and should be culturally specific and account for other needs (trauma, stress, and physical needs).
In addition to the destruction caused by the earthquake, a considerable amount of political unrest occurred in 2015. There were ongoing protests in mid- to late 2015 in the Terai region because of tensions over the new constitution. This caused India to halt the flow of fuel into Nepal for several months, ultimately causing long lines for fuel and a lack of fuel for cooking. The import of other essential supplies, such as medicine, raw materials, and so on, from India was halted as well (Pathak, 2015).
Our research was designed to identify how infant feeding was affected during the specific time frame following the earthquake and during the fuel crisis because of the combination of disaster displacement, resource constraints, the convergence of humanitarian groups following the earthquake in Nepal, and previous research on untargeted distribution of human milk substitutes after disasters. The research questions are as follows:
What factors created barriers or facilitators for breastfeeding in the earthquake relocation camps?
What are general physical needs and concerns while residing in an earthquake relocation camp?
What are the perceptions of family well-being and sense of community in the earthquake recovery camps?
How do the sense of community, the fuel crisis, and displacement due to the earthquake relate to infant feeding?
This knowledge can lead to a better understanding of infant feeding in emergencies and crisis settings.
Methods
Design
A prospective, cross-sectional, mixed-methods design was used to address the study aims. The two main methods used were qualitative and observational data. The rationale for this design was that the earthquake created a rapidly changing situation for the people and groups throughout Nepal. This approach also may be categorized as a rapid ethnographic assessment (Guerrero et al., 1999; Trotter, Needle, Goosby, Bates, & Singer, 2001) through which we gathered information about groups and locations that were relevant to maternal and child health. This rapid method of data collection postdisaster with an emphasis on rapid and semistructured qualitative data gathering is appropriate when data are perishable after disasters (Phillips, 2014).
We obtained human subjects research approval from the institutional review board of the University of Delaware for work in May and June, as well as the follow-up work in November. We obtained consent by explaining the study verbally in Nepali and then asking participants if they would like to participate in the research. We also gave written information and consent form copies to all participants (in Nepali).
Setting
We located the key earthquake relocation camps from news reports and from the knowledge of one of the coauthors (Nepalese). Various nongovernmental and governmental groups ran the earthquake relocation camps in which the data were collected (see Figure 1). The conditions in the camps were quite crowded immediately after the earthquake. The latrine space was shared among many people. Many larger INGOs partnered with smaller local nongovernmental organizations (NGOs) for the mother–infant tents. They offered sanitary pads, a quiet place to breastfeed babies, and a place to change diapers. Women who gave birth during and after the earthquake returned to the earthquake relocation tents within 1 or 2 days of giving birth. Six months after the earthquake, the mother–infant tents were no longer present, since humanitarian groups stopped providing relief, even though families remained in the displacement camps.

Earthquake relocation camp.
The qualitative interviews with mothers took place approximately 7 months after the April 25, 2015, earthquake. Decisions about feeding children (Joshi, Agho, Dibley, Senarath, & Tiwari, 2012; Osei et al., 2015) and infants are partially driven by broader cultural and religious ideas. Specifically, breastfeeding an infant is important for kinship, nutrition, and community and family bonds (Aryal, 2007; Paneru, 1981). For example, in Hinduism (the dominant religion in Nepal), two babies who receive human milk from the same woman may be deemed as siblings even though biologically they may have different mothers (Paneru, 1981).
Infant feeding practices in Nepal are influenced by social and economic systems (Khanal, Sauer, & Zhao, 2013; Panter-Brick, 1992). For example, residing in urban versus rural areas, family economic status, and education levels are also related to the duration and frequency of breastfeeding (Karkee, Lee, Khanal, & Binns, 2014). Specifically, women who work in informal occupations are ineligible for official maternity leave benefits (Locks et al., 2015), and this may impact duration of breastfeeding.
The perception of low milk supply may lead mothers to decide to introduce early solids or liquids to the infant, therefore reducing rates in exclusive breastfeeding (Rogers, Baral, Sharma, & Stephens, 2015; Thet et al., 2016). Weaning practices vary among the different castes and ethnic groups in Nepal (Moffat, 2002; Rogers et al., 2015). For example, according to Rogers et al. (2015), in the Tamang community, one of the indigenous groups of Nepal, mothers may wean their infants later than other caste groups.
One of the main “weaning foods,” or first solid food, in Nepal is known as sarbottam pitho, meaning “super flour” or “most excellent flour” (Krantz, 1983). Sarbottam pitho is now marketed and mass produced as a weaning food for infants or first complementary food but was originally created as a malnutrition intervention (Krantz, 1983). Before the advent of super flour, soy was being fed to small children in rural parts of Nepal as whole kernels, which the children were unable to digest. Once the super flour (made from ground roasted soy) was implemented as a major malnutrition intervention, it became common practice not only for health and humanitarian workers to use in interventions but also for most families to use as an introductory food beginning around age 5 to 6 months. In Nepal, it is considered traditional practice to make pitho or litho (cooked pitho) for infants and toddlers as their first and main source of solid food (Siwakoti, 2014). Also a part of postpartum Nepalese cultural practices, the consumption of ghee, rice, sugar, and jwano (carom/thyme seed) is seen to increase lactation (Paneru, 1981). Jwano is usually made for postpartum mothers in the form of a soup.
Sample
Families who were relocated after the 2015 earthquakes were the target sample. For this project, women had to be 18 years of age. The key requirement for participation was that the women were displaced by the 2015 earthquake. Potential participants were identified using a combination of convenience and snowball sampling. This sampling method was used because the location of the major airport in Nepal in the Kathmandu Valley area determined our accessibility. Most of the data were collected in the Kathmandu Valley, but 2 participants were interviewed in the district of Sindhupalchowk (just northeast of Kathmandu) and 1 participant was interviewed in the rural village of Ramkot, just northwest of Kathmandu. Remote villages in Nepal are hours and days away from the urban center of Kathmandu; therefore, it was not feasible to reach them. When many of the participants repeated key themes, saturation was reached (Guest, Bunce, & Johnson, 2006).
Data Collection
There were two phases for the data collection (see Table 1). For both phases of fieldwork, we conducted daily audio debriefings among the research team to recount the conversations we had with various program officers and then these were transcribed; field notes were transcribed daily to prevent loss of valuable information. We wrote meticulous notes immediately after speaking with the participants and then created audio debriefs at the end of each day of data collection. Notes from fieldwork were edited for meaning and context by the second author because of his local knowledge of the fieldwork sites.
Phases of Data Collection.
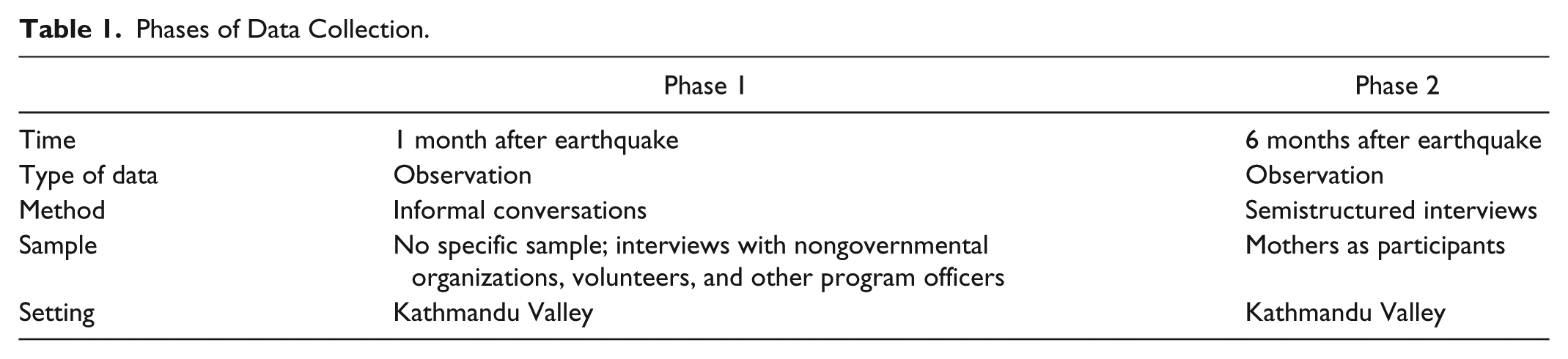
Phase 1 involved reconnaissance fieldwork 4 weeks after the earthquake, did not contain any structured interviews, and was primarily designed to capture broader social issues related to the earthquake response (see Penta et al., 2016). During Phase 1, we met with program officers offering maternal, nutrition, and psychosocial support services to gather information about the overall situation of support services and migration of earthquake victims. We entered relocation camps of earthquake survivors, documented locations of the camps, and took photographs of the setting.
In Phase 2, we collected the semistructured interview data from participants (mothers). The interviews took place over a span of 10 days in four different relocation camps during fall 2015, approximately 6 months after the earthquake.
Most of the people who were living in the camps had arrived a few days or weeks after the earthquake and had been living there since that time. We built rapport with the displaced communities by entering the relocation camps several times and talking informally with the families. Data were gathered using field notes, semistructured interviews, photographs in the field, and contextual information (e.g., local news reporting) during the fieldwork deployment. Informed consent and questions for the interviews were translated to Nepali, and interviews were conducted in Nepali by the second author, who is trained in anthropological research methods.
During Phase 2, the semistructured interviews ranged from 45 min to 2 hr. There were 22 questions in the interview guide (see Supplementary Material available online). The qualitative interview contained questions on feeding choices, perceptions about urgency of needs, psychological well-being, sense of community in the tent camps (or village), and some demographic information (natal village, caste/ethnicity, occupation, birth and delivery location and method, and occupation of the infants’ fathers).
Photographs and contextual (observational) data were also gathered from villages and neighborhoods surrounding the displacement camps for a broader understanding of daily life and access to resources during the time of data collection. These data collection methods were selected because they provide information about the living conditions and perceptions of daily life during the earthquake recovery. In addition, documentation of the setting through photographs was used to link the setting to the participant interview data. This provided a more holistic picture of the participants’ needs and perceptions related to infant feeding, well-being, and health.
We also compared the findings from the interviews with our observations and photographs from fieldwork, which is a form of triangulation (Thurmond, 2001). Triangulation through observation and photographs validated the content of qualitative interviews. For example, we documented many instances of firewood stored next to tent camps, which confirmed information from the qualitative interviews—that this was the main way in which families were cooking (instead of gas fuel for cooking). We also observed close living spaces, dirty infant bottles, and other aspects of the environment that emphasized difficult living conditions in the tent camps.
Data Analysis
To minimize the bias of interaction with participants and to manage reflexivity, during data collection, we had daily debriefings that included reflections of our perceptions of infant feeding and the data collection settings. The lead researcher was breastfeeding her toddler during the time of fieldwork. Although in some cases, this may have facilitated rapport with the Nepalese mothers, we were also cognizant of the influence of Western ideas associated with infant feeding. Because the participants spoke Nepali and the lead researcher did not speak Nepali, it may have diffused some of the potential projections of Western notions of infant feeding that may have occurred through direct conversations.
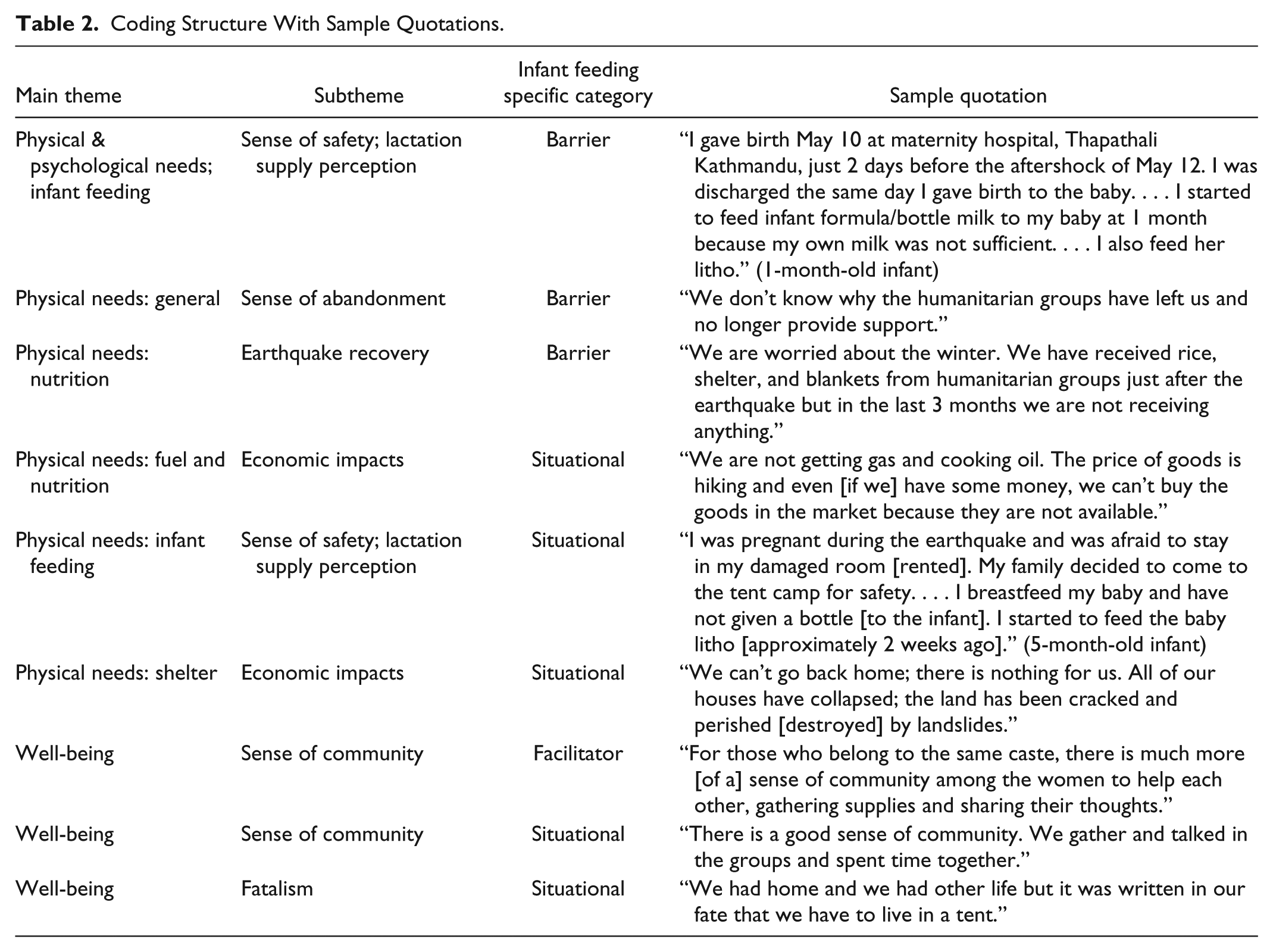
Phrases and words were coded using an open-coding approach in which some categories of findings were either consolidated according to theme or further divided into new subcategories for the content analysis (Bernard, Wutich, & Ryan, 2016). For example, the broad theme of physical needs led to the subtheme of difficulties caused by blockade such as use of firewood for cooking (see Table 2). We continually adapted the instrument of questions as we interviewed infant caretakers (Bernard et al., 2016; Corbin & Strauss, 1990). For example, after Day 1 of interviews, we noticed that the participants mentioned that they had to return (to the camps) from the maternity ward very shortly after giving birth; therefore, the question about place of birth was added. The researchers independently reviewed the aggregated field notes and created lists of the themes and subthemes. The researchers then came to agreement on the main themes and subthemes and coded them as seen in Table 2.
Coding Structure With Sample Quotations.
Results
Participant Demographic Characteristics
The participants were mothers ages 19 to 29 years (see Table 3). There was a 67-year-old grandmother as the primary infant caretaker who answered questions about her infant granddaughter because the mother of the infant was in the hospital.
Participant Demographics.
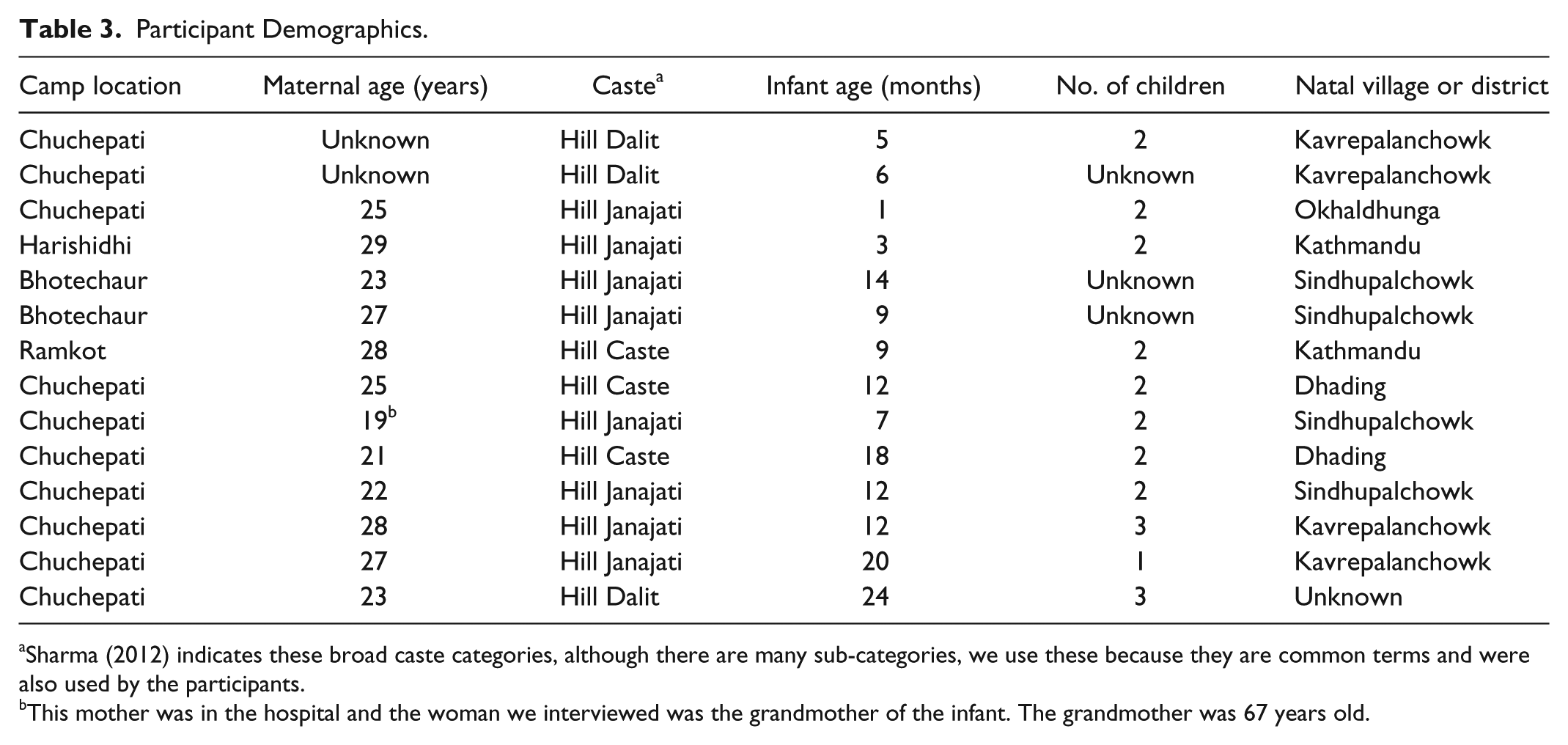
This mother was in the hospital and the woman we interviewed was the grandmother of the infant. The grandmother was 67 years old.
Thematic Findings
Results are presented in the order of the research questions and the ways in which the three core coded themes emerged: description of issues relevant to infant feeding, description of physical needs, and sense of community. Research Question 4 is addressed in the Discussion section because it relates to the interpretation of how all of the factors throughout the themes may relate to infant feeding (implications for infant feeding). Throughout all of the core themes, there were additional subthemes (i.e., sense of abandonment by the government as a subtheme of physical needs after the earthquake and fuel crisis). The subthemes can also be categorized as barriers to, facilitators of, or situational to safe infant feeding and breastfeeding.
Research Question 1: Infant Feeding Issues
We observed many mothers breastfeeding their babies while we interviewed them. However, low perceived milk supply was a common theme. This perceived low milk supply prompted many women to supplement with infant formula or complementary solid foods: “I started to feed [formula brand name removed] bottle milk to my baby because my own milk was not sufficient to nurse [the baby]. I also feed her litho” (1-month-old infant). Several similar statements suggest that the participants felt like they were not producing enough milk for their infants: “I did not make enough milk so I gave [formula brand name removed] to the baby.”
Participants specifically expressed perceptions that their milk supply was “bad” after approximately 3 to 4 months of breastfeeding. Upon further questioning of what they meant by bad, the participants indicated that there was not enough milk for the infant. We asked about this feeling in relation to the timing of the earthquake, but participants focused more on the general age of the infant in terms of milk production. It is interesting that the statements from the women did not explicitly connect the earthquake to their low supply, but they talked about the general timing and perceptions of coming to the tent camp and then feeling as though they could not continue breastfeeding: “I fed [my baby] with the breast but my milk was [bad].”
There were instances of participants indicating that humanitarian groups distributed formula after the earthquake, but some of the mothers continued breastfeeding without using the distributions of formula. The infant formula that was distributed was described as powder in packets—“They [the NGOs] handed out four packets of litho [per family]. . . . We tried to get more food for the baby but they just didn’t give her anything”—and was handed out without a clear assessment procedure: “The humanitarian groups gave packets of [infant formula], but I was still breastfeeding my baby.”
In the earthquake relocation camps, we encountered both the homemade version of sarbottam pitho and the commercialized version (which is sold in stores as a dry cereal powder). Several participants expressed the belief that homemade sarbottam pitho was superior in quality compared with the store-bought sarbottam pitho. It is difficult to determine the relationship between use of complementary foods and the earthquake. However, several participants indicated that they fed solids to their infants at only 1 or 2 months of age while residing in the earthquake relief/relocation camps.
Participants also indicated that they relied on intergenerational knowledge about breastfeeding and weaning practices, specifically with regard to cultural beliefs about lactation spices and complementary foods. Although we interviewed one grandmother as the primary infant caretaker, grandmothers were also present in two additional instances during interviews with mothers. The grandmothers often reinforced what the mothers said about learning how to make homemade complementary solids for the infants (sarbottam pitho) or to use jwano (spice) soup for lactation support. When we asked one mother if she ate jwano soup to facilitate lactation, she responded by saying that there would be no other way to produce human milk: “If I don’t eat the soup [jwano], how can I make the milk?” When participants were asked, “Where did you learn how to make sarbottam pitho?” nearly all of the participants indicated that they learned the practice from their mothers or mothers-in-law.
In some cases, we saw dirty bottles (infant bottle with teats) on the ground near the infant and mother during observation and participant interviews. One pair of participants was the aunt and grandmother of an infant whose mother was hospitalized for tuberculosis and was therefore separated from her infant. The infant was 9 months old and was cared for by the grandmother and occasionally breastfed by the aunt. However, it should be noted that this instance of wet-nursing was connected to the mother’s illness, not the earthquake, although these events occurred within the same year. Aside from this instance, evidence of wet-nursing among mothers was scarce.
Research Question 2: Physical Needs
Of the 14 participants we interviewed about infant feeding, all had been directly impacted by the earthquake, and 13 of them had homes that were completely collapsed or uninhabitable following the earthquake (one participant tried to return to her rented room after the earthquake but was unable to afford the rent). Some of the participants we spoke to who gave birth after the earthquake returned to their tents (from the hospital) within 1 day of giving birth. Food, fuel, and shelter were difficult to obtain: “We have empty stomachs. The kids ask about food and when they will eat, but they don’t understand; they just want food.”
Identification of physical needs included worries about obtaining food, cooking food, perception of low human milk supply (as described in the previous section), illness, and exposure to cold temperatures. Many families talked about sleeping in the mud on the ground of their tents throughout the monsoon season into the autumn months: “There was nothing for new moms and babies after the earthquake.” Many of the concerns about exposure to the environment were specific to needs of the infants: “If it [our house] was collapsed, we could lose our baby, but we were lucky; it was badly damaged but not totally collapsed.” Physical shelter for infants was a key concern. Most of the participants lived in tarps or tents and expressed concerns about the freezing temperature at night:
We had come to the school ground quite later than other people and the tents were already distributed. One night, it rained whole night and there was water collected in the ground; we spent without sleeping. My baby became sick.
Sense of safety and security also emerged as a subtheme within the core theme of physical needs. The participants expressed distress over the uncertainty of their future and their children’s well-being. Participants expressed that they felt safer in the tent camps than partially collapsed rented rooms. They were afraid that another earthquake would occur. Participants also emphasized a sense of abandonment—“The government of Nepal has forgotten about us. . . . It would be better if we had died in the earthquake, without shelter and a way to make an income”—and resentment toward the government: “The politicians came for our votes during elections, but they didn’t come help us after the earthquake.”
The participants also expressed concerns for medical needs due to illnesses and needs for medication, combined with poor living conditions in the camp: “The baby cries so much at night. . . . She seems to be in pain.” Some of the infants and young children were likely ill but were not receiving medical support: “The baby eats dirt and clay and her bowel is black. Once we went to the doctor and said we should return. The baby only wants to breastfeed.” The mother with the infant eating dirt indicated that humanitarian medical groups were not frequently visiting the relocation camps. Observation supported this statement (i.e., we did not encounter health groups or health workers in the 10 days of interviews).
Research Question 3: Well-Being & Sense of Community
Finally, caretakers in the settlements expressed that infant care was a communal activity and the responsibilities of infant and child care were shared. This kinship of breastfeeding was reflected in the ways in which women supported one another in the villages and tent camps. Communal caretaking of infants was evident in the relocation camps and settlements.
In nearly all of the participants’ interviews, there was evidence either in the data from the interviews or through the physical presence of other caretakers assisting with daily care activities (bathing, feeding, and playing). We observed families cooking and engaging in daily caretaking activities and children playing in the tent camps. When talking with the families, multiple families and women with infants clustered together. Participants expressed mutual care and support for childcare: “We all live in this camp and we should help each other because we are here and we have nothing to do.” The participants expressed that these caretaking activities were not contingent upon biological kinship: “We are not related but our babies are the same age so we stay together.”
Discussion
The aims of identifying factors related to the earthquake and fuel crisis were addressed by linking participants’ perceptions with infant feeding choices. Although observational findings reflected the cultural norm of breastfeeding, there were factors identified that may have acted as barriers to breastfeeding and safe infant feeding (e.g., early introduction of complementary solids, untargeted distribution of human milk substitutes) and stress related to relocation and poor living conditions after the earthquake.
The media statement released by the government of Nepal (described in Setting section) regarding distributions of human milk substitutes could be viewed as a media “success story” in international disasters and policies on adhering to the World Health Organization’s (1981) International Code of Marketing of Breast-milk Substitutes. This statement was released very quickly after the disaster, which is rather atypical in disaster scenarios. However, since many participants indicated that several NGOs and other groups were distributing human milk substitutes in the earthquake relocation camps, this brings into question how effective this messaging was in preventing formula distribution. The themes from this study reflect themes from previous research on infant feeding in emergencies and indicate that uncontrolled distribution of infant formula is pervasive and ongoing (Gribble et al., 2011). Additional research should extend the research questions that we focused on in this project to other postdisaster and crisis settings to establish patterns and evidence for the impact of cultural, social, and organizational issues related to infant and young child feeding practices in emergencies. A key area of interest is the distribution of powdered infant formula. To what extent are local groups informed about best practices for assessment and control of infant formula? How does social media influence the mass influx of unsolicited formula donations?
Future research aims should also continue to clarify links between cultural factors and infant feeding. Evidence and research-based interventions should incorporate culturally informed knowledge about infant feeding to those contexts (i.e., jwano as a spice to boost lactation in Nepalese families). Research in this area could also link these interventions with measurable outcomes of feeding choices and health outcome data. The research presented here is unique to the point in time in which the data were collected. However, relocation will continue to occur in future disaster events. Infant feeding in relocation settings may be different depending on the duration and origin of the emergency (i.e., human-made or natural disaster). In Greece, for example, several groups have been working with the mass influx of migrant and refugee arrivals to provide infant feeding support (Svoboda, 2017). During and after disasters in which families are highly transient, research on feeding and interventions may be more difficult to carry out.
Because the participants also indicated that the price of food and sanitary items was unusually high because of the blockade and fuel crisis, there may be a relationship between socioeconomic status and infant feeding practice among the families living in the tent camps. Even though caretaking for many of our participants was expressed to be a communal activity, this kinship could not replace the stark resource deprivation that was exacerbated by the co-occurring conditions caused by the earthquake and the fuel crisis. Future research should also address this important question of whether infant feeding in emergencies is affected by changes in social networks caused by postdisaster migration.
This research is one of the first studies to link seasonal changes and political turmoil to infant feeding, also a common theme in the data. Seasonal changes similar to the ones identified by our research (cold weather and lack of shelter) have been found to have adverse impacts on maternal and child health (Hartig & Catalano, 2013) but have not been explored specifically in the context of a fuel crisis that exacerbates resource deprivation. In the present study, the data themes cluster around lack of access to gas fuel as having a direct impact on feeding of infants and children. Because physical health is linked to overall well-being (Gatt, Burton, Schofield, Bryant, & Williams, 2014), it is important to identify the physical needs of displaced families. Our methodology resulted in data that presented a snapshot of some of these physical needs, but we were unable to provide medical support or advice to the participants. Research teams accompanied by medical and health workers (specifically, lactation specialists, doulas, and female community health workers) may be an ideal model of intervention and action research, although it is less commonly applied in social science research (Denscombe, 2014) than through monitoring and evaluation programs carried out by large INGOs. A relatively low-cost and simple intervention in the disaster or refugee location camps is to provide information to humanitarian workers and families about infant feeding (i.e., messages about how stress will not cause lactation/human milk to “dry up,” messages about controlling infant formula, assessments of families, and safe preparation of food and feeding supplies).
The aforementioned media release on controlling infant formula after the earthquake, along with other contextual factors, could be categorized as situational factors related to infant feeding. It is important to note that situational factors could become facilitators or barriers, depending on the mechanisms of these factors. For example, the media release on formula distribution is a facilitator as long as it was received by the primary and key groups working directly with mothers and infants affected by the earthquake.
Finally, the sense of community among people who are relocated warrants additional research. Although the current study focused on the intersection of child and maternal well-being with relocation, it would be useful and interesting to see how specific variations occur in both the perceptions and behaviors related to a sense of community among people relocated after disasters. Although this issue has been studied with regard to Hurricane Katrina (Chamlee-Wright & Storr, 2009) and in other areas of the world (Bulley, 2014), longer term tent communities in Nepal have not been systematically studied. The ongoing blockade and fuel crisis that began after the earthquake may also have unique effects on how sense of community is perceived and “acted out” among Nepalese earthquake victims. The emphasis on family and communal care of infants could be categorized as a situational factor for infant feeding. Specifically, the emphasis on family influences on feeding choices (e.g., sarbottam pitho) and nutrition suggests that interventions postdisaster should include grandmothers and other members of the extended family. Similarly, the use of specific spices (jwano) to increase lactation should be considered in support and interventions during disaster recovery, even if the mechanism is partially through altering perceptions of low milk supply. Family influences could also become facilitators or barriers, depending on the influence of in-laws and their perception of the “appropriate” duration and methods of infant feeding. In literature on family influences on infant feeding, grandmothers can influence maternal choices regarding infant feeding (Negin, Coffman, Vizintin, & Raynes-Greenow, 2016). Mothers-in-law in South Asia can also influence decisions about infant feeding (Sharma & Byrne, 2016).
All of these areas require further research to build upon theoretical work and to begin to understand how these findings can be applied in community interventions to bolster the well-being of mothers and families affected by disasters and humanitarian emergencies. Clear guidelines about infant and young child feeding in emergencies for health workers and humanitarian groups would increase the likelihood of situational factors (that accompany the disaster and affected communities) acting as breastfeeding facilitators rather than barriers. These guidelines exist in many groups working with maternal and child health, but they require careful and deliberate implementation (i.e., local people involved in the outreach, use of a variety of communication channels for health messaging, and integration of infant and young child feeding in emergencies into disaster response protocols).
Limitations
A possible limitation is that there may have been instances in which the meanings of key phrases or words were misinterpreted by the researchers. Even though one of the researchers for this project is Nepalese, there still may have been regional differences in dialects and meanings of words. We may also have been biased in interpreting data from the fieldwork and interviews because of our personal experiences with infant feeding as it is situated in our cultural worldviews. Inherent in the nature of this type of cross-sectional research is the understanding that results are relevant only for the period of time collected and may have changed after the research was conducted.
Conclusion
The fuel blockade in mid- to late 2015 combined with the earthquake recovery was a complex humanitarian emergency. Our study provides a basis for future studies that bolster knowledge about the complex issue of infant feeding in emergencies. Breastfeeding support, hygienic living conditions, cultural factors, and potential exhaustion of (or removal from, in cases of relocation) social support networks should all be considered in postdisaster interventions for infant feeding.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Travel and salary for this work was supported by the National Science Foundation under Grant Nos. 1331269 and 1331572 Subcontract 14-007985 A 00 and by the Centers for Disease Control and Prevention through Grant No. 5P01TP000288 and Research Contract 200-2014-60654. Additional support was provided by the Natural Hazards Research Center and the Society for Community Research and Action. Fieldwork was conducted when the first author was working at the University of Delaware Disaster Research Center. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the Disaster Research Center, the National Science Foundation, the Centers for Disease Control and Prevention, the Natural Hazards Center, or the Society for Community Research and Action.
Supplementary Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.