
Abstract
Background:
Human milk is a rich source of omega-3 long-chain polyunsaturated fatty acids, which are postulated to be important for brain development. There is a lack of data on the human milk fatty acid composition of Cambodian women compared with data from Western women.
Research Aim:
The aim of this study was to determine the human milk fatty acid composition of women living in Cambodia and compare it with that of women living in Australia.
Method:
Human milk samples from Cambodian (n = 67) and Australian (n = 200) mothers were collected at 3 to 4 months postpartum. Fatty acid composition was analyzed using capillary gas chromatography followed by Folch extraction with chloroform/methanol (2:1 v/v), and fat content was measured gravimetrically.
Result:
Compared with Australian participants, human milk from Cambodian participants contained a significantly lower level of total fat (2.90 vs. 3.45 g/dL, p = .028), lower percentages of linoleic acid (9.30% vs. 10.66%, p < .0001) and α-linolenic acid (0.42% vs. 0.95%, p < .0001), but higher percentages of arachidonic acid (0.68% vs. 0.38%, p < .0001) and docosahexaenoic acid (0.40% vs. 0.23%, p < .0001).
Conclusion:
Differences in human milk fatty acid composition between Cambodian and Australian participants may be explained by differences in the dietary patterns between the two populations.
Keywords
Background
Exclusive breastfeeding of infants during the first 6 months of life and continuing breastfeeding with appropriate introduction of complementary foods for up to 2 years of age is recommended by the World Health Organization (2017). One of the key nutrients in human milk that has received special attention is omega-3 (n-3) long-chain polyunsaturated fatty acid (LCPUFA), particularly docosahexaenoic acid (DHA), because of its important role in neurodevelopment (Innis, 2014). Although infants are able to synthesize DHA and other LCPUFAs from essential fatty acids, α-linolenic acid (ALA) and linoleic acid (LA), the conversion rate may not be sufficient to meet requirements, so it is important for infants to obtain an adequate amount of DHA and other LCPUFAs from human milk (Innis, 2014).
Human milk LCPUFA composition is determined largely by maternal dietary intake (Innis, 2014). There is evidence that women from Asian countries with higher seafood intake also have higher human milk DHA levels (Yuhas et al., 2006). Human milk fatty acid patterns of women from industrialized Western countries that share similar “low seafood and high omega-6 (n-6)/n-3 polyunsaturated fatty acid (PUFA) ratio” dietary patterns are generally similar: high in saturated fatty acids but low in DHA content (Yuhas et al., 2006). The human milk fatty acid composition of women in Cambodia, whose residents typically consume a diet that is high in fish (Food and Agriculture Orgnization of the United Nations, 2014) is unknown. The aims of this study were (1) to assess the human milk fatty acid composition of lactating women in Cambodia and (2) to compare it with that of women from an industrialized western country.
Methods
Design
This is a retrospective nonequivalent two-group comparison study. We used human milk samples of Cambodian and Australian women collected from two previous nutritional studies (Condo et al., 2016; Huynh et al., 2017a; Whitfield et al., 2016) to address the aim of the study. These samples had been preserved at −80°C for future use.
The study was approved by the relevant human research committees (Women’s and Children’s Hospital [WCH] in South Australia, Cambodian National Ethics Committee for Health Research, and the University of British Columbia–Children’s and Women’s Health Centre of British Columbia).
Setting
The study samples were collected in Cambodia and Australia. Cambodia is a developing country with 15.4% of its population undernourished in 2012, and almost 70% of its children were either stunted or underweight (Food and Agriculture Organization of the United Nations, 2014). The dietary pattern of the Cambodian population consists of mainly cereals, contributing to 70% of the total energy intake, and small amounts of fats, vegetables, and fruits (Food and Agriculture Organization of the United Nations, 2014). About 80% of the Cambodian population lives in the rural areas; participants recruited for this study were from rural Prey Veng province. On average, 73.5% of lactating mothers in Cambodia exclusively breastfeed their infants during the first 6 months of the infants’ lives (Prak et al., 2014). This rate is slightly higher among women living in urban areas (75.3%) than women living in rural areas (64.1%) (Prak et al., 2014).
Australia is a developed country whose population is generally well-nourished, and the dietary pattern is more diverse. Carbohydrate contributes to approximately 45% of total energy intake (Australian Bureau of Statistics, 2014). Participants in this study were recruited from two South Australian public hospitals, Flinders Medical Centre (FMC) and WCH. FMC is the largest hospital in the southern area, providing medical service to the southern-area populations as well as some rural areas. WCH is located in North Adelaide and provides the largest maternity and obstetric service in the state. More than 90% of Australian mothers initiated exclusive breastfeeding after delivery, but this rate declining gradually with time, and only about 15% of infants are still exclusively breastfed by the age of 5 months (Department of Health, 2017).
Key Messages
These are the first data on the fatty acid composition of human milk from Cambodian women.
Our study is the first to compare human milk fatty acid composition of women from Cambodia and Australia. The human milk of the Cambodian women was significantly higher in docosahexaenoic acid but lower in total fat content, linoleic acid, and α-linolenic acid compared with the human milk from the Australian women.
Differences in human milk fatty acid profile between the two populations are likely due to their different dietary habits.
Samples
Cambodian Samples
The precollected milk samples of the Cambodian cohort were from a double-blind randomized controlled trial investigating the effect of thiamine-fortified fish sauce consumption on the thiamine status of mothers and their infants (Whitfield et al., 2016) (the trial was registered at ClinicalTrials.gov, identifier NCT02221063). Participants were recruited from rural Prey Veng province in October 2014. Participants were eligible if they were aged 18 to 45 years, between 3 and 8 months’ gestation with singleton pregnancy, and planned to exclusively breastfeed their infants for 6 months. Milk samples were collected at the end of the 6-month study period, during April 2015, at an average of 4 months postpartum. Surplus milk from participants (n = 67) who provided human milk samples for thiamine analysis were used for this study. The thiamine intervention had no effect on human milk fatty acid composition.
Australian Samples
The precollected milk samples of the Australian cohort were from the Pregnancy Iodine and Neurodevelopment in Kids (PINK) study, which assessed the association between maternal iodine status during pregnancy and the neurological development of infants (Condo et al., 2016; Huynh et al., 2017a, 2017b). A total of 784 participants were recruited from two local public hospitals, WCH and FMC, between 2011 and 2012. Participants were eligible for the PINK study if they were less than 20 weeks’ gestation and able to give informed consent. Human milk was collected at 3 months postpartum to assess iodine status, and surplus samples were stored at −80°C. Of 529 participants who had surplus samples and had given consent for further analysis, 200 were randomly selected for the present study. The sample size was based on the availability of samples. With a total of 267 samples (ratio approximately 3:1), we have 80% power to detect a mean difference of 0.2% in n-3 LCPUFAs between the two cohorts given the standard deviation in our study.
Measurement
The total fat content of human milk was determined according to the conventional modified Folch method (Folch, Lees, & Stanley, 1957). In brief, 200 µL of thawed and homogenized human milk was used for lipid extraction with chloroform and methanol (2:1 v/v); the total weight of lipids was estimated gravimetrically. Extracted lipids were transmethylated to fatty acid methyl ester (FAME) with 1% sulfuric acid in methanol at 70°C for 3 hours. During this procedure, all fatty acids were released from their structured lipids (triglycerides, phospholipids, and cholesterol esters) into the overall fatty acid pool. FAME was then extracted with heptane for analysis by gas chromatography.
The separation and quantification of FAME were carried out using a Hewlett-Packard 6890 (Hewlett-Packard, Palo Alto, CA) gas chromatograph equipped with a BPX70 capillary column (50 m × 0.32 mm, film thickness 0.25 mm; SGC, Victoria, Australia). A commercial reference mix of FAME was injected with each batch of samples for quality control, and the coefficient of variation ranged from 1.0% to 4.5%. The fatty acids in samples were identified and quantified on the basis of the retention time and peak area of a commercial reference mix of FAME (Nu-Chek-Prep, Waterville, MN) using the Hewlett-Packard ChemStation data system.
Data Collection
All participants provided individual written informed consent in the original study; those who consented for their human milk samples to be used for future investigation were included in the study. The socioeconomic status of participants in both cohorts, including age, race, educational background, and parity, was collected at the time of enrollment on the basis of self-report, by face-to-face interview. Maternal height and weight were measured at the time of enrollment. All analyses were carried out at Waite Lipid Analysis Centre by the first author and a research assistant using standardized techniques and methods in July and August 2016.
Cambodia
Human milk was collected at an average of 4 months postpartum. The full expression of a single breast (that was not most recently emptied) was collected in the morning using a breast pump during a nurse visit at the end of the randomized controlled trial. Human milk samples were first transported on ice to the National Institute of Public Health in Cambodia within 5 hours of collection and then transported on dry ice to Canada, where samples were kept at −80°C. The samples were shipped on dry ice to Australia and stored at −80°C in a freezer that was centrally monitored until analysis.
Australia
Human milk was either collected at a clinical appointment at the hospital or at the participant’s home at 3 months postpartum. Participants were instructed to collect 10 to 15 mL of foremilk into a container (70-mL sterilized pot; Southern Cross Scientific, Edwardstown, Australia) between 5 and 9 a.m. before the first feed of the day. The samples were first stored in a home freezer or a freezer at the hospital and then transported to the laboratory using an insulated container with a freezer brick at an average of 9 days after collection. All the human milk samples were then stored at −80°C before analysis.
Data Analysis
Human milk fatty acid data are reported as weight percentage of total fat. Data were checked for normality, and the median and interquartile range are reported for continuous variables that were not normally distributed and the mean and standard deviation for those with normal distributions. Categorical variables are presented as numbers with percentages. Differences in demographic characteristics between the Australian and Cambodian cohorts were assessed using the Mann-Whitney U test and the χ2 test. The fatty acid data were not normally distributed and were log-transformed for statistical analysis. Comparison of human milk fatty acid composition between Cambodian and Australian cohorts was conducted using generalized linear regression with and without adjustment for demographic variables with p values less than .20 in univariate analysis examining the association between demographic variables and fatty acid concentration. Statistical analyses were carried out using SPSS Version 23.0 (IBM, Armonk, NY), and the significance level was set at .05.
Results
Characteristics of Participants
The two cohorts were demographically quite different (Table 1). Compared with Australian participants, Cambodian participants were significantly younger (M = 26.2 [SD = 4.7] vs. 33.2 [SD = 4.6] years, p < 0.0001) with lower body mass index (BMI) (median = 22.4 [interquartile range = 20.9-24.3] vs. 25.0 [interquartile range = 22.2-27.4] kg/m2, p < .0001). The median gestational age of the infants at birth was 39 weeks in both groups.
Demographic Characteristics of the Sample (N = 267).
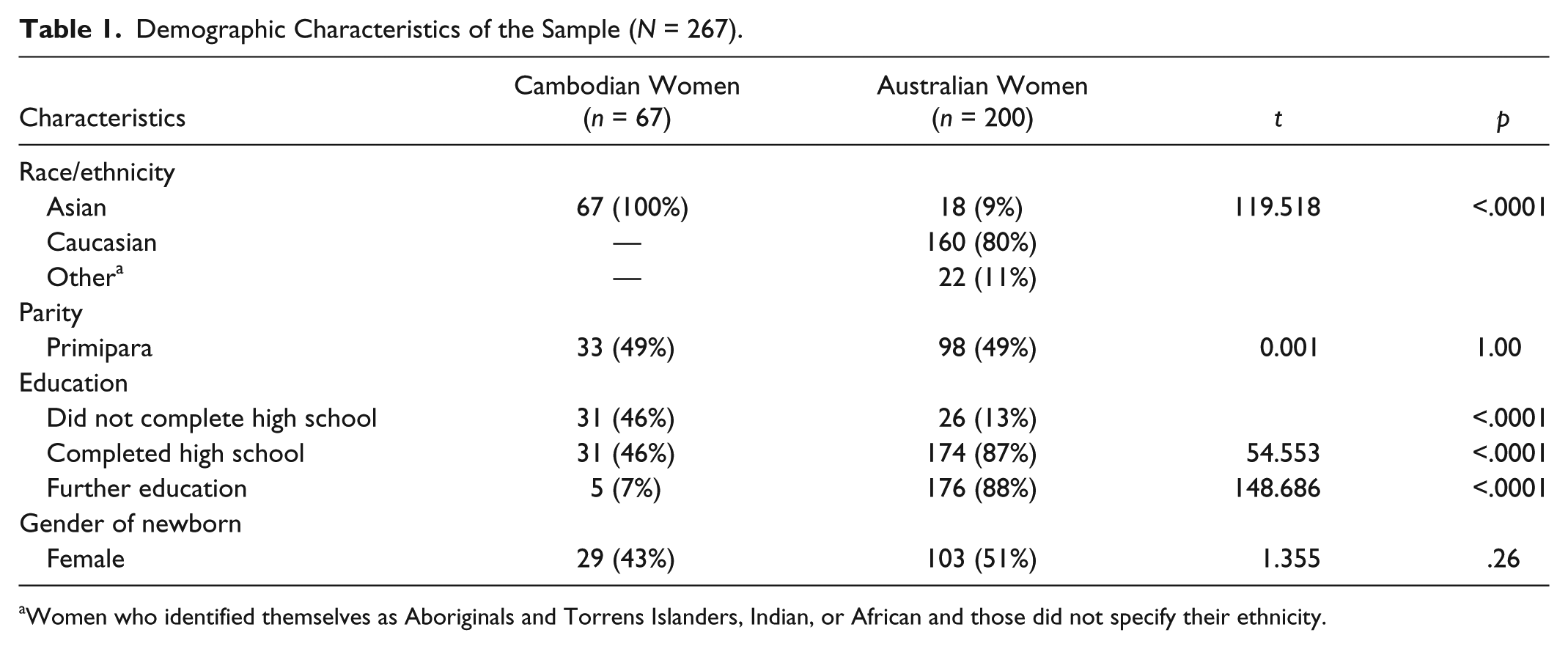
Women who identified themselves as Aboriginals and Torrens Islanders, Indian, or African and those did not specify their ethnicity.
Human Milk Fatty Acid Composition
Human milk was collected a median of 15 weeks postpartum (interquartile range = 9-22) in the Cambodian cohort and at 13 weeks postpartum (interquartile range = 13-14) in the Australian cohort. No difference was found in the milk fatty acid composition of Cambodian participants who were assigned to either the intervention or the placebo group, so the combined data are presented.
The total fat content of human milk of Cambodian participants was significantly lower than that of Australian participants (2.90 vs. 3.45 g/dL, p = .028). Palmitic acid (16:0) and oleic acid (18:1 omega-9) are the two main fatty acids in the milk samples (Table 2), which make up approximately 50% of the total fatty acids in both cohorts. The percentages of trans, monounsaturated, and n-6 PUFAs were lower, while saturated fatty acids were higher in the Cambodian cohort compared with the Australian cohort (Table 2). Although the percentage of total n-3 fatty acids was lower in the Cambodian cohort compared with the Australian cohort, the percentage of DHA (22:6 n-3) in the Cambodian cohort was almost double that in the Australian cohort. These differences persisted after adjustment for differences in demographic characteristics, including mother’s age, race, BMI, and educational background and infant’s age at the time of collection.
Comparison of Human Milk Fatty Acid Composition in Each Group as Weight Percentage of Total Fat (w/w%) (N = 267).
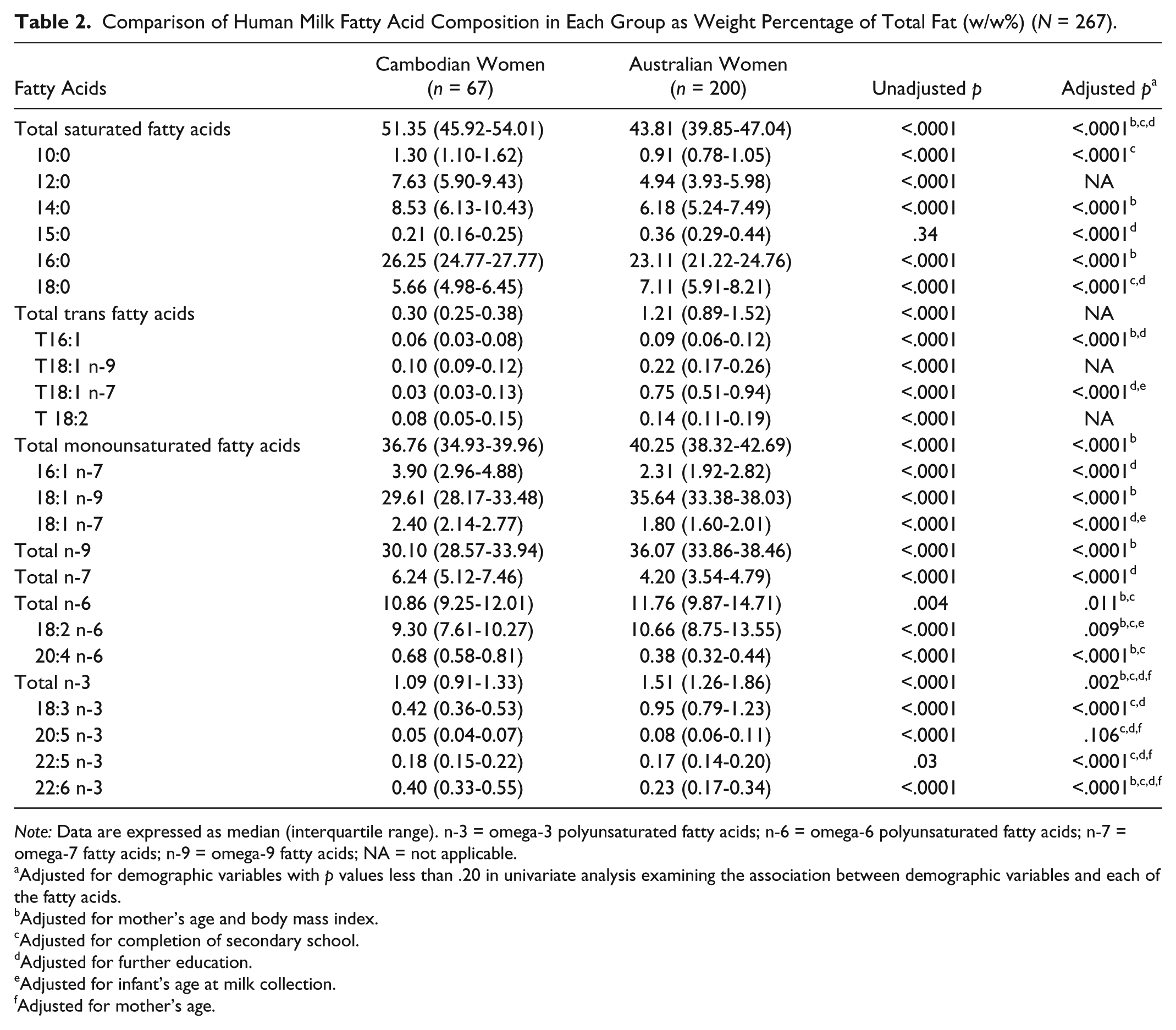
Note: Data are expressed as median (interquartile range). n-3 = omega-3 polyunsaturated fatty acids; n-6 = omega-6 polyunsaturated fatty acids; n-7 = omega-7 fatty acids; n-9 = omega-9 fatty acids; NA = not applicable.
Adjusted for demographic variables with p values less than .20 in univariate analysis examining the association between demographic variables and each of the fatty acids.
Adjusted for mother’s age and body mass index.
Adjusted for completion of secondary school.
Adjusted for further education.
Adjusted for infant’s age at milk collection.
Adjusted for mother’s age.
Discussion
We have reported the first study of the human milk fatty acid composition of Cambodian participants and compared fatty acid composition with that of Australian participants. Our results demonstrate that the human milk of Cambodian women was lower in total fat content and the percentage of trans fat content but higher in the percentage of short- to medium-chain fatty acids and DHA compared with Australian participants.
The differences observed in human milk fatty acid composition between participants in Cambodia and Australia may be explained by differences in the dietary patterns of the two countries. Although dietary intake data were not collected in our study, the national food balance sheet (Food and Agriculture Organization of the United Nations, 2014) indicates that the Cambodian dietary pattern is characterized by high intake of carbohydrate, mainly from white rice, which contributes to more than 70% of daily energy intake, while fat and protein contribute to less than 10% of energy intake. In contrast, carbohydrate contributes to 45% of total daily energy in Australian women of childbearing age, while protein and fat make up 18% and 35% of daily energy intake, respectively (Australian Bureau of Statistics, 2014). It has been reported that among lactating women whose diet was sufficient in energy but inadequate in dietary fat, human milk was rich in lauric acid (12:0) and myristic acid (14:0), which can be synthesized endogenously from dietary carbohydrate (Insull, Hirsch, James, & Ahrens, 1959). Thus, the higher content in lauric and myristic acids and overall total saturated fatty acids in the human milk of the Cambodian cohort may be explained by the high carbohydrate intake in the Cambodian diet. Compared with the Cambodian diet, the typical Australian diet has much less cereal grain and vegetable products but is higher in meat, egg, and dairy products (Australian Bureau of Statistics, 2014; Food and Agriculture Organization of the United Nations, 2014). Moreover, the percentage of trans fat content in the human milk of the Australian participants was significantly higher than in Cambodian participants, which may reflect higher intake of fast food and processed food in Australia, as trans fat in human milk is derived only from dietary sources (Innis & King, 1999). In addition, high dairy consumption in the Australian diet may also contribute to the high trans fat content in human milk from Australian participants. Interestingly, the human milk of the Australian participants contains a significantly higher percentage of ALA (and thus total n-3 PUFA) but a lower percentage of DHA than that of Cambodian participants. This may be explained by lower intake of fish and seafood products among Australian women, as fewer than 20% of Australian women reported consuming fish at least once a day (Australian Bureau of Statistics, 2014) compared with 95% of Cambodian women (In et al., 2015). DHA in human milk may be sourced from the maternal diet directly or endogenously converted from ALA to eicosapentaenoic acid, to docosapentaenoic acid, and eventually to DHA. However, the rate of conversion from ALA to DHA is very limited (Innis, 2014). Therefore, the higher percentage of ALA but lower percentage of DHA seen in the milk samples of Australian participants compared with Cambodian participants may also reflect the inefficient conversion of ALA to DHA.
Although our Cambodian sample was small, it has been shown that a majority of the Cambodian population share similar dietary patterns despite small regional and seasonal variations (In et al., 2015). The Australian participants in our study were randomly selected from the PINK study, whose participants were recruited from two major public hospitals in South Australia. The participants in the PINK study appear to be representative of South Australian pregnant women, since demographic characteristics were similar to those previously reported (Scheil et al., 2016).
Limitations
One of the limitations of our study is that the human milk samples were collected at different time points after birth, and different fractions of human milk were collected in the two cohorts, which may have contributed to the observed differences in fatty acid composition. However, human milk fatty acid composition is relatively stable once mature human milk is fully established, which is approximately 2 weeks after birth (Ballard & Morrow, 2013). Because the milk samples were collected an average of 3 to 4 months postpartum in both cohorts, the small difference in the timing of collection is expected to have a minimal impact on the observed differences in fatty acid composition between the two cohorts. The total fat content of human milk may change over a course of breastfeeding, as it has been shown that total fat content was higher in hindmilk than in foremilk (Ballard & Morrow, 2013), hence the use of different milk fractions (foremilk vs. full milk) may introduce bias to the results of total fat content. However, fatty acid composition is independent of total fat content, because it is expressed as a percentage of total fat. A study conducted by Gibson and Kneebone (1980) determined the fatty acid composition of human milk from 19 participants on days 3 and 5 postpartum, before and after feeding. No differences were found in fatty acid composition measured before or after feeding on either day (Gibson & Kneebone, 1980). Therefore, the impact of the different protocols used in the collection of human milk samples on the observed differences in fatty acid composition between the two cohorts should be minimal.
Another limitation of our study is that we did not assess the dietary intake of the participants. Although the fatty acid composition of human milk is determined primarily by maternal dietary patterns, particularly the type of fat in the diet, the differences in the socioeconomic status between the two cohorts might potentially contribute to the different fatty acid compositions between the cohorts. Further research, with a larger sample size and detailed dietary records of the populations and the use of a “gold standard” method of human milk collection to sample human milk multiple times over a 24-hour period, is warranted to confirm the findings of this study.
Conclusions
Differences in fatty acid profiles between Australian and Cambodian participants were seen in total fat and in n-6 and n-3 PUFAs, including LA, AA, ALA, and DHA. These differences are likely a reflection of differences in dietary patterns between the two populations. Further research to investigate the level of human milk fatty acid content that is associated with optimal growth and development of infants and the dietary pattern associated with optimal human milk fatty acid composition is warranted.
Footnotes
Acknowledgements
We thank the mothers for their participation; staff members from Helen Keller International, Cambodia; the Cambodian Ministry of Planning; the Cambodian Ministry of Health; the National Institute for Public Health; and Healthy Mothers, Babies and Children at the South Australian Health and Medical Research Institute for their assistance with recruitment and data collection.
Authors’ Note
Content in this manuscript was part of Chang Gao’s thesis submitted to the University of Adelaide to fulfill a bachelor of food and nutrition science honors degree, of which the student was awarded first-class honors. The student has commenced the PhD program in science with the University of Adelaide.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Maria Makrides and Robert A. Gibson have received honoraria for scientific advisory board contributions to Fonterra. All honoraria are paid to Healthy Mothers, Babies and Children, South Australian Health and Medical Research Institute, to support continuing education activities for students and postgraduates. No other authors declare any conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PINK study was funded by a National Health and Medical Research Council (NHMRC) project grant (626800). Cambodian data collection was undertaken with the financial support of a Grand Challenges Canada Stars in Global Health Round VI Phase I grant (S6 0490-01-10). Chang Gao was supported by the School of Agriculture, Food and Wine for the honors degree scholarship and project funding. Kyly C. Whitfield received funding support through the International Development Research Centre Doctoral Research Award and the Canadian Institutes of Health Research Doctoral Award – Frederick Banting and Charles Best Canada Graduate Scholarship. Maria Makrides was supported by the NHMRC Principal Research Fellowship (APP1061704), and Robert A. Gibson was supported by the NHMRC Senior Research Fellowship (APP 1046207).