
Abstract
Background:
The most utilized pasteurization method in donor human milk banks is Holder pasteurization (heating 62.5 °C for 30 min). However, many bioactive proteins are heat sensitive and are inactivated.
Research Aim:
To determine the results of a range of heating regimes on the activities of xanthine oxidase, lactoperoxidase and lysozyme, the concentrations of immunoglobulin A and lactoferrin, as well as bacterial inactivation.
Method:
This prospective, cross-sectional, intervention study was designed to measure the influence of heating temperatures on bioactive components in donor human milk. Milk samples were processed at 40, 50, 55, 62.5, 75, 127 °C and the activities of the enzymes, and the concentration of immune proteins, were measured.
Results:
No bacterial colonies were detectable, using standard culture methods, after heating above 50 ºC. All proteins studied retained over 60% concentrations or activities when the pasteurization temperature was 50 ºC or lower, while their concentrations or activities were lost at higher temperatures. For lactoferrin, the residual concentration was above 80% when heating temperature was under 55 °C, while only 20% remained after Holder pasteurization. Both xanthine oxidase and lactoperoxidase had little residual activity when temperatures were above Holder pasteurization. Lysozyme retained a greater proportion of residual activity than other proteins, following heating at all temperatures.
Conclusions:
The concentrations or activities of immune proteins and bioactive enzymes decreased when heated above 50 °C. The results of this study can be used to design temperature control guidance during alternative methods of pasteurization.
Keywords
Key Messages
The effect of a range of temperatures on bioactive proteins is still unknown.
Human milk heated below 50 ºC retained over 60% concentration for immunoglobulin A, lactoferrin and activity of xanthine oxidase, lactoperoxidase and lysozyme, while Holder pasteurization (heating at 62.5 ºC for 30 min) inactivated bioactive proteins in human milk.
Lysozyme had a high activity retention when heated up to 127 °C, suggesting its relatively high heat stability.
Heating-induced loss of activities of biomolecules in human milk suggests temperature control is needed even for alternative pasteurization methods.
Background
Human milk provides optimal nutrition for human infants. Breastfed infants have many advantageous outcomes, both in the short and long term, when compared with formula-fed infants (Meng et al., 2021). These outcomes are ascribed in part to the various nutrients and bioactive proteins present in human milk.
Donor human milk is, however, usually heat-treated to reduce bacterial counts prior to feeding newborn infants (Zhang et al., 2022). Currently, a common pasteurization method in donor human milk banks is Holder pasteurization (HoP), where milk is heated at 62.5 °C for 30 min (Meng et al., 2021). Although ongoing efforts are being made to explore alternative pasteurization methods for human milk, it is inevitable that some heat will be produced during the processing, for example, high pressure and microwave processing produces heat. Many bioactive proteins are, however, sensitive to heat processing (Bakar et al., 2021).
It is particularly important to study the individual components of human milk and the changes that occur in donor human milk during heat pasteurization. The bioactive proteins in human milk: immunoglobulin A (IgA), lactoferrin, xanthine oxidase (XO), lactoperoxidase (LPO), and lysozyme, have each received attention (Lönnerdal, 2016). IgA, accounting for 90% of the total immunoglobulins, is able to transfer maternal immunity protect infants from pathogens via the entero-mammary pathway (Perrin et al., 2017). Lactoferrin constitutes the most concentrated component of bioactive proteins in human milk, with antibacterial, antioxidant, and anti-inflammatory activities (Picaud & Buffin, 2017). XO is an important protein in the milk fat globule membrane, and it provides antimicrobial protection in the neonatal gut (Zhang et al., 2022). The activity of LPO—a member of the peroxidase family of enzymes—is dependent on hydrogen peroxide generation by the XO, and has a key role in preventing maternal mastitis as well as protecting newborn infants from gut infection (Zou et al., 2021). Lysozyme is an essential antibacterial enzyme in human milk, and its concentration in human milk is extremely high when compared to bovine milk (Chandan et al., 1965).
The aim of this research was to determine the results of a range of heating regimes on the activities of xanthine oxidase, lactoperoxidase and lysozyme, the concentrations of immunoglobulin A and lactoferrin, as well as bacterial inactivation.
Methods
Research Design
A prospective, cross-sectional, intervention study was selected, (Hartle et al., 2018) as the study aim was to determine the results of temperatures on bioactive components of human milk. Ethics approval for the collection of human donor milk samples was sought and obtained from the Human Research Ethics Committee of RBWH and University of Queensland Human Research Ethics. Project (2019002894), and was approved on December 19, 2019.
Setting and Relevant Context
The Australian health system is a publicly funded health system, centrally financed in a similar way to the National Health Service of the United Kingdom. The Royal Brisbane Women’s Hospital (RBWH) is a large public hospital centrally located within Brisbane, the capital city of the state of Queensland. It was opened more than 150 years ago, and over 4,800 babies were delivered in the Maternity Department in the last year (2021). At the Grantley Stable Neonatal Unit within the RBWH more than 1,500 premature and seriously ill babies, from the large area of Queensland and northern New South Wales (approximately 1.9 million km2), are treated each year. The Human Milk Bank was within the RBWH but is now located within the Red Cross Service, nearby in Brisbane, and is provided with donor milk from mothers over 18 years old of a variety of ethnic backgrounds. The milk is screened and pasteurized to ensure its drug and microbiological safety.
Sample
One human milk sample each was collected from three individual donors who had given birth to term babies. As the genetic variance of the immunological components targeted in this study was unknown, the study excluded non-Caucasians. Inclusion criteria were women who were expressing human milk and who approached the Milk Bank with excess milk. The sample size was deemed appropriate for the testing.
Measurement
After collection, the individual human milk samples were transported to the laboratory on ice in less than 30 min, aliquoted and stored at -80 °C. All milk samples were thawed at room temperature and carefully mixed before use. Raw (unpasteurized) cow milk was purchased from a local “health food” store. Infant formulas were purchased from a local supermarket and reconstituted with distilled water to a concentration of 150 g/L. As there were large differences in the activities of bioactive components when comparing pre- and post-heated samples, the small sample numbers (n = 3) were found to be statistically valid and reliable (using triplicate assays) for quantifying the effects of heating.
Three individual human milk samples were treated at 40, 50, 55 or 62.5 °C for 30 min, 75 °C for 15 s, or 127 °C for 15 s. For samples processed below 80 °C, four polypropylene tubes each containing 1 ml of milk were immersed in a shaking water bath at the corresponding treatment temperature, with three tubes used for assays and one tube used to monitor temperature by a thermocouple. When the desired temperature was reached, milk was kept in the water bath for the time prescribed above. After this time, the tubes were immediately transferred to an ice slurry bath to cool. For 127 °C heating, a rotating oil bath was used with three glass tubes containing 2 ml of human milk each, for 15 s, then cooled immediately on ice.
The total plate count of live bacteria in raw and processed human milk samples was analyzed using spread plate technique on nutrient agar and incubated at 37 °C for 48 hr and the bacterial numbers were expressed as colony forming units per ml (CFU/ml). Concentrations of IgA and lactoferrin in human milk were determined using specific human ELISA kits (Abcam, Victoria, Australia) according to the manufacturer’s protocol. Fluorescence was recorded with a FLUOstar Omega fluorimeter (BMG Labtech, North Carolina, USA) at excitation/emission wavelengths of 544/590 nm. In raw cow milk and infant formulae, IgA was measured with an IgA cow ELISA kit (ab190516) from Abcam, and lactoferrin was determined using an ELISA kit (E11126) from Bethyl Laboratories (Alabama, USA). XO activity was determined by the rate of production of hydrogen peroxide as described by Zou et al. (2020). LPO activity was evaluated by measuring the rate of formation of resorufin, which is a red-fluorescent oxidation product derived from the Amplex Red substrate, as described by Zou et al. (2021). Lysozyme activity was measured based on a turbidimetric assay using Micrococcus lysodeikticus (Sigma-Aldrich, New South Wales, Australia) as the substrate, as described by Sousa et al. (2014). Fresh Micrococcus lysodeikticus cell suspension (0.015% w/v) was prepared by dissolving Micrococcus lysodeikticus ATCC 4698 lyophilised cells in potassium phosphate buffer (50 mM, pH 6.24). The reaction was initiated by adding 0.1 ml of appropriately diluted human milk to 2.5 ml substrate. The decrease in absorbance at 450 nm was immediately recorded for 3 min at 10 s intervals using UV-Vis spectrophotometer 1800 (Shimadzu, Kyoto, Japan), at 25 °C. Human lysozyme standard (Sigma, St. Louis, MO) was used to quantify the concentration of lysozyme. For each pasteurization parameter, three individual samples were measured in triplicates (nine measurements in total). Hence, the results represent the average of nine measurements. The results were expressed in repeatability measures (SD). For the measurement of IgA, lactoferrin using ELISA kit, we followed the user manual for the calibration, cleaning, and checking the equipment. For other measurements, quality control procedures included the use of blanks and triplicate samples. All SDs had CVs below 10% of the means.
Data Collection
Milk analysis was completed between December and February 2020. Frozen unpasteurized human milk samples, from informed donors from the Queensland Milk Bank, were obtained in sterile storage bags. Donors were screened for infectious diseases and drugs as required by the Queensland Milk Bank. Women were approached by the Queensland Milk Bank staff at the time of donor registration. Women were provided with written information regarding the study and opportunity for further information or clarification at that time or at a convenient time for phone follow-up. Consent was obtained prior to study commencement. Samples were deidentified upon collection and no further donor information was recorded.
Data Analysis
All replicate data were expressed as mean and standard deviation. Statistical analysis was conducted using SPSS (Version 25.0). One-way ANOVA was used for significance analysis, with Tukey being selected as “Equal Variances Assumed.”
Results
Total Microbial Count in Human Milk
The effects of temperature on the inactivation of bacteria in human milk are shown in Table 1. The initial number of bacteria (as colony forming units, CFU) in human milk in the three samples varies from 3.15 ± 0.09 to 4.78 ± 0.10 log10 CFU/ml. After treatment at 40 °C, there is only about 0.6 log10 CFU/ml reduction in total bacterial count for all three samples. No bacteria are found in samples treated at 50 °C or above. Therefore, to achieve a 4 log10 reduction in total bacterial count in human milk, heat treatment at 50 °C for 30 min is sufficient, while milk treated at 40 °C for 30 min produces only a slight reduction in total viable bacteria.
The Results of Treatment at Different Temperatures on Total Bacterial Counts in Human Milk Samples (N = 3).
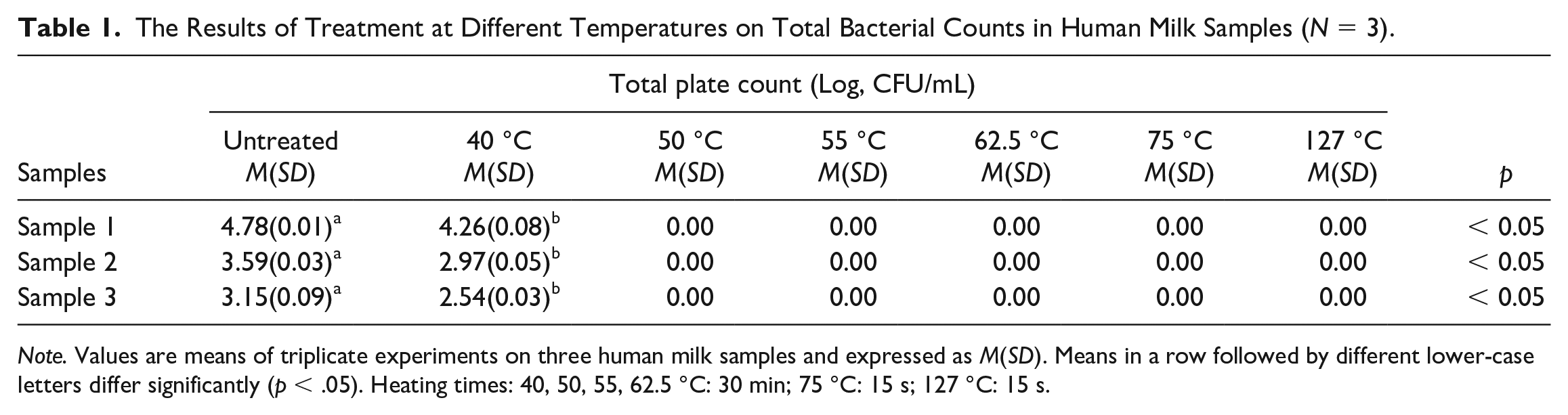
Note. Values are means of triplicate experiments on three human milk samples and expressed as M(SD). Means in a row followed by different lower-case letters differ significantly (p < .05). Heating times: 40, 50, 55, 62.5 °C: 30 min; 75 °C: 15 s; 127 °C: 15 s.
Immunoglobulin A Concentration in Human Milk
The effect of temperature on concentration of IgA, as determined by its immunoreactivity as an antigen to the antibody in the kit, in human milk, is shown in Figure 1A. The immunoreactivity in three different raw human milk samples is shown in Table 2. The mean retention of the immunoreactivity of IgA decreases as the temperature increases from 40 to 127 °C (Figure 1A).
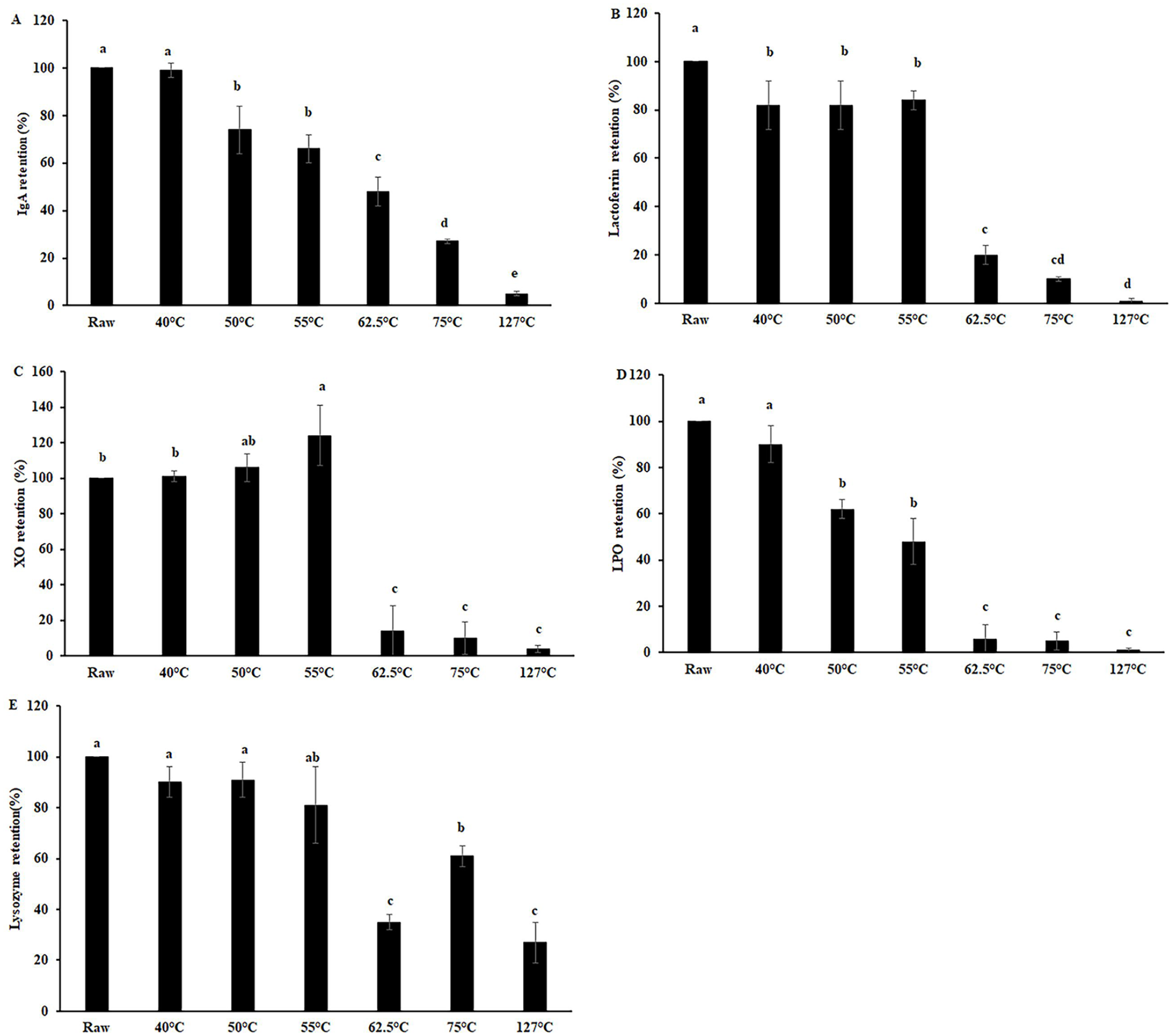
Effect of Heating Human Milk (N = 3) at Different Temperatures on Retention of (A) Immunoglobulin A (IgA), (B) Lactoferrin, (C) Xanthine Oxidase (XO), (D) Lactoperoxidase (LPO), and (E) Lysozyme Concentration or Activity.
Bioactive Components in Three Raw Human Milk, One Raw Cow Milk and Four Infant Formulae Samples (N = 3).
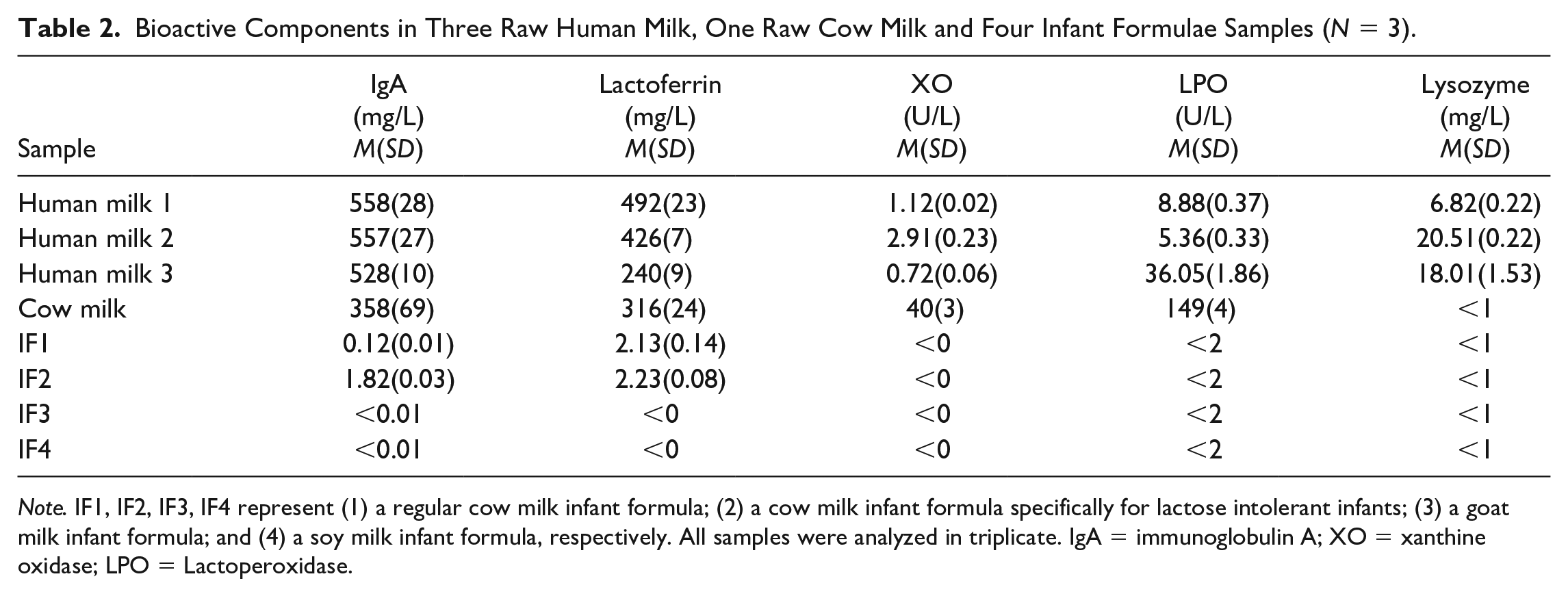
Note. IF1, IF2, IF3, IF4 represent (1) a regular cow milk infant formula; (2) a cow milk infant formula specifically for lactose intolerant infants; (3) a goat milk infant formula; and (4) a soy milk infant formula, respectively. All samples were analyzed in triplicate. IgA = immunoglobulin A; XO = xanthine oxidase; LPO = Lactoperoxidase.
Lactoferrin Concentration in Human Milk
The concentration of lactoferrin in the three different raw human milk samples analyzed is shown in Table 2, which was within the range of 440–4400 mg/L for mature human milk reported by Rai et al. (2014). The mean retention of lactoferrin processed at 40, 50, 55, 62.5, 75, and 127 °C is shown in Figure 1B. Over 80% of lactoferrin is maintained while heating up to 55 °C for 30 min (Figure 1B). The concentration of lactoferrin sharply drops to 20% retention following HoP treated human milk at 62.5 °C; but this retention is significantly higher compared to at 75 °C and 127 °C.
Xanthine Oxidase Activity in Human Milk
The XO activity in three different untreated human milk samples is shown in Table 2. The percent retention of the enzymatic activity of human milk XO in three separate human milk samples does not decrease or even increases when the heating temperature is below 55 °C
Lactoperoxidase Activity in Human Milk
The LPO activity in three different raw human milk samples is demonstrated in Table 2. The percent retention of the enzymatic activity of human milk LPO when heated at 40, 50, 55, 62.5, 75, and 127 °C decreases gradually in Figure 1D.
Lysozyme Activity in Human Milk
The lysozyme activity in three different untreated human milk samples is shown in Table 2. The percent retention of the lysozyme activity using Micrococcus lysodeikticus as the substrate does not change significantly when heating at temperature below 55 °C and the retention is higher at 75 °C than at 62.5 °C (Figure 1E).
Bioactive Components in Raw Cow Milk and Infant Formulae
The concentrations of IgA and lactoferrin in raw cow milk are similar to those in human milk (Table 2). LPO and XO activities in raw cow milk are much higher than that in human milk. The activity of lysozyme in cow milk is much lower than that in human milk (Table 2). The activities or concentrations of the above latter five components are very low in four infant formulae (IF) samples tested (Table 2). These results suggest significant loss of activity or concentration of important bioactive components during the processing of raw cow milk into infant formulae.
Discussion
All bioactive proteins studied had over 60% concentration or activity when the heating temperature was at or below 50 ºC, while their activity or concentration was lost upon heating to higher temperatures. Weaver et al. (1998) found that IgA levels in 1590 human milk samples ranged from 422 to 1105 mg/L.
Permanyer et al. (2010) and Franch (2010) reported human milk IgA concentration to be in the range of 550 mg/L to 9100 mg/L. Upon processing the human milk under HoP conditions, the IgA content significantly decreased to ~48% of the original concentration, which is consistent with other studies (Contador et al., 2013). These variations in different studies may be explained by differences during HoP, including the time taken to reach the exact temperature, cooling time, as well as the stage of lactation, and the amount of milk treated. In the present study, small aliquots (1 ml) were thermally processed and cooled by an ice-water bath immediately after heating, while 400 µL to 10 ml sample volumes were used in other reports. Since higher volumes of milk are processed in human milk banks, about 150 ml per bottle, it could be anticipated that a higher loss of IgA may happen in these circumstances, since longer times are required to meet the required temperature and then cool down after heating. We found that heat treatments as low as 50 ºC significantly affected the IgA concentration in human milk.
In untreated raw human milk, we noted that the concentration of lactoferrin was similar to that reported previously (Rai et al., 2014). Following HoP, our lactoferrin concentration retention results were consistent with previous reports (Tully et al., 2001). However, others reported that only 9% of lactoferrin concentration was maintained after HoP (Christen et al., 2013; Ewaschuk et al., 2011). These differences may, again, be caused by differences in heating and cooling rates, treatment volumes, and pasteurization bottle parameters, which may affect the overall heat transfer rate during processing.
We focused on three milk enzymes in this study: LPO, XO, and lysozyme. XO generates “reactive oxygen species” (peroxide/H2O2) and has been reported to inhibit S. aureus, E. coli and Salmonella (Harrison, 2006). Milk XO is also bacteriostatic in the neonatal gut, as the neonatal stomach is pH neutral (Harrison, 2006). LPO in milk, as well as peroxidases in saliva, form an antimicrobial “oxidative enzyme system” by using H2O2 to produce “reactive nitrogen species” from nitrate or microbiocidal hypothiocynate from thiocyanate (Bansal et al., 2021). Previously we examined, for the first time, the interaction of human milk with infant saliva during suckling (Al-Shehri et al., 2015). We found that human milk XO is activated by raised hypoxanthine and xanthine levels from infant saliva (10-fold higher than adult saliva), to produce peroxide. This activates LPO and saliva peroxidases to generate bacteriostatic free radicals that inhibit pathogenic bacteria in vitro, for example, S. aureus (Sweeney et al., 2018).
Low activity of XO in human milk has been reported previously (Zou et al., 2020). This may be due to the high percentage (> 95%) of an inactive form of XO present in human milk compared with 30%−40% in cow milk (Zou et al., 2020). Xanthine oxidase has two inactive forms: demolybdo-XO lacks molybdenum (Mo; and possibly molybdopterin conjugate), and desulfo-XO, which, although containing Mo, has the catalytically essential Mo = S group replaced by inactive Mo = O (Gutteridge et al., 1978). XO activity increased as the heating temperature raised from 40 °C to 55 °C, although it was significantly higher than in the raw milk sample only at 55 °C. This increased XO activity caused by low heating may be due to the transformation of inactive forms of XO to the active form. HoP processed human milk had higher XO activity than high temperature short time (HTST, 75 °C/15 s) pasteurized milk. To our knowledge, no previous data are available for the effect of heat treatment on human milk XO, presumably because of detection limits. The XO activity in human milk was much lower compared to previously reported XO activity in cow milk (Zou et al., 2020).
Previous researchers have reported that LPO are limited, due to LPO’s very low activity in human milk, but the highly sensitive Amplex Red assay used here made accurate quantification possible. Others reported it to be undetectable (Sousa et al., 2014), or of very low activity (Akinbi et al., 2010) in human milk. As shown in Table 2, the activity of human LPO measured here was only residual compared to that found in cow milk, which was in accordance with the study of Gothefors and Marklund (1975). LPO has been reported to be partially active when subjected to treatments using HoP (62.5 °C/30 min) or “high temperature-short time” (HTST) conditions. It has been reported that LPO is sensitive to heating over 80 °C (Barrett et al., 1999). For cow milk, Marín et al. (2006) reported a 50% reduction in LPO activity at 68 °C/105 min and 72 °C/6 min. For camel milk, however, 50% inactivation of LPO activity at 67 °C for 37 min and 71 °C for 4.4 min was reported (Trujillo et al., 2007). For human milk there appears to be no data available for the effects of pasteurization on LPO activity, because this enzyme has previously been considered to be “undetectable” in human milk (Sousa et al., 2014). Our results show that the degree of LPO denaturation increased with increasing temperature, with almost complete inactivation at and above 62.5 °C. When human milk was treated at or below 50 °C for 30 min, LPO activity had a retention of at least 60%. Considering the species differences and the low activity of LPO we detected in human milk, our results are comparable to previously available data.
Lysozyme is another major antimicrobial enzyme (Bansal et al., 2021), in much higher concentrations in human milk than cow milk. Sousa et al. (2014) reported that lysozyme activity in raw colostrum was 18,000 U/ml, measured using the same method as here, which was equivalent to 44 mg/L if calculated with the standard curve generated here. Sousa et al. also found that the activity of lysozyme in colostrum was almost three times higher than in mature milk. Lysozyme activity decreased significantly after HTST heating, at 75 °C for 15 s, which was in agreement with the research reported by Giribaldi et al. (2016) and Mayayo et al. (2016). This lysozyme retention was significantly higher (p < .05) than after HoP processing. This may be due to the longer time of heating during HoP. There was no significant decrease in the retention of lysozyme activity in milk treated at 40, 50 or 55 °C for 30 min, which has not been previously reported in the literature. The retention of lysozyme in HoP treated human milk reported here was in accordance with other reports, ranging from 40% to 80% (Czank et al., 2009; Sousa et al., 2014; Viazis et al., 2007). We highlight the effect of heating on some of the most important bioactive components in human milk. The physiological significance of loss of activity and or concentration of the bioactive enzymes and proteins upon heating, as measured in this study, will be an interesting future study.
Limitations
For a more comprehensive picture on the detrimental effects of heating on quality of human milk, other components of interest should be studied, for example, vitamins and oligosaccharides. The concentrations of bioactive components in human milk can vary greatly between lactating women owing to numerous factors. Although the number of samples were small, due to the large differences in activities of bioactive components in pre- and post-processed samples, the results were statistically significant. A larger number of samples may provide representative data for a particular population of donors. Also, some information about the participants providing the milk samples—data that was not collected—may have been relevant to provide, for example, postpartum duration, the time of sample collection during the day, age of the mother, and so on. As donors from only Caucasian background were included in the study, participants from a wider genetic background should be included in the future.
Conclusions
Based on our results, the overall processing temperature for alternative pasteurization, for examle, using high pressure, microwave, or pulsed electric field, should be controlled at or below 50 °C to retain the majority (over 60%) of the bioactive components’ activities in milk. The concentrations or activities of IgA, lactoferrin, and LPO in human milk decreased with increases in heating temperature, while there was a significant increase in XO activity following an increase in temperature from 40 °C to 55 °C. The highly sensitive fluorimetric methods that were used here outperformed those previously reported, and allowed accurate reporting of the effects of pasteurization on human milk LPO and XO activities. The results of this study will be useful in designing temperature limits during alternative pasteurization, to facilitate better donor human milk for infants.
Footnotes
Author Contribution(s)
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time this article was published, Jie Zhang was a research student at School of Agriculture and Food Science, The University of Queensland, Australia. Research advisors were John A. Duley, David M. Cowley, Paul N. Shaw, Peng Zhou, Nidhi Bansal. Authors report no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Australian National Health and Medical Research Council Ideas Grant (GNT1182038).