
Abstract
Background:
Web-based prenatal education is increasingly employed, but its association with increased breastfeeding and predictors of breastfeeding success is uncertain.
Research Aims:
Our primary aim was to evaluate our live, online intervention’s association with exclusive breastfeeding at hospital discharge. Secondarily, we aimed to describe participants’ reports of the intervention on predictors of breastfeeding success.
Method:
We used a retrospective quasi-experimental cohort design to assess the association between our intervention and exclusive breastfeeding at discharge. The intervention consisted of an evidence-based live, online, 2-hour class open to all prenatal patients and supporters at our urban community medical center from June 2020 through April 2022. Patient characteristics and breastfeeding rates were extracted from the electronic medical record. Samples were drawn using stratified random sampling. Three logistic regression models were conducted to assess the associations between the intervention and exclusive breastfeeding. Two surveys assessed the participant reports of the intervention.
Results:
Samples of the first model, comprised of 160 participants and 160 non-participants, were similar in important characteristics. Participants were 2.12 times (95% CI [1.12, 3.69]) more likely to exclusively breastfeed. Participants reported positively on the impacts of the intervention on breastfeeding predictors.
Conclusions:
Our live, online intervention was significantly associated with an increased likelihood of exclusive breastfeeding at hospital discharge. A randomized, prospective examination of the intervention’s association with breastfeeding duration would further define its impact.
Keywords
Key Messages
A knowledge gap exists regarding how web-based prenatal education can be best employed to impact breastfeeding rates.
Participants of our live, online prenatal educational intervention exhibited twice the likelihood of exclusive breastfeeding at hospital discharge compared with non-participants.
When the analysis was restricted to only those who had had a Cesarean delivery, there was no association between the intervention and exclusive breastfeeding.
Online interactive, web-based prenatal education can improve breastfeeding rates.
Background
Citing breastfeeding, or the provision of human milk as a public health imperative, the American Academy of Pediatrics (AAP), in its July 2022 policy statement, reemphasized its recommendation for exclusive breastfeeding for the first 6 months of life. The Academy’s recommendation to include breastfeeding in a child’s nutrition broadened to as long as mutually desired by mother and child for 2 years or beyond (Younger Meek & Noble, 2022). This policy is consistent with the World Health Organization (WHO) and the United States Center for Disease Control and Prevention (U.S. CDC) recommendations. The Joint Commission, the oldest and largest standards-setting and accrediting body in health care in the United States, uses Perinatal Quality Measure PC-05 to seek exclusive human milk feeding during the newborn’s entire hospitalization (The Joint Commission, 2015). However, fewer than 60% of U.S. women achieve their breastfeeding goals (Sriraman, 2018). By 6 months of age, according to the most recent U.S. CDC Breastfeeding Report Card, only 25% of infants receive exclusively human milk, and 56% receive any human milk (U.S. CDC, 2022).
While this chasm between breastfeeding recommendations and each family’s reality is multi-factorial and marked by racial and social inequities (U.S. CDC, 2019), the critical question for addressing our “public health imperative” is whether we can narrow this gap by targeting well-demonstrated predictors of breastfeeding success. Among these predictors are prenatal breastfeeding education (particularly focused on setting accurate expectations and improving maternal self-efficacy; Gregory et al., 2015; Redshaw & Henderson, 2012; Shafaei et al., 2020), strength of maternal breastfeeding intent (Colaizy et al., 2012; Ross-Cowdery et al., 2017), and partner/family support (Karmacharya et al., 2017; Mueffelmann et al., 2015; Thomas et al., 2017; Wang et al., 2018).
As the utilization of web-based healthcare and health education has increased significantly during the COVID-19 pandemic, examining whether breastfeeding success can be positively influenced via a live online platform is of increased interest and importance. Some studies have examined the relationship between web-based prenatal education, self-efficacy, knowledge, and attitudes about breastfeeding (Abuidhail et al., 2019; Amin et al., 2022; Sari & Altay, 2020). Other studies have examined postnatal web-based interventions to support breastfeeding (Cavalcanti et al., 2019). However, evidence is lacking regarding the relationship between interactive online prenatal education and improved breastfeeding rates and predictors of breastfeeding success (Gavine et al., 2022; Pradipta et al., 2021; Wong & Chien 2023).
One of the perinatal factors most strongly associated with lower exclusive breastfeeding is Cesarean delivery. In their analysis of 48 studies (representing data from 553,306 women in 31 countries), Prior et al. (2012) found that rates of early breastfeeding (any initiation or at hospital discharge) were lower after Cesarean delivery compared with after vaginal delivery (pooled OR: 0.57 (95% CI [0.50, 0.64]; p < 0.001). This discrepancy in early breastfeeding rates between vaginal and Cesarean deliveries underlies the importance of considering delivery type when examining breastfeeding-related outcomes, particularly early breastfeeding.
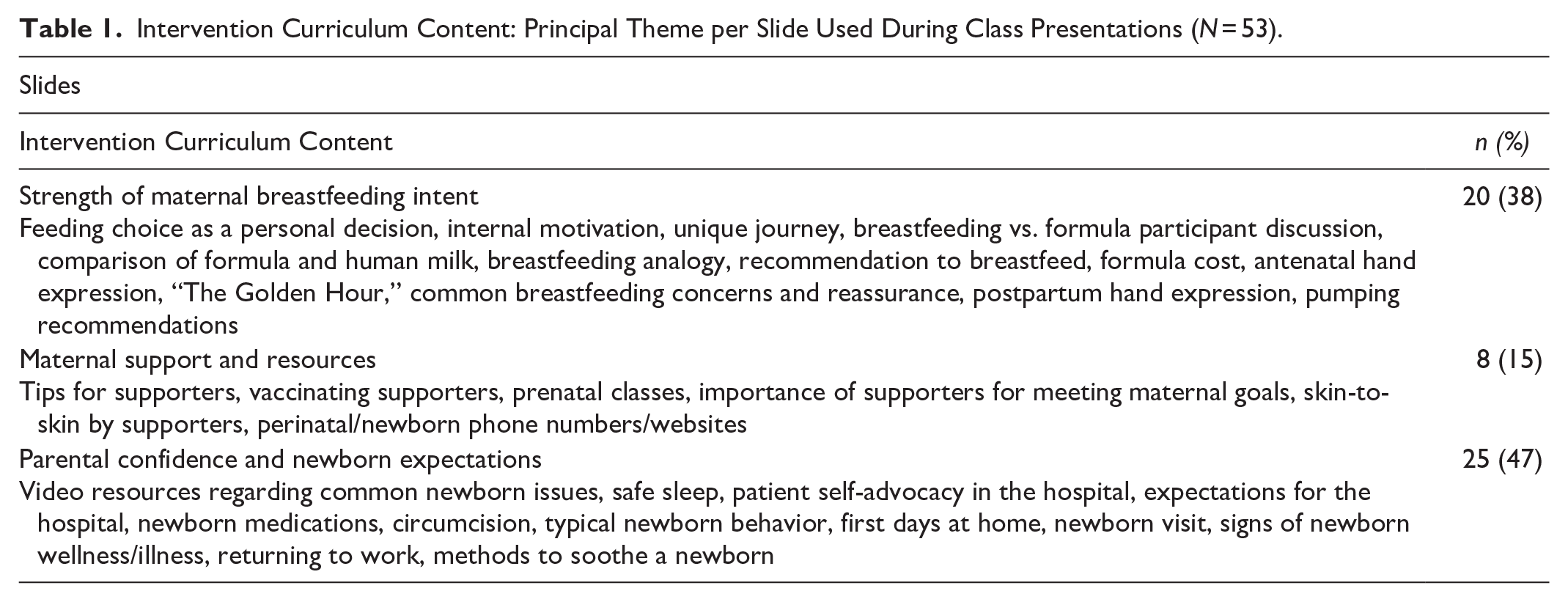
The objective of this quality improvement intervention was to implement a live, web-based prenatal class, which we designed with an evidence-based broad newborn curriculum (Table 1; Supplemental Figure 1—see the online Supplemental Materials), and to determine its association with exclusive breastfeeding (defined as the parent feeding their child only their own milk and inclusive of supplemental devices) from birth to hospital discharge. Further, we hypothesized that the intervention would have a stronger association with exclusive breastfeeding among participants delivering vaginally than by Cesarean section, given that the negative early breastfeeding predictor of Cesarean delivery might outweigh the benefits of our educational intervention (Li et al., 2021). Our secondary aim was to understand participants’ perception of the intervention regarding known breastfeeding predictors: strength of maternal breastfeeding intent, maternal self-efficacy and accurate expectations, and partner/family support.
Intervention Curriculum Content: Principal Theme per Slide Used During Class Presentations (N = 53).
Methods
Research Design
By retrospective quasi-experimental cohort design, we evaluated the intervention’s association with exclusive breastfeeding at hospital discharge. The Kaiser Permanente Northern California Institutional Review Board reviewed our quality improvement study and did not characterize it as research.
Setting and Relevant Context
This intervention occurred at an urban community medical center in Sacramento, California, with approximately 3,000 deliveries per year. According to internal institutional data for 2022, English is the primary language spoken by 93% of patients delivering at the medical center, and the intervention was offered in English only. The study hospital is part of a large not-for-profit healthcare organization and about 23% of deliveries are publicly insured, for which a low-income level is a prerequisite. The medical center offers no-cost consultation with an International Board Certified Lactation Consultant (IBCLC) 7 days a week, both on the postpartum unit and in the newborn follow-up visit after discharge. The medical center does not have a Baby Friendly USA designation. On the labor and delivery unit, maternal feeding intent is asked and recorded in the electronic medical record (EMR) upon admission. Human milk substitutes are available per parent request. No banked donor human milk is provided as an alternative to a human milk substitute. Most dyads are discharged approximately 24 hours after vaginal delivery and 48 hours after Cesarean section delivery. Per neonatal hypoglycemia protocol, oral dextrose gel is offered twice to treat asymptomatic hypoglycemic infants (screened due to hypoglycemia risk factors) before a human milk substitute is introduced, unless parental preference is for a human milk substitute. For 2020–2023, exclusive breastfeeding at hospital discharge (with criteria identical to The Joint Commission PC-05 criteria) for the medical center averaged 71%.
Sample
Our target population for the intervention was all pregnant patients from 24 to 36 weeks gestational age obtaining prenatal care at our medical center. All women in this target population met the inclusion criteria for participation. The intervention was standardly offered at prenatal visits and participation was voluntary and without compensation. Patients choosing to enroll did so via a phone call to the health education department or at prenatal visits by requesting an obstetric provider to assist with electronic enrollment.
Our initial population totaled 4,912 patients (Figure 1). Exclusion criteria for analysis were mothers of infants born at less than 37 weeks of gestation, or requiring neonatal intensive care unit (NICU) admission. Participants who were not patients but were health professionals attending the intervention for educational purposes were also excluded from the analysis. Likewise, participants who did not give birth at our medical center were excluded from the analysis. A total of 481 participants attended the intervention, with an average of 24 participants per session (range of 10–40 participants per session). After applying exclusion criteria, 332 participants and 3,868 non-participants remained for analysis (Figure 1).
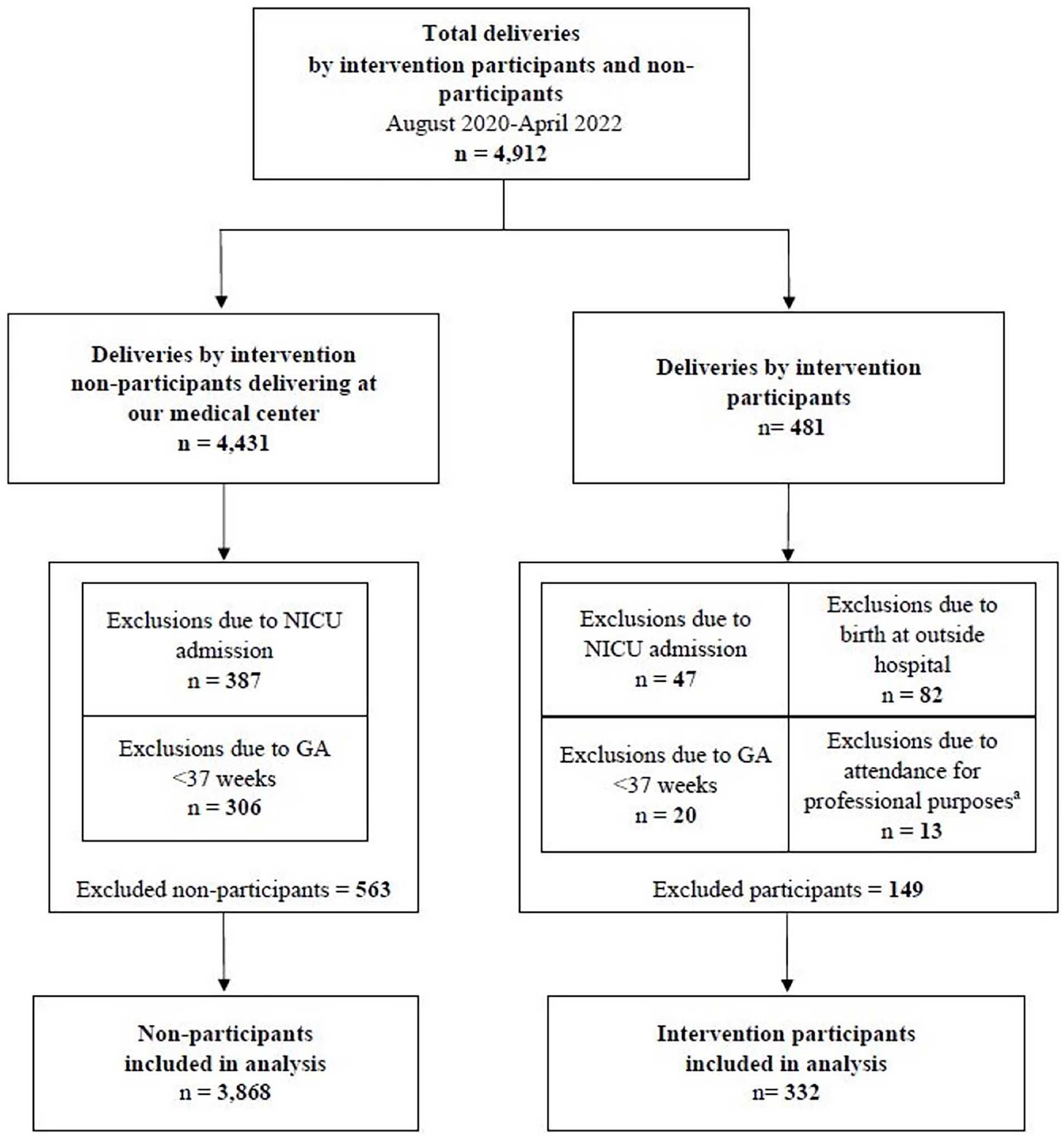
Participant and Non-Participant Flow From Delivery to Analysis.
Samples for three different models were drawn using stratified random sampling with a 1:1 ratio for intervention and non-intervention patients. The first model aimed to understand if the intervention was significant in the intervention versus non-intervention group. The second and third models aimed to examine the significance by delivery method. A power analysis to estimate the sample size for the first two models was performed with the goal of achieving 80% power (effect size of 0.69) at a 5% significance level. The effect size of each model was based on 160 intervention participants and 160 patients who did not receive the intervention. In the first model, participants who delivered both vaginally and using the Cesarean method were included. In the second model, only those delivering vaginally were included. Due to the limited number of patients who delivered by Cesarean section, the third model was comprised of 70 intervention participants and 70 who did not receive the intervention.
To understand the participant-reported influence of the intervention, we distributed surveys to all intervention participants immediately upon completion of the class and again after hospital discharge. We received 117 responses from the post-intervention survey. Thirty-seven participants responded to the post-hospitalization survey.
Measurement
Intervention
The intervention studied was a 2-hour, interactive, online prenatal education class, built on a curriculum with evidence-based components for expectant mothers and their supporters. Core curriculum components included key breastfeeding predictors: strength of maternal breastfeeding intent, maternal self-efficacy and accurate expectations, and partner/family support (Table 1; Supplemental Figure 1). Curriculum content aligns with The American Academy of Pediatrics’ policy statement on breastfeeding and the use of human milk (Younger Meek & Noble, 2022) and recommendations on newborn care (Bloomfield et al., 2020).
The intervention was created by pediatricians (this manuscripts’ authors J.G. and L.W.) with input from our medical center’s IBCLCs and obstetricians. To promote the adult learning model of peer-centered group discussion, the class was designed to be interactive, with participants encouraged to ask questions and converse largely through the chat feature. The class was offered one evening per month and facilitated by two pediatric hospital medicine physicians and one IBCLC, all compensated for their time. The rationale for selecting pediatricians to co-facilitate the intervention was twofold: (1) to draw patients interested in meeting with a pediatrician prenatally, independent of infant-feeding goals; (2) because physician-recommended breastfeeding has been associated with increased breastfeeding success (Gurmankin et al., 2002; Lawrence, 1982). In promoting the class to potential participants, two points were emphasized: (1) the program’s broad newborn care curriculum and interaction with a pediatrician (with the intent to draw participants regardless of feeding intentions); and (2) the importance of bringing partners/supporters to the class.
Intervention participants were defined as pregnant patients who attended the 2-hour prenatal education class. Attendance was recorded as individuals who joined the online meeting room. Hospital staff were not informed about which patients had participated in the intervention during patients' delivery hospitalization. Variables were analyzed for intervention participants and non-participants delivering August 2020–April 2022. Independent variables consisted of intervention (classified as yes and no), delivery method (classified as vaginal and Cesarean delivery), maternal age (classified as < 25 years, 25–34years, and > 34 years), and birth weight (classified as < 2.5 kg, 2.5–4 kg, and > 4 kg). The dependent variable of exclusive breastfeeding was extracted from the infant feeding flowchart as documented by nurses in the electronic medical record.
Participants were given two surveys to assess how they perceived the value of having attended the intervention. These surveys were non-validated and were comprised of 5-point Likert scale questions (ranging from strongly agree to strongly disagree), as well as open-ended questions. Variables assessed by the Likert scale included how likely participants were to recommend the intervention, whether the intervention strengthened their intent to exclusively breastfeed, their perception of how well the intervention promoted accurate breastfeeding expectations, and whether the intervention improved their supporter’s confidence (Table 5). Open-ended response questions consisted of participant perceptions of their most valued aspects of the intervention (Figure 2). Study team members (authors J.G. and L.W.) independently evaluated the free-text responses and coded them according to common themes. The evaluators then compared their findings to reach concurrence for the final reported result.
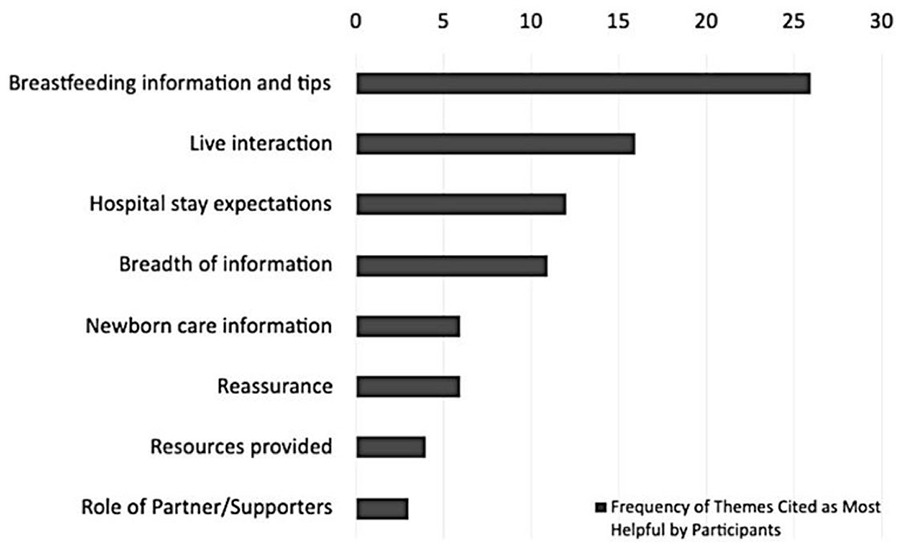
Most Valuable Aspects of the Intervention by Participant Survey.
Data Collection
Between August 2020 and June 2022, the intervention was applied, and the patient variables and feeding method data following discharge from birth hospitalization were extracted by the data analyst from the electronic medical record (EMR). Survey data were collected via a voluntary, online anonymous questionnaire immediately post-intervention (by an electronic survey link placed in the chat and QR code on the final presentation slide at the end of the class) and again by e-mail after hospital discharge. Data were stored separately from patient medical records securely on a password-protected system.
Data Analysis
Descriptive statistics (counts and percentage of total) were computed for demographic variables for the intervention and non-intervention patients. Logistic regression models were conducted using SAS® Enterprise Guide® software (Version 8.2; SAS Institute Inc., Cary, NC, USA). The first model assessed the association between feeding method and independent variables regardless of delivery mode. The second and third models assessed the same association retaining all variables from the first model, except the delivery method, while limiting the model to include only vaginal (second) and Cesarean (third) modes of delivery.
Parity was not in any of the models, given the small sample of multiparous women in the intervention compared with the non-intervention group. The model goodness of fit was determined using Deviance and Pearson chi-square. A p value of 0.05 was considered significant. For the participant-reported surveys, descriptive analysis, such as the percentage of the total, was evaluated to identify the effects of the intervention on breastfeeding success predictors.
Results
Characteristics of the Sample
Patient characteristics, including birth weight, maternal age, and delivery method, showed similar distributions as presented in Table 2. Most babies (n = 143 in each group, 89.4%) had birthweights 2.5–4 kg. Most patients (n = 120 participants, 75%; n = 127 non-participants, 79.4%) delivered vaginally, and approximately 60% (n = 101 participants, 63.1%, n = 98 non-participants, 61.3%) were 25–34 years old.
Demographics and Feeding Method of Participants in the Study by Group (N = 320).
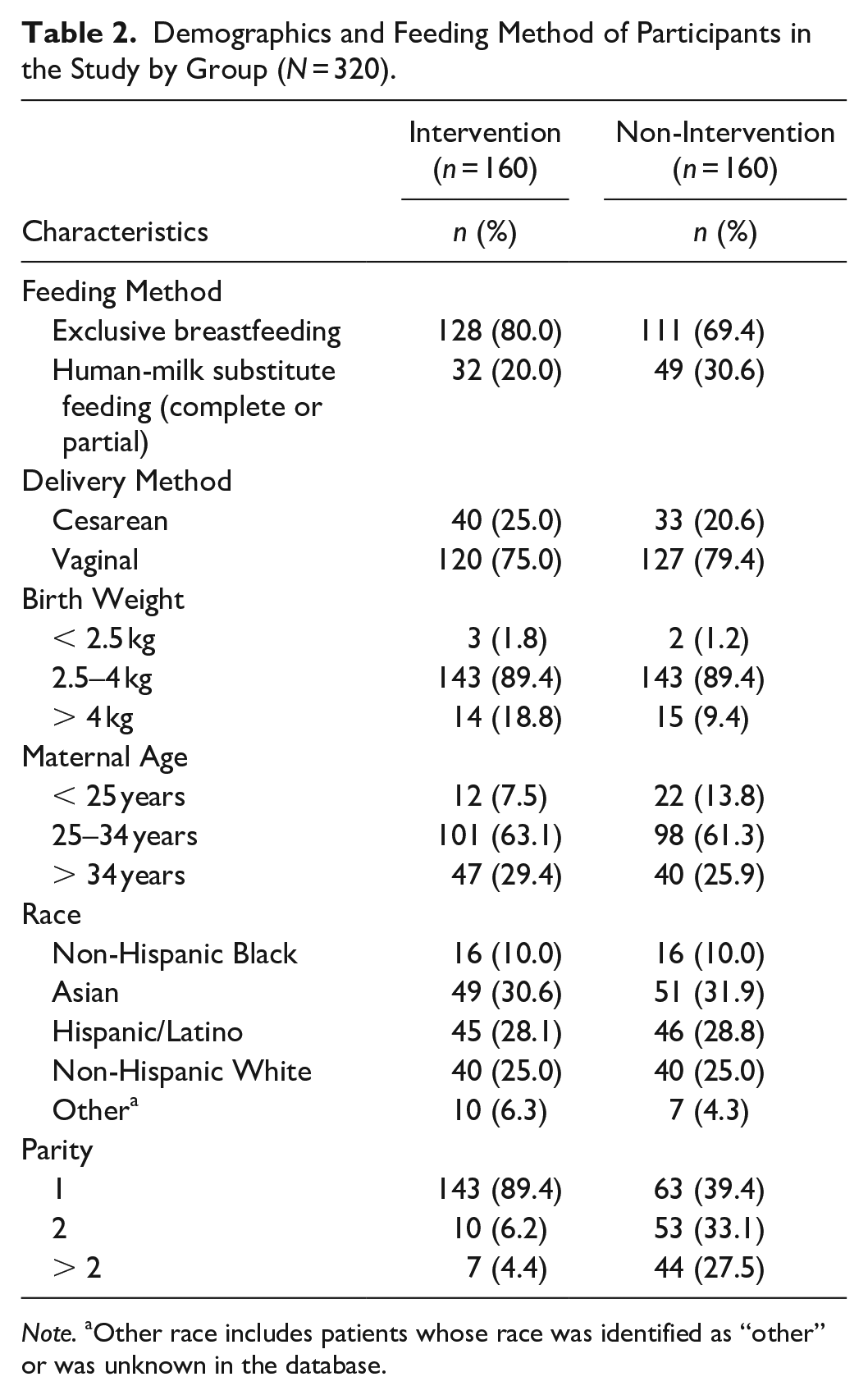
Note. aOther race includes patients whose race was identified as “other” or was unknown in the database.
Exclusive Breastfeeding Among Participants and Non-Participants
Intervention participants were 2.12 times (95% CI [1.12, 3.69]) more likely than non-intervention patients to exclusively breastfeed at hospital discharge, after adjusting for delivery type, maternal age, and birth weight (Table 3).
Characteristics Associated With Exclusive Breastfeeding Among Pregnant Patients (N = 320).
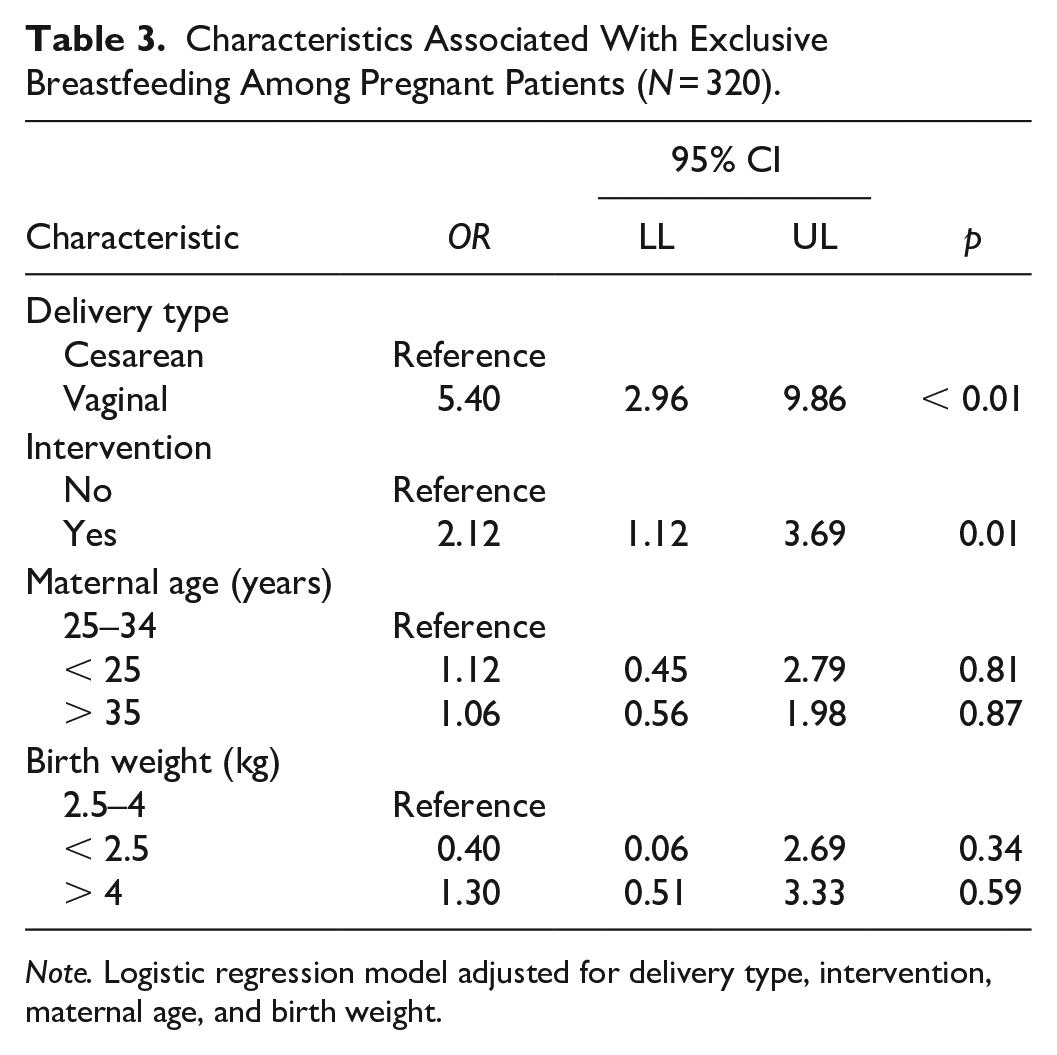
Note. Logistic regression model adjusted for delivery type, intervention, maternal age, and birth weight.
Exclusive Breastfeeding Among Vaginal and Cesarean Delivery
The model for patients delivering vaginally yielded a significant association between exclusive breastfeeding and the intervention. Participants delivering vaginally were 1.93 times (95% CI [1.06, 3.62]) more likely to exclusively breastfeed at hospital discharge than non-intervention patients, adjusting for maternal age and birth weight. However, the model for patients with Cesarean delivery did not reveal a significant association between breastfeeding and the intervention (Table 4).
Characteristics Associated With Exclusive Breastfeeding Among Patients Delivering Vaginally and Cesarean Section.
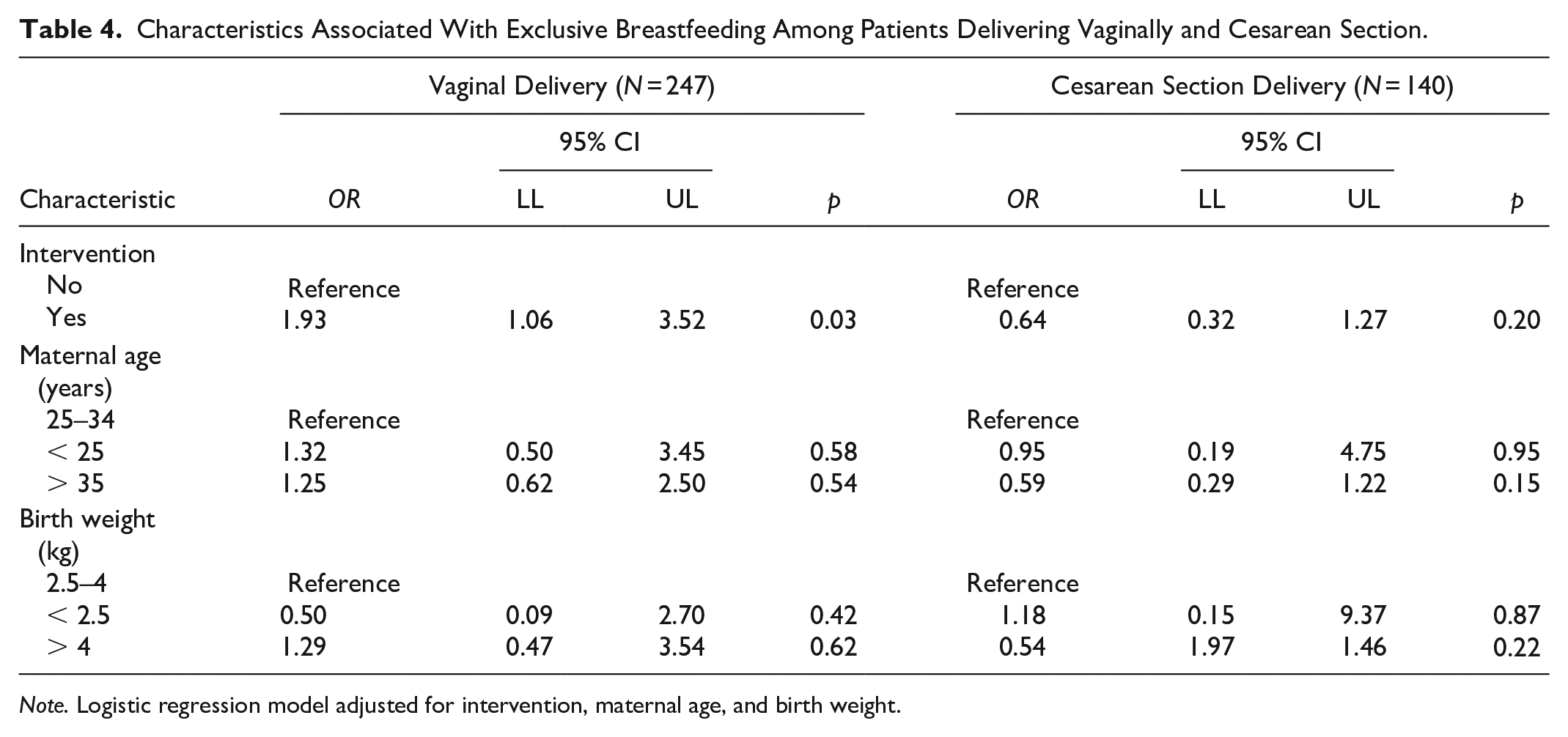
Note. Logistic regression model adjusted for intervention, maternal age, and birth weight.
Participant Reports Regarding the Intervention
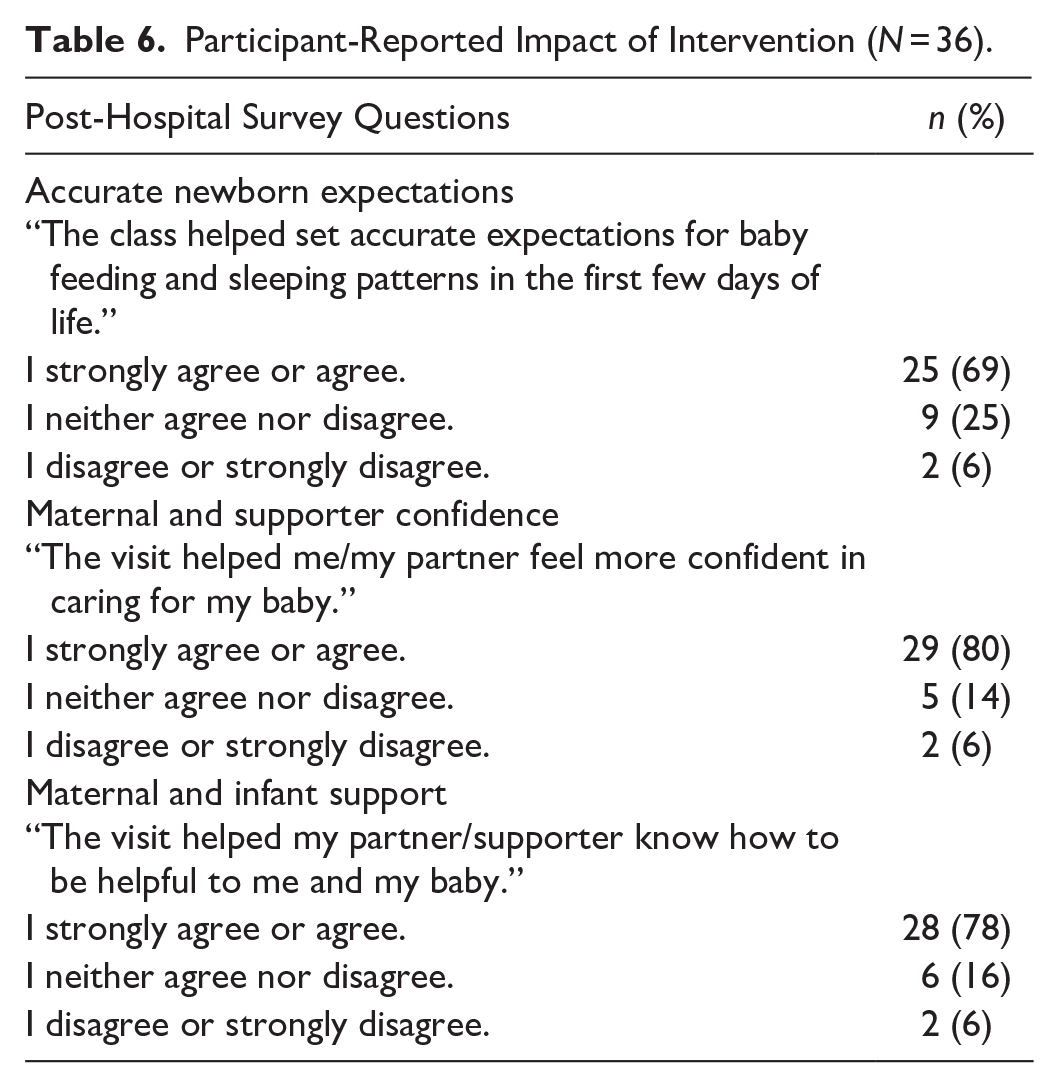
On the immediate-post-intervention survey, 89% (n = 104) of respondents reported that they were very likely or likely to recommend the program to others. Likewise, immediately after the intervention 51% (n = 60) of survey respondents reported increased strength of exclusive breastfeeding intent compared with their strength of intent before the visit (Table 5). On the post-hospitalization survey, the majority of responding participants reported the intervention set accurate expectations, improved maternal and supporter confidence, and improved maternal and infant support (Table 6).
Participant-Reported Impact of Intervention (N = 117).
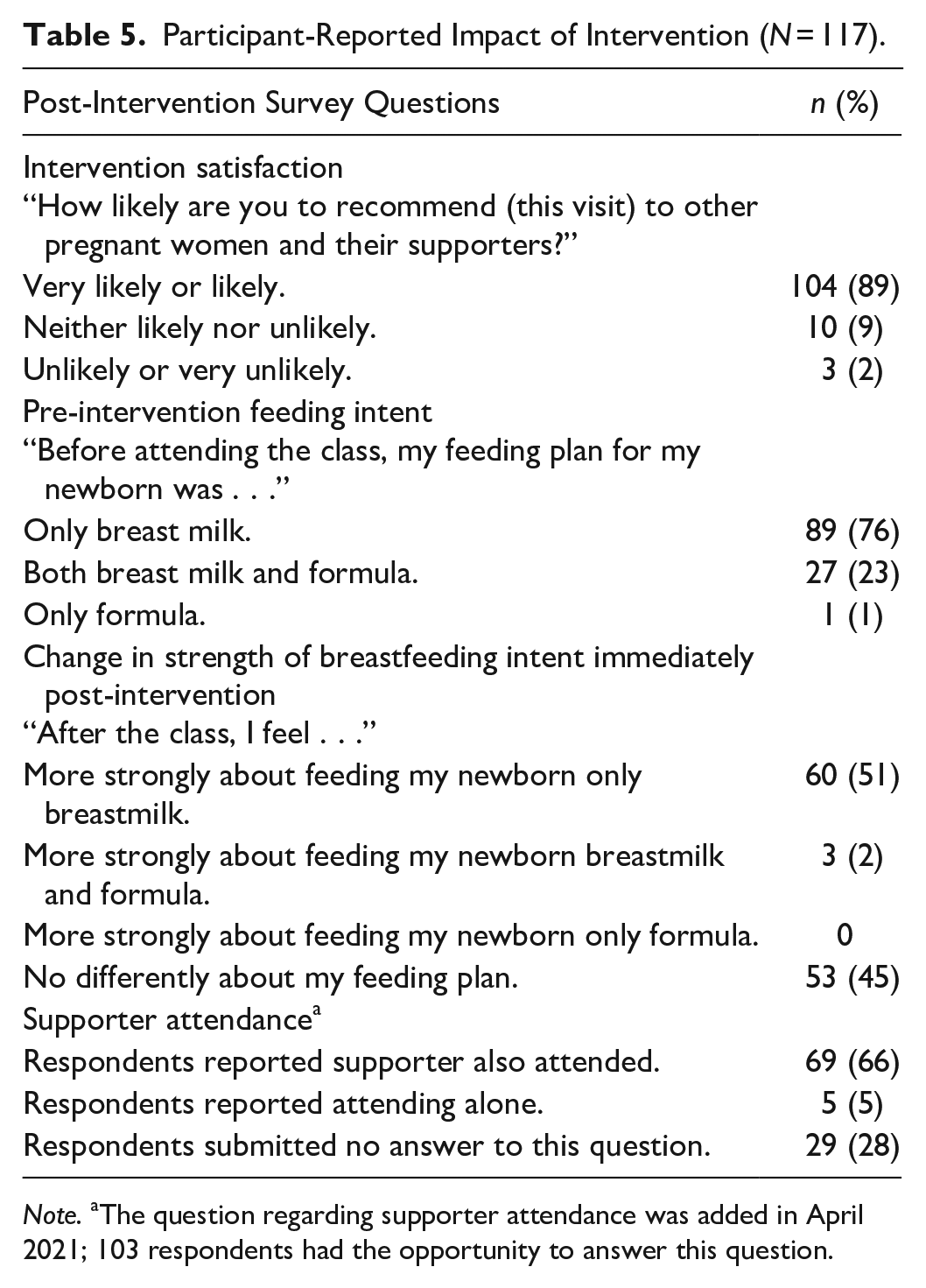
Note. aThe question regarding supporter attendance was added in April 2021; 103 respondents had the opportunity to answer this question.
Participant-Reported Impact of Intervention (N = 36).
Discussion
Although inviting healthcare professionals into the home is a centuries-old practice that has waned in recent decades (Kao et al., 2008), inviting providers into the home through online video has surged since the COVID-19 pandemic (Mann et al., 2020). This may be an enduring invitation, as online healthcare and health education has been shown to be cost-efficient (de la Torre-Díez et al., 2015), convenient for both patients and healthcare providers (Powell et al., 2017), and an effective way to improve health outcomes (Kichloo et al., 2020).
Given this shift in the method of health education delivery, our findings are important because they add to limited knowledge regarding how live prenatal education via online video can positively affect important public health outcomes. Our interactive, web-based intervention was associated with participants being twice as likely to exclusively breastfeed at hospital discharge compared with non-participants, and participants reported positive effects on known predictors for breastfeeding success.
Our study informs which qualities can make a web-based intervention successful. The prenatal education model it examines was well-received and was created to be feasible and reproducible. In our institution, the same two pediatricians and one IBCLC who initiated the intervention in 2020 continue to facilitate the monthly class, and four additional medical centers in our health system launched this intervention in 2022 and continue to sustain it. Data at subsequent sites is not yet available. In the larger body of literature, Palmquist et al. published the specifics of a similarly designed but student-facilitated live, online prenatal educational intervention in 2020; however, to our knowledge, associated outcomes have not been published (Palmquist et al., 2020).
While increased odds of exclusive breastfeeding for participants held under multivariable analysis for patients delivering vaginally, those delivering by Cesarean delivery demonstrated no association between the intervention and increased exclusive breastfeeding. While our small Cesarean delivery sample size may limit the accuracy of this result, we propose that two factors might explain the lack of increased breastfeeding in this group. First, the effect of our intervention may be less than the strength of the association between Cesarean delivery and early human-milk substitute feeding (Li et al., 2021; Prior et al., 2012). It is also possible that the breastfeeding predictors our intervention targets (breastfeeding intent, self-efficacy, and support) are less likely to influence the many contributors to early human milk substitute supplementation associated with Cesarean delivery, such as delayed lactogenesis and increased maternal and newborn comorbidity (Andrikopoulou et al., 2021; Macharey et al., 2020).
The intervention curriculum is built on evidence-based breastfeeding predictors, and participant survey responses suggest that the intervention supports those predictors, which contributes to the reproducibility of the intervention. Perhaps the most influential breastfeeding predictor participants reported as improved by this intervention is the strength of maternal breastfeeding intent (Colaizy et al., 2012; Ross-Cowdery et al., 2017). The U.S. CDC’s Pregnancy Risk Assessment Monitoring System (PRAMS) data, reporting on 16,000 mothers from 2000 to 2003, showed that women with definite intention were more likely to initiate breastfeeding (OR = 24.3, 95% CI [18.4, 32.1]) and to breastfeed for ≥ 4 weeks (OR = 7.12, 95% CI [5.95, 8.51]) compared with women of tentative intention (Colaizy et al., 2012). About half of our respondents reported that the intervention strengthened their intent to exclusively breastfeed. This result includes nine participants who reported intent to combination feed prior to the visit but in the immediate post-visit conversion of intent had changed their goals to exclusive breastfeeding, suggesting the intervention’s positive impact on breastfeeding intent. Moreover, more than half of the participants entering the intervention with an exclusive breastfeeding intent reported an increased strength of intent immediately after the visit, again suggesting the possibility that it positively affected breastfeeding intent for those participants.
Some participants also reported favorably on the intervention’s impact on their social support. More than two-thirds of respondents reported bringing a supporter to the class. Furthermore, most of those who completed the survey reported the intervention improved confidence for them and/or their supporter and added to supporter knowledge on how to be helpful to mother and baby. Wang et al. (2018) showed the positive effects of supporters, particularly fathers, on breastfeeding success using the data from Infant Feeding Practices Study II, a U.S. CDC-funded investigation of infant feeding and care practices through the first year of life. In the study, participants who perceived that the father preferred exclusive breastfeeding were more likely to initiate breastfeeding (adjusted odds ratio (aOR) = 1.9; 95% CI [1.0, 3.7]), and less likely to stop breastfeeding at any time (exclusive breastfeeding: adjusted hazard ratio (aHR) = 0.8; 95% CI [0.6, 0.9]); any breastfeeding: aHR = 0.6; (95% CI [0.5, 0.7]).
Considering the Healthy People 2030’s goal of increasing the use of telehealth to improve access to health services (U.S. Department of Health and Human Services, 2020), our descriptive data could be considered in the design of online resources, as they suggest intervention aspects that survey respondents found were important. First, survey respondents appreciated the breadth of the curriculum. The design and promotion of this intervention with a comprehensive curriculum was intentional and aimed to attract participants of all feeding intentions rather than only those with intent to breastfeed. Second, respondents commented on the value of pediatricians and an IBCLC as co-facilitators. Pediatrician recommendations to breastfeed may have been integral to the intervention’s impact, considering the influence physician recommendations can have on patient decisions (Gurmankin et al., 2002; Lawrence, 1982). Third, the live interactive format (also employed by Palmquist et al., 2020) providing opportunity for engagement was also favored by respondents. The chat feature was prominently used, which may have provided participants with the anonymity and comfort needed to be candid. Given that adult learning models suggest that an interactive format with content responsive to participant interests contributes to effective learning (Kennedy & Parish, 2021; Knowles, 1990), our employment of this format may have contributed to our positive results. Although more research is needed to confirm this, online prenatal educational models without live interaction may be less likely to be successful than a live, interactive model (Abuidhail et al., 2019; Sari & Altay, 2020).
Notably, many key demographics were similar between patients who received the intervention and our sample of patients who did not. This suggests that any benefits associated with intervention participation are not attributable to those demographic characteristics. While previous studies have documented an increased use of telehealth (especially involving video) among non-Hispanic White participants compared with Hispanic and Non-Hispanic Black participants in the United States (White-Williams et al., 2023), our results showed no racial differences between participants and non-participants in this online intervention. Given that racial disparities in breastfeeding and breastfeeding-related support are well-documented in the United States (Boone et al., 2019; Jones et al., 2015), the equality of online participation in this study may be of interest.
Limitations
Our retrospective quasi-experimental design confers the primary limitation that patients with a stronger exclusive breastfeeding intent may have been more likely to self-select for the intervention. To mitigate this potential bias, our enrollment strategy aimed to attract expectant parents with varied breastfeeding intent. Despite this attempt, 76% of our respondents reported a pre-intervention intent to exclusively breastfeed, whereas unpublished data from 2019 suggest only 60% of our medical center’s prenatal patient population intends to exclusively breastfeed.
Our findings have additional limitations. First, while our intervention and comparison patients were similar in many characteristics known to influence breastfeeding success, future analysis defining socioeconomic status and maternal/partner education levels would be valuable (Boone et al., 2019; Jones et al., 2015). Second, parity, which is known to be associated with exclusive breastfeeding, was not adjusted for in the multiple regression model given the small sample of multiparous women in the intervention compared with the non-intervention group. Third, for evaluating the participant-reported effect of the intervention on known breastfeeding promoters, pre-post intervention comparison questionnaires using validated scales—such as the Infant Feeding Intensions Scale (Nommsen-Rivers et al., 2010)—would improve the reliability of these findings. Lastly, our post-intervention questionnaire response rate was lower than desired (35%) and both response bias and loss to follow-up bias are possible. However, the demonstration of favorable remarks on all targeted breastfeeding predictors is encouraging.
Conclusions
Participants of our live, online prenatal educational intervention were twice as likely to exclusively breastfeed through hospital discharge as patients who did not attend the intervention. One exception may be in patients undergoing Cesarean delivery; however, our small sample size may have limited the accuracy of these results. Participants reported that the intervention supports evidence-based predictors of breastfeeding success. Our findings add to limited evidence of the potential efficacy of live, online prenatal education. A prospective, randomized examination of the intervention’s association with breastfeeding duration would further define its potential impact.
Supplemental Material
sj-pdf-1-jhl-10.1177_08903344241297607 – Supplemental material for A Live Online Prenatal Educational Model: Association With Exclusive Breastfeeding at Discharge
Supplemental material, sj-pdf-1-jhl-10.1177_08903344241297607 for A Live Online Prenatal Educational Model: Association With Exclusive Breastfeeding at Discharge by Julia M. Gabhart, Lina N. Wasio, Panupong U-thaiwat, Yi W. Chen and James Main in Journal of Human Lactation
Footnotes
Acknowledgements
Thank you to physician leadership at Kaiser South Sacramento Medical Center, including Dr. Jasmine Nguyen, Chief of Pediatric Hospital Medicine, Dr. Sean Cooke, Chief of Pediatrics, and Dr. Rachel Dong, Chief of Obstetrics and Gynecology at Kaiser South Sacramento Medical Center who supported the vision and funding for this novel project. Thank you to Gerrit Mulholland, IBCLC, who also facilitated the class, and Mary Wagner Davis, IBCLC, who mentored the initial curriculum design.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by Obstetrics, Pediatrics, and Health Education Departments of Kaiser Permanente South Sacramento Medical Center.
Supplemental Material
Supplemental Material may be found in the “Supplemental Material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.