
Abstract
Background:
Postnatal breastfeeding rates are low, so breastfeeding education is necessary and should be initiated prenatally. Standard breastfeeding education methods have shown limited effectiveness. Therefore, there is a need for innovative, memorable, and engaging breastfeeding education approaches during the prenatal period.
Research Aims:
This study aimed to evaluate the effect of antenatal breastfeeding education delivered through the Pecha Kucha method on postpartum breastfeeding self-efficacy, infant feeding attitude, and breastfeeding satisfaction.
Method:
This randomized controlled study was conducted with 70 pregnant women—35 in an experimental group and 35 in a control group—at the gynecology and obstetrics clinic of a hospital. The data were collected using the Descriptive Information Form, Antenatal Breastfeeding Self-Efficacy Scale, Postpartum Breastfeeding Self-Efficacy Scale (PBSS), Infant Feeding Attitude Scale (IFAS) and the Visual Analog Scale-Satisfaction (VAS-S).
Results:
In the study, in the control group, IFAS scores significantly decreased between baseline and both the 2nd and 4th week assessments, whereas in the experimental group, scores significantly increased (p < 0.001). PBSS scores significantly increased in the experimental group (z = -3.519, p < 0.001). The mean VAS-S scores increased in the experimental group (p = 0.001), while they decreased in the control group (p = 0.005).
Conclusion:
Breastfeeding education delivered via the Pecha Kucha method increased postpartum breastfeeding self-efficacy, positively influenced infant feeding attitudes, and enhanced breastfeeding satisfaction, suggesting it may be a promising and innovative approach for antenatal breastfeeding education.
Background
Breastfeeding provides all the essential nutrients required for an infant’s growth and development. At the same time, it is also beneficial for the infant’s psychological and emotional development (Dodou et al., 2021). Therefore, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) recommend that mothers initiate breastfeeding as soon as possible after birth, exclusively breastfeed their infants for the first 6 months, and continue breastfeeding until the age of 2 (WHO, 2020). However, only an estimated 48% of infants under 6 months of age worldwide are exclusively breastfed (UNICEF, 2025). Breastfeeding rates are influenced by various factors, including insufficient mother’s milk, fatigue, difficulties in latching the baby to the breast, premature births, misinformation about breastfeeding, and self-efficacy (Kocabey & Karakoç, 2022; Mostafa Farag et al., 2020).
Breastfeeding self-efficacy reflects a mother’s ability to breastfeed her baby and her perceptions of breastfeeding. The mother’s ability to breastfeed correctly, concerns about milk insufficiency, and breastfeeding anxieties may affect breastfeeding self-efficacy (Aktürk & Kolcu, 2023; Dennis, 1999). Studies have shown that antenatal breastfeeding education increases the perception of breastfeeding self-efficacy (Araban et al., 2018; Shafaei et al., 2020). A systematic review found that mothers who received antenatal breastfeeding education started breastfeeding earlier and had more positive breastfeeding knowledge, self-efficacy, and breastfeeding attitudes (Kehinde et al., 2023). At the same time, the increase in breastfeeding attitudes positively affect breastfeeding satisfaction. Breastfeeding satisfaction is defined as an outcome experienced by women through meeting their breastfeeding goals, expectations, and needs (Leff et al., 1994). Breastfeeding education is reported to increase breastfeeding satisfaction. (Awaliyah et al., 2019; Ericson et al., 2021). Breastfeeding education, while influencing breastfeeding self-efficacy and breastfeeding satisfaction, also affects mothers’ infant feeding attitudes (Khasawneh et al., 2020). Women who receive breastfeeding education have more positive infant feeding attitudes compared to those who do not (Abdulahi et al., 2021; Tseng et al., 2020).
Pecha Kucha is derived from a Japanese term that means "conversation" (Bakır et al., 2022). It is a presentation format consisting of 20 slides, each shown for 20 seconds, commonly used in education. The presentation lasts 6 minutes and 40 seconds, and most of the slides consist only of images. In Pecha Kucha presentations, slides typically feature visuals, images, graphics, and very few words (Liao et al., 2020; White & Louis, 2023). There are various educational methods available to initiate and sustain breastfeeding (Badaczewski et al., 2017; Maleki-Saghooni et al., 2020).
The Pecha Kucha method is an effective teaching strategy that utilizes visual and auditory elements to deliver concise information. It has been shown to enhance learners’ attention, comprehension, and long-term retention, particularly in educational and health-related settings (Bakır et al., 2022; Gün Kakaşçı & Durmaz, 2022). Using the Pecha Kucha method in breastfeeding education helps present information in a clear and memorable way. Although this technique has been applied in various fields, its effect on antenatal breastfeeding education, specifically regarding postpartum breastfeeding self-efficacy, infant feeding attitudes, and breastfeeding satisfaction, has not yet been studied. Therefore, this research aims to fill this gap by evaluating the effect of antenatal breastfeeding education delivered through the Pecha Kucha method on postpartum breastfeeding self-efficacy, infant feeding attitudes, and breastfeeding satisfaction, thereby contributing to the literature and guiding future studies. We hypothesized that antenatal breastfeeding education delivered through the Pecha Kucha method would positively influence postpartum breastfeeding self-efficacy, infant feeding attitudes, and breastfeeding satisfaction
Key Messages
• Postpartum breastfeeding rates are low, and various breastfeeding education methods are applied to increase these rates.
• The Pecha Kucha method is easy to understand, memorable, visual, and auditory, making it an effective strategy for breastfeeding education.
• This method has been found to increase breastfeeding self-efficacy, infant feeding attitudes, and breastfeeding satisfaction.
• Pecha Kucha is a practical, concise, and understandable method that can be easily implemented in breastfeeding education.
Methods
Research Design
This study was a two-arm, randomized controlled trial (RCT) and was designed to examine the effect of antenatal breastfeeding education delivered through the Pecha Kucha method on postpartum breastfeeding self-efficacy, infant feeding attitudes, and breastfeeding satisfaction. The RCT design is well-suited for educational interventions as it provides robust evidence by randomly assigning participants to intervention and control groups, thereby reducing potential confounding factors. Ethical approval for the study was obtained from the Scientific Research Ethics Committee of a university (Decision No. 2024-1, July 11, 2024), and permission was granted by the institution where the study was conducted. The trial was registered with ClinicalTrials.gov (Identifier: NCT06528782).
Setting and Relevant Context
This study was conducted at the Non-Stress Test (NST) unit of the Obstetrics and Gynecology Department at Etlik City Hospital, located in Ankara, the capital city of Turkey. Ankara is a large metropolitan area with a diverse population from various socioeconomic and educational backgrounds. This unit is regularly visited by women in the antenatal period for routine prenatal monitoring and fetal well-being assessments, and serves mainly urban pregnant women.
Standardized breastfeeding education and support are routinely offered in this unit by trained healthcare professionals, including midwives, nurses, and lactation support providers, through antenatal sessions and postnatal follow-up programs. However, many women have limited access to breastfeeding support outside the hospital, which may negatively affect breastfeeding practices. It is widely recommended that the most effective breastfeeding education programs aiming to increase exclusive breastfeeding rates during the first 6 months should begin during the antenatal period and continue into the postpartum period (Şensoy & Koçak, 2021).
Breastfeeding rates in Turkey remain below global targets. According to the 2018 Turkey Demographic and Health Survey, 71% of infants are breastfed within the first hour of birth, while only 41% are exclusively breastfed for 6 months (Hacettepe University Institute of Population Studies, 2019). Globally, UNICEF (2020) reports similar figures, with 43% early initiation and 41% exclusive breastfeeding rates. These data highlight the ongoing need for effective breastfeeding promotion. Given this context, innovative and engaging antenatal education methods, including the Pecha Kucha technique, may help improve breastfeeding knowledge and practices in this population.
Sample
The study population consisted of pregnant women attending routine prenatal monitoring at the NST unit of Etlik City Hospital in Ankara, Turkey. Pregnant women who met the inclusion criteria were approached in person by the researcher and provided with verbal and written information about the study during their NST appointment. Those who voluntarily agreed to participate and provided written informed consent were included. Inclusion criteria were: being at least 18 years old, speaking and understanding Turkish, having completed at least primary education, having a gestational age of ≥ 38 weeks (this was chosen to allow immediate implementation and follow-up of breastfeeding education after birth), having no chronic illness (defined as any long-term medical condition, e.g., diabetes, hypertension, cardiovascular disease, recorded in the patient’s medical history), and having no communication barriers. Exclusion criteria were applied prior to randomization and included participants with medical indications preventing breastfeeding, multiple pregnancies, mental illness, those unwilling to continue participation, those who did not give birth within 2 weeks after the education session, those whose infants were admitted to the neonatal intensive care unit (NICU) after birth, and pregnant women who could not be reached by phone during the follow-up period.
The sample size calculation was performed using G*Power 3.1.9.4 software. The primary outcome was the Postpartum Breastfeeding Self-Efficacy Scale (PBSS). Based on Tseng et al. (2020), an effect size of 0.91 (Cohen’s d), a two-tailed independent samples t test, a Type I error rate (α) of 0.05, and a power (1–β) of 0.95 were specified. Under these parameters, the required total sample size was 64 participants (32 per group). Since this was an intervention study, a 10% dropout rate was considered, and the target sample size was increased to 70 participants (35 per group). Out of 145 women assessed for eligibility, 50 did not meet the inclusion criteria and 20 declined participation. Participants were recruited consecutively from eligible pregnant women attending the gynecology and obstetrics clinic. A total of 75 women were randomized into two groups: the Pecha Kucha intervention group (n = 37) and the control group (n = 38). During follow-up, two participants from the intervention group were excluded (one due to NICU admission of the baby and one due to being unreachable by phone) and three from the control group (two unreachable by phone, one who did not give birth within 2 weeks). Consequently, the study was completed with 70 participants, with 35 in each group (Figure 1).
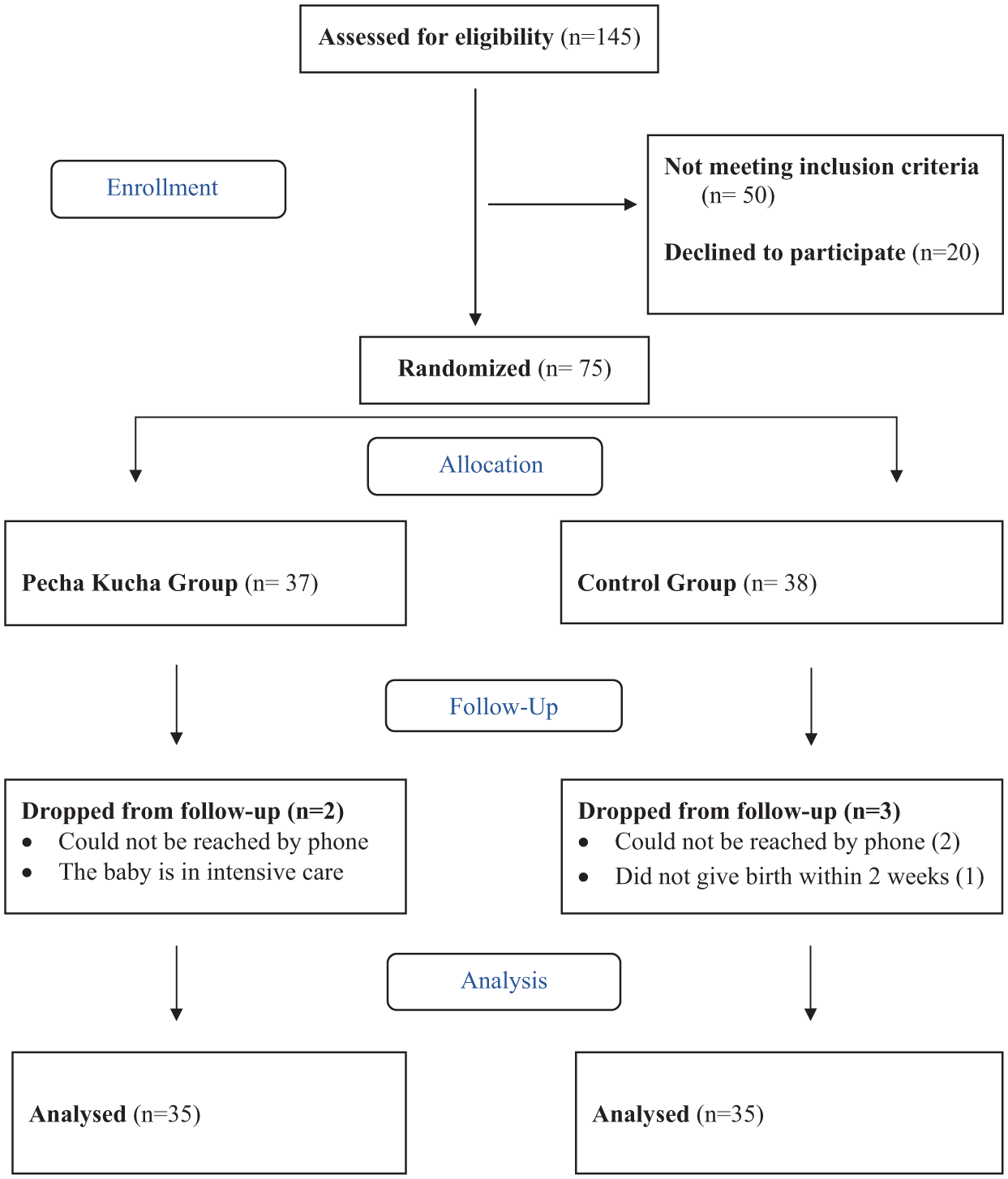
Consort flow diagram.
The Intervention
Experimental (Pecha Kucha) group
Eligible pregnant women assigned to the experimental group provided written and verbal informed consent. At the initial encounter, participants completed the Descriptive Information Form, Antenatal Breastfeeding Self-Efficacy Scale-Short Form (ABSS), and Infant Feeding Attitude Scale (IFAS) prior to the educational session. Breastfeeding education was personally delivered by the researcher to each participant using the Pecha Kucha method, following a standardized script to ensure consistent presentation. The session consisted of a 20-slide PowerPoint presentation, with each slide displayed for 20 seconds, totaling 6 minutes and 40 seconds. Slides were predominantly visual with minimal text, designed to convey clear, focused messages. Content addressed both informational and practical aspects of breastfeeding: the importance and benefits of human milk, its composition, positive effects on mother and infant, initiation of breastfeeding, correct positioning and latching, breastfeeding positions, and expression and storage of mother’s milk. The session was conducted face-to-face in the NST unit. This education aimed to support both awareness and practical knowledge about breastfeeding. Follow-up assessments were conducted at 2 and 4 weeks post-intervention. Two weeks after the session, participants completed the Postpartum Breastfeeding Self-Efficacy Scale-Short Form (PBSS), IFAS, and the Visual Analog Scale Satisfaction (VAS-S) via telephone. At 4 weeks, the same measures were repeated. Participant engagement and retention were supported through regular telephone reminders throughout the follow-up period.
Control group
Eligible pregnant women assigned to the control group provided written and verbal informed consent. At the initial encounter, participants completed the Descriptive Information Form, ABSS, and IFAS. Participants in the control group received only the hospital’s routine antenatal breastfeeding education as part of standard prenatal care, with no additional intervention from the researcher. Follow-up assessments were conducted at 2 and 4 weeks, identical to the experimental group, using the PBSS, IFAS, and VAS-S. Retention and engagement were similarly supported through regular telephone reminders during the follow-up period.
Measurement
The research data were collected using the Descriptive Information Form, Antenatal Breastfeeding Self-Efficacy Scale (ABSS), Postpartum Breastfeeding Self-Efficacy Scale (PBSS), Infant Feeding Attitude Scale (IFAS), and Visual Analog Scale - Satisfaction (VAS-S).
Descriptive information form
The descriptive information form includes three sections and 18 questions, covering sociodemographic characteristics, obstetric history and breastfeeding-related topics. The Descriptive Information Form was developed based on the literature (Dodou et al., 2021; Savaş et al., 2024; Tseng et al., 2020).
Breastfeeding Self-Efficacy Scale–Short Form (BSS-SF)
Breastfeeding Self-Efficacy Scale-Short Form (BSS-SF) developed by Dennis and Faux, consists of 14 items. The Turkish validity and reliability study was conducted by Aluş Tokat et al. in 2010. The scale can be used in both antenatal and postpartum periods to assess women’s confidence in their breastfeeding abilities. It uses a 5-point Likert scale: 1 = Not at all confident, 2 = Not confident, 3 = Sometimes confident, 4 = Confident (4), and 5 = Very confident. The total score ranges from 14 to 70, with lower scores indicating lower breastfeeding self-efficacy. In the original scale, the Cronbach’s alpha for the antenatal form is 0.87, and for the postpartum form, it is 0.86 (Aluş Tokat et al., 2010). In this study, the Cronbach’s alpha of the scale was found to be 0.90 in the antenatal form and 0.94 in the postpartum form in the 2nd week, and 0.97 in the 4th week.
Infant Feeding Attitude Scale (IFAS)
Infant Feeding Attitude Scale developed by De La Mora and Russell, women’s attitudes toward breastfeeding, infant feeding choices, and breastfeeding duration. The Turkish validity and reliability study was conducted by Ekşioğlu et al. in 2016. The scale consists of 17 items in a 5-point Likert type ranging from 1 (strongly disagree) to 5 (strongly agree). Nine items affirm breastfeeding, and eight include positive statements about formula feeding. Higher total scores indicate more positive attitudes toward breastfeeding, whereas lower scores indicate more positive attitudes toward formula feeding. The scale’s total score range from 17 to 85. The original scale’s Cronbach’s alpha is 0.71 (Ekşioğlu et al., 2016). In this study, the Cronbach’s alpha value of the scale was found to be 0.76 in the first encounter, 0.86 in the second week, and 0.92 in the fourth week.
Visual Analog Scale–Satisfaction (VAS-S)
Visual Analog Scale–Satisfaction is also used to measure other components including satisfaction, in addition to pain. The VAS-S is a single-item visual analog scale (VAS) used to assess satisfaction and does not have formal reliability or validity data, but it has been widely used in clinical and research settings to measure subjective satisfaction (Ericson et al.,2017; Sarı & Güngör Satılmış, 2023). In our study, the VAS-S was also used to evaluate mothers’ breastfeeding satisfaction levels. The VAS-S is a 10 cm ruler with the phrase "Not satisfied" at one end and "Very satisfied" at the other end. The mother is asked to rate her breastfeeding satisfaction from 1 to 10 after the education. The high scores obtained from the scale also indicate high satisfaction.
To minimize selection bias, participants were randomly assigned to the experimental and control groups using the Random.org online randomization tool, ensuring an equal chance of allocation. All eligible pregnant women attending the NST unit during the data collection period were consecutively approached and provided with standardized verbal and written information about the study. Data entry was performed by an individual blinded to group assignments, with codes A and B used during analysis. Group assignments were revealed to the researcher only after completion of data analysis to maintain assessor blinding and reduce potential bias.
Data Collection
The study was conducted at the NST unit of the obstetrics and gynecology department of a hospital from July 11 to September 15, 2024. Pregnant women who volunteered and met the inclusion criteria were informed about the study’s aim and content through one-on-one meetings conducted by the researcher to ensure privacy. Written and verbal informed consent was obtained prior to data collection. Data were collected face-to-face by the same trained researcher during NST appointments. All participant data were coded and securely stored in password-protected files accessible only to the research team to ensure confidentiality
Data Analysis
Data were analyzed using SPSS (Version 25). Descriptive statistics were first calculated for demographic variables, which were presented as frequency (n) and percentage (%). Continuous variables were reported as mean and standard deviation M (SD) for normally distributed data or as median and interquartile range (IQR) for non-normally distributed data. The normality of continuous variables was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests, depending on sample size. For comparisons between two independent groups, the Independent-Samples t test was applied to normally distributed data, and the Mann-Whitney U test was used for non-normally distributed data. For dependent group comparisons, the Wilcoxon signed-rank test was employed for non-normally distributed data, and the Friedman test was used for analyses involving more than two repeated measures, with post-hoc Bonferroni correction applied where appropriate. Spearman correlation analysis was performed for non-normally distributed continuous variables. The significance level was set at p < 0.05 for all comparisons.
Results
Characteristics of the Sample
The demographic characteristics of the pregnant women in both groups are presented in Tables 1 and 2. The educational status of the experimental group was 42.9% (n = 15) school/faculty and 31.4% (n = 11) high school, while 51.4% (n = 18) of the participants in the control group had a high school education. No statistically significant relationship was found between educational status and the groups (p = 0.195). Regarding employment status, 71.4% (n = 25) of participants in the experimental group and 88.6% (n = 31) in the control group were not working. The average length of marriage was 4.94 (3.84) years in the experimental group and 4.94 (4.46) years in the control group, with no significant difference between groups (p = 0.853). Most participants in both groups reported not smoking: 85.7% (n = 30) in the experimental group and 91.4% (n = 32) in the control group. It was determined that none among the participants in either group consumed alcohol. The average gestational age was 39 (1) weeks in both groups. Regarding parity, 54.3% (n = 19) of participants in the experimental group and 45.7% (n = 16) in the control group had been previously pregnant. Most participants had not experienced miscarriage or abortion: 74.3% (n = 26) in the experimental group and 77.1% (n = 27) in the control group. Additionally, 68.6% (n = 24) of participants in the experimental group and 74.3% (n = 26) in the control group reported that their pregnancies were planned and intentional. Overall, 62.9% (n = 44) of participants believed their breastfeeding knowledge was sufficient, and among the 54.3% (n = 38) who received breastfeeding education, 63.4% (n = 24) were educated by a midwife. Finally, 67.1% (n = 47) of participants gave birth vaginally.
Descriptive Characteristics of Pregnant Women (N = 70).
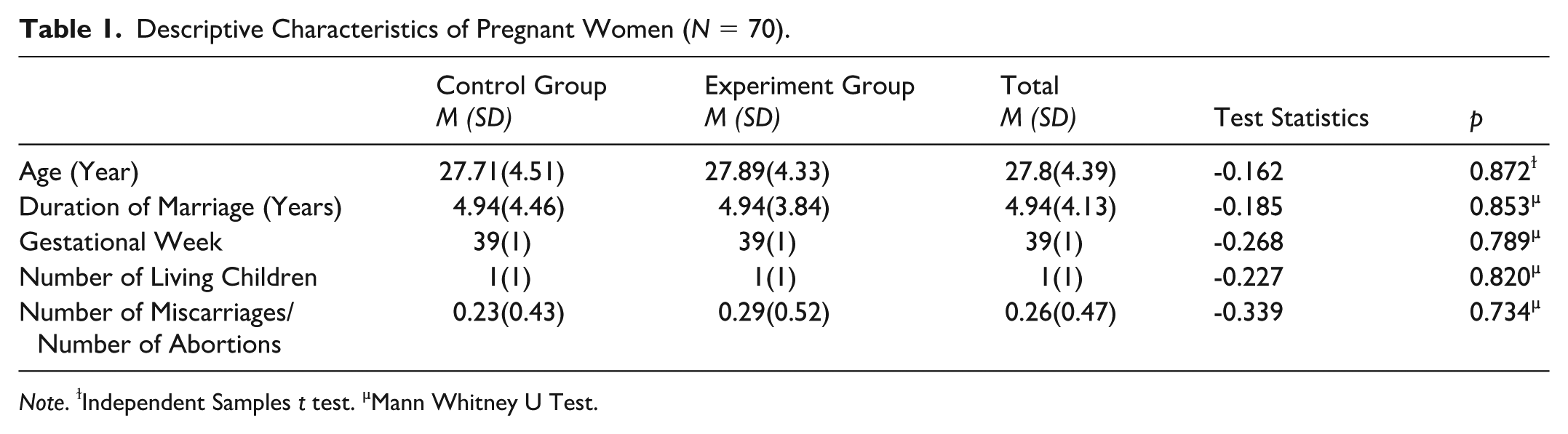
Note. ɫIndependent Samples t test. µMann Whitney U Test.
Descriptive Characteristics of Pregnant Women (N = 70).
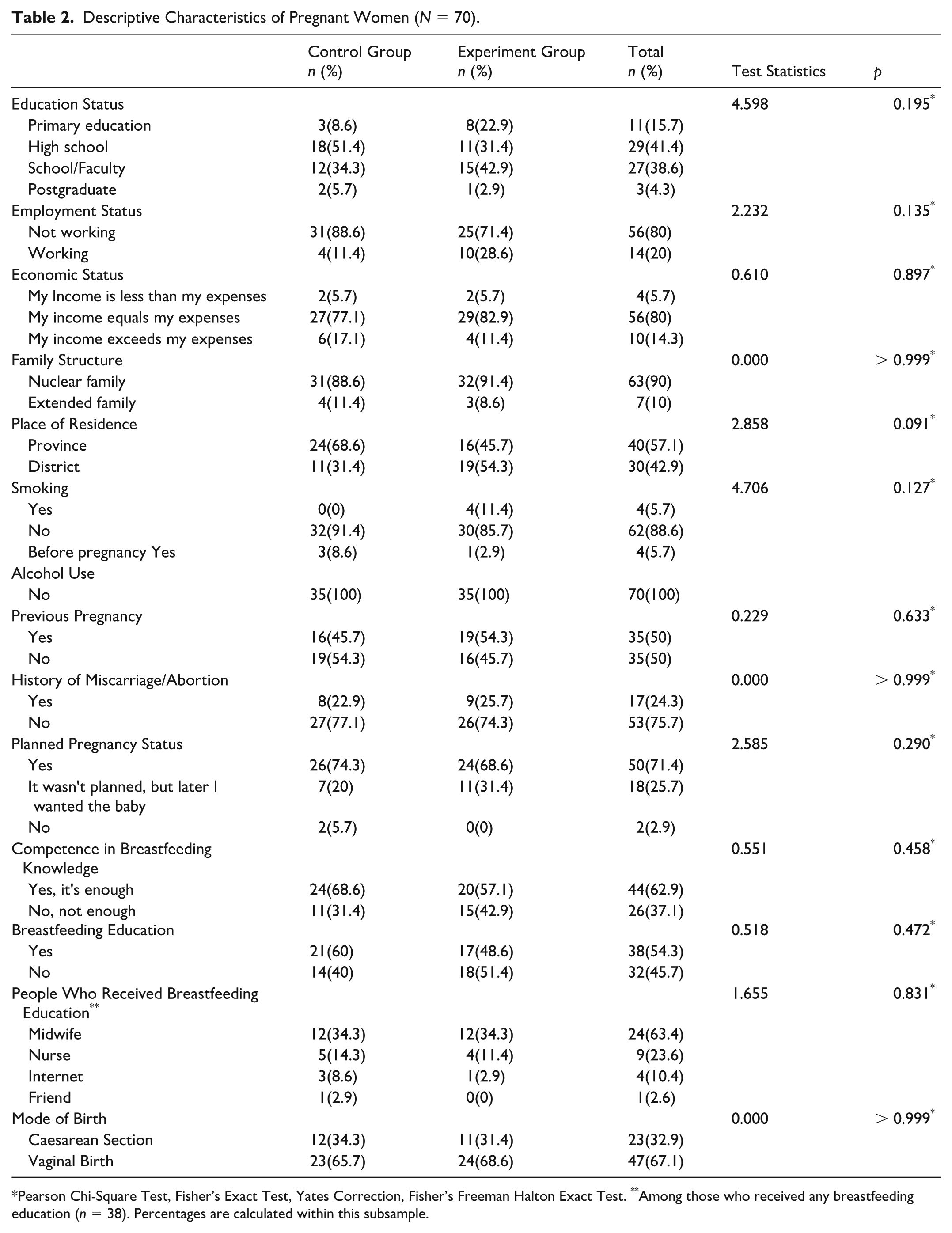
Pearson Chi-Square Test, Fisher’s Exact Test, Yates Correction, Fisher’s Freeman Halton Exact Test. **Among those who received any breastfeeding education (n = 38). Percentages are calculated within this subsample.
According to Spearman correlation analysis (Table 3), VAS-S Week 2 scores showed significant positive correlations with all other variables. These correlations were moderate with ABSS (r = 0.347, p = 0.003) and IFAS (First Encounter; r = 0.454, p < 0.001), and strong with PBSS Week 2 (r = 0.749, p < 0.001), IFAS Week 2 (r = 0.723, p < 0.001), PBSS Week 4 (r = 0.811, p < 0.001), and IFAS Week 4 (r = 0.753, p < 0.001). VAS-S Week 4 scores were also strongly correlated with IFAS Week 2 (r = 0.765, p < 0.001), PBSS Week 4 (r = 0.858, p < 0.001), and IFAS Week 4 (r = 0.880, p < 0.001), while their association with ABSS was not significant (r = 0.187, p = 0.122). IFAS (First Encounter) scores were significantly correlated with all scales, showing moderate associations with PBSS Week 2 (r = 0.545, p < 0.001) and PBSS Week 4 (r = 0.510, p < 0.001). PBSS Week 2 scores demonstrated a strong correlation with PBSS Week 4 (r = 0.917, p < 0.001) and IFAS Week 2 (r = 0.670, p < 0.001). IFAS Week 2 was strongly correlated with IFAS Week 4 (r = 0.925, p < 0.001). Overall, PBSS and IFAS scores across different time points showed consistently strong inter-scale correlations, while ABSS demonstrated weaker and more variable associations.
Correlation Between Scale Scores.
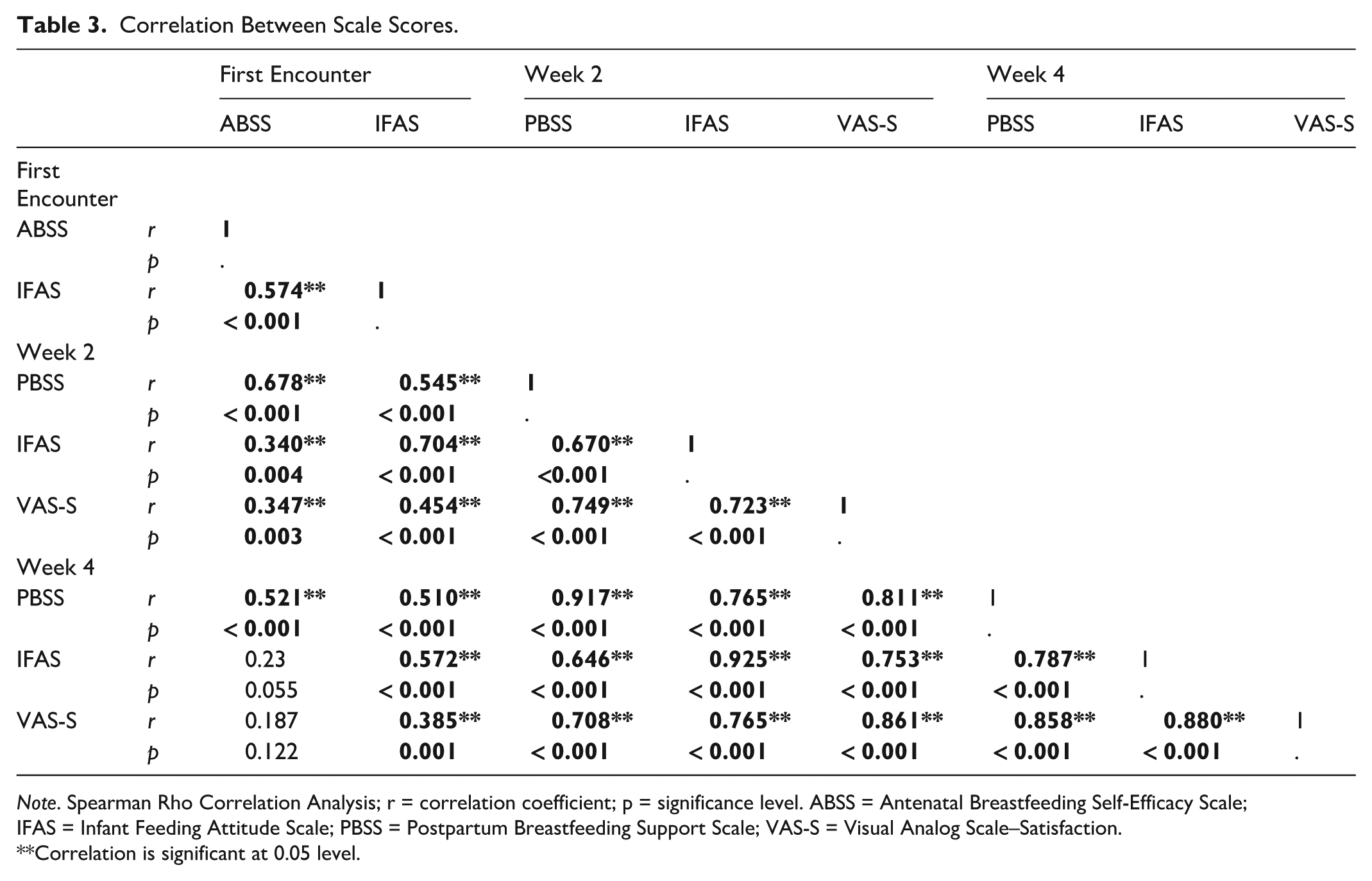
Note. Spearman Rho Correlation Analysis; r = correlation coefficient; p = significance level. ABSS = Antenatal Breastfeeding Self-Efficacy Scale; IFAS = Infant Feeding Attitude Scale; PBSS = Postpartum Breastfeeding Support Scale; VAS-S = Visual Analog Scale–Satisfaction.
Correlation is significant at 0.05 level.
The scales that showed significant differences between the study groups were VAS-S at Week 2 (p = 0.021), VAS-S at Week 4 (p < 0.001), ABSS (p = 0.020), IFAS at Week 2 (p = 0.036), PBSS at Week 4 (p = 0.008), and IFAS at Week 4 (p = 0.001). Among the scales where significant differences were identified, it was determined that the participants in the experimental group had significantly higher scores compared to the participants in the control group on all scales except for the ABSS. In the ABSS, the control group scored higher than the experimental group (Table 4).
Scale Scores by Control and Experimental (Pecha Kucha) Groups (N = 70).
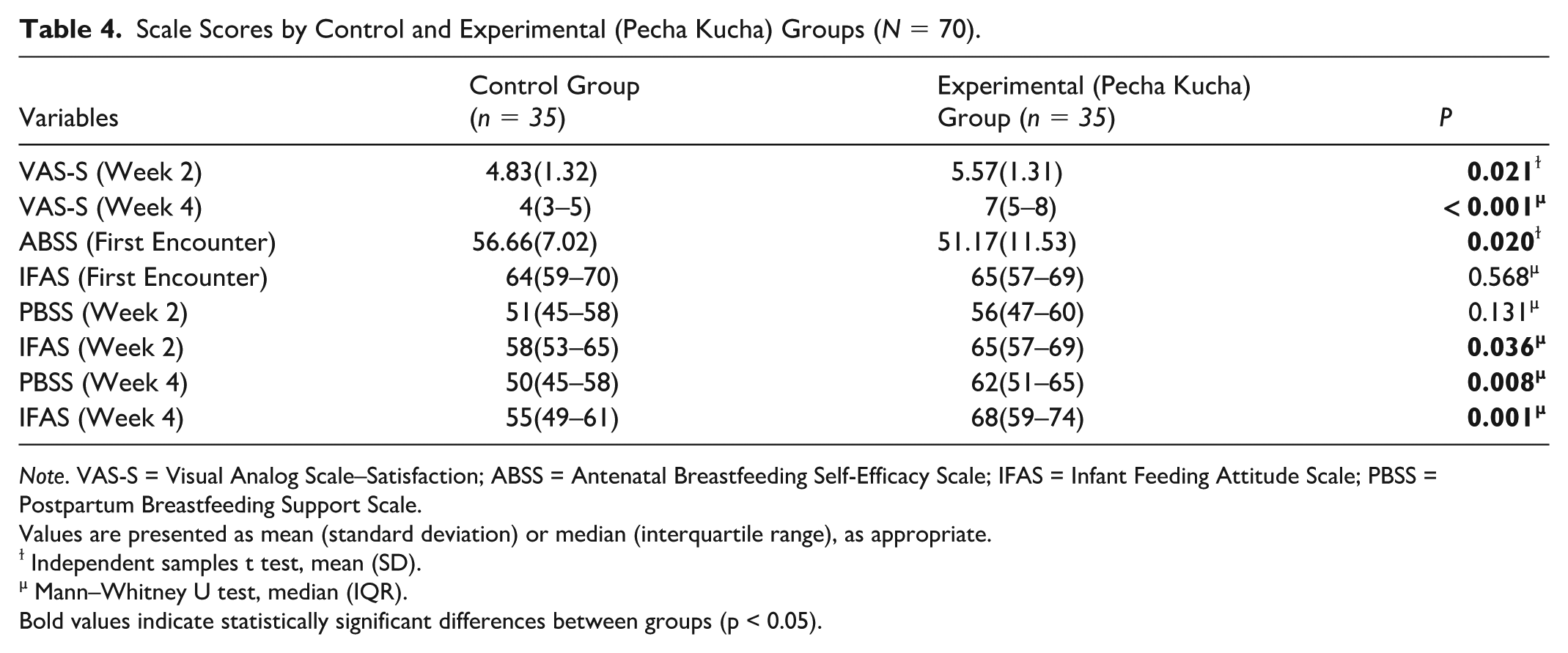
Note. VAS-S = Visual Analog Scale–Satisfaction; ABSS = Antenatal Breastfeeding Self-Efficacy Scale; IFAS = Infant Feeding Attitude Scale; PBSS = Postpartum Breastfeeding Support Scale.
Values are presented as mean (standard deviation) or median (interquartile range), as appropriate.
ɫ Independent samples t test, mean (SD).
µ Mann–Whitney U test, median (IQR).
Bold values indicate statistically significant differences between groups (p < 0.05).
Infant Feeding Attitude Scale
The IFAS measurements were repeated three times. In the results of the analysis of the change in the three measurement scores over time in the study groups, it was found that the IFAS scores changed significantly over time in both groups (p < 0.001). In the control group, there were significant changes between the first encounter and the Week 2 measurements (p = 0.021) and between the first encounter and the Week 4 measurements (p < 0.001), while the change between the Week 2 and Week 4 measurements was not significant (p = 0.219). Accordingly, the IFAS scores declined significantly from baseline at both Week 2 and Week 4. The measurement intervals in which significant changes were detected in the experimental group were the first encounter and Week 2 (p = 0.001) and Week 2 and Week 4 (p = 0.010). In the experimental group, the Week 4 IFAS score increased significantly compared to the first encounter and the Week 2 measurement scores (Table 5).
Changes in the Infant Feeding Attitude Scale Over Time by Study Groups (N = 70).
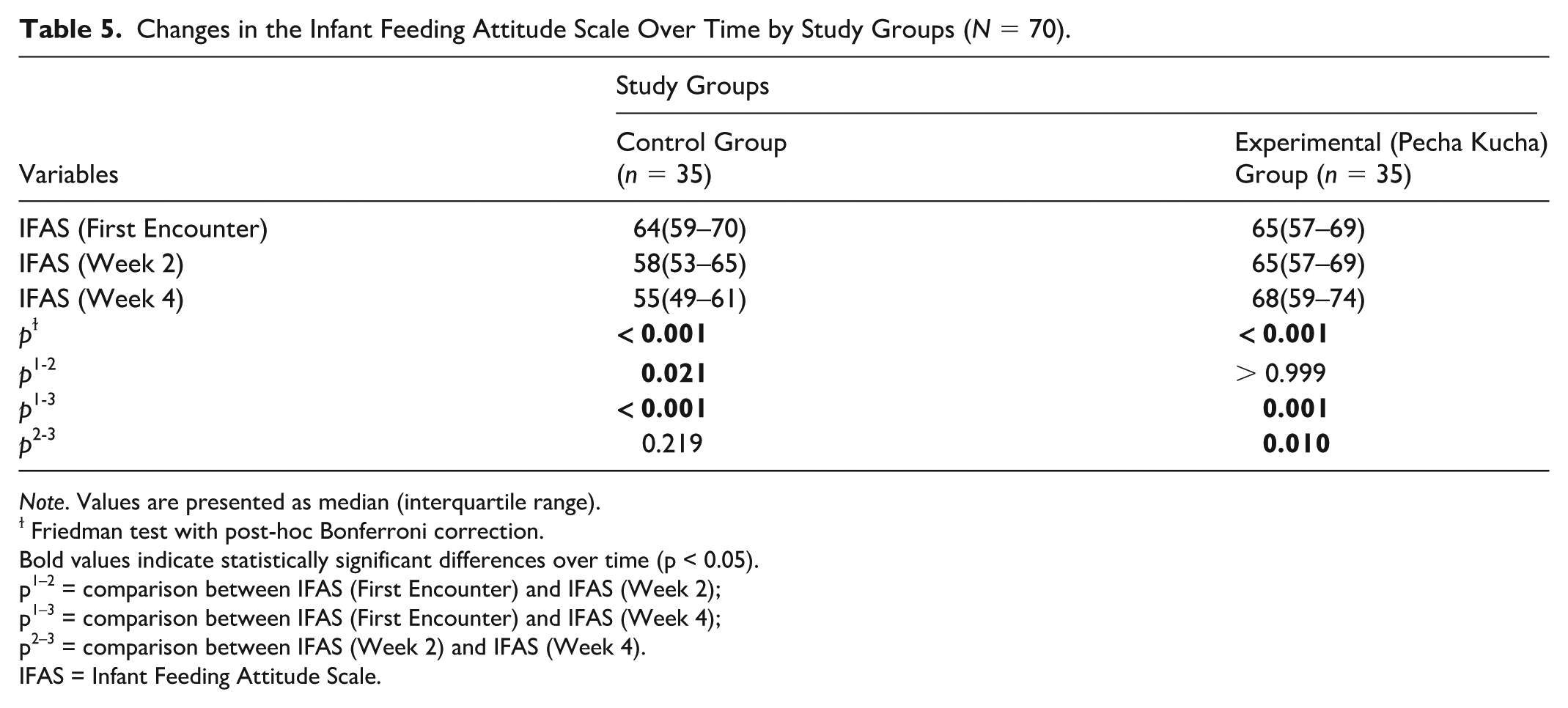
Note. Values are presented as median (interquartile range).
ɫ Friedman test with post-hoc Bonferroni correction.
Bold values indicate statistically significant differences over time (p < 0.05).
p1–2 = comparison between IFAS (First Encounter) and IFAS (Week 2);
p1–3 = comparison between IFAS (First Encounter) and IFAS (Week 4);
p2–3 = comparison between IFAS (Week 2) and IFAS (Week 4).
IFAS = Infant Feeding Attitude Scale.
Breastfeeding Self-Efficacy
Analysis of PBSS scores over time showed significant changes between the measurements in both study groups (p = 0.001). In the control group, Breastfeeding Self-Efficacy scores at both Week 2 and Week 4 were significantly lower compared to baseline (p = 0.018 and p = 0.001, respectively), but there was no significant difference between Week 2 and Week 4 scores (p > 0.999). In the experimental group, the increase observed at Week 2 compared to baseline was not statistically significant, while the score at Week 4 was significantly higher than both baseline and Week 2 measurements. (Table 6).
Change in Breastfeeding Self-Efficacy Scale Over Time by Study Groups (N = 70).
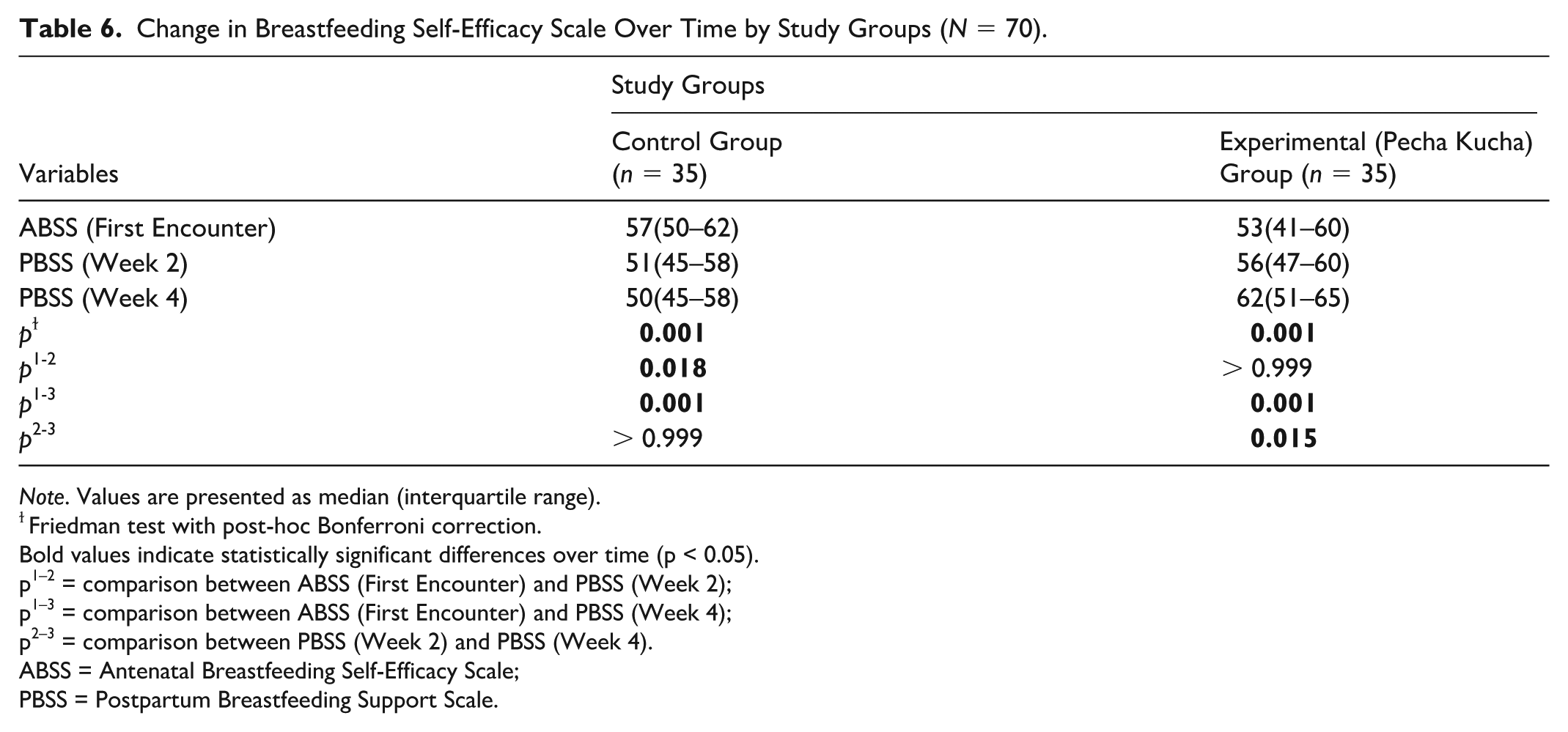
Note. Values are presented as median (interquartile range).
ɫFriedman test with post-hoc Bonferroni correction.
Bold values indicate statistically significant differences over time (p < 0.05).
p1–2 = comparison between ABSS (First Encounter) and PBSS (Week 2);
p1–3 = comparison between ABSS (First Encounter) and PBSS (Week 4);
p2–3 = comparison between PBSS (Week 2) and PBSS (Week 4).
ABSS = Antenatal Breastfeeding Self-Efficacy Scale;
PBSS = Postpartum Breastfeeding Support Scale.
Visual Analog Scale Satisfaction
A significant change in VAS-S scores was observed between the two measurements in both groups (p < 0.05). In the experimental group, the median VAS-S score increased from 6 (5–6) at Week 2 to 7 (5–8) at Week 4 (z = -3.409, p = 0.001). Of the participants in the experimental group, 26 had an increased score, five had a decreased score, and four had no change. In the control group, the VAS-S score significantly decreased at Week 4 compared to Week 2 (z = -2.828, p = 0.005), with 18 participants showing a decrease, five an increase, and 12 no change (Table 7).
Change in Visual Analog Scale Satisfaction Over Time by Study Groups (N = 70).
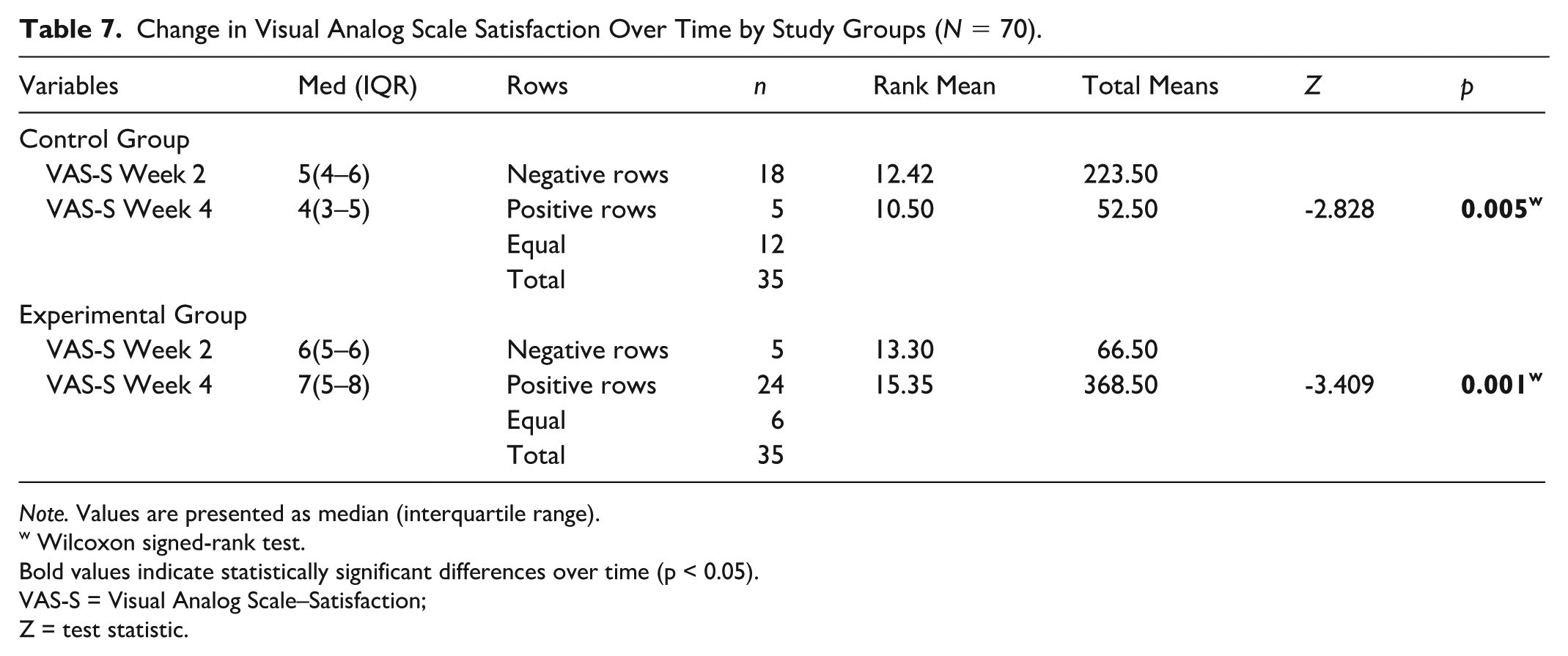
Note. Values are presented as median (interquartile range).
w Wilcoxon signed-rank test.
Bold values indicate statistically significant differences over time (p < 0.05).
VAS-S = Visual Analog Scale–Satisfaction;
Z = test statistic.
Discussion
Breastfeeding has played an important role in the nutrition and growth of infants from the past to the present (Yüksel & Bal Yılmaz, 2021). To ensure the sustainability of breastfeeding and increase its rates, pregnant women should be provided with breastfeeding education by healthcare professionals. Breastfeeding education is provided through various methods. This study examined the effects of antenatal breastfeeding education provided through the Pecha Kucha method on postpartum breastfeeding self-efficacy, infant feeding attitudes, and breastfeeding satisfaction. The antenatal and early postpartum periods represent critical phases during which women exhibit an increased demand for comprehensive and evidence-based information on breastfeeding. Therefore, during this period, there is a need to seek information from many sources and to receive education on breastfeeding (Baker & Yang, 2018). In our study, sociodemographic and obstetric characteristics were found to be similar between the experimental and control groups, ensuring homogeneity (Tables 1 and 2). According to the results, it was determined that the sociodemographic and obstetric characteristics of all pregnant women participating in the study were similar in the experimental and control groups. These results are important in terms of homogeneity between the groups. It was determined that 54.3% of the pregnant women had received breastfeeding education before, and this education was received from (63.4%) midwives, (23.6%) nurses and (10.4%) online. In the study by Bednarek et al. (2023), it was reported that the majority of women (85%) obtained information about breastfeeding from the internet, while 58.5% received information from healthcare personnel (Bednarek et al., 2023). In the study by Uyar and Beydağ (2022), it was stated that mothers obtained breastfeeding information from the internet (69.2%) and from healthcare personnel (67.6%; Uyar & Beydağ, 2022).
Self-efficacy is an important factor in breastfeeding, and higher self-efficacy is associated with greater breastfeeding continuation (Aktürk Kuru & Kolcu, 2023; Öztürk et al., 2022). Our study indicates that Pecha Kucha-based antenatal breastfeeding education had a positive effect on postpartum breastfeeding self-efficacy compared to standard education. While self-efficacy declined in the control group, women educated with the Pecha Kucha method showed sustained improvement, suggesting that this approach can help maintain and strengthen maternal confidence in breastfeeding during the early postpartum period. In the literature, there has been no study evaluating the effect of breastfeeding education delivered through the Pecha Kucha method on breastfeeding self-efficacy. However, there are studies in the literature where breastfeeding education has been delivered through various methods and breastfeeding self-efficacy has been examined. In the study by Dodou et al. (2021), it was concluded that breastfeeding education delivered via phone increased breastfeeding self-efficacy (Dodou et al., 2021). In the study by Ocaktan Çetindemir and Cangöl (2024), it was found that women who received breastfeeding education using the "teach-back" method had higher breastfeeding self-efficacy compared to women who received standard breastfeeding education (Ocaktan Çetindemir & Cangöl, 2024). In the study by Selvi et al. (2021) it was found that the group that received breastfeeding education during pregnancy had higher breastfeeding self-efficacy levels. It was found that the breastfeeding self-efficacy levels of women who received education in the postpartum period were similar to those who did not receive education (Selvi et al., 2021). As in our study, the literature also indicates that both antenatal and postpartum breastfeeding education increase breastfeeding self-efficacy (Chipojola et al., 2020; Wong et al., 2021). Pecha Kucha based breastfeeding education enhances self-efficacy more than standard methods by using visuals and concise information, aiding better retention.
Having knowledge about breastfeeding during the antenatal period positively influences infant feeding attitudes. Breastfeeding education provided during this period is one of the best ways to encourage positive infant feeding practices. Therefore, women should be informed and encouraged about breastfeeding starting from the pregnancy period in order to improve their infant feeding attitudes (Abdulahi et al., 2020; Abuidhail et al., 2019). Our study showed that infant feeding attitudes developed differently between groups. While the control group displayed a decline in attitudes over time, women who received Pecha Kucha-based education demonstrated more positive attitudes by the later follow-up. Notably, no prior research has specifically investigated the effect of the Pecha Kucha method on infant feeding attitudes, highlighting the novelty of this study and the need for further research in this area. However, there are many studies that examine infant feeding attitudes using different education methods (Parry et al., 2019; Piro & Ahmed, 2020). In their study, Savaş et al. (2024) found that mothers who received breastfeeding education based on psychosexual development theory had a greater increase in their infant feeding attitudes compared to mothers who received standard breastfeeding education (Savaş et al., 2024). Piro and Ahmed (2020) stated that pregnant women who received breastfeeding education had higher infant feeding attitudes 2 months postpartum compared to those who did not receive the education (Piro & Ahmed, 2020). Abdulahi et al. (2021) found that the group that received peer-supported breastfeeding education had higher infant feeding attitudes compared to the group that did not receive the education (Abdulahi et al., 2021). Consistent with these results, our study also supports the positive role of structured antenatal education in shaping infant feeding attitudes.
Breastfeeding satisfaction is the sense of fulfillment or contentment experienced during breastfeeding, resulting from meeting the needs of both the mother and the infant. Mothers’ knowledge, attitudes, self-efficacy, and social support regarding breastfeeding all play a significant role in influencing their breastfeeding satisfaction (Awaliyah et al., 2019). Enhancing infant feeding attitudes and breastfeeding self-efficacy is essential for increasing maternal satisfaction with breastfeeding. In our study, breastfeeding satisfaction improved over time among women who received Pecha Kucha-based antenatal education, whereas a decline was observed in the control group. These findings suggest that innovative and engaging educational methods may contribute to sustaining positive breastfeeding experiences. In the literature, there are studies that indicate breastfeeding education affects breastfeeding satisfaction (Ahmed & Roumani, 2020; Hu et al., 2020). Hu et al. (2020), in their study aimed at investigating the effects of a health belief model-based intervention on breastfeeding knowledge, breastfeeding behaviors, and breastfeeding satisfaction in women who had Cesarean sections, reported that the experimental group had higher breastfeeding satisfaction at discharge, 42 days postpartum, and 4 months postpartum compared to the control group (Hu et al., 2020). Ahmed and Roumani (2020), in their study aimed at evaluating the effects of web-based breastfeeding education and follow-up on breastfeeding self-efficacy and satisfaction in mothers during the 1st, 2nd, and 3rd months postpartum, reported that web-based breastfeeding education and follow-up increased the mothers’ breastfeeding self-efficacy and satisfaction (Ahmed & Roumani, 2020). Women should begin receiving breastfeeding education during the antenatal period, as increased knowledge in this area has been shown to enhance breastfeeding self-efficacy in the postpartum period. Providing this education through engaging and memorable methods is crucial to maximize its effectiveness. The Pecha Kucha method, characterized by its visual and time-limited presentation style, is an approach that can be effectively utilized in antenatal education. This method not only promotes self-efficacy but also positively influences infant feeding attitudes and overall maternal satisfaction. Based on the experience gained in this study, Pecha Kucha can feasibly be integrated into routine antenatal care, particularly in time-constrained clinical settings. Future research could examine the effects of incorporating participant feedback, interactive discussions, or extended follow-up periods on maternal outcomes, providing further evidence to optimize the method’s effectiveness. Therefore, this method holds promise for improving the quality and reach of antenatal breastfeeding education.
Limitations of the Study
This study has several limitations. First, it was conducted in a single center with participants limited to pregnant women in their third trimester, which restricts the generalizability of the findings to other populations, stages of pregnancy, and clinical settings. Second, the reliance on self-reported data may have introduced social desirability or recall bias, potentially influencing the accuracy of responses. Third, the absence of blinding in group assignment and outcome assessment may have introduced performance or detection bias. Finally, the relatively short follow-up period limited the ability to evaluate the long-term effects of the intervention on sustained breastfeeding behaviors and outcomes. Additionally, the sample size was calculated based on a large effect size (Cohen’s d = 0.91) reported by Tseng et al. (2020), which may have overestimated the true effect and limited generalizability across settings.
Conclusion
The Pecha Kucha method represents a concise and engaging approach to antenatal breastfeeding education. Its visual and auditory format facilitates understanding and retention of information, making it a practical tool for healthcare professionals. Implementing this method in prenatal education programs may enhance maternal confidence and satisfaction in breastfeeding, and could serve as an effective alternative to traditional teaching methods.
Footnotes
Ethical Considerations
Permission for the study was obtained from the Scientific Research Ethics Committee of a university (decision No. 2024-1, July 11, 2024). Permission was obtained from the institution where the study was conducted. Pregnant women were informed about the study by the researcher before participating in the study and their written and verbal informed consent was obtained.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this study are available on request from the corresponding author.
Trial Registration
This study was registered at ClinicalTrials.gov (Identifier: NCT06528782).