
Abstract
Background:
Technology-based breastfeeding support interventions have shown mixed effectiveness. International studies have reported improved breastfeeding outcomes, whereas U.S.-based studies have demonstrated variable results.
Research Aim:
The aim of this study was to describe the association between engagement with a personalized text-based breastfeeding support platform and infant feeding outcomes.
Methods:
This secondary observational within-trial analysis used data from a randomized, controlled trial conducted at an urban tertiary care center (January 2020–January 2021). The parent trial compared usual care with an intervention consisting of weekly educational text messages plus on-demand personalized breastfeeding support. This analysis included only participants randomized to the intervention arm. The exposure of interest was participant engagement with the breastfeeding support platform. The primary outcome was breastfeeding exclusivity at 6 weeks postpartum, obtained through direct text report or medical record documentation. Secondary outcomes included additional infant feeding measures and parental mood assessment. Of 216 subjects in the randomized, controlled trial, 92 intervention-arm subjects were included.
Results:
Participants were 45.7% (n = 42) Black, 52.2% (n = 48) primiparous, and 58.7% (n = 54) with commercial insurance. Overall, 54.4% (n = 50) of participants submitted at least one breastfeeding question, most frequently during the first postpartum week. There was no difference in the primary outcome between those who queried the platform and those who did not (48% vs. 48.8%, p = .94). There were no differences in the secondary outcomes analyzed.
Conclusion:
Engagement with a personalized text-based breastfeeding support platform was not associated with improved breastfeeding outcomes at 6 weeks postpartum. Further research is needed to clarify how technology-based interventions can effectively support breastfeeding families.
Keywords
Introduction
Breastfeeding is a public health priority due to the numerous child and maternal health benefits. The U.S. Centers for Disease Control and Prevention, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists recommend exclusive breastfeeding for the first 6 months of infant life with continued breastfeeding through 2 years and beyond as mutually desired by the parent and child (American College of Obstetricians and Gynecologists, 2021; Centers for Disease Control and Prevention, 2022; Meek & Noble, 2022).
In the United States, 83.2% of parents attempt breastfeeding with 24.9% exclusively breastfeeding at 6 months and 35.9% reporting breastfeeding at 12 months (Centers for Disease Control and Prevention, 2022). The significant differences in the rates of initiation, continuation, and exclusivity underscore the difficulty in establishing and maintaining breastfeeding even in parents motivated to do so. Professional and informal support during this time can positively impact breastfeeding outcomes (Gavine et al., 2022).
Recently, digital technologies have been leveraged to provide breastfeeding education and support in the prenatal and immediate postpartum periods. Although these programs appear to improve breastfeeding outcomes internationally, similar programs in the United States have yielded mixed results (Bender et al., 2022; Gallegos et al., 2014; Jiang et al., 2014; Lewkowitz et al., 2020; Martinez-Brockman et al., 2018; Moniz et al., 2015).
One of the limitations of digital platforms is that they typically educate or engage parents passively. Although this makes such platforms convenient for healthcare providers, it is also possible that it renders the support provided too reliant on parent motivation and less adaptable to individual needs. If this hypothesis is true, it would suggest that parents who engage with digital platforms may be more likely to achieve their desired breastfeeding outcomes. Therefore, this study‘s aim was to describe the relationship of parent engagement with a text-based breastfeeding support platform and infant feeding outcomes.
Methods
Research Design
This is a secondary observational within-trial analysis of a randomized, controlled trial (RCT) (Bender et al., 2022). The RCT was approved by our institutional review board and registered at ClinicalTrials.gov (NCT04108533).
Setting and Relevant Context
The RCT was conducted in a Baby-Friendly academic tertiary care center with ~4,000 deliveries per year in a northeastern metropolis in the United States. Standard in-hospital postpartum care at this institution included at least one encounter with a lactation consultant prior to hospital discharge. There is no standard post-discharge lactation support. A hospital-based warmline is available. Lactation support is pursued by individual patients on their own as needed.
Sample
Details of the parent RCT have been published previously and are reviewed briefly here (Bender et al., 2022). Eligible patients had a nonanomalous singleton gestation, no contraindications to breastfeeding, were able to communicate in English, and had access to a cellphone with unlimited text-messaging. Parents were enrolled in the late preterm period and asked to send a confirmatory text message for participation prior to delivery. After delivery of a healthy term neonate, parents were randomized in a 1:1 fashion to text-based support or usual care.
Key Messages
Research has previously demonstrated that breastfeeding support, both professional and informal, can improve breastfeeding outcomes. Electronic or telehealth support, however, has had mixed success in improving breastfeeding outcomes; this may be related to the passive nature of this intervention and its reliance upon parent engagement for success.
In this secondary analysis, parents who engaged with a text-based breastfeeding support platform did not have improved breastfeeding outcomes at six weeks postpartum.
Peak engagement with the platform occurred in the first week postpartum
This study illustrates the limitations of digital breastfeeding support and identifies the first week postpartum as a time of focus for future interventions to improve breastfeeding
Intervention
For this secondary analysis, we have limited the population to only parents randomized to the text-based support arm. These parents received a congratulatory text after delivery. Thereafter, they received weekly informational and/or motivational text messages about breastfeeding. They also received weekly text messages asking for details on infant feeding (inquiry texts), including type of feeding, method of feeding, reasons for choosing said infant feeding style, and frequency of each type of feeding. Figure 1 provides examples.
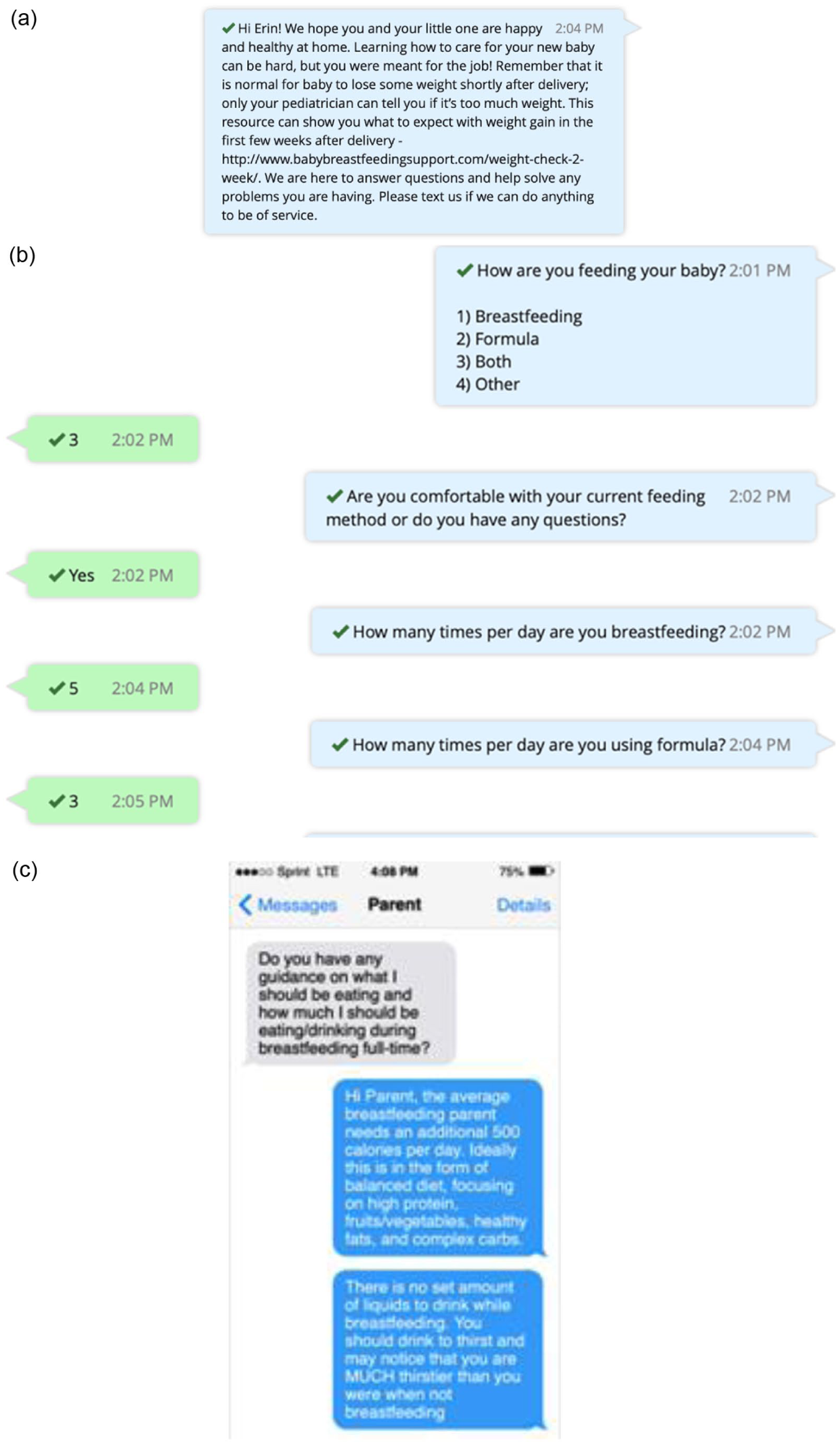
Breastfeeding support platform text message examples: (a) informational text message, (b) inquiry text message; (c) two-way conversation.
Each type of weekly text continued until 6 weeks postpartum. These parents also had the option of asking questions or presenting breastfeeding concerns via text as needed. The main author, a board-certified OBGYN with a special interest in breastfeeding medicine, responded to parent questions and concerns daily. Text conversations were the preferred method of communication. The goal of using text messaging primarily was to determine the efficacy of an intervention with minimal patient burden (with respect to traveling to an appointment, for example) and minimal provider/healthcare burden (when considering the feasibility of scaling up a clinical program). Study participants were able to seek alternative lactation support if desired. Rarely, referrals were made for telehealth or in-person visits with lactation or healthcare professionals for unresolved or ongoing breastfeeding challenges. In these cases, the primary author sent a message to central scheduling noting that a breastfeeding concern was present and requesting a visit. There was no direct communication between the primary author and healthcare providers. The healthcare providers did not have access to the text-based platform communications.
Parents who did not engage with the program continued to receive weekly messages. They were included in the original RCT and this secondary analysis if they had data available on the primary outcome.
Two hundred and sixteen parents were randomized in the original RCT from January 2020 to January 2021. One hundred and six were randomized to the intervention arm; 92 had data on the primary outcome and were included in this study.
The original RCT had a target enrollment of 190 subjects to detect a 50% increase in breastfeeding exclusivity from the baseline rate of 40%. The sample size for this secondary analysis was fixed based on the parent trial and is therefore underpowered to detect this same difference between groups. This trial would be powered to detect a rate of breastfeeding exclusivity of 68% in the experimental group or a 28% difference in exclusivity between groups.
Measurement
For this study, the exposure of interest was engagement with the breastfeeding support platform. This was defined in two ways: (a) asking one or more questions of the platform during the 6 weeks of trial enrollment or (b) responding to ≥50% (three or more of six) of inquiry texts received. We chose this number because three was the median number of responses in the overall cohort. We also considered number of inquiry text responses as a continuous variable.
Importantly, although the exposure was defined as participant engagement with the program, it is important to underscore that the responses participants received also must be considered part of the experimental exposure. For example, a particular participant’s perception of a response may have affected their willingness to engage further with the program. In this study, the primary author responded to every patient inquiry.
The primary outcome was breastfeeding exclusivity at 6 weeks postpartum. Patients were considered to be exclusively breastfeeding if they reported only breastfeeding and/or feeding expressed breastmilk. This was ascertained either by affirmative response to the sixth week inquiry text, as reviewed earlier, or by review of documentation at the postpartum visit. It is not possible to determine how this information was obtained at each individual postpartum visit, but typical clinical practice at the time of study completion was to elicit infant feeding method by verbal interview with the postpartum provider.
Secondary feeding outcomes included any breastfeeding at 6 weeks postpartum and rate of formula use. Any breastfeeding included the provision of any breastmilk directly or via breastmilk expression as reported in the sixth week inquiry text or by review of documentation at the postpartum visit. Additional secondary outcomes included postpartum visit completion and parent mood. Parent mood was assessed with the Patient Health Questionnaire-2, a brief questionnaire asking about depressed mood and anhedonia over the past 2 weeks. Scores on the questionnaire range from 0 to 6, with scores of 3 or more indicating a need for further evaluation for postpartum mood disorder. This was administered via text message at 2 and 6 weeks postpartum.
Data Collection
Eligible parents were approached in person or via secure message in the electronic medical record, and written informed consent was obtained. Consented parents were sent a confirmatory text message for participation prior to delivery. Recruitment for the parent RCT began in January 2020 and concluded in October 2020. Follow-up and data collection concluded in January 2021.
The primary author collected demographic, obstetric, delivery, and postpartum data through direct chart review of the electronic medical record. Although the primary author was not blinded to study arm at the time of data abstraction, she was not participating in active clinical care of enrolled participants. Infant feeding practices were reported by the parent through the text-based platform. Data reviewed for this secondary analysis were deidentified.
Data Analysis
Parents who engaged with the platform were compared with those who did not. We considered each form of engagement separately as well as together. Data are presented as number (percent), mean (standard deviation), and median (interquartile range) depending on the variable and its distribution. Bivariate comparisons of demographic and clinical characteristics and labor and delivery outcomes were performed with Fisher’s exact tests and χ2 tests for categorical variables and unpaired, two-tailed t tests or Wilcoxon rank-sum tests for continuous variables, where appropriate. Median differences with Hodges–Lehmann 95% confidence intervals (CIs) for nonparametric comparisons and risk differences/odds ratios with 95% CIs for categorical outcomes were calculated for select outcomes. Effect sizes and 95% CIs are presented to quantify the magnitude and precision of observed differences. Multivariable logistic regression modeling was used to adjust for all confounders and calculate adjusted odds ratios (aORs). p Values of <.05 were considered statistically significant. All analyses were performed using Stata software (StataCorp LLC, College Station, TX).
Results
Engagement as Question
The median number of questions sent to the platform was one per parent. The number of questions per parent ranged from zero to 21. Most questions were posed in the first postpartum week, as shown in Figures 2 and 3.
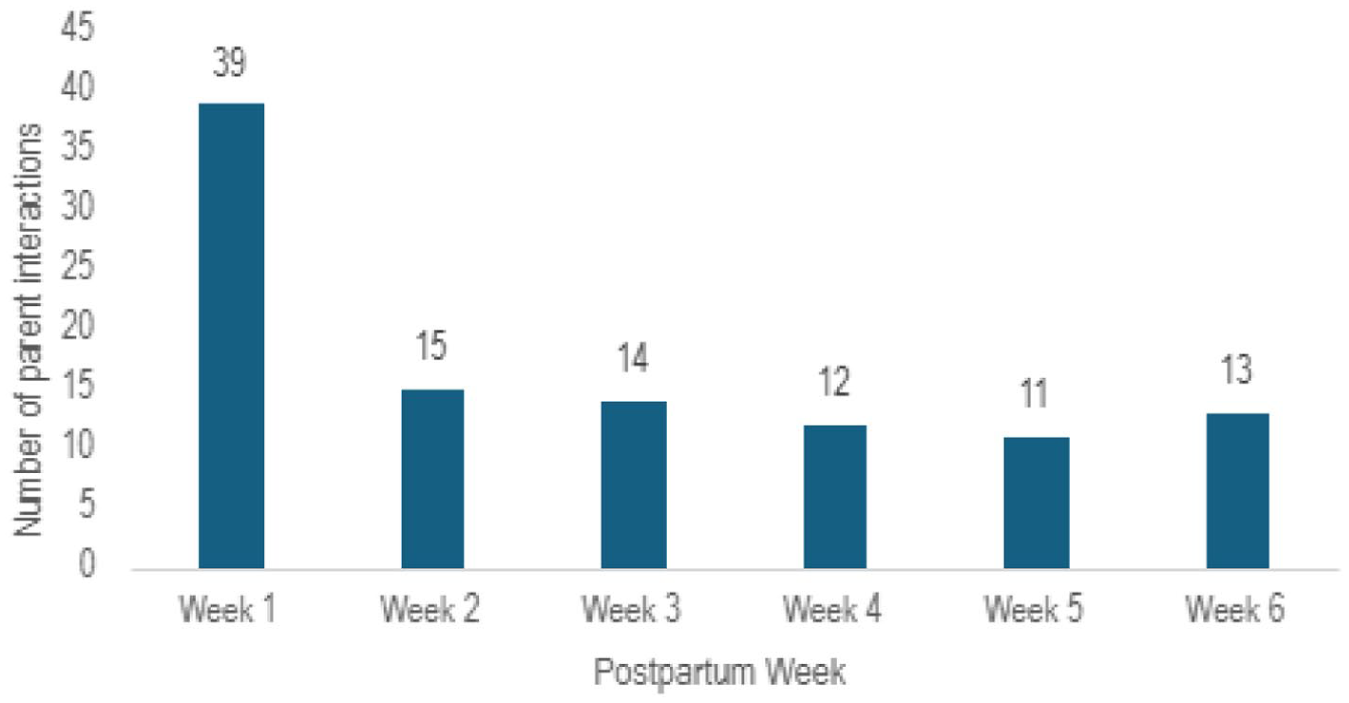
Number of parents interacting with breastfeeding support platform by postpartum week.
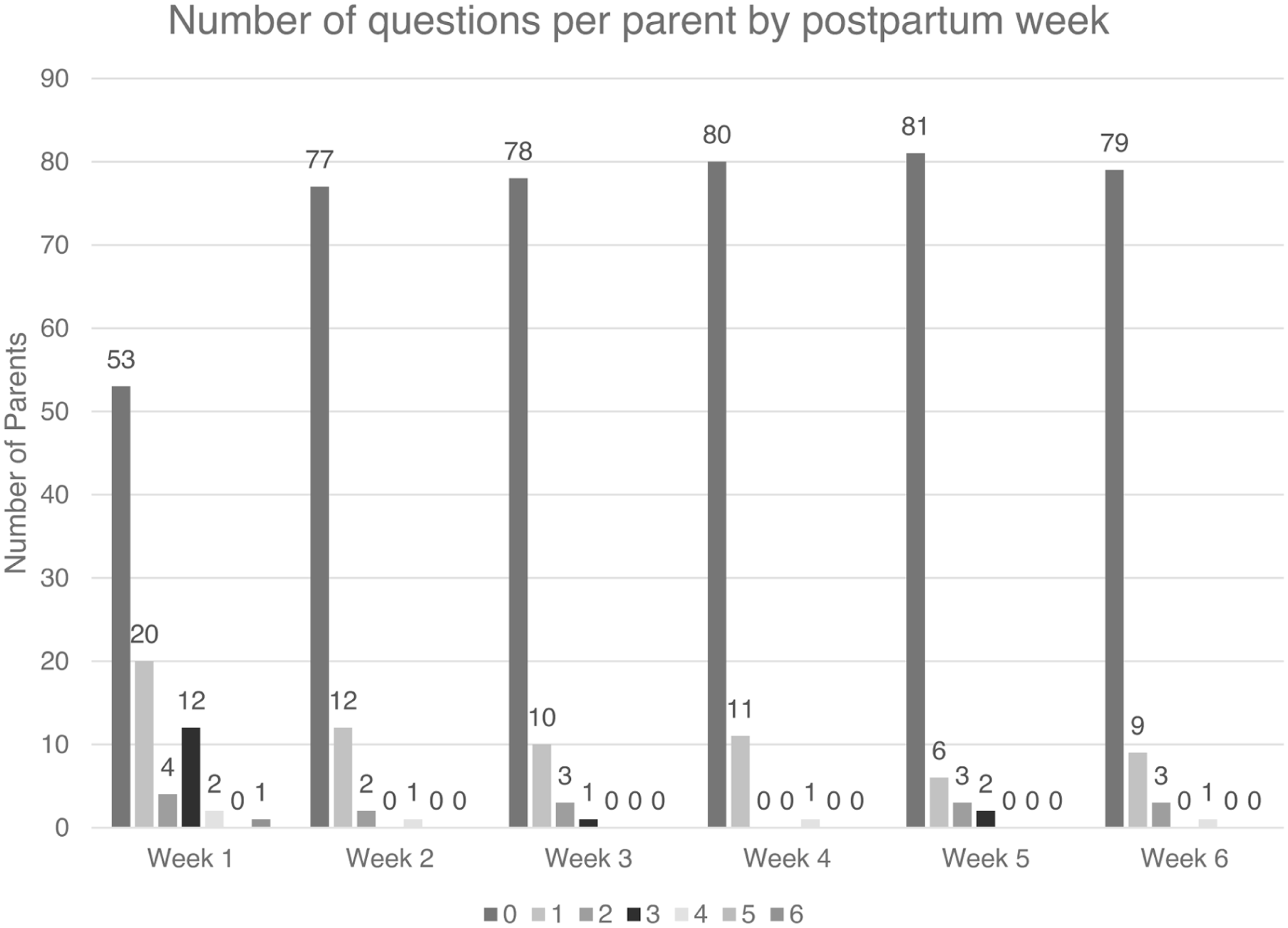
Number of questions sent to breastfeeding support platform per parent by postpartum week.
Fifty parents (53.7%) engaged with the platform during the first 6 weeks postpartum. Table 1 compares the demographic and delivery characteristics of these parents with those of parents who did not engage with the text-based platform. Parents who engaged with the platform were more likely to be primiparous (64% vs. 37.2%, p = .01).
Parent Characteristics by Question Engagement.
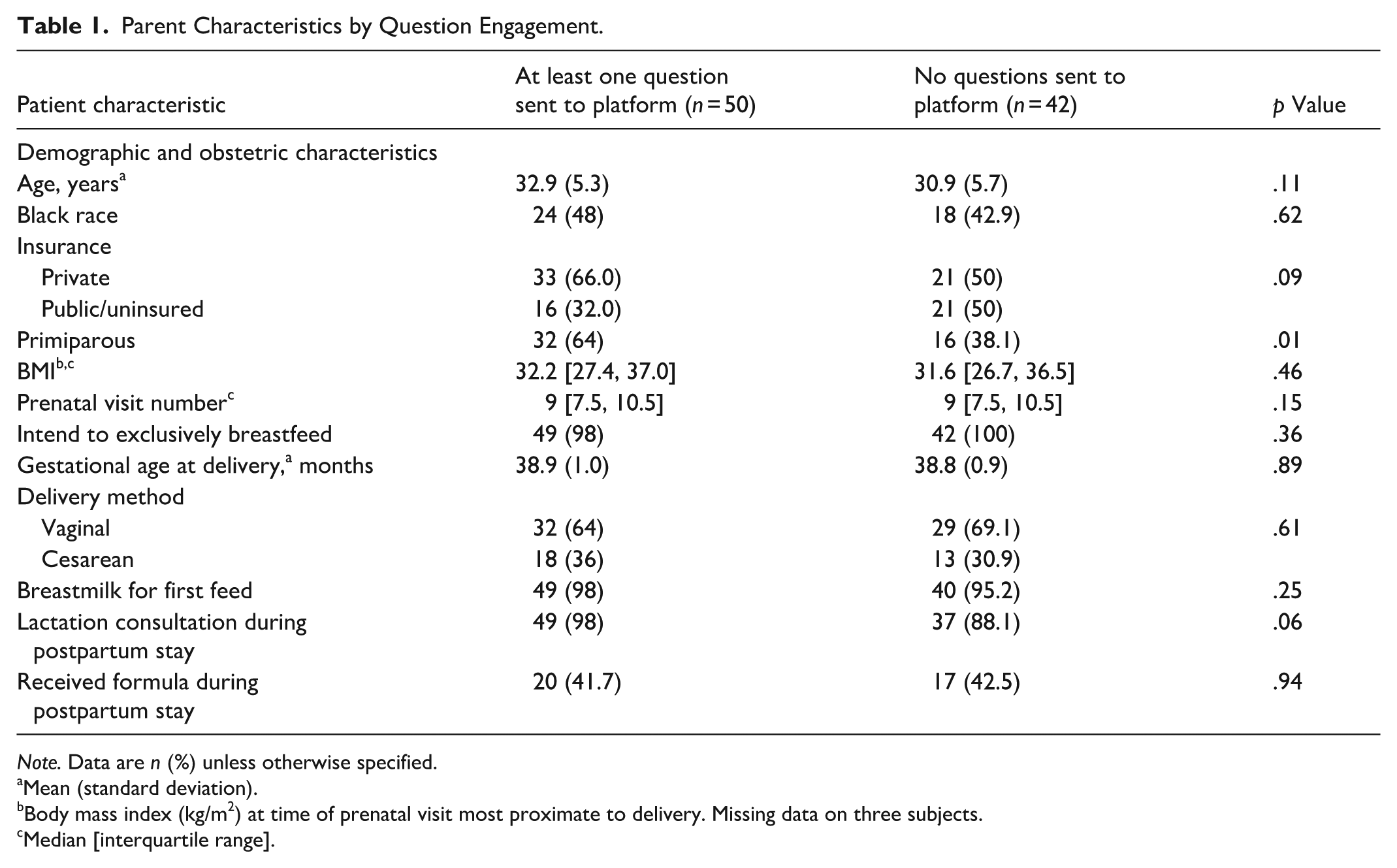
Note. Data are n (%) unless otherwise specified.
Mean (standard deviation).
Body mass index (kg/m2) at time of prenatal visit most proximate to delivery. Missing data on three subjects.
Median [interquartile range].
There was no difference in the primary outcome by platform engagement. Twenty-four parents (48%) who engaged with the platform were exclusively breastfeeding at 6 weeks postpartum compared with 21 (50%) of those who did not engage with the platform (risk difference −3.2%, 95% CI 0.18–0.12, p = .85). This remained true after adjustment for parity (aOR 1.15, 95% CI 0.48–2.74). There were no differences in breastfeeding exclusivity by number of interactions with the platform (p = .76). There also were no differences between groups in the secondary outcomes reported in Table 2.
Breastfeeding and postpartum outcomes by question engagement.
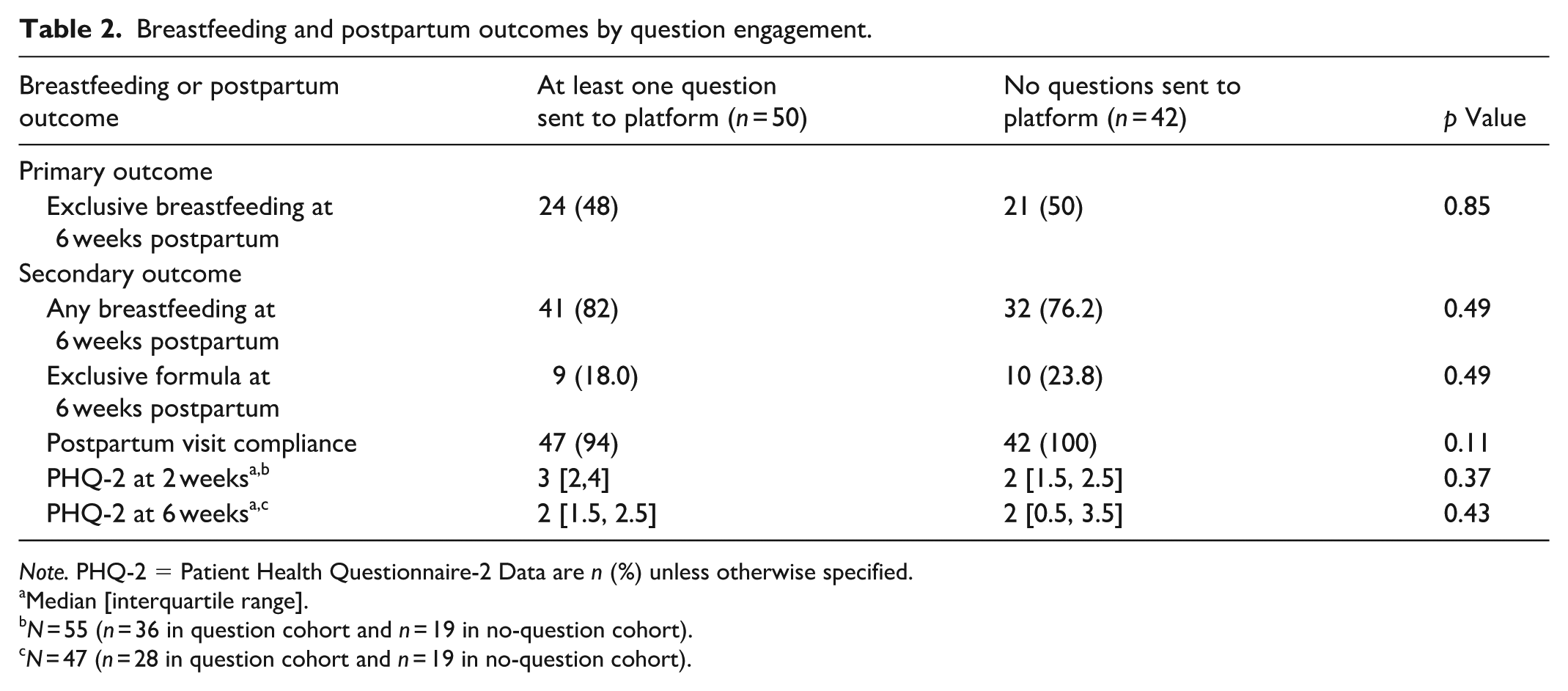
Note. PHQ-2 = Patient Health Questionnaire-2 Data are n (%) unless otherwise specified.
Median [interquartile range].
N = 55 (n = 36 in question cohort and n = 19 in no-question cohort).
N = 47 (n = 28 in question cohort and n = 19 in no-question cohort).
We then assessed question engagement as a continuous rather than categorical variable. There was no difference in the number of questions received from those who were or were not breastfeeding exclusively at 6 weeks postpartum (median one vs one; median difference 0; p = .77).
Engagement as Responding to Inquiry Texts
The median number of inquiry text responses was three per parent. The number of responses per parent ranged from zero to six. Fifty-two (55.9%) individuals responded to at least half the inquiry texts received. Parents who responded to inquiry texts were more likely to be older, of non-Black race, or privately insured. As shown in Table 3, there were no other differences in the other demographic or obstetric characteristics examined by parent engagement.
Parent Characteristics by Response Engagement.
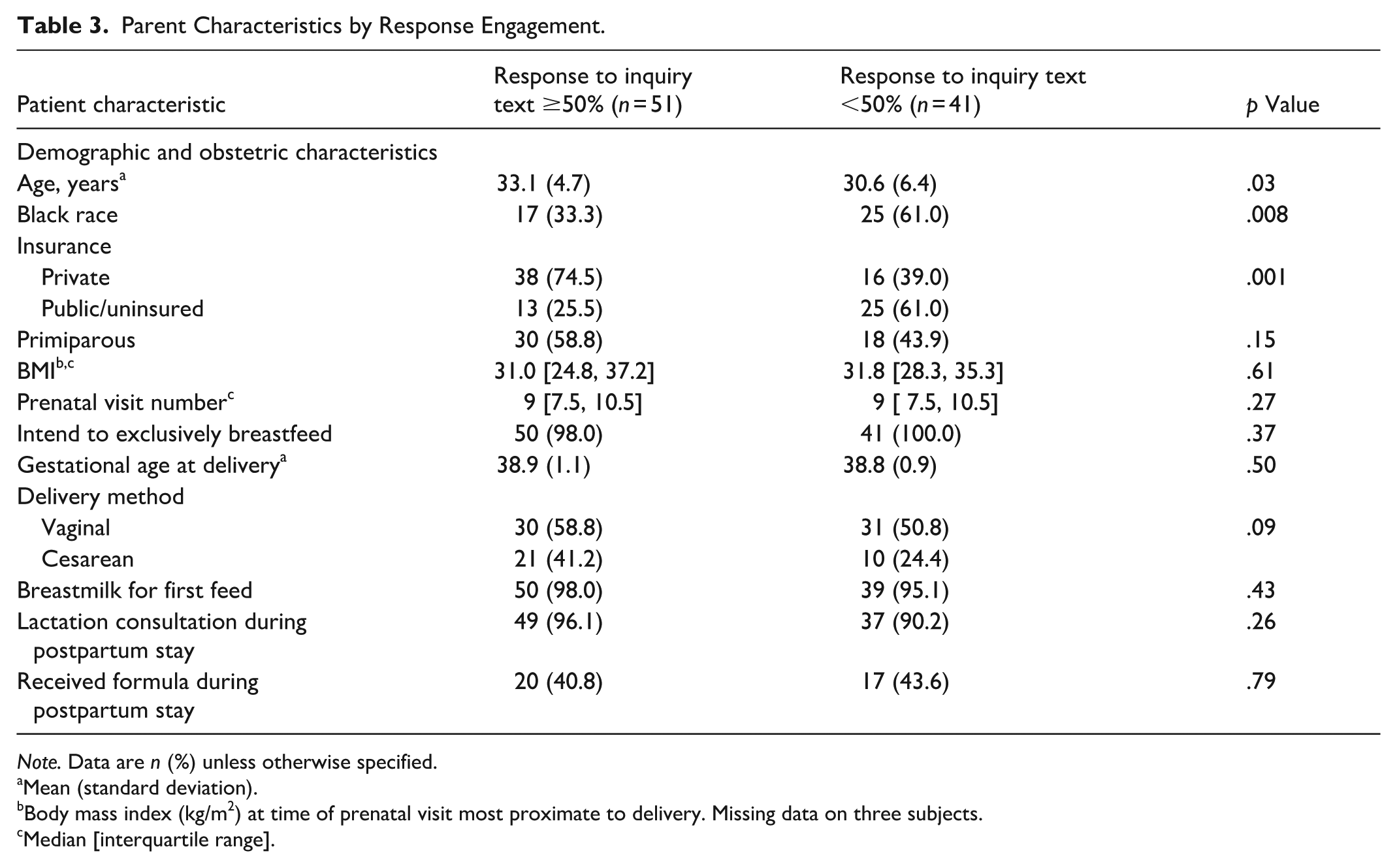
Note. Data are n (%) unless otherwise specified.
Mean (standard deviation).
Body mass index (kg/m2) at time of prenatal visit most proximate to delivery. Missing data on three subjects.
Median [interquartile range].
As shown in Table 4, there were no differences in the primary or secondary outcomes examined by parent inquiry text engagement. Although exclusive breastfeeding at 6 weeks postpartum occurred in 28 parents (54.9%) responding to >50% of inquiry texts compared with 17 (41.5%) responding to <50% (risk difference 15.5%, 95% CI −30.2 to −0.98), there was no difference after adjustment for age, race, and insurance status (aOR 1.60, 95% CI 0.66–3.91).
Breastfeeding and Postpartum Outcomes by Response Engagement.
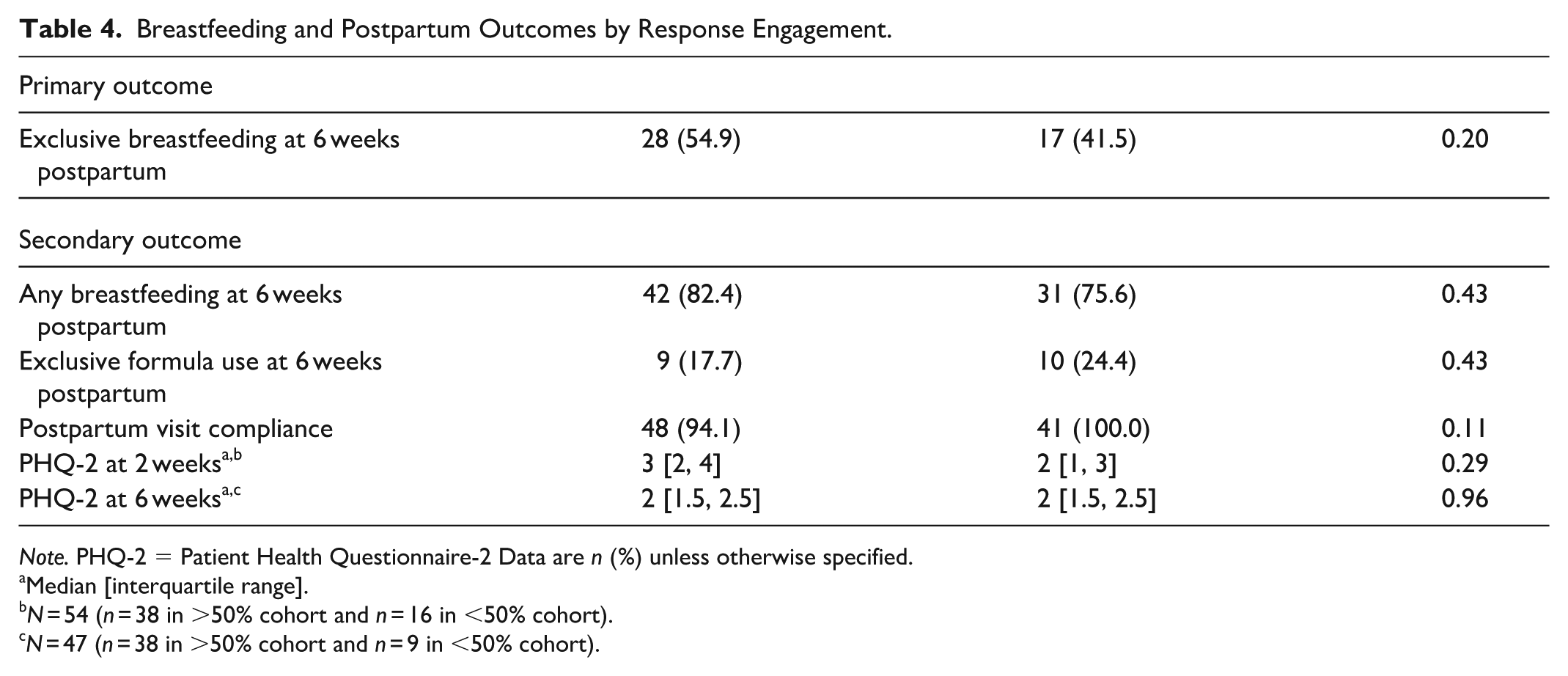
Note. PHQ-2 = Patient Health Questionnaire-2 Data are n (%) unless otherwise specified.
Median [interquartile range].
N = 54 (n = 38 in >50% cohort and n = 16 in <50% cohort).
N = 47 (n = 38 in >50% cohort and n = 9 in <50% cohort).
We then assessed inquiry text engagement as a continuous rather than categorical variable. Parents who were exclusively breastfeeding at 6 weeks postpartum responded to more inquiry texts than those who were not exclusively breastfeeding (median four vs. 2, p = .011). This association persisted after adjustment for race, age, and insurance status (aOR 1.30, 95% CI 1.04–1.63).
Engagement by Both Inquiry and Question Texts
There were 34 parents (36.6%) who were engaged in both question and inquiry texting as previously defined. There were no differences in the primary or secondary outcomes between engaged parents and unengaged parents when this definition of engagement was applied.
Discussion
In this secondary observational within-trial analysis of an RCT of text-based breastfeeding support, most parents were engaged with the text-based platform. However, platform engagement, as defined by sending a question to the platform, number of questions sent to the platform, or categorical response to texts received from the platform, was not associated with a difference in breastfeeding exclusivity at 6 weeks postpartum. We did note that parents who were exclusively breastfeeding at 6 weeks postpartum responded to more inquiry texts.
These findings are similar to those reported by Lewkowitz et al. (2020). In an RCT of 170 parents comparing a breastfeeding smartphone application with a sham application, breastfeeding rates and exclusivity were similar between the groups in the overall cohort and did not change after censoring for parents who did not use their smartphone application. Similarly, Martinez-Brockman et al. (2018) conducted a two-arm RCT of 174 women participating in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); these participants were randomized to the WIC standard of care, which included a breastfeeding peer counseling program or the standard of care plus two-way text messaging. They reported no significant difference in the odds of exclusive breastfeeding in these two groups. They did find, however, that the intensity of engagement in the first 2 weeks postpartum was a strong predictor of breastfeeding exclusivity. We hypothesize that differences in our patient population may underly our disparate results. Specifically, our patient population was majority privately insured (58%) and thus may have had access to alternative lactation support, whereas the Martinez-Brockman population consisted of only women eligible for WIC. In contrast, Unger et al. (2018) conducted a three-arm RCT in Kenya comparing one-way text messaging, two-way text messaging, and a control group and reported a higher probability of exclusive breastfeeding in the intervention arms. Specifically, the probability of exclusive breastfeeding at 10 and 16 weeks was higher in the one-way text-messaging arm and at 10, 16, and 24 weeks in the two-way text-messaging arm. This study reported a high rate of engagement, with 83% of participants in the two-way text-messaging arm asking questions of the platform (although not all related to breastfeeding). It is difficult to compare these results with those of our study directly due to the disparate setting and patient population of the two.
The results of this study should be interpreted with caution. The lack of difference in breastfeeding outcomes could mean that parents engaged in the program truly did not have different breastfeeding outcomes. Alternatively, parents who asked questions of the program may have been experiencing breastfeeding difficulty such that their breastfeeding outcomes would have been worse than the nonengaged group had they not been able to access the program. When considering this scenario, the outcome of no difference between the groups could be interpreted as a positive finding. It is also possible that parents engaged with the program were more motivated to breastfeed. In this scenario, however, we would have expected better breastfeeding outcomes with patient engagement, which was not observed. Lastly, parents who were having a more positive breastfeeding experience may have been more willing to engage with the program.
The observed association between higher inquiry-text response rates and exclusive breastfeeding merits further discussion. This relationship may reflect confounding, whereby underlying factors such as breastfeeding motivation, self-efficacy, prior experience, or access to resources influenced both engagement and outcomes. Alternatively, reverse causation is plausible: parents who were successfully breastfeeding may have been more inclined to respond to texts because they were experiencing fewer barriers, felt more confident, or remained more engaged with infant feeding routines. Conversely, parents experiencing breastfeeding difficulties may have disengaged from inquiry texts, producing an apparent association that does not represent a causal effect of engagement itself. Because engagement was not randomized in this within-trial observational analysis, causal inference regarding engagement and outcomes is limited.
We found that peak platform engagement occurred in the first week postpartum. This may be a critical time for parent education and support to help clarify and achieve breastfeeding goals. Future technology-based support research should focus on this period as a bridge from inpatient support to outpatient support.
This study has several strengths. The parent RCT was performed at a large, Baby-Friendly, academic health center with a diverse parent population. Infant feeding data were collected in real time using text messaging, thereby limiting recall bias in our parents. The use of a single investigator for triaging and responding to breastfeeding concerns minimizes variation in the intervention.
This study is not without limitations. As a single-center study, our results may not be generalizable to other parent populations despite our diverse cohort. This was a secondary analysis of an RCT, and as a result, differences in the baseline characteristics of those who did or did not engage with the platform existed. Adjusted models, however, were used to compensate for these confounders. There is no universal definition of engagement with an electronic platform, and thus, we defined it in different ways in this study. Breastfeeding outcomes were obtained from multiple modalities (i.e., patient direct report via text and chart review), which may not be equivalent to one another. The use of a single investigator for responding to breastfeeding concerns has the potential to bias results. Lastly, we were underpowered to detect differences in all the outcomes analyzed.
Conclusion
In summary, this secondary analysis did not find that engagement with a text-based breastfeeding support platform improved breastfeeding outcomes at 6 weeks postpartum. Ongoing work is needed to determine the best means of supporting parents in achieving their breastfeeding goals.
Footnotes
Acknowledgements
We acknowledge the Penn Medicine Center for Health Care Transformation and Innovation for its assistance in creating and maintaining the text-based platform used in the parent study. We also acknowledge the study participants.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.