
Abstract
Background:
The workplace experience of low-wage breastfeeding employees is not well studied.
Research Aims/Questions:
To identify low-wage employees’ workplace barriers and facilitators to breastfeeding at 4 and 6 months.
Methods:
Data were collected from 111 low-income participants in a Washington, DC, pediatric clinic. Eligible participants had a child less than 3 years old, were employed when their child was less than 1 year old, and had either breastfed while employed or never breastfed because they planned to return to work.
Results:
81.0% of participants breastfed at least 4 months, and 69.8% breastfed for 6 months or greater. Participants who worked in the childcare sector had the highest breastfeeding rates at 4 (92.3%) and 6 months (80.0%) compared to other job sectors. Employees with greater levels of support in the workplace were more likely to breastfeed at 4 (p = .01) and 6 months (p = .02). Employees who were provided break times to pump had higher odds (odds ratio [OR] = 8.80, 95% CI: 1.90/40.68) of breastfeeding at 4 months. Additionally, having supportive coworkers and managers was associated with higher odds of breastfeeding at 4 months (OR = 7.55; 95% CI:1.58/36.07). Factors associated with having a manager supportive of employees’ breastfeeding included working in childcare (p = .009), having a higher education (p = .046), and having a written workplace breastfeeding policy (p = .04).
Conclusions:
Greater enforcement of breastfeeding policies, improved workplace accommodations, and enhanced support from managers and coworkers may improve breastfeeding rates in low-wage employees.
Keywords
Introduction
Exclusive breastfeeding is recommended for the first 6 months, followed by continued breastfeeding, with the addition of complementary foods, for at least 2 years (Meek et al., 2022). The U.S. Healthy People 2030 goal is for 54.1% of U.S. infants to be breastfed at least 12 months (Increase the proportion of infants who are breastfed at 1 year-Healthy People 2030, n.d.). For infants born in the United States in 2021, only 39.5% were breastfed at 12 months (CDC, 2024).
One of the barriers to prolonged breastfeeding is employment. Birth parents who are employed full-time are less likely to breastfeed at 6 and 12 months compared to those who are unemployed (Cunningham et al., 2024; Hamner et al., 2021; Mandal et al., 2010; Ryan et al., 2006). This negative association is particularly strong for low-income birth parents who return to work when their child is less than 3 months old (Hamner et al., 2021; Lubold, 2016).
Prior studies have found that barriers to breastfeeding in the workplace include lack of flexible schedules, lactation accommodations, breastfeeding policies, effective communication, and support from colleagues (Taylor et al., 2020). There are variable results regarding how manager/coworker support and lactation accommodations impact breastfeeding duration. While some studies have shown no significant association (Dagher et al., 2016; Hilliard, 2017; Scott et al., 2019), one study found an indirect positive association of workplace support on breastfeeding duration through improved breastfeeding self-efficacy (Wallenborn et al., 2019).
To improve support for breastfeeding employees, the 2010 Affordable Care Act (ACA) amended section 7 of the Fair Labor Standards Act to require covered employers to provide “reasonable break time for an employee to express breast milk for her nursing child for 1 year after the child’s birth.” Employers are also required to provide “a place, other than a bathroom, that is shielded from view and free from intrusion from coworkers and the public, which may be used by an employee to express breast milk” (H.R. 3590. Patient protection and Affordable Care Act, 2010). In 2022, the Providing Urgent Maternal Protections for Nursing Participants (PUMP) Act expanded employee protection to include lactating people working as teachers, nurses, agricultural workers, truck drivers, and part-time employees (H.R. 117-102. Providing Urgent Maternal Protections for Nursing Mothers Act, 2022). Employers with fewer than 50 employees who can demonstrate that this provision would cause an “undue hardship” may be exempt. Additionally, Washington, DC’s, the Child’s Right to Nurse Human Rights Amendment Act of 2007 (Bill B17-0133), requires that employers “provide reasonable daily unpaid break periods . . . so that the employee may express breast milk. . . . An employer shall make reasonable efforts to provide a sanitary room . . . where an employee can express her breast milk in privacy and security” (The child’s right to nurse human rights amendment act of 2007, 2007).
Despite enactment of these laws, U.S. breastfeeding employees, especially those working low-wage jobs, still experience workplace discrimination and lack of support (Mandal et al., 2010). Low-wage workers are half as likely as middle-income workers and one-third as likely as high-wage workers to receive reasonable break time and private space for pumping (Kozhimannil et al., 2016).
Although studies have evaluated employees’ breastfeeding experiences, few have focused on low-wage African American employees. Taylor’s 2020 systematic review of workplace lactation support concluded that “little research has been conducted that learns about the experiences of low-income and minority women with workplace lactation support” (Taylor et al., 2020). This study aimed to help fill that gap by surveying predominantly non-Hispanic Black, low-wage, employed mothers about their workplace support for breastfeeding.
Key Messages
The workplace experiences of non-Hispanic Black, low-wage, breastfeeding employees have not been well studied.
This study shows that non-Hispanic Black, low-wage employees were more likely to breastfeed if their managers and/or coworkers were supportive of breastfeeding, were provided adequate break times, and their workplace had a written breastfeeding policy.
The findings from this study are significant because they identify barriers to breastfeeding for non-Hispanic Black, low-wage employees and provide suggestions for ways to mitigate these barriers.
Objective
The objectives were to describe workplace breastfeeding experiences for low-wage employees in Washington, DC, and to identify workplace barriers and attributes associated with breastfeeding at 4 and 6 months.
Methods
We conducted a cross-sectional study. Data were collected between May 22, 2020, and May 11, 2022, in an academic hospital-based clinic and an affiliated community-based pediatric clinic in Washington, DC, during in-person and virtual medical clinic visits. The survey included closed- and open-ended questions modified from validated surveys (Olson and Fulmer, 2017; Ray & Rayens, 2024) or developed by three study team members, who are medical experts in lactation. Eligible participants had to be at least 18 years of age, speak English, have a child less than 3 years old who was receiving Medicaid benefits, and had been employed when their child was less than 1 year old. In addition, participants must have breastfed while employed, stopped breastfeeding prior to employment because of work, or never breastfed because of work. Exclusion criteria included a contraindication to breastfeeding (e.g., maternal HIV [considered a contraindication at the time of the survey], HTLV-1, street drug use, infant galactosemia). In addition, early in the COVID-19 pandemic (May 22, 2020, to March 15, 2021), participants were excluded if they or their child had COVID-19 symptoms to minimize exposure to the research team. We selected a target sample size of 100 because it allowed us to describe the breastfeeding experiences of low-wage workers and was feasible, given that we were recruiting during the pandemic. With this sample size, we had 80% power to detect an association of .2 between breastfeeding until 4 months and support in the workplace, with an alpha of .05.
A research team member prescreened potential participants for eligibility by reviewing the child’s medical record for Medicaid status and age. The research team member spoke with potentially eligible participants in a private examination room, described the study, and confirmed eligibility. Next, participants completed the informed consent process and were given the choice of having the survey questions read to them or completing the survey themselves via REDcap. The participants received a $10 incentive upon completion of the survey. This study was considered exempt by Children’s National Hospital IRB (IRB Pro00013413) and DC Health IRB (IRBPH # 2020-2).
Outcomes
The primary outcomes were breastfeeding or expressing and feeding human milk at 4 and 6 months.
Independent Variables
Independent variables included demographic characteristics (age, race/ethnicity, education) and occupation type. All independent variables were categorical (see Table 1).
Participants’ Demographic Characteristics and Distribution and Odds Ratios (OR) of Breastfeeding at 4 and 6 Months.
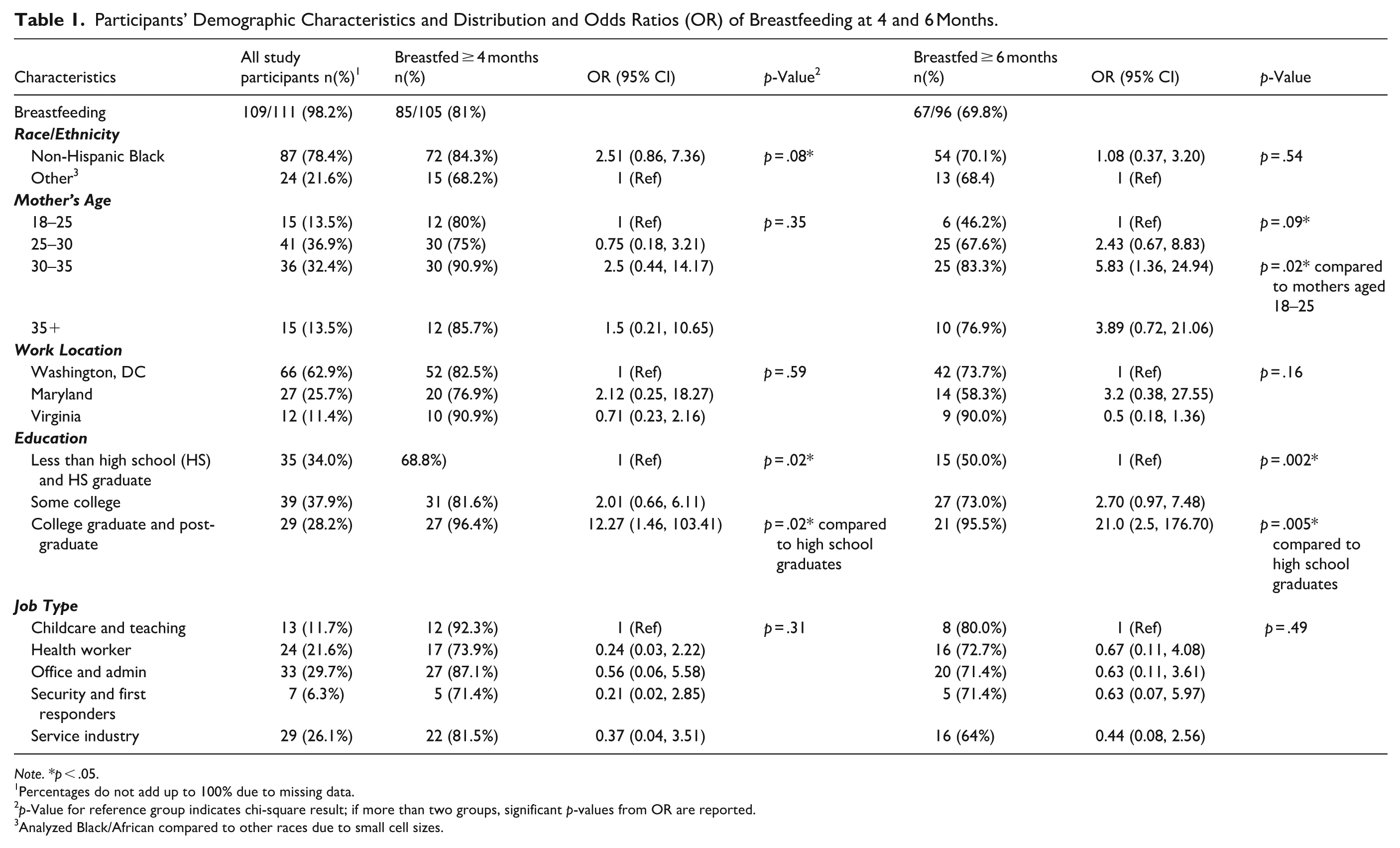
Note. *p < .05.
Percentages do not add up to 100% due to missing data.
p-Value for reference group indicates chi-square result; if more than two groups, significant p-values from OR are reported.
Analyzed Black/African compared to other races due to small cell sizes.
Participants were asked about seven workplace characteristics: 1) written policies for breastfeeding/pumping, 2) designated space for breastfeeding/pumping (other than a bathroom), 3) paid parental leave, 4) quality of space for breastfeeding/pumping, 5) adequate break times to pump, 6) support from managers, and 7) support from coworkers. Each characteristic was dichotomous (yes/no). A supportive work environment score was calculated by combining the responses to these seven questions to indicate an additive score of zero to seven, with zero indicating that the participant reported none of the previously listed supports (i.e., a nonsupportive work environment), and seven indicating that the participant had a highly supportive work environment.
Analytic Methods
Quantitative data analysis included descriptive analysis and bivariate analysis. Chi-square analysis and odds ratios were used to examine the association between breastfeeding at 4 and 6 months with each independent variable. Variables associated with breastfeeding duration in the bivariate analysis (p < 0.05) or found important in the literature were included in the final multivariable logistic regression models. Adjusted odds ratio (aOR) and 95% confidence intervals (CI) between determinants and breastfeeding outcomes are reported. Additionally, we ran a multivariable logistic regression model to identify variables associated with participants reporting that their manager supports breastfeeding/ pumping in the workplace. Chi-square tests were conducted for each workplace accommodation variable to better understand associations with breastfeeding duration. Qualitative data analysis was used to contextualize the quantitative findings. Responses to the open-ended questions were inductively coded and grouped into overarching themes.
Results
Demographics
Study team members invited 113 eligible birth parents to participate in the study. Two parents refused to participate, and 111 participants completed the survey. Of those participants with infants ≥4 months (n = 105), 81.0% breastfed 4 months or longer, and 69.8% of infants ≥6 months (n = 96) breastfed for at least 6 months (Table 1). Most study participants were between 25–35 years old (n = 77, 69.3%) and were non-Hispanic Black or African American (n = 87, 78.4%). Approximately one-quarter (n = 29, 26.1%) had a college degree. Participants primarily worked in administrative or office jobs (n = 33, 29.7%), followed by the service industry (restaurant, retail, fast food, etc.) (n = 29, 26.1%), and health care (n = 24, 21.6%) (Table 1).
Two (1.8%) participants indicated that they never breastfed because of employment, and 21 (18.9%) stopped breastfeeding before returning to work because of employment. Additional reasons participants stopped breastfeeding before returning to work included perceived insufficient milk (42.9%), pain (14.3%), poor latch (14.3%), and not receiving breastfeeding help (14.3%).
Of the 88 participants who breastfed when they returned to work, 48 (54.5%) exclusively breastfed/pumped. Participants reported returning to the workplace after having their child in the following timeframes (n = 107 responses): (1) <4 weeks (n = 5, 4.7%); (2) 4 to 8 weeks (n = 16, 15.0%); (3) 8 to 12 weeks (n = 27, 25.2%); and (4) more than 12 weeks (n = 59, 55.1%). Most participants (n = 74, 69.2%) were employed 30 or more hours per week.
Participants with higher education had greater odds of breastfeeding until 4 or 6 months (Table 1). Participants aged 30–35 years had the highest odds of breastfeeding and 5.83 times higher odds (95% CI: 1.36/24.94) of breastfeeding at 6 months compared to those aged 18–25 (Table 1). Participants who worked in the childcare sector had the highest breastfeeding rates at 4 (92.3%) and 6 months (80.0%). Employees who were security workers or first responders had the lowest breastfeeding rates at 4 months (71.4%), and employees in the service industry had the lowest breastfeeding rates at 6 months (64.0%) (Table 1).
Workplace Accommodations
Only 22.4% (n = 24) of participants responded that they received paid parental leave, 19.8% (n = 21) had written workplace policies for breastfeeding/ pumping, and less than half reported adequate break times to pump (n = 48, 44.9%). One-third of participants said their workplace had a designated space (other than a bathroom) for pumping (n = 34, 32.4%). Of those who did have a designated space, less than half said the space was in excellent or good condition (n = 14, 42.4%). A statistically significant association was found between having adequate break times for pumping and breastfeeding at 4 (OR = 8.80, 95% CI: 1.90/40.68, p < 0.001) and 6 months (OR = 3.04, 95% CI: 1.13/8.14, p < .02) (Table 2).
Reasonable Breaks, Accommodations, and Support in the Workplace and Breastfeeding at 4 and 6 Months.
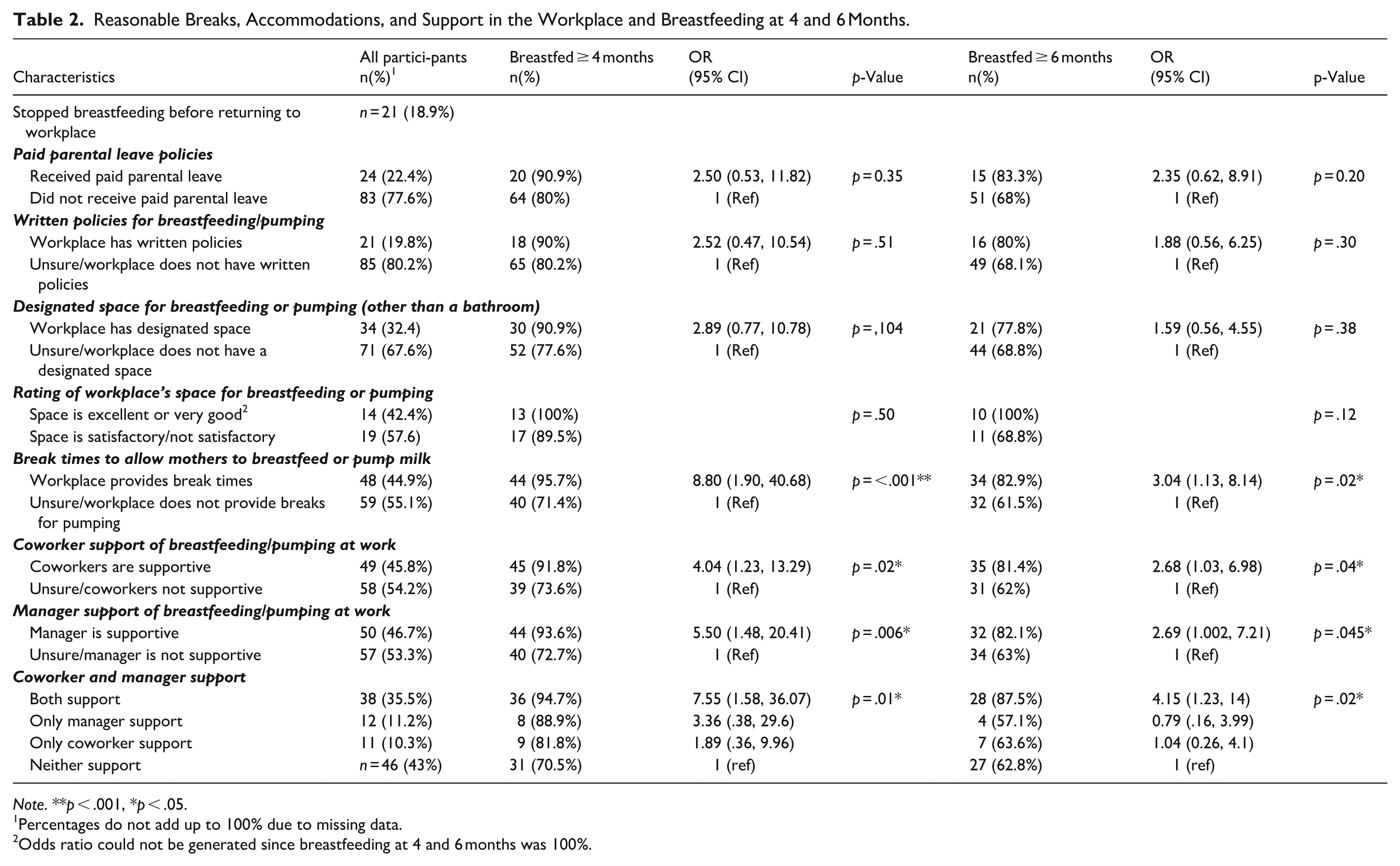
Note. **p < .001, *p < .05.
Percentages do not add up to 100% due to missing data.
Odds ratio could not be generated since breastfeeding at 4 and 6 months was 100%.
Predictors of Breastfeeding at 4 and 6 Months
After adjusting for age of the birth parent, race/ ethnicity, education, and job type, the odds of breastfeeding increased by 78% for every 1-point increase in the supportive work environment score at 4 months (aOR = 1.78, 95% CI: 1.14/2.79) and by 51% at 6 months (aOR = 1.51, 95% CI: 1.06/2.16). Additionally, participants with a college degree had significantly greater odds of breastfeeding at 6 months compared to those without a college degree (aOR = 15.04, 95% CI: 1.44/156.93) (Table 3).
Multiple Logistic Regression Analysis of Maternal Characteristics and Breastfeeding at 4 and 6 Months.
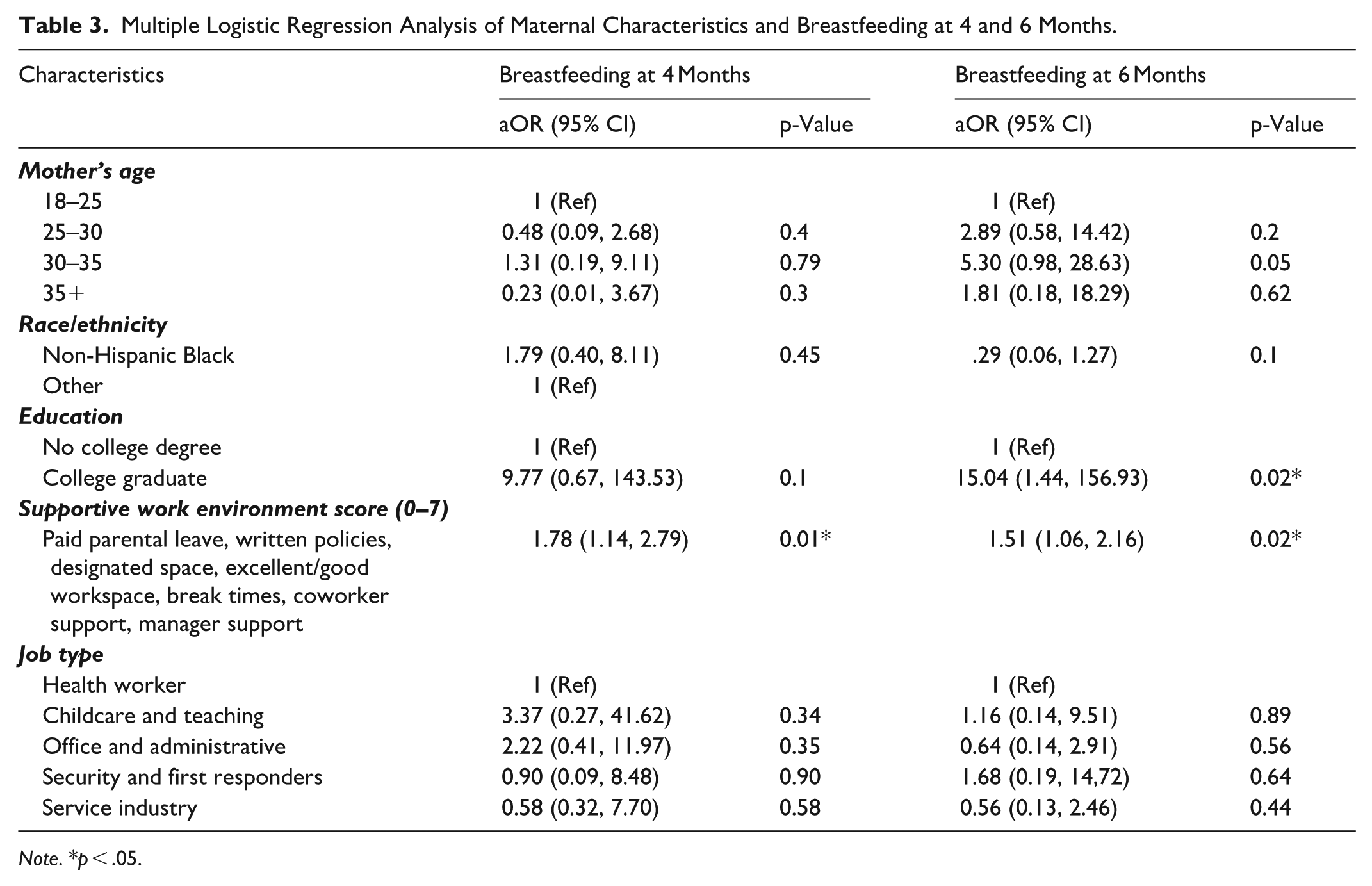
Note. *p < .05.
Coworker Support
Nearly half (n = 49, 45.8%) of participants reported having supportive coworkers. These employees had significantly greater odds of breastfeeding until 4 months (OR = 4.04, 95% CI: 1.23/13.29) and 6 months (OR = 2.68, 95% CI: 1.03/6.98) compared to those with unsupportive coworkers (Table 2).
Participants with supportive coworkers (n = 49) reported that they felt their coworkers would cover their job duties (n = 36; 73.5%) or change their break times (n = 21; 42.9%) to allow the participant to pump/breastfeed. Thirty-four participants (69.4%) responded that their coworkers said positive comments about breastfeeding, such as “That’s great that you’re still breastfeeding,” “Breastfeeding is so natural and wonderful,” “I know it’s hard to pump. It’s another job you’re doing. I fully support you,” and “Let me know when you go, so I can cover you.”
Of the 58 (54.2%) participants with either unsupportive coworkers or who were unsure if their coworkers were supportive, six (10.3%) commented that their coworkers would think less of them, and 11 (19.0%) would be embarrassed if they breastfed. Ten coworkers (17.2%) made unsupportive comments, including “Breastfeeding moms work less,” “Children over a certain age shouldn’t be breastfed,” and “Why are you taking so long?”
Manager Support
About half of participants reported they had supportive managers (n = 50, 46.7%). Participants with supportive managers had 5.50 greater odds (95% CI: 1.48/20.41) of breastfeeding until 4 months, and 2.69 greater odds (95% CI: 1.002/7.21) of breastfeeding until 6 months compared to those with unsupportive managers. Twenty-four (48%) of these employees responded that their managers would adjust their hours, 30 (70.0%) cover their job duties so they could pump, and 29 (58.0%) made supportive comments, such as “Breast is best,” “We support you,” “I know you need to pump, so you can use my office space to do so,” “Pump as often as you need to, there is no time limit,” and “I’m proud that you are breastfeeding.”
Participants who reported that their managers were either unsupportive or unsure if their manager was supportive said they thought their job would be at risk if they breastfed (n = 10,17.5%) or their manager would think less of them (n = 8,14%). Twelve (21.1%) said their manager made unsupportive comments (n = 12, 21.1%), such as “Go pump in the bathroom or your car,” “You’re pumping again?” “One year policy,” “You can’t do it in areas like break rooms,” and “It is not appropriate to have certain parts of your body exposed in the break room,” or suggested “to give my baby formula.”
Fifty participants (49.0%) felt comfortable asking their manager for breastfeeding accommodations. Employees with female managers felt more comfortable asking for accommodations (n = 33, 66.0%) compared to those with male managers (n = 17, 34.0%). Approximately one-third of participants (n = 38, 35.5%) indicated they had support from both their coworkers and manager, all but two of them breastfed until at least 4 months (n = 36, 94.7%), and 87.5% (n = 28) breastfed 6 months or longer.
After adjusting for education, race/ethnicity, age, written workplace policies, and manager’s gender, respondents who worked in childcare and teaching had significantly higher odds (aOR = 9.55, 95% CI: 1.74/52.31, p = .009) of reporting a supportive manager compared to those who worked in health care (Table 4). Additionally, participants who had written workplace breastfeeding policies (aOR = 3.43, 95: CI: 1.05/11.24, p = .04) or were college graduates (aOR = 3.18, 95% CI: 1.02/9.91, p = .046) were more likely to report supportive managers. There was no significant association between the manager’s gender, the respondent’s age or race/ethnicity, and having a supportive manager.
Multiple Logistic Regression Analysis of Manager Support.
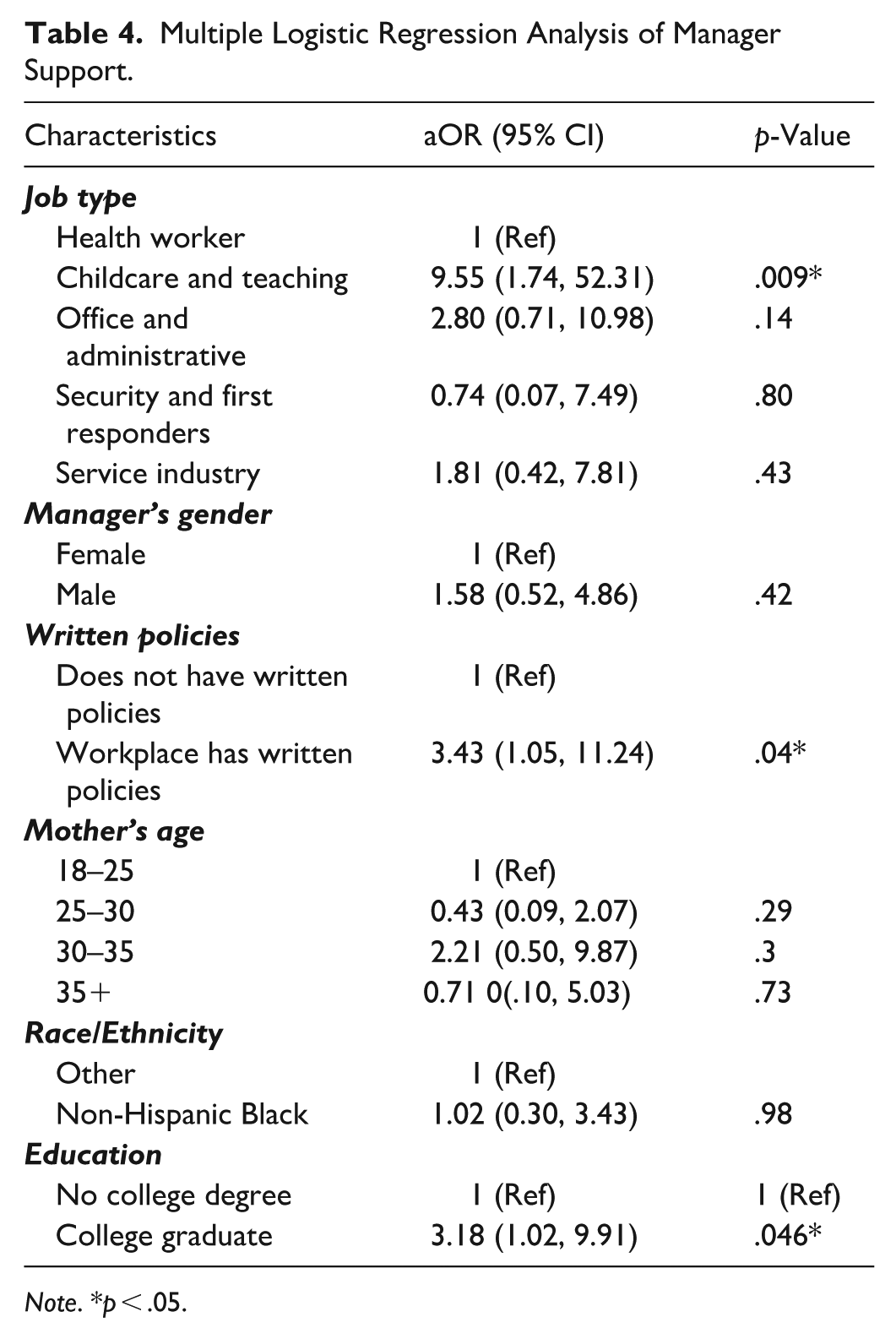
Note. *p < .05.
Overall Experience About Breastfeeding While Employed (Qualitative Feedback)
When asked what factors made it easier to pump in the workplace, 52 participants provided open-ended responses, and the top three themes identified related to: 1) breaks and flexibility to pump (n = 17), 2) private and/or designated space to pump (n = 17), and 3) adequate support from coworkers and managers (n = 17). One mother said, “I had my own space . . . I wasn't pressured to finish at a certain time.” Another participant stressed the importance of social support, saying, “Having the proper support staff [helped make pumping in the workplace easier].” Several participants (n = 6) also mentioned that having adequate supplies and resources, such as a wireless pump and a kitchen with a sink and refrigerator, made pumping in the workplace simpler. Three participants had jobs close to home or the baby’s childcare and breastfed during breaks.
When asked what made breastfeeding/pumping in the workplace more challenging, nearly half of the 58 respondents indicated they did not have a private and/or designated place to pump (n = 27). Five participants complained of having to pump in an unsanitary bathroom. Thirteen participants indicated a lack of breaks and having an unsupportive manager or coworker as barriers. One participant intended to breastfeed for 1 year but stopped breastfeeding 2 weeks after she returned to work because of breast pain from not being able to pump at work. Eight participants said the nature of their job made it challenging to pump in the workplace. One mother said, “I often have back-to-back clients and notes to finish, so after the first week back, I couldn't pump at work anymore.” Several participants (n = 11) mentioned they were unaware of state or federal laws mandating employers provide space and time to pump.
Discussion
This study evaluated the experiences of low-wage, predominantly non-Hispanic Black breastfeeding employees, a group that has largely been understudied. We found that employees were more likely to breastfeed at 4 and 6 months if they reported having supportive coworkers and/or managers, adequate break times, and/or a written breastfeeding policy. In our study, having a supportive manager was significantly associated with breastfeeding for a longer duration. Some studies have reported similar findings, while others have reported no association between workplace support and breastfeeding duration (Dabritz et al., 2009; Scott et al., 2019; Taylor et al., 2020). Two systematic literature reviews cited articles demonstrating an association between employees’ breastfeeding duration and the employer providing time and space to express milk (Cunningham et al., 2024; Scott et al., 2019). Most of these articles were either conducted outside the United States or studied high-wage earners, military personnel, or adolescents. Outcome measures included job satisfaction, self-efficacy, and obesity but not duration as an independent variable (Reifsnider et al., 2018; Spitzmueller et al., 2016; Whipps & Honoroff, 2019; Whitley et al., 2019).
A few articles are more closely aligned with our study. A study using semi-structured interviews of 24 African American participants in Washington, DC’s, Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) program evaluated workplace support for human milk feeding. Lactation accommodations and employer support were highly variable, and environments conducive to pumping influenced some participants’ feeding decisions or breastfeeding duration (Schindler-Ruwisch et al., 2020). A prospective study of a racially diverse population found that women who exclusively breastfed were more likely to report a supportive work environment with space and time to express milk (Howard et al., 2022). Two studies found that women were more likely to breastfeed if their workplace was flexible (Guendelman et al., 2009; Hardison-Moody et al., 2018). One study found employees with both adequate break time and private space to pump had 2.3 times greater odds (95% CI 1.03, 4.95) to exclusively breastfeed until 6 months (Kozhimannil et al., 2016). A study of 500 predominantly White and married employees found that female coworker support positively affected mothers’ decisions to continue breastfeeding (Zhuang et al., 2019).
Our study is one of the few to evaluate the association between workplace support and breastfeeding duration in the United States, specifically among non-Hispanic Black, low-wage workers.
These employees face a unique combination of barriers, including implicit bias; structural, systemic, and medical racism that has led to inequities in educational opportunities; higher rates of employment in low-wage, less flexible positions; and shorter parental leave than White employees (Labor Force Characteristics by Race and Ethnicity, 2023, 2024). These factors contribute to non-Hispanic Black women having the lowest breastfeeding rates nationally. The results from this study identify an opportunity to help remedy these breastfeeding disparities through the enforcement of workplace accommodation laws and educating employers about the importance of creating supportive workplace environments.
In our study, employees working in healthcare or security had the lowest breastfeeding rates at 4 months. Although studies have shown variability in breastfeeding rates among high-wage healthcare workers (e.g., physicians) based on level of training and specialty type, high-wage healthcare workers generally have high rates of breastfeeding initiation and duration (Alvarez et al., 2015; Gasior et al., 2024; Gupta et al., 2019; McDonald et al., 2021). It is hypocritical that low-wage health care workers in our study experienced the least supportive environments, given that all major medical groups encourage providers to support breastfeeding in their patients. It is crucial that healthcare leaders extend this same support to all their employees, regardless of income or status.
About half of the participants (45%) in our study returned to work less than 12 weeks postpartum. Participants who returned to work earlier had a shorter breastfeeding duration compared to those who returned later. This aligns with a U.S. national study showing that states with paid family leave policies have higher rates of any and exclusive breastfeeding than states without these policies and substantiates the need for a national paid parental leave policy (Rosenberg et al., 2024).
Participants who said that returning to work was one of the reasons they stopped breastfeeding identified perceived insufficient milk, breastfeeding pain, and not receiving help with breastfeeding as additional reasons they stopped breastfeeding. These are the most common reasons women stop breastfeeding (Hornsby et al., 2019) and underscore the need for healthcare, lactation, and WIC providers to address these common barriers. This also illustrates the importance of supporting evidence-proven education and support initiatives for breastfeeding parents, such as baby-friendly hospitals and WIC peer counselors.
Unfortunately, only a minority of employees in this study reported that their workplaces complied with the legal requirement of giving space and time for employees to express their milk. A national study of employees who gave birth between 2011 and 2012 found that 40% of their workplaces provided both break time and a private space to pump (Kozhimannil et al., 2016). These authors could not find recent, unbiased, peer-reviewed national data about U.S. workplace compliance with the ACA and PUMP Act, which calls attention to the need for structured documentation of workplace adherence to these laws.
Limitations
Our selection criteria resulted in higher rates of breastfeeding than previously reported in low-wage, non-Hispanic Black employees. This study had a small sample size and study location and may not represent low-wage workers’ experiences nationally. However, the sample size was larger than many studies on this topic and offers important insights into the experiences of low-wage, non-Hispanic Black workers in the Washington, DC, area. In addition, while there was no comparison group with higher-income employees, it is possible to compare the experiences with those of higher-wage workers who are overrepresented in peer-reviewed literature. Although our study is not prospective, research has shown that breastfeeding duration recall may be accurate for 6 years after delivery (Amissah et al., 2017). The study was conducted prior to instituting Washington, DC’s, paid parental leave law in 2020, which could have affected the duration of maternal leave and breastfeeding outcomes.
Conclusion
This original research study is one of a few studies that have evaluated workplace support of breastfeeding low-wage earners among mostly non-Hispanic Black employees. Results from this study indicate that employees were more likely to breastfeed if their managers and/or coworkers were supportive of breastfeeding, were provided adequate break times, and their workplace had a written breastfeeding policy. Educating staff about the importance of supportive work environments, encouraging the development and distribution of breastfeeding policy, and increasing oversight and enforcement of breastfeeding laws could improve workplace support and lead to longer breastfeeding duration among low-wage, non-Hispanic Black employees.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344261452634 – Supplemental material for Barriers and Facilitators for Breastfeeding Among Low-Wage Employees in the Washington, DC, Area
Supplemental material, sj-docx-1-jhl-10.1177_08903344261452634 for Barriers and Facilitators for Breastfeeding Among Low-Wage Employees in the Washington, DC, Area by Jennifer AF Tender, Elaine Cooper Russell, Janay Ezekwe, Kathleen Logan and Amira A Roess in Journal of Human Lactation
Footnotes
Acknowledgements
The authors thank Sahira Long, MD, IBCLC, for her assistance with the study design, and also the participants for sharing their experiences.
Author Note
Elaine Cooper Russell was a PhD student supervised by Amira Roess, PhD, MPH, when writing this manuscript.
Ethical Considerations
This study was considered exempt by Children’s National Hospital IRB (IRB Pro00013413) and DC Health IRB (IRBPH # 2020-2). All participant information was de-identified.
Consent to Participate
Participants received an information sheet, but participant consent was not required.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DC Department of Health (DC Health).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trial Registration
There were no trial registration or grant numbers.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.