
Abstract
Breastfeeding is one of the most cost-effective health interventions in existence, improving child survival through improved health and nutritional status and providing numerous benefits to the mother, including lowering the risk of breast, ovarian, and endometrial cancer. Current WHO guidelines recommend exclusive breastfeeding (EBF) for the first 6 months of an infant’s life, which Ministries of Health across Southern Africa support. However, rates of EBF in this region, particularly Sub-Saharan Africa, vary widely and fail to reach global targets. Botswana and South Africa offer specific examples of this variation. Need to return to work has been highlighted as a significant barrier to sustained EBF among women who initiate EBF. Broader workplace structures and expectations for women hinder EBF, particularly in Southern Africa. The informal sector, which employs the majority of women in Southern Africa, often lacks labor protections and social benefits. Conditions within the workplace or at school are also not conducive to the specific demands of EBF, without dedicated space to express milk, facilities to safely store breastmilk, or protected time for breastmilk expression. Guidelines around how best to support breastfeeding women vary widely, and few lay out specific strategies to support EBF in the workplace. Women, regardless of where they live, deserve the choice to elect EBF for their infant. Persistent barriers to EBF prevent postpartum women and their infants, particularly in Southern Africa, from realizing its countless benefits.

Keywords
Background
Exclusive breastfeeding (EBF) could prevent over 800,000 childhood deaths annually (Victora et al., 2016). Breastfeeding also offers maternal health benefits with a recent study noting that scaling EBF to 90% could prevent over 72,000 female deaths later in life from noncommunicable diseases, including cancer, hypertension, and diabetes (Bhandari et al., 2025). Ministries of Health across Southern Africa support the current WHO recommendation of six months of EBF (Government Ministries and UN Agencies Launch National Breastfeeding Promotion Campaign, 2023; World Health Organization, 2013). Rates of EBF vary from 31% to 59% in 2017 to 2023 across Southern Africa (United Nations Children’s Fund, Division of Data, Analysis, Planning and Monitoring, 2024). The need to return to work has been identified as a significant barrier to sustained EBF among women who initiate EBF, highlighting the need for greater attention to breastfeeding support among working mothers in these settings (Dutheil et al., 2021; Horwood et al., 2020, 2021; Luthuli et al., 2020; Mahgoub et al., 2002; Seabela et al., 2023).
Importantly, one breastfeeding related challenge unique to Southern Africa is the high prevalence of HIV, of which Southern Africa is the global HIV epicenter. Current guidelines for women living with HIV encourage breastfeeding in conjunction with continued use of antiretroviral treatment to achieve and maintain sustained HIV viral suppression (World Health Organization, 2021). Breastfeeding has more recently been promoted as a choice for women living with HIV in the US and Europe who are on a treatment regimen with an undetectable HIV viral load (European AIDS Clinical Society, 2023; HHS Panel on Treatment of HIV During Pregnancy and Prevention of Perinatal Transmission National Institutes of Health, 2024).
Here we examine breastfeeding rates and the disconnect between intention and actual practice of exclusive breastfeeding in two Southern African countries: Botswana and South Africa. Both Botswana and South Africa are upper-middle income countries in Southern Africa that have navigated complex breastfeeding policies, sharing similarities in structural workplace barriers while maintaining distinct policy histories and national breastfeeding rates. While the focus of this paper is on two representative countries in Southern Africa, it is notable that some women in the United States face similar issues to those we describe here. For example, women from low-income, racial and/or ethnic minority backgrounds in the United States have reported returning to work often within 2–6 weeks of birth due to financial barriers and lacking access to private pumping spaces and refrigeration, precluding continuation of EBF (Office of the Surgeon General [US] et al., 2011).
Up to 40% of women in Botswana may initiate breastfeeding (World Breastfeeding Trends Initiative (WBTi), 2025a), only 20% of which will engage in EBF through six months. Previous research has shown that many women in Botswana plan to breastfeed for 18 months or more; however, income generating commitments outside of the home lead to the early termination of exclusive breastfeeding (Mahgoub et al., 2002). Nearly 80% of women in South Africa initiate breastfeeding, of which only 8% will continue through six months (World Breastfeeding Trends Initiative (WBTi), 2025b); the majority of women cannot continue because of the need to return to work (Maponya et al., 2021). This is highlighted by a mixed-method study in South Africa that revealed that women earning less than $175/month returned to work within two weeks postpartum due to financial strain, despite their desire to take maternity leave and engage in EBF (Luthuli et al., 2020). Another mixed-method study included a longitudinal cohort of 24 women working in the informal sector (e.g., domestic workers) in South Africa, 18 participants of which returned to work following giving birth. Three were back within two weeks, and one even earlier than two weeks, due to financial pressures (Horwood et al., 2021). Only one participant managed to continue expressing breastmilk after returning to work.
Key Messages
Current WHO guidelines recommend exclusive breastfeeding (EBF) for the first six months of an infant’s life, which Ministries of Health across Southern Africa support.
Rates of EBF in Southern Africa vary widely and fail to reach global targets.
The return to work represents a significant barrier to exclusive breastfeeding through six months.
Guidelines around how best to support breastfeeding women who return to work vary widely, and protections may be unevenly implemented.
Breastfeeding Policy and Need for Innovation
Workplace leave policies and breastfeeding protections do not support the majority of women (Horwood et al., 2020; Mgongo et al., 2024; Remmert et al., 2020; Seabela et al., 2023). While the Basic Conditions of Employment Act mandates four months of maternity leave in South Africa, employers are not obligated to pay employees during this period (Claassen, n.d.; Department of Health [South Africa], 2014). In South Africa, employees who have been contributing to the Unemployment Insurance Fund (UIF) can claim maternity benefits (Maternity Leave in South Africa, n.d.), but this is typically not the case for workers in the informal sector (e.g., street vendors, domestic workers, farmers). In South Africa, an estimated 42% of women run unregistered, informal businesses (South African Department of Statistics, 2023), while in Botswana, over 72% of women are employed informally (International Labour Organization, 2024). Under Botswana law, women are entitled to 12 weeks of maternity leave. However, the maternity pay does not meet international guidelines around what is required to cover basic cost-of-living expenses (Botswana, n.d.).
Women face additional barriers upon the return to work. The South African Department of Health (DOH) published guidelines in 2019 to support breastfeeding in the workplace, including a workplace policy template, safety requirements for breastfeeding spaces at work, and sample breastfeeding schedules for working mothers. The Basic Conditions of Employment Act in both countries mandates paid breastfeeding or expressing breaks (e.g., two 30-minute breaks) for breastfeeding mothers for up to six months after return to work (Claassen, n.d.; Code of Good Practice on the Protection of Employees During Pregnancy and After the Birth of a Child, 1998; Department of Health (South Africa), 2014; Parliament of Botswana, 1982). However, formal guidelines are geared toward formal sector workplaces (e.g., government, corporate, institutions of higher education), and the South African DOH does not enforce these policies in either the private or public sector (Maponya et al., 2021; South Africa Department of Health, 2019). Little is published on the adherence to and effectiveness of workplace policies, and how this may contribute to lower-than-expected increases in EBF rates (Miatton et al., 2025). The International Labor Organization estimates that only 20% of all countries meet adequate standards for breastfeeding or expressing breaks and breastfeeding facilities (Global Breastfeeding Collective et al., 2025). It is projected that only 6 of 94 low- and middle-income countries will meet World Health Organization’s Global Nutrition Target for breastfeeding by 2030 (Bhattacharjee et al., 2021). There is no country-specific evaluation of the efficacy of current policies, preventing effective revisions to better support EBF in either South Africa or Botswana.
In addition, many women are not aware of their rights, and employers often do not provide adequate breastfeeding-friendly facilities (Martin-Wiesner, 2018). Only 18.3% of domestic workers (n=2,625) surveyed in Western Cape, South Africa, believed they were entitled to daily breastfeeding or expressing breaks; 10.6% thought they would not receive any maternity protection benefits (Pereira-Kotze et al., 2023). The few studies conducted among working mothers in Southern Africa highlight that, along with pressure to return quickly, fear of job loss due to frequent breaks to express milk, absence of onsite childcare, and lack of private, sanitary spaces at work, particularly in the informal sector, and cultural stigma against public breastfeeding all prevent women from achieving to EBF goals (Balogun et al., 2015; Farista & Jaga, 2024; Horwood et al., 2020; Luthuli et al., 2020; Seabela et al., 2023). In 2022 the Child, Youth and School Health Cluster of the South African DOH, with support from the WHO and United Nations Children’s Fund, identified revitalization strategies to reimplement the Mother-Baby Friendly Initiative (MBFI), initially implemented in 2003 in South Africa. The MBFI has been shown to significantly increase the early initiation of breastfeeding, but has been unsuccessful in overcoming barriers to EBF encountered upon the return to work (Lubbe et al., 2024; Martin-Wiesner, 2018).
Better support for milk expression is one way to support continued breastfeeding for women who need to return to work in Botswana and South Africa. In an effort to bolster EBF among working mothers, the South African DOH recommends hand expression of milk when women are separated from their infants (South Africa Department of Health, 2007), while the Botswana Ministry of Health encourages working mothers to express milk at night to be used by caretakers during the day (Lubbe et al., 2024; Martin-Wiesner, 2018; Ministry of Health [Botswana], 2012). However, hand-expression of breastmilk can be labor-intensive and uncomfortable, and may fail to produce an adequate milk supply for some, particularly those with older babies or those who cannot express with regular frequency (Tonya et al., 2023; Chen et al., 2023). Breast pumps are not universally available, and data on the feasibility and acceptability of breast pumps among women in Botswana and South Africa, and more broadly in Southern Africa is lacking (Tonya et al., 2023). Also lacking are data on strategies to overcome barriers to safe milk storage. Those who are able to express breastmilk must often address lack of appropriate sanitation and refrigeration conditions to safely store expressed breastmilk both at home and in the workplace (Horwood et al., 2020). The majority of workplaces in Botswana and South Africa also lack requisite minimal conditions to promote continued expression of breast milk, specifically clean private spaces, refrigeration, and hand-washing facilities (Mabaso et al., 2020; Maponya et al., 2021).
Caregivers play an important role in infant feeding once a mother returns to work. Caregivers must be comfortable in the handling of expressed breastmilk and have knowledge of safe milk storage and an understanding of EBF’s importance (Muleka et al., 2023); A 2023 survey of caregivers found that over 40% did not know that EBF should be sustained for 6 months (Muleka et al., 2023; National Academies of Sciences et al., 2025). Supporting a mother’s desire to continue breastfeeding her infant after return to work requires training household caregivers in labeling and storage of expressed milk, and education campaigns to increase comfort with handling milk (Maponya et al., 2021; Muleka et al., 2023). Few studies have evaluated how to best support caregivers in these contexts, though one approach that may have a positive impact would include the involvement of caregivers in pre- and post-natal clinic visits to capacitate caregivers to successfully support breastfeeding (Seabela et al., 2023).
Conclusion
Successful EBF for an infant’s first six months of life is suboptimal among mother-child dyads in Botswana and South Africa who may benefit from the health benefits most. Despite clear and evidence-based global guidelines, implementation is poor. Multiple reports have estimated an increase to possibly 32% of EBF by 2016 after the 2010–2011 Tshwane Declaration in South Africa promoting EBF for the first six months, while after similar policy changes in 2016, Botswana has seen an increase in EBF (0–5 months) to around 30% according to recent UNICEF reports. These estimates remain far below global targets of 50% (Global Breastfeeding Collective et al., 2025). An absence of routine monitoring systems for tracking implementation and compliance with breastfeeding-friendly policies and workplace protections makes it difficult to evaluate the magnitude of challenges experienced by women who wish to have their infant continue to receive breastmilk exclusively through six months of life (Martin-Wiesner, 2018).
Where countries have introduced policies to promote breastfeeding in the workplace, these policies are particularly non-enforceable in informal workplace settings, settings that employ a disproportionately high number of women with newborns in places such as Botswana and South Africa. To overcome these challenges, data must be collected from all persons involved in the infant feeding cascade. Currently, there is a lack of sufficient data from women, caretakers, or employers to understand approaches to increase the prevalence of EBF for a full six months, particularly when a woman who is breastfeeding must return to work.
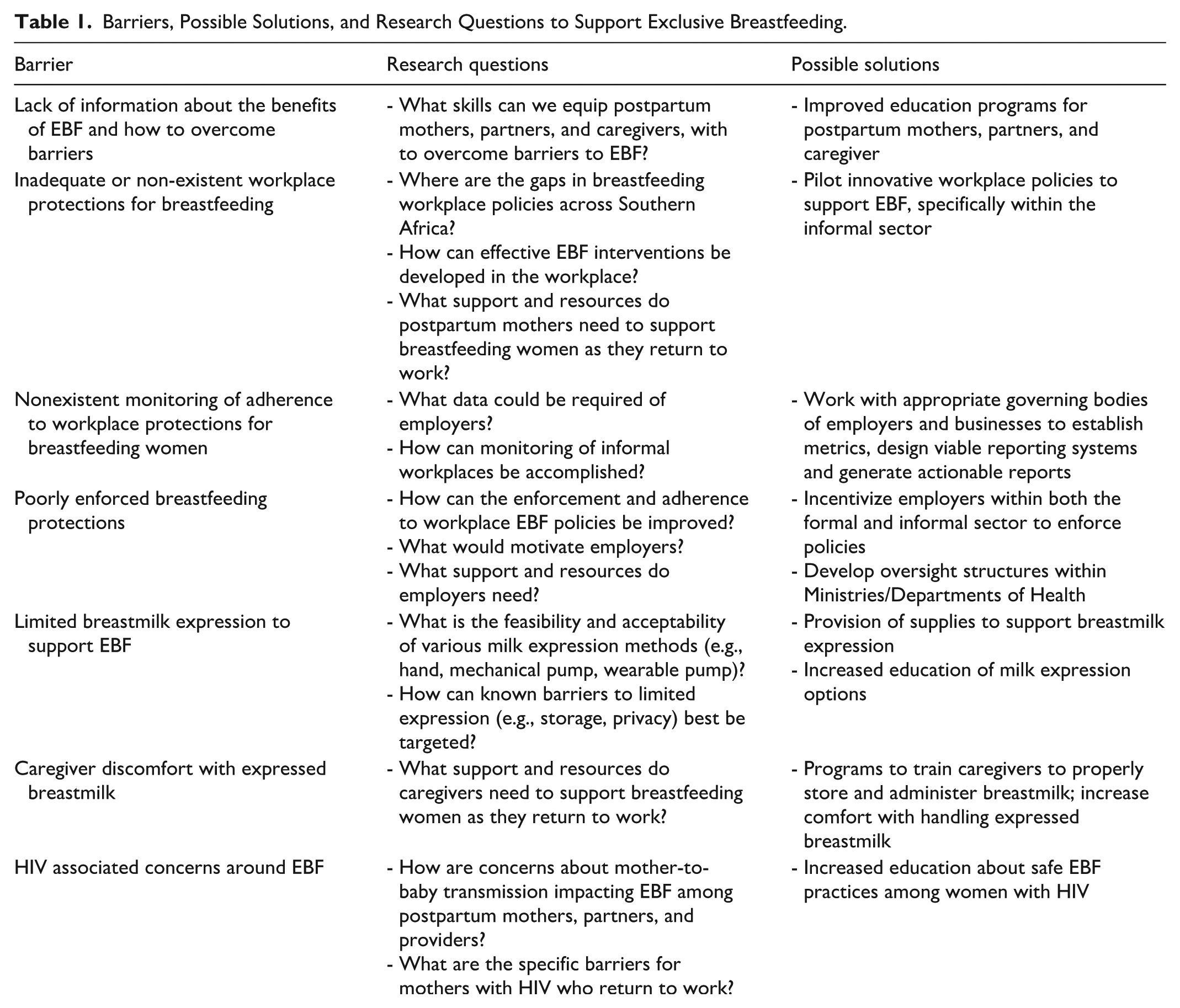
While barriers to safe and effective milk expression exist, many could be overcome with targeted efforts and improved infrastructure that incorporate input from mothers, businesses, and governing bodies (World Alliance for Breastfeeding Action, 2022; Table 1). Research is urgently needed to identify acceptable approaches to support EBF, particularly for women who must or choose to return to work. Optimal approaches identified through research require implementation of disaggregated metrics to measure success and/or identify further opportunities. Women, regardless of where they live, need and deserve the choice to choose EBF. Persistent barriers to EBF prevent postpartum women and their infants, particularly in Southern Africa, from realizing its countless benefits.
Barriers, Possible Solutions, and Research Questions to Support Exclusive Breastfeeding.
Footnotes
ORCID iDs
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christina Psaros is the President and Co-Founder of EQUILACT, Inc. Kathleen Powis and Sara R. Schenkel are Co-Founders of EQUILACT, Inc. EQUILACT, Inc. is a 501c organization whose mission is to break down barriers to breastfeeding among persons in resource-constrained settings. Christina Psaros has grant funding from Gilead Sciences that is unrelated to this manuscript.