
Abstract
Background:
Breast milk is the gold standard of infant nutrition, providing powerful nutritional and immunological protection and decreased mortality due to infection. The World Health Organization recommends using human breast milk from a milk bank if the mother is unable to provide for her own child.
Aim:
To determine the knowledge and acceptance of donor human milk use among women attending the Haydom Lutheran Hospital in Tanzania.
Methods:
An analytical cross-sectional study collected data at the Reproductive and Child Health Care, Neonatal Care units and postnatal ward at Haydom Lutheran Hospital. A total of 260 mothers aged ≥ 18 were included in the study.
Results:
In all, 86% of participants were unaware of human milk banks, 75% had limited knowledge of them, and 67% were willing to donate milk. Fear of having insufficient milk for their infants was the main reason for not donating. A total of 61% would use donated milk. Infectious diseases were the main reason for not using donated milk. In all, 89% who agreed to use donated milk were willing to donate and 67% of those who opposed using donated milk were unwilling to donate. Level of education was associated with willingness to donate (AOR 4.79, 95% CI [1.3, 17.6], p = 0.018) and receive donated breast milk (AOR 6.01. 95% CI [1.6, 23.2], p < 0.01).
Conclusion:
We found high potential acceptability for donating and using human donor milk for infants, with the only association being the level of education. However, further engagement is needed to foster awareness of its importance for communities while addressing cultural, religious, and health concerns.
Key Messages
Before this study, there was no data on whether women attending Haydom Lutheran Hospital knew about human milk banks and their acceptability.
Although the majority had no previous knowledge of human milk banks, more than half were open to the idea of donating their own human milk.
Infectious disease and lack of human milk for their own children were significant concerns for opposing using or donating donated human milk.
A potentially high acceptability was found in the community, with targets for further community engagement to foster awareness.
Introduction
Breast milk is the gold standard for infant nutrition, offering essential nutrients and strong immune protection against gastrointestinal infections, while significantly lowering infant mortality (World Health Organization [WHO], 2023). Exclusive breastfeeding is recommended for the first 6 months of life, and when a mother’s own milk is unavailable, donor human milk (DHM) serves as the preferred substitute (Goodfellow et al., 2016; WHO, 2011, 2023). Previous studies have shown that improving breastfeeding behavior would save 823,000 infants annually, with 87% of those being infants under 6 months old (Victora et al., 2016; Walters et al., 2019).
DHM is donated by mothers and processed by the milk bank to be used by the recipient baby who cannot get it from their own mother (Hoodbhoy, 2013). Human milk banks (HMB) systematically collect, pasteurize, store, and distribute donated human breastmilk (Hoodbhoy, 2013). There are 750 HMBs in 66 countries, and more than 800,000 infants receive donor human milk annually, suggesting that over 1 million liters of milk are donated annually in support of optimal infant nutrition and breastfeeding. In South Africa alone, there are 70 hospitals with HMB services (Bhoola & Biggs, 2021; European Milk Bank Association, 2021).
However, due to a lack of knowledge on the importance of DHM, most mothers prefer infant formula over it (Alemu et al., 2021; Yang et al., 2020). Neonates, especially those who are premature and low birth weight, are more susceptible to morbidity and mortality, especially those who do not receive breast milk in the early days (Iloh et al., 2018; United Nations Children’s Fund [UNICEF], 2006). In low-income countries such as Tanzania, neonatal mortality contributes to 40% of under-five deaths (WHO, 2022b).
As an example, neonates who received DHM were at the lowest risk of prolonged hospital stay and neonatal complications, such as necrotizing enterocolitis, compared to those who received infant formula (Yang et al., 2020). This illustrates the benefits of DHM for neonates.
Several studies across Africa have shown that most mothers possess limited knowledge of HMB, resulting in low willingness to use or donate donor breast milk (Bhoola & Biggs, 2021; Iloh et al., 2018; Kimani-Murage et al., 2019; Mantji et al., 2019; Ogundele et al., 2022). However, a study conducted in South Africa demonstrated a significant increase in mothers’ willingness to donate and use donor breast milk following targeted education (Goodfellow et al., 2016).
Achieving the Sustainable Development Goal (SDG) target of fewer than 12 deaths per 1,000 live births by 2030 requires efforts, including promoting the use of breast milk as a key intervention (Alkema et al., 2014;WHO, 2022a, 2022b).
Tanzania has not yet established any HMB. In the absence of such infrastructure, only a small number of neonates whose mothers are unable to breastfeed due to illness or death receive breast milk through informal wet nursing by close relatives. This limited access underscores the urgent need for structured, safe alternatives to support infant nutrition and survival. Several studies have documented the practice of informal milk sharing, whereby breast milk is directly donated from one mother to another. This enables mothers with surplus milk to provide nourishment to newborns whose mothers have insufficient milk supply, or who are severely ill, or deceased (Kimani-Murage et al., 2019). This practice is discouraged due to the fear of contact infections, mainly human immunodeficiency virus (HIV). As a result, infant formula is mostly preferred over DHM (Mantji et al., 2019).
In rural communities, cultural diversity often contributes to limited knowledge about HMBs. Therefore, establishing HMBs requires raising awareness to address and mitigate the fears associated with traditional milk-sharing practices. This study aims to assess the knowledge and acceptability of DHM among women attending Haydom Lutheran Hospital in Tanzania.
Methods
This was an analytical cross-sectional study, conducted between October 2022 and October 2023. The study was conducted at Haydom Lutheran Hospital, a remote faith-based referral hospital in the Manyara region, approximately 300 km off-road southwest of Arusha. The area is inhabited by diverse ethnic groups, with the majority being the Iraqw and Datooga. The hospital serves seven districts across four regions, providing care for over 1 million people in its catchment area. It provides Level III neonatal care under the pediatrics department, caring for about 1,500 neonates annually, most of whom are premature with birth weights ≤ 1,500 g. The unit is equipped with radiant warmers, oxygen concentrators, suction devices, resuscitation equipment, and CPAP for advanced respiratory support, with care delivered by trained nurses and medical doctors under pediatrician oversight (Haydom Lutheran Hospital, 2015). Although no full-time neonatologist is available, ongoing staff training in neonatal resuscitation and infection prevention supports the feasibility of introducing a HMB in this resource-limited setting.
Women attending reproductive and child health services (RCHS), the neonatal care unit (NICU), and or receiving postnatal care (PNC) during the time of the study were enrolled. The inclusion criteria were women aged ≥ 18 years with children under 2 years. Exclusion criteria were women who did not consent to participate and those with mental health problems.
The calculated sample size was 236 participants, based on an assumed baseline knowledge rate of 18.9% regarding human milk banks (Bhoola & Biggs, 2021a), as no baseline data for HLH existed. A 95% confidence interval and a marginal error of 0.05 was used. A further 10% was added to compensate for non-responders.
Data Collection and Analysis
A structured questionnaire was administered by trained research assistants to participants. The questionnaire had four parts, totaling 30 questions in Swahili, the lingua franca in Tanzania. The first part collected sociodemographic and obstetric information, such as age, sex, and tribe. The second part assessed knowledge of human milk donation, and the third part assessed the acceptability of human milk donation and HMBs. The fourth part identified myths about human milk donation. Knowledge questions were adapted from the existing literature, with each question on DHM and HMBs marked with 1 point, for a total of 12 marks; 9–12 equals good knowledge, 6–8 equals satisfactory knowledge, and 0–5 equals poor knowledge (Tian et al., 2021). The study was conducted at three sites (RCHS, NICU, and postnatal). Data collectors introduced themselves to potential participants and explained the study’s aim. After obtaining consent, participants completed the questionnaires anonymously. In case of any misunderstanding, the data collectors clarified the question. Every participant had to sign a consent form, be > 18 and be allowed to exit the study at any point.
Data was collected, entered, and analyzed using SPSS (Version 20). Descriptive statistics were performed, with frequencies and percentages used for categorical data. Frequency distribution and percentages were used to assess mothers’ knowledge. A multivariate logistic regression was done, including age, tribe, residency, religion, occupation, education level, marital status, and parity, to investigate factors associated with acceptance of donating and using DHM to calculate the crude and adjusted odds ratios to determine the strength of association. A p value < 0.05 was considered statistically significant.
Due to low numbers, the tribal associations of Nyaturu, Hehe, Chagga, Haya, and Ngoni were grouped into a variable labelled “others.” Likewise, for residency, people from Kilimanjaro and Tabora regions were grouped under “others.”
Ethical clearance was granted by NIMR (Ethical number: NIMR/HQ/R.8a/Vol.IX/4109), and local permission was obtained from the executive director of HLH.
Results
A total of 260 women aged 18 and above were recruited, with one person later dropping out. The most common tribal affiliation was Iraqw (58%), and the most common parity was between one and three children (63%). The majority of participants were from the Manyara region (78%), were Christian (83%), and were married (83%). Close to half (47%) had primary education, and 36% were housewives. Additional sociodemographic characteristics of the participants are shown in Table 1.
Sociodemographic Characteristics Distribution of the Participants (n = 260).
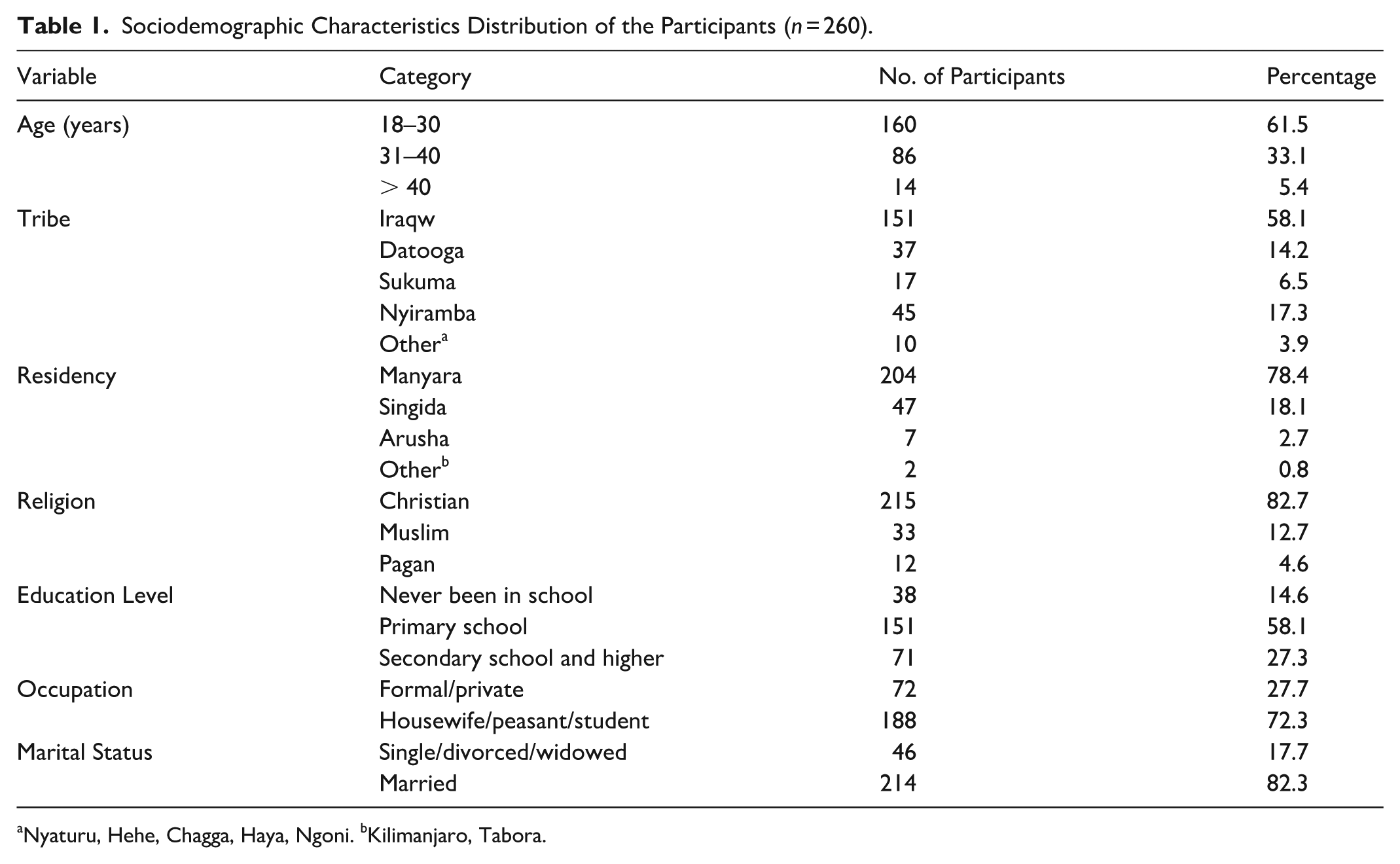
Nyaturu, Hehe, Chagga, Haya, Ngoni. bKilimanjaro, Tabora.
Table 2 shows the obstetrics and breastfeeding history. The majority (82%) had spontaneous vertex delivery; for 82% the baby was born at term; and 89% exclusively breastfed for 6 months.
Obstetrics and Breastfeeding History of the Participants (n = 260).
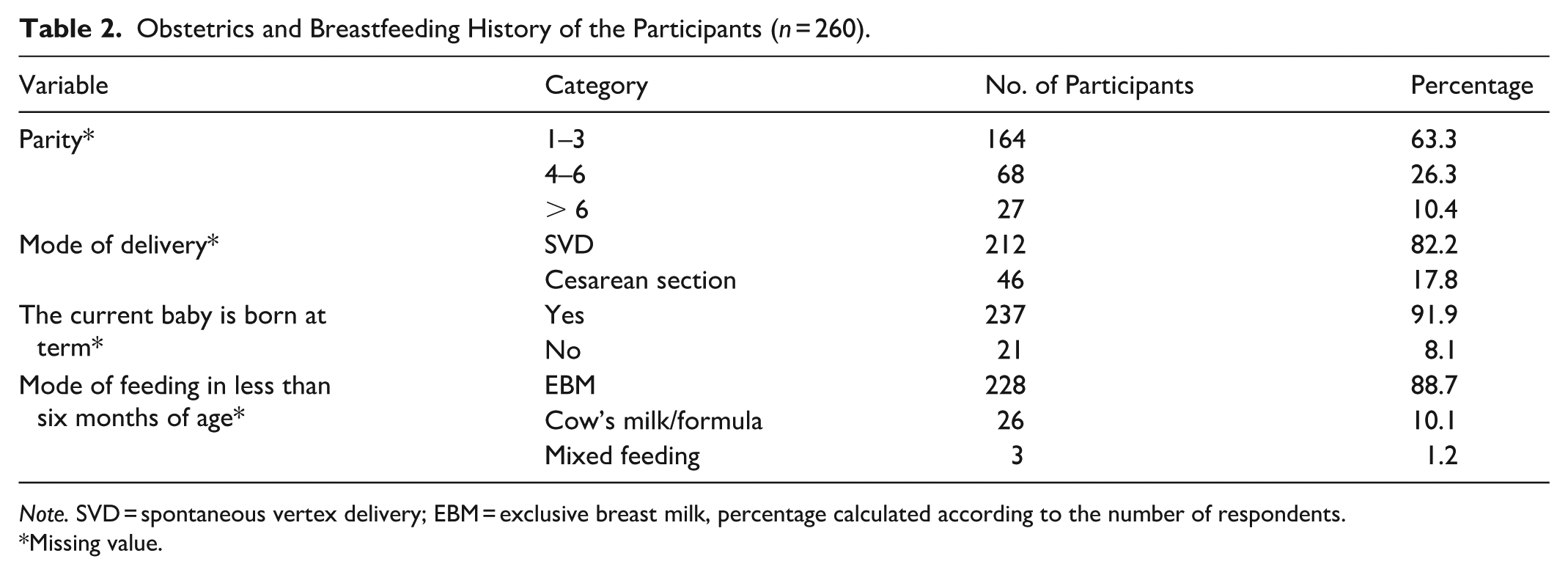
Note. SVD = spontaneous vertex delivery; EBM = exclusive breast milk, percentage calculated according to the number of respondents.
Missing value.
Knowledge of HMB
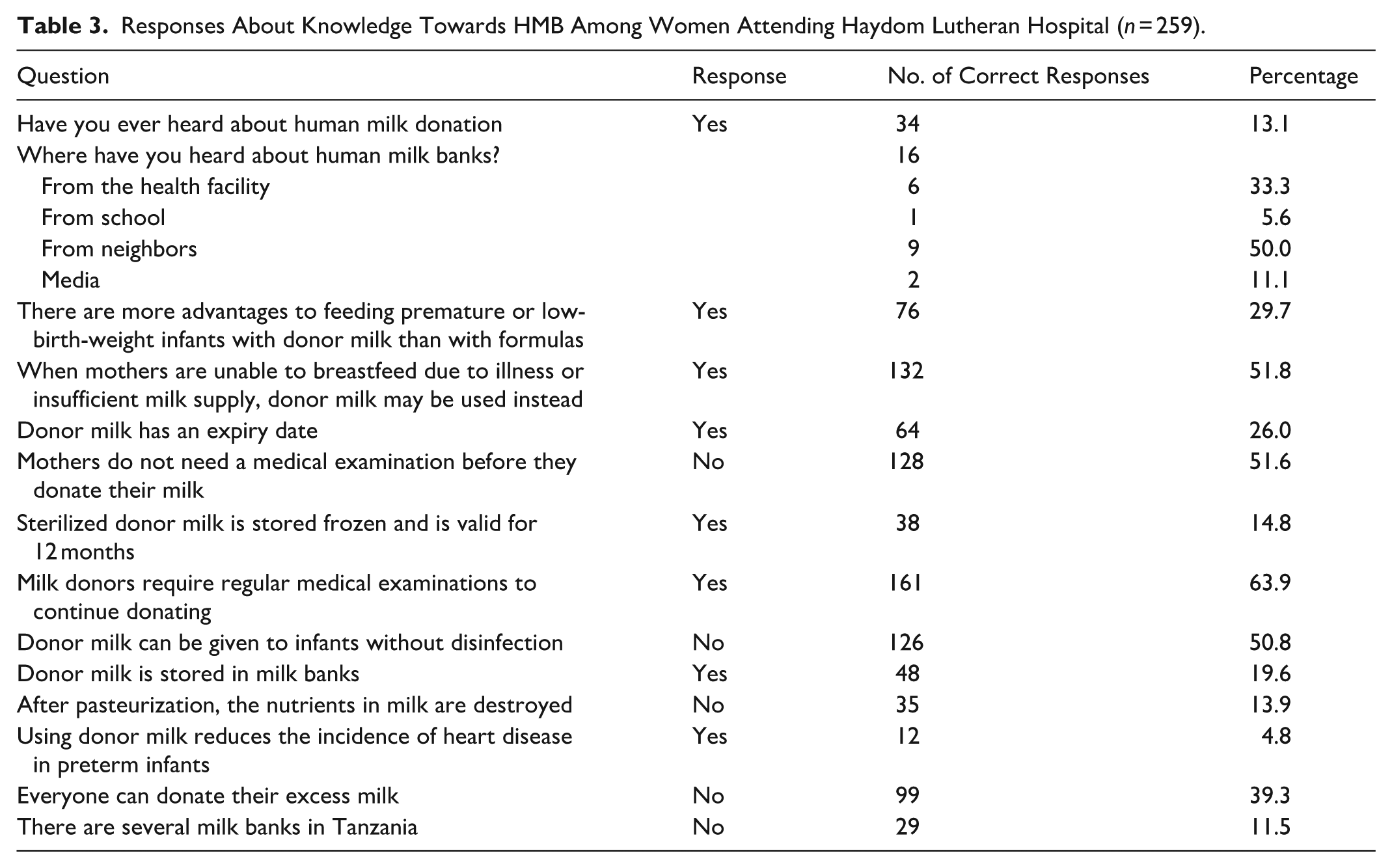
A total of 86% of participants were unaware of DHM, whereas 33.3% had heard of it from health facilities. Regarding the 12 knowledge questions, 29.7%, 51.8%, and 26% knew the benefits, use, and expiration of donor human milk, respectively. However, 51.6%, 13.9%, and 11.5% recognized that donors require examinations, that pasteurization does not destroy nutrients, and that there is currently no HMB in Tanzania, respectively. The details are summarized in Table 3. Figure 1 shows the knowledge scores.
Responses About Knowledge Towards HMB Among Women Attending Haydom Lutheran Hospital (n = 259).
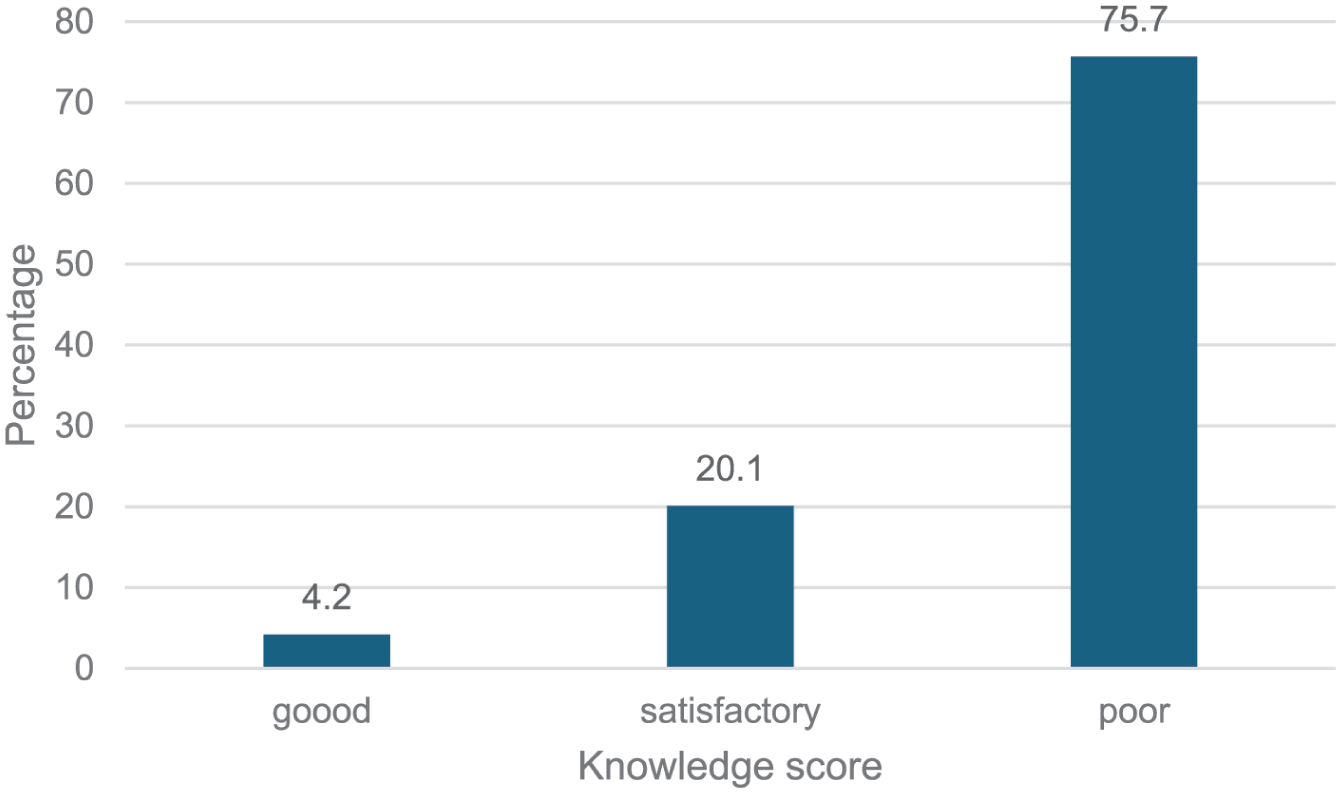
Knowledge scores on HMBs among women attending Haydom Lutheran Hospital.
Acceptability and Myths Towards HMB Among Women Attending Haydom Lutheran Hospital
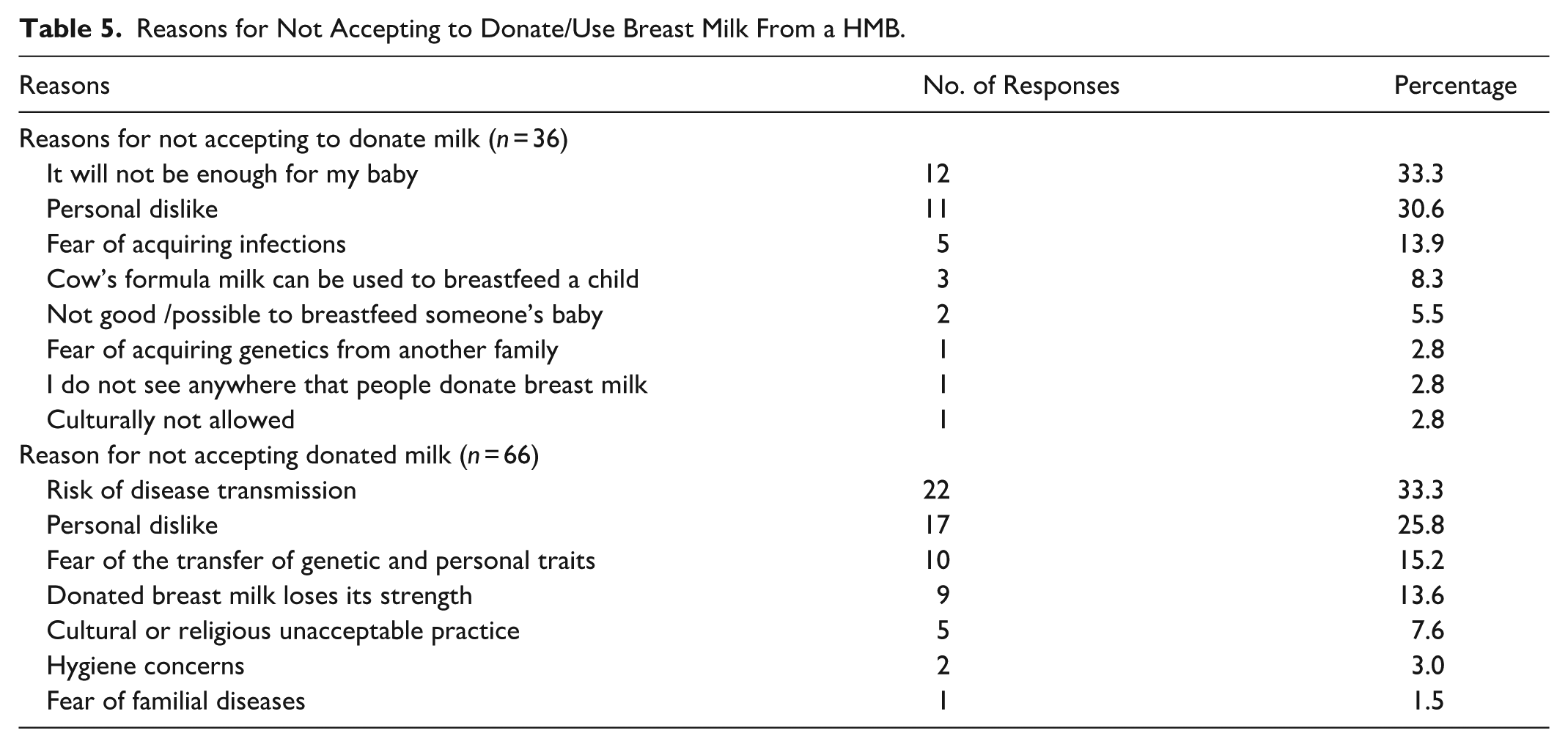
A total of 97% of participants had never donated or breastfed another baby. About 67.1% of participants were ready to donate their own milk to HMB if asked. Among those who were not ready to donate their own milk, the main reason was fear that their milk would not be enough for their baby (32.4%). Among women who participated, 61% were ready to accept donated milk for their babies if needed. Among those who opposed using human-donated milk, the main reasons were the risk of disease transmission (33.3%) and personal dislike (25.8%). Other reasons are clarified in Tables 4 and 5.
Acceptability, Willingness, and Myths Towards Human Milk Bank Among Women Attending Haydom Lutheran Hospital.
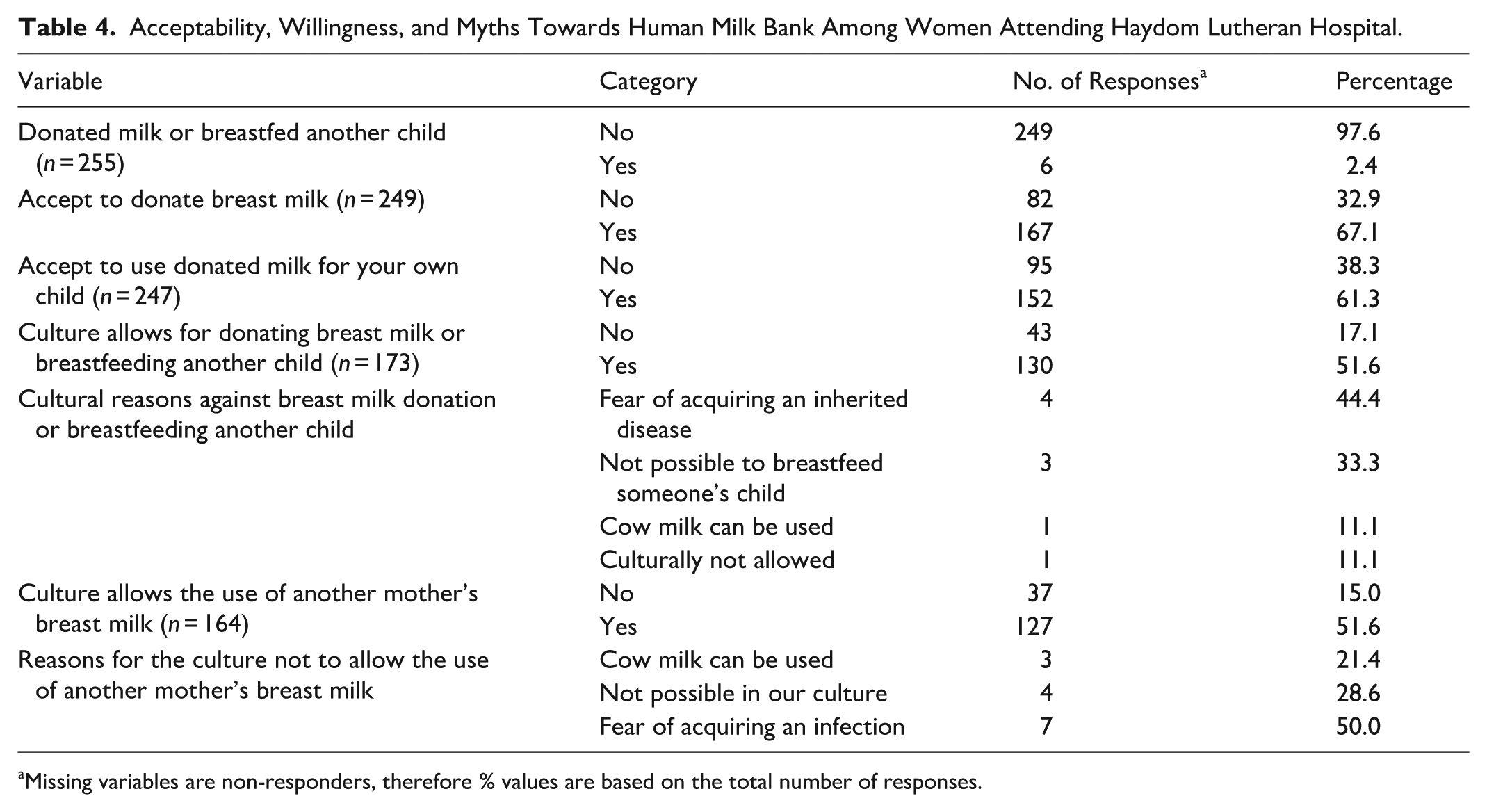
Missing variables are non-responders, therefore % values are based on the total number of responses.
Reasons for Not Accepting to Donate/Use Breast Milk From a HMB.
Factors Associated With Acceptability Toward DHM Among Women Attending Haydom Lutheran Hospital
Evidence indicated that the acceptability of donating human milk among women was associated with secondary school or higher education, with an AOR of 4.79 (95% CI [1.3, 17.57], p = 0.018).
However, for DHM use, there was evidence of associations in both groups: primary school education had an AOR of 3.2 (95% CI [1.09, 9.85], p = 0.03), and secondary school or higher education had an AOR of 6.01 (95% CI [1.55, 23.21], p = 0.009). No other variables showed evidence of association (see Tables 6 and 7).
Factors Associated With Acceptability of Donating DHM Among Women Attending Haydom Lutheran Hospital (N = 249).
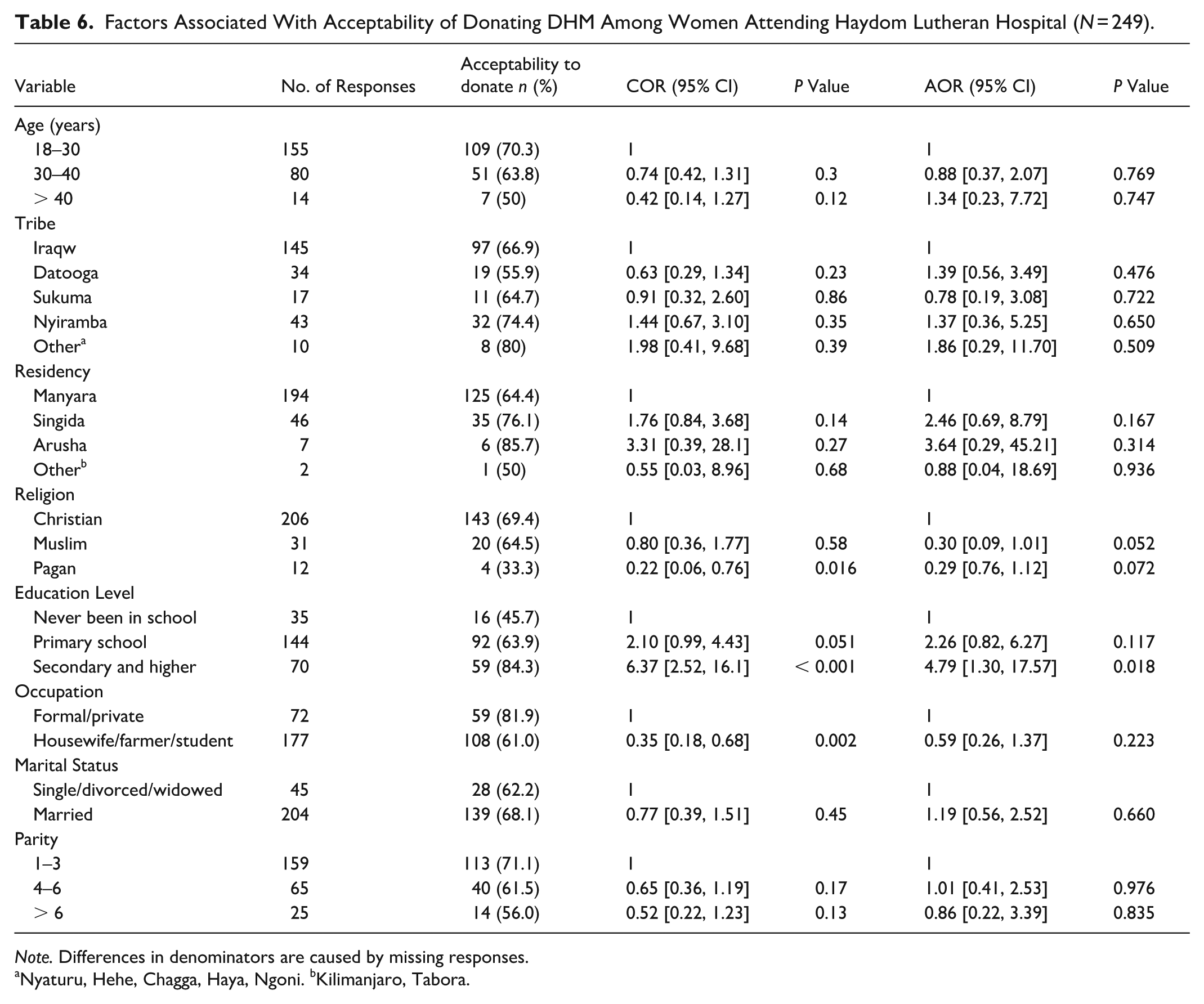
Note. Differences in denominators are caused by missing responses.
Nyaturu, Hehe, Chagga, Haya, Ngoni. bKilimanjaro, Tabora.
Factors Associated With Acceptability to Use DHM Among Women Attending Haydom Lutheran Hospital (N = 248).
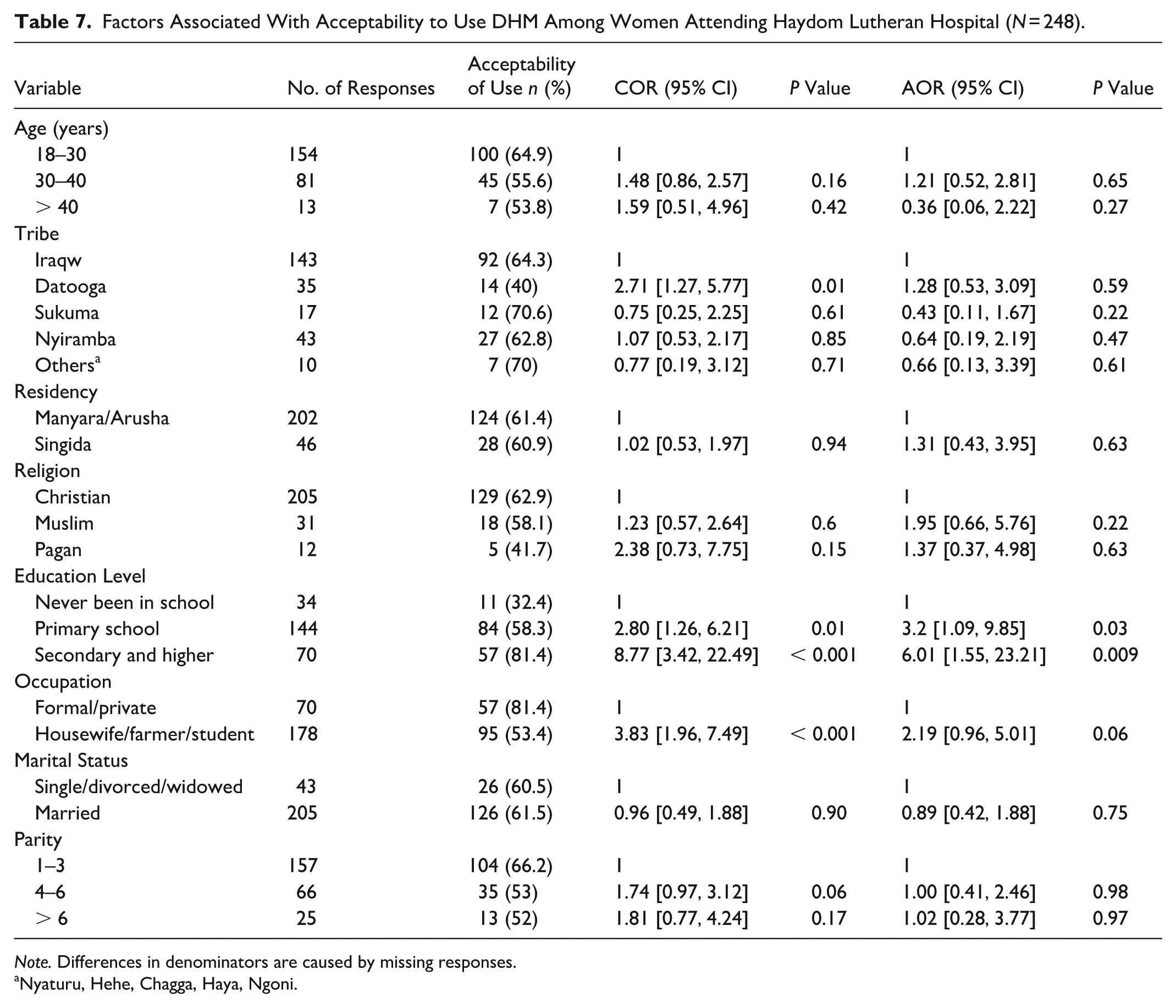
Note. Differences in denominators are caused by missing responses.
Nyaturu, Hehe, Chagga, Haya, Ngoni.
Discussion
This study aimed to assess knowledge, acceptability, and myths among women attending HLH regarding HMB. Our study found that 14% of participants had heard of HMB and obtained information from the health facility. Studies conducted in Kenya and Nigeria showed that more than one quarter of all participants and up to a half, respectively, had ever heard of HMB. However, only 12% in a different study from Tanzania had ever heard about HMB, which is comparable to our results (Kimani-Murage et al., 2019; Kimaryo et al., 2024; Ogundele et al., 2022). Based on our study’s results, the idea of HMB in Tanzania appears to be unfamiliar and shows a need to raise awareness.
Most participants had low HMB knowledge scores, with 75% scoring below 6 points. This result is comparable with the findings from Limpopo in South Africa, which showed that women did not know about DHM (Bhoola & Biggs, 2021; Mantji et al., 2019). Likewise, a multi-center study from Nigeria revealed a significant lack of awareness, too, with one-quarter of the participants unfamiliar with the concept of DHM (Iloh et al., 2018). Similarly, low levels of familiarity with HMB were found among populations in China and Nepal, where awareness was confined to a small fraction of people (Sapkota et al., 2024; Tian et al., 2021). Conversely, an online survey in Malaysia demonstrated that over half of the respondents possessed a good understanding of both milk sharing and HMB (Ramachandran et al., 2024). Compared to other countries, our study shows that women attending HLH have low overall knowledge of donor milk and need to improve it. This may relate to the socioeconomic and educational characteristics of the area in which our study was conducted. The participating regions had lower general levels of formal education and limited access to technology and modern communication channels. We hypothesize that in this context this directly limited prior exposure to and awareness of DHM. This is supported by our finding that participants unfamiliar with DHM at baseline had significantly lower knowledge about it. Thus, lower baseline knowledge in our cohort may not reflect a general lack of interest, but, rather, a lack of opportunity to access relevant information, suggesting that educational background is a key factor shaping awareness due accessibility of said information.
This study shows that despite having limited knowledge, more than half of the participants accept donor milk, either as donors or recipients. This is similar to several studies which reported high acceptability rates in Nepal, India, Turkey, Kenya, Uganda and Tanzania, while significantly lower rates were found in Ethiopia and Nigeria (Ekşioğlu et al., 2015; Gelano et al., 2018; Kimani-Murage et al., 2019; Kimaryo et al., 2024; Namuddu et al., 2023; Ogundare et al., 2023; Sapkota et al., 2024; Taksande et al., 2024) showing a variable picture over several countries.
One of the most frequently mentioned reasons for not accepting DHM in our study was fear of transmitting infections or of passing on genetic and personal traits. These reasons for not accepting donated milk have been shown in other studies from a variety of countries, such as Ethiopia, Turkey, Kenya, Tanzania, Uganda, Malaysia, and Nigeria (Ahmed et al., 2024; Alemu et al., 2021; Gelano et al., 2018; Ekşioğlu et al., 2015; Kimani-Murage et al., 2019; Kimaryo et al., 2024; Namuddu et al., 2023; Ogundele et al., 2022; Ramachandran et al., 2024).
A survey from South Africa showed a significant improvement in knowledge and acceptance after counseling and educating the women (Goodfellow et al., 2016). Similarly, in Nigeria, the majority of participants indicated that they would be more likely to accept donor human milk if provided with additional information (Ogundare et al., 2023), highlighting that perhaps lower or no education can be counteracted by actively improving awareness about breast milk donation and its use at HMBs. Likewise, in Nepal, 74% of study participants had heard of HMB through obtaining information from health facilities (Taksande et al., 2024).
In our study, we found evidence that women with primary or secondary education, or higher, were more likely to accept the use of DHM than those who never had formal education. Interestingly, this evidence was observed only among women with secondary education or higher when donating DHM. Why primary education had no impact is not clear yet. Our results are similar to a study conducted in Uganda which showed that graduates had higher odds of donating human milk. However, in the study from Uganda, this was only the case for the univariate analysis, whereas in our study the effect was still seen after conducting a multivariate analysis (Ahmed et al., 2024).
Limitations
The main limitation of this study was the restriction of the sample to women attending a single rural hospital rather than to women from the surrounding villages. Therefore, the results may not reflect the urban context or the country as a whole. Another limitation is the predominance of area-specific groups, which could be addressed by conducting larger-scale surveys across multiple areas. Additionally, the questionnaire was not designed to elaborate in depth on how education would impact the acceptability of donating or using DHM.
Conclusion
This study highlights the acceptability of donating and using DHM for infants. However, there is a need to engage with and further emphasize the importance of DHM in communities, while addressing cultural, religious, and health concerns, and building awareness of the value of breastfeeding and milk. Also, this study shows that overall acceptability among women and staff is a cornerstone for establishing a DHM at HLH and can be advanced to the next practical level. More information about human milk banks should be provided to mothers through the antenatal clinic, a vital setting where more mothers are seen daily. However, greater effort is needed from the government in policymaking, political support, and financial investment.
Footnotes
Acknowledgements
We extend our gratitude to our families for their support and to the mothers who participated in this study.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data underlying this article are available at Haydom Lutheran Hospital. Access can be requested through the hospital administration.