
Abstract
Background:
We aimed to evaluate the efficacy, safety, and cost-effectiveness of suction-assisted retrograde intrarenal surgery (SA-RIRS) compared with conventional retrograde intrarenal surgery (RIRS) and to compare outcomes between suction catheters and suction sheaths in the management of upper urinary tract stones ≤30 mm.
Methods:
A systematic review and meta-analysis of randomized controlled trials (RCTs) were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines. PubMed, Embase, Cochrane Library, and Web of Science were searched to September 2025. Eligible RCTs compared SA-RIRS (catheter or sheath) with conventional RIRS in adults. Primary outcomes were stone-free rate (SFR), total complications, and operative time; secondary outcomes included hospital stay, reoperation rate, stone retropulsion, basket use, and laser time. Risk of bias (RoB) was assessed using the Cochrane RoB 2.0, and evidence certainty was rated with the Grading of Recommendations, Assessment, Development, and Evaluation.
Results:
Six RCTs involving 843 patients (SA-RIRS: 420; conventional RIRS: 423) were included. SA-RIRS significantly improved SFR (odds ratio [OR] = 4.00, 95% confidence interval [CI]: [2.92, 5.48], p < 0.001) and reduced total complications (OR = 0.40, 95% CI: [0.17, 0.97]), stone retropulsion (OR = 0.26, p = 0.03), and basket use (OR = 0.01, p < 0.001). Subgroup analysis demonstrated that both suction sheaths (OR = 4.46) and suction catheters (OR = 2.64) significantly improved SFR compared with conventional RIRS, with sheaths showing greater complication reduction (OR = 0.27 vs 0.77). No significant differences were observed in operative time, hospital stay, or reoperation rate. Evidence certainty was high for all outcomes.
Conclusions:
SA-RIRS provides superior stone clearance and safety compared with conventional RIRS. Although sheath-based systems offer the highest SFRs and complication reductions, suction catheters also significantly improve clearance and remain a cost-effective option for impacted ureteral stones. Findings support integrating SA-RIRS into routine endourological practice, with device selection guided by stone location and resource availability.
Trial Registration PROSPERO:
CRD420251149743.
Keywords
Introduction
Urolithiasis is a major global health burden, with a lifetime prevalence of approximately 10% and a rising incidence driven by lifestyle and dietary changes.1,2 Retrograde intrarenal surgery (RIRS) is the first-line minimally invasive treatment for upper urinary tract stones ≤2 cm. 3 Despite significant advances, conventional RIRS still faces important limitations: stone retropulsion (15%–30% of cases) prolongs operative time and reduces stone clearance 4 ; stone dust and hemorrhage obscure visibility, necessitating frequent interruptions; elevated intrarenal pressure (IRP >30 mm Hg) is associated with infectious complications such as urosepsis (incidence 5%–18%) 5 ; residual fragments (RFs >2 mm) increase recurrence and reintervention rates 6 ; and reliance on stone baskets adds procedural complexity and cost.
Suction-assisted RIRS (SA-RIRS) has emerged as a transformative approach, integrating active aspiration to remove debris in real time, maintain low IRP, and minimize retropulsion—advantages not achievable with conventional access sheaths.7,8 Clinically, SA-RIRS technologies fall into two main categories:
Suction catheters (e.g., CVAC Aspiration System,
8
VC-URSL catheter
9
): Small-caliber devices (1.2–11.9F) for targeted fragment removal, often paired with semirigid ureteroscopes. Suction sheaths (e.g., FANS,
10
S-UAS
11
): Larger bore systems (10–14F) with integrated suction, compatible with flexible ureteroscopes for continuous IRP control and improved caliceal access.
Although individual randomized controlled trials (RCTs) have reported promising outcomes for SA-RIRS,7–12 heterogeneity in device design, patient populations, and outcome definitions has hindered definitive conclusions. Previous reviews have either included non-RCTs or focused on single device types, lacking direct comparisons between suction catheters and sheaths.13,14 Furthermore, cost-effectiveness data remain scarce, with only three RCTs providing relevant economic analyses.7,11,12
To address these gaps, we conducted the first meta-analysis exclusively of RCTs to compare SA-RIRS with conventional RIRS in terms of efficacy (e.g., stone-free rate [SFR]), safety, and subgroup differences between suction catheters and sheaths. Given the limited available data, we also provide a preliminary assessment of cost-effectiveness. We hypothesized that SA-RIRS—particularly sheath-based systems—would achieve higher SFRs, shorter operative times, and lower complication rates compared with conventional RIRS and catheter-based approaches.
Methods
Literature search and eligibility criterion
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement. 15 A comprehensive literature search was performed in four major electronic databases—PubMed, Embase, Cochrane Library, and Web of Science—from their inception to September 1, 2025. The search strategy combined Medical Subject Headings and free-text terms related to RIRS, suction or negative pressure techniques, and urinary tract stones. Detailed search strategies for each database are provided in Supplementary Table S1.
To minimize publication bias, we also performed manual searches of the reference lists of all the included studies and of three recent high-impact reviews on SA-RIRS.13,14,16 No restrictions were applied to the publication year, but non-English studies were excluded to avoid language-related extraction bias.
Studies were eligible if they met the following criteria: RCTs comparing suction-assisted retrograde intrarenal surgery (SA-RIRS) using any suction device (catheters or sheaths) with conventional RIRS without suction; adult patients (≥18 years) with renal or ureteral stones located above the iliac vessels; stone size ≤30 mm in accordance with the European Association of Urology guidelines 2 ; and reporting at least one relevant clinical outcome such as SFR, operative time, complication rate, hospital stay, reoperation rate, stone retropulsion, or stone basket use. We excluded non-RCT designs, studies involving pediatric patients, trials with unextractable or overlapping data, and studies evaluating suction techniques outside endocorporeal laser lithotripsy.
Study quality assessment
Two reviewers (Y.L. and H.W.) independently assessed the methodological quality of each included RCT using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool. 17 This tool evaluates five key domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, and completeness of outcome data. Given that suction devices are visually distinct from conventional instruments, performance bias was considered inherently high across all studies. Discrepancies between reviewers were resolved through discussion with a third senior reviewer (H.Z.). No studies were excluded solely on the basis of bias risk; instead, RoB was incorporated into the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) rating and sensitivity analyses.
Data extraction
Data were independently extracted by two reviewers (Y.L. and Z.Z.) using a prepiloted standardized Excel form and cross-checked by a third reviewer (Y.Z.) for accuracy. Extracted information included study characteristics (first author, year, country, sample size, device type and model, laser type and parameters), patient demographics (age, gender, body mass index [BMI]), stone characteristics (size, density, location), and clinical outcomes. Outcomes were recorded as defined in each study, including SFR (definition and follow-up time), operative time (from ureteroscope insertion to stent placement), complication rates (classified by Clavien–Dindo grade), and secondary outcomes such as hospital stay, reoperation rate, stone retropulsion, basket use, and laser time. When outcome definitions or time points were unclear, we attempted to contact the study authors; in the absence of responses, data were extracted as reported.
Statistical analysis
Meta-analyses were performed using Review Manager version 5.4 (Cochrane Collaboration, London, UK). 18 For dichotomous outcomes (e.g., SFR, complications, reoperations, retropulsion, basket use), pooled effect sizes were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). For continuous outcomes (e.g., operative time, hospital stay, laser time), mean differences (MDs) with 95% CI were calculated.
Heterogeneity was assessed using the I2 statistic and Cochran’s Q test. An I2 value <50% was considered low heterogeneity, and a fixed-effects model was applied; an I2 ≥50% indicated substantial heterogeneity, and a random-effects model was used to account for between-study variability. Potential sources of heterogeneity were explored through subgroup analyses stratified by suction device type (catheter vs sheath) and sensitivity analyses excluding studies at high RoB. In addition, potential publication bias was evaluated through the visual inspection of funnel plots. 19
Certainty of evidence
The certainty of evidence for each outcome was evaluated using the GRADE approach via GRADEpro GDT software (https://gradepro.org/). 20 All outcomes began with a high certainty rating because of the inclusion of RCTs. Downgrading was considered for RoB, inconsistency (I2 >75% without plausible explanation), indirectness (populations or interventions not representative of clinical practice), and imprecision (wide 95% CI crossing the null or small sample size). A two-tailed p-value of <0.05 was considered statistically significant.
Results
Literature search and study selection
The initial database search yielded 282 records. After removing 68 duplicates, 214 records remained for screening. Title and abstract review excluded 137 records, including 72 non-RCTs, 38 studies evaluating nonsuction techniques, and 27 studies involving pediatric populations. The remaining 77 full-text articles were assessed for eligibility, of which 71 were excluded because they were non-RCTs (n = 32), had a sample size <15 patients (n = 18), were non-English publications (n = 9), involved overlapping patient cohorts (n = 11), or did not use contemporary devices (n = 1). Ultimately, six RCTs7–12 met the inclusion criteria and were analyzed in this meta-analysis (Fig. 1).
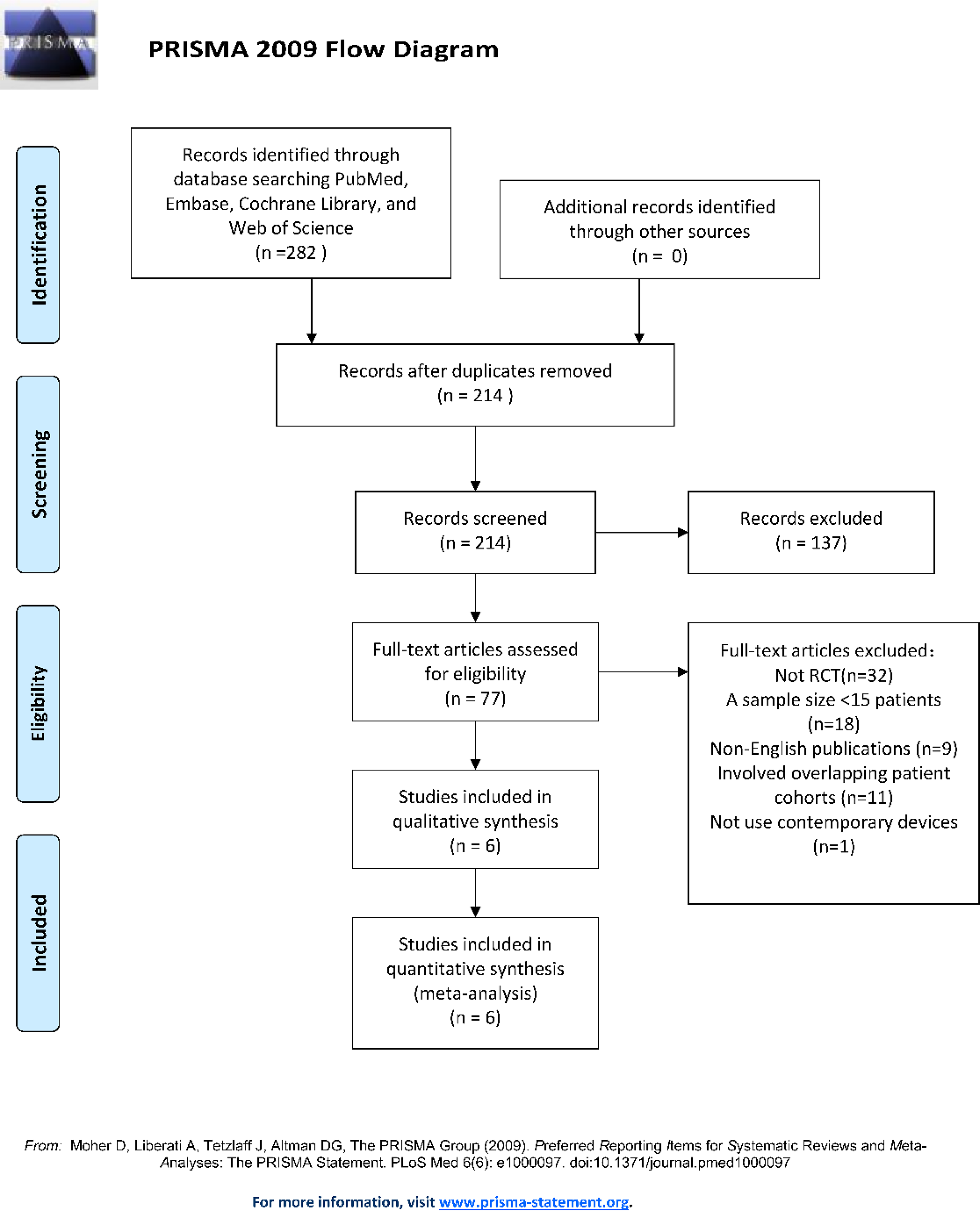
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. RCT = randomized controlled trial.
These studies were published between 2018 and 2025 and conducted across seven countries, including China (three studies), the United States (one study), Italy (one study), and a multicenter trial involving the Philippines, Malaysia, and Turkey (one study). Three RCTs investigated suction catheters (CVAC 1.0, 8 VC-URSL, 7 VCC 9 ), whereas three examined suction sheaths (perfusion/suction platform, 12 FANS, 10 S-UAS 11 ).
Baseline characteristics of included studies
Across the six RCTs7–12, a total of 843 patients were enrolled, comprising 420 in the SA-RIRS group and 423 in the traditional RIRS group. Baseline demographics and stone characteristics were generally well balanced, with no statistically significant differences in age, gender, BMI, or stone density between groups (Table 1). The mean age ranged from 46 to 63 years, BMI from 23.9 to 32.0 kg/m2, and male predominance was noted in both groups (55.6%–60.0% in SA-RIRS vs 51.0%–60.0% in traditional RIRS).
Stone burden ranged from 8.8 to 21.9 mm, with the exception of Matlaga et al., 8 who reported a significantly higher burden in the traditional RIRS group (19 ± 11 mm vs 14 ± 6.5 mm, p = 0.002). Stone density, reported in five studies, ranged from 612.0 to 1022.8 Hounsfield unit (HU) and was comparable between groups. Stones were predominantly located in the renal pelvis (32.5%–45.6%) and proximal ureter (32.5%–36.9%), with lower calix stones accounting for 8.1%–13.1%. All studies utilized holmium: yttrium-aluminum-garnet lasers, and Matlaga et al. 8 additionally used thulium fiber laser (TFL) in 16% of SA-RIRS cases. Baseline renal function and preoperative urinary tract infection rates (11.3%–18.8%) did not differ significantly between groups (p > 0.05).
Table of Baseline Characteristics
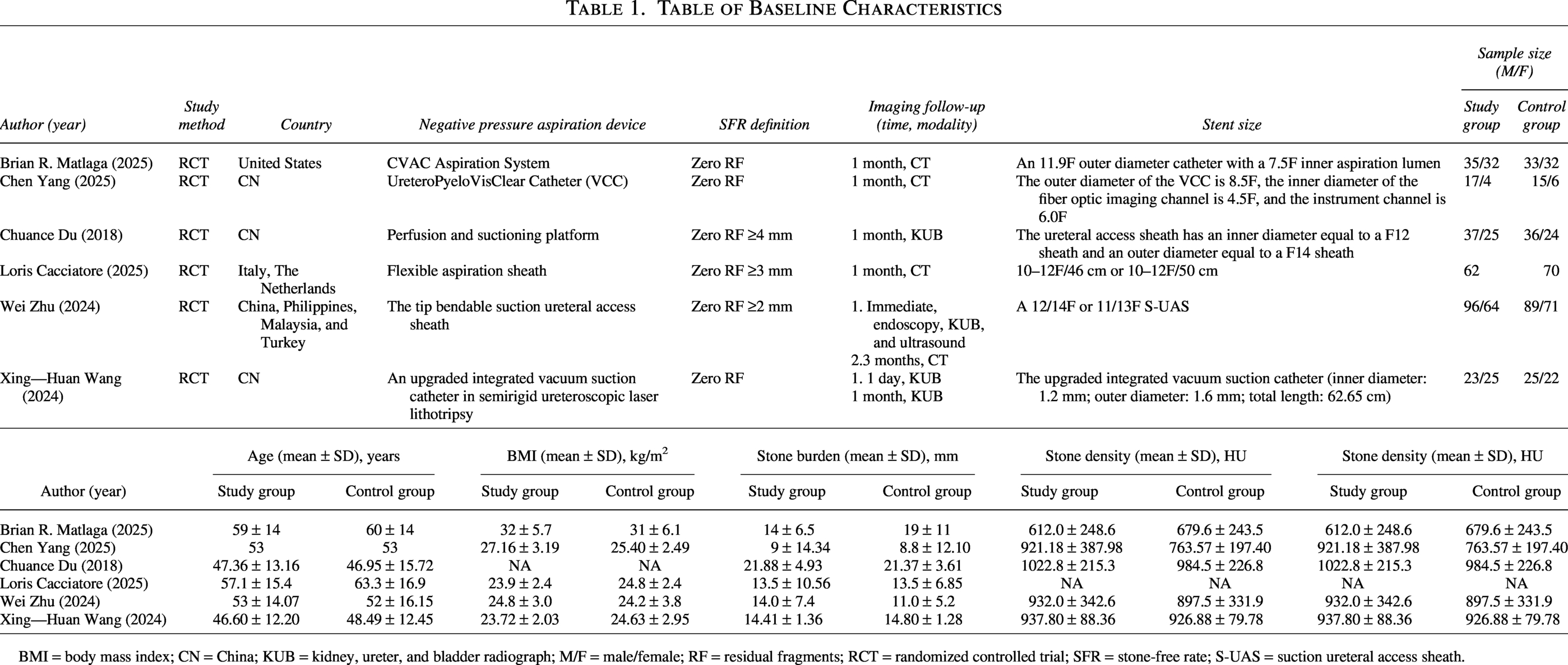
BMI = body mass index; CN = China; KUB = kidney, ureter, and bladder radiograph; M/F = male/female; RF = residual fragments; RCT = randomized controlled trial; SFR = stone-free rate; S-UAS = suction ureteral access sheath.
RoB assessment
The methodological quality of the six included RCTs was assessed using the Cochrane RoB 2.0 tool (Fig. 2). Overall, two studies were evaluated as having a low RoB, whereas the remaining four studies were deemed to have “some concerns.” Importantly, no studies were rated as having a high RoB. Regarding specific domains, the randomization process (Domain 1) and missing outcome data (Domain 3) were at a low risk across all six trials (100%), indicating appropriate sequence generation, allocation concealment, and minimal attrition. For deviations from the intended interventions (Domain 2), two studies raised some concerns, whereas the other four were at low risk. In terms of the measurement of the outcome (Domain 4), two studies presented some concerns, whereas the remaining four maintained a low risk. Finally, for the selection of the reported result (Domain 5), five out of six studies demonstrated a low RoB, with only one study raising some concerns. Overall, the trials presented acceptable methodological quality for inclusion in the meta-analysis.
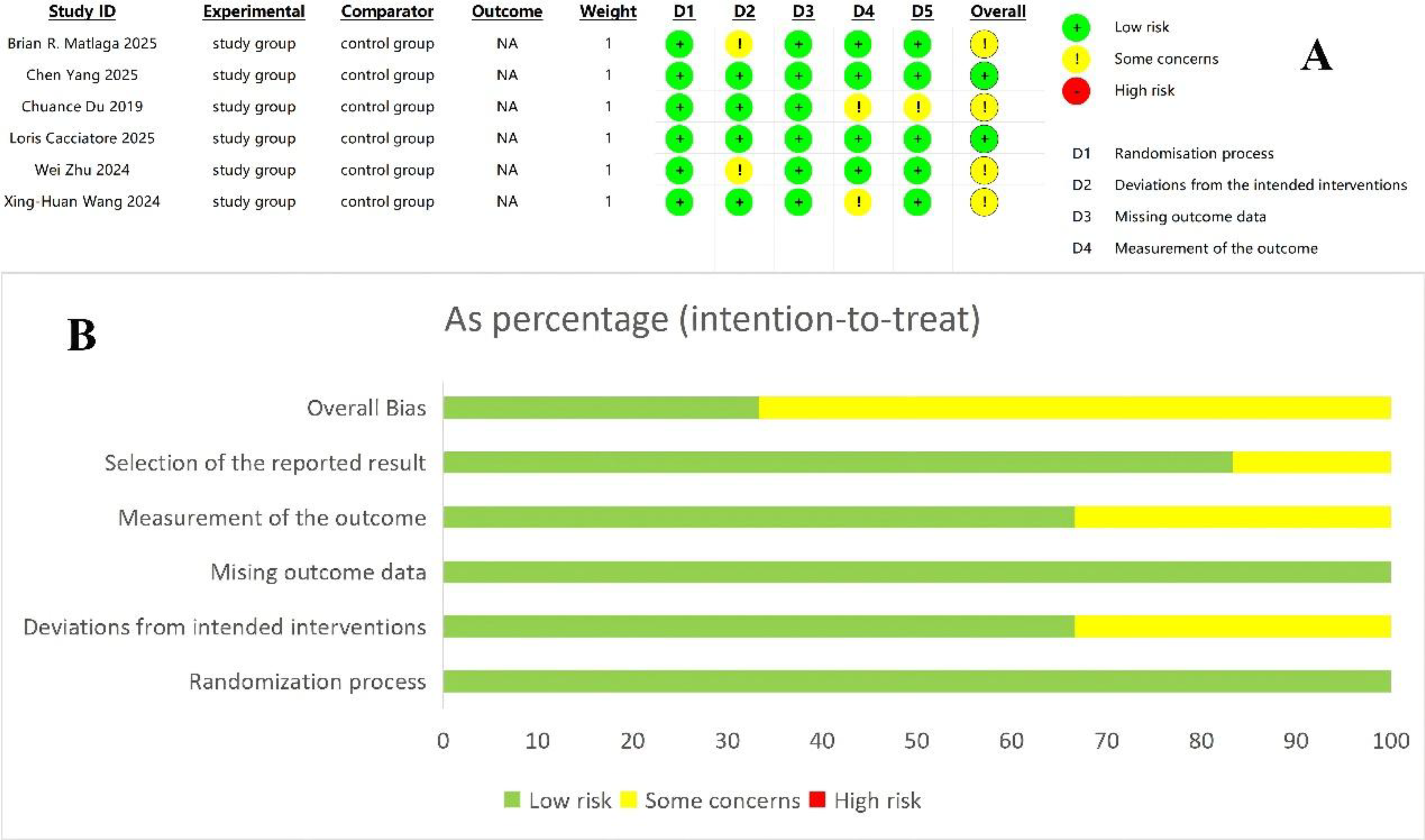
Risk-of-bias summary and risk-of-bias graph. NA = not available.
Meta-analysis of outcomes
Primary outcome
Stone-free rate
All six RCTs reported SFR, with follow-up ranging from 24 hours to 3 months. Pooled analysis demonstrated that SA-RIRS significantly improved SFR compared with traditional RIRS (OR = 4.00, 95% CI: [2.92, 5.48], p < 0.001), with low heterogeneity (I2 = 12%, p = 0.34) (Fig. 3). Subgroup analysis based on device type revealed that suction sheaths were associated with a markedly higher SFR (OR = 4.46, 95% CI: [3.13, 6.37], p < 0.001) and low heterogeneity (I2 = 39%), exemplified by Cacciatore et al. 10 reporting a 1-month SFR of 95% vs 67% (p < 0.005) and Zhu et al. 11 reporting a 3-month SFR of 87.5% vs 70% (p < 0.001). Furthermore, a specific comparison between traditional RIRS utilizing standard nonsuction ureteral access sheaths vs suction sheaths confirmed that the integration of suction significantly improves stone clearance over standard access sheaths. In addition, suction catheters also significantly improved SFR (OR = 2.64, 95% CI: [1.33, 5.23], p = 0.005), with zero heterogeneity (I2 = 0%). Despite variations in catheter design—such as Wang et al. 7 (VC-URSL, multichannel) achieving a 1-day SFR of 91.7% vs 74.5% (p = 0.025) and Matlaga et al. 8 (CVAC, single-channel) reporting comparable individual rates—the updated pooled data support the efficacy of both catheter and sheath systems.
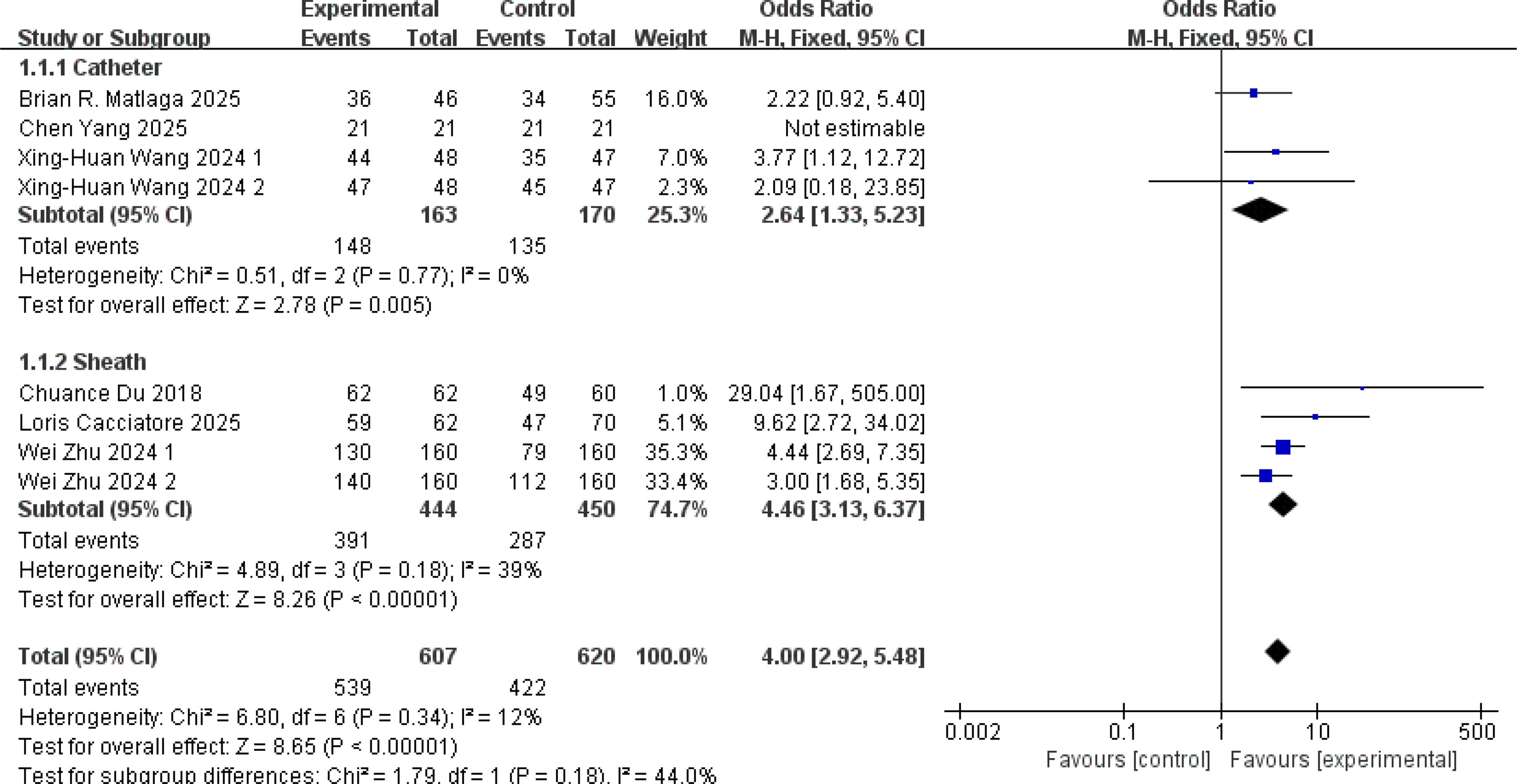
Forest plot of stone-free rate (catheter vs sheath). CI = confidence interval.
To address imaging limitations and differences between the trials, an additional subanalysis was performed exclusively evaluating studies that utilized noncontrast CT to determine the SFR (Matlaga et al., 8 Yang et al., 9 Cacciatore et al., 10 and the 3-month follow-up of Zhu et al. 11 ). This subanalysis confirmed that SA-RIRS maintained a significantly higher SFR even under the strictest imaging criteria (OR = 3.39, 95% CI: [2.18, 5.28], p < 0.001), with moderate heterogeneity (I2 = 45%) (Fig. 4).
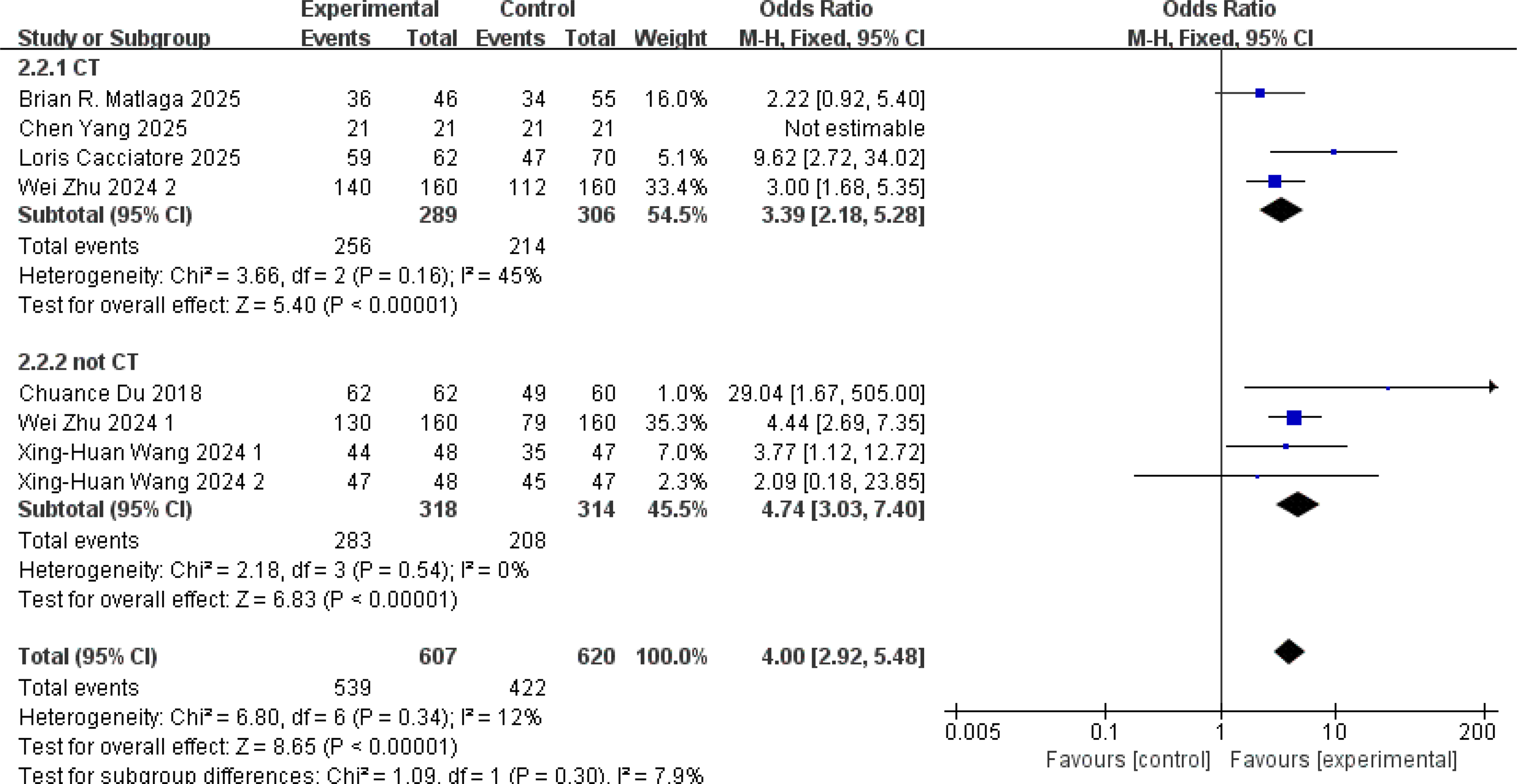
Forest plot of stone-free rate (CT-based vs non-CT-based assessment).
Operative time
Mean operative time ranged from 25.3 to 66.0 minutes across the included studies. Pooled analysis showed no significant difference between SA-RIRS and traditional RIRS (MD = −6.55 minutes, 95% CI [−16.23, 3.12], p = 0.18), with high heterogeneity (I2 = 96%, p < 0.001) (Fig. 5). Subgroup analysis confirmed the absence of significant differences for both suction catheters (MD = −4.88 minutes, 95% CI [−15.42, 5.66], p = 0.36; I2 = 78%) and suction sheaths (MD = −8.18 minutes, 95% CI [−29.15, 12.80], p = 0.44; I2 = 98%). Heterogeneity was primarily driven by learning curve effects, as reported by Matlaga et al., 8 and differences in stone burden, as noted by Zhu et al. 11
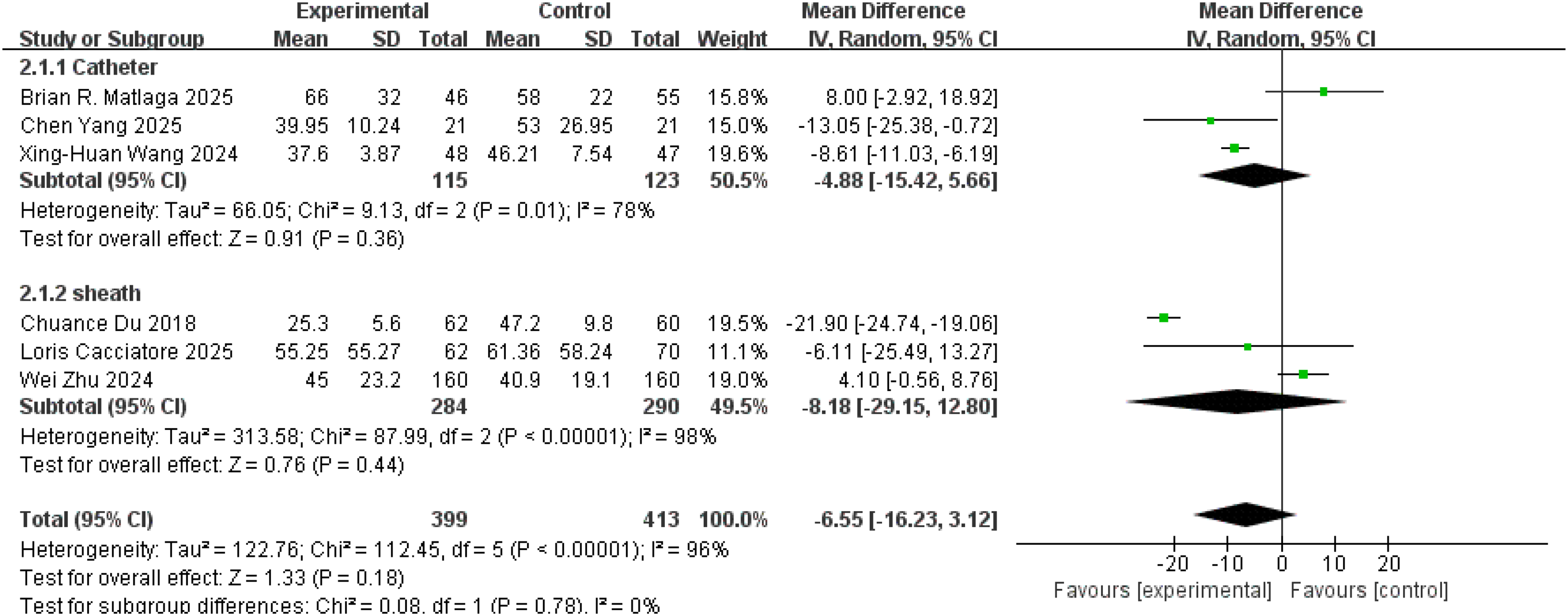
Forest plot of operative time.
Total complications
Six RCTs (n = 822 patients) reported total complication rates. SA-RIRS significantly reduced complications compared with traditional RIRS (OR = 0.40, 95% CI: [0.17, 0.97], p = 0.04), although with high heterogeneity (I2 = 70%, p = 0.005) (Fig. 6). Subgroup analysis indicated that suction sheaths were associated with significantly lower complication rates (OR = 0.27, p < 0.001, I2 = 4%), driven by reductions in postoperative fever and ureteral injury, whereas suction catheters showed no significant difference (OR = 0.77, p = 0.71). Most complications were mild (Clavien–Dindo I/II), including transient hematuria and low-grade fever, whereas severe complications (Clavien–Dindo III/IV) were rare (0.6%). For a detailed view, refer to Supplementary Table S2.
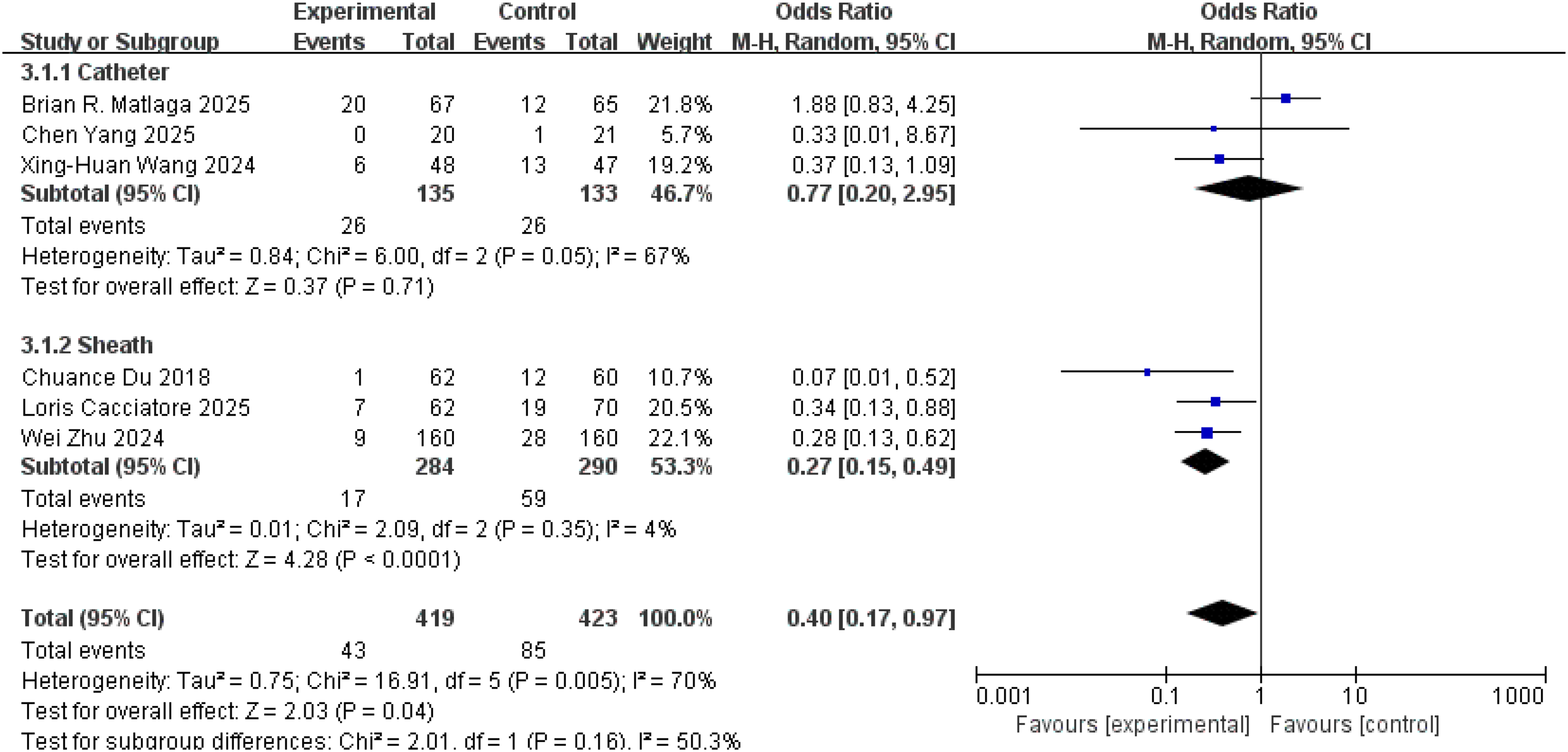
Forest plot of total complications.
Secondary outcomes
Hospital stay, reported in four studies, averaged 2.0–4.5 days and did not differ significantly between groups (MD = −0.05 days, p = 0.49, I2 = 0%) (Fig. 7A). Reoperation rates, reported in three studies, showed a nonsignificant trend toward reduction in the SA-RIRS group (OR = 0.28, p = 0.06) (Fig. 7B). Stone retropulsion, assessed in two studies, was significantly lower with SA-RIRS (OR = 0.26, p = 0.03, I2 = 0%) (Fig. 7C). Similarly, stone basket use, reported in two studies, was markedly reduced in SA-RIRS (OR = 0.01, p < 0.001) (Fig. 7D). Laser time, reported in two studies, showed no significant difference between groups (MD = −3.02 minutes, p = 0.37) (Fig. 7E).
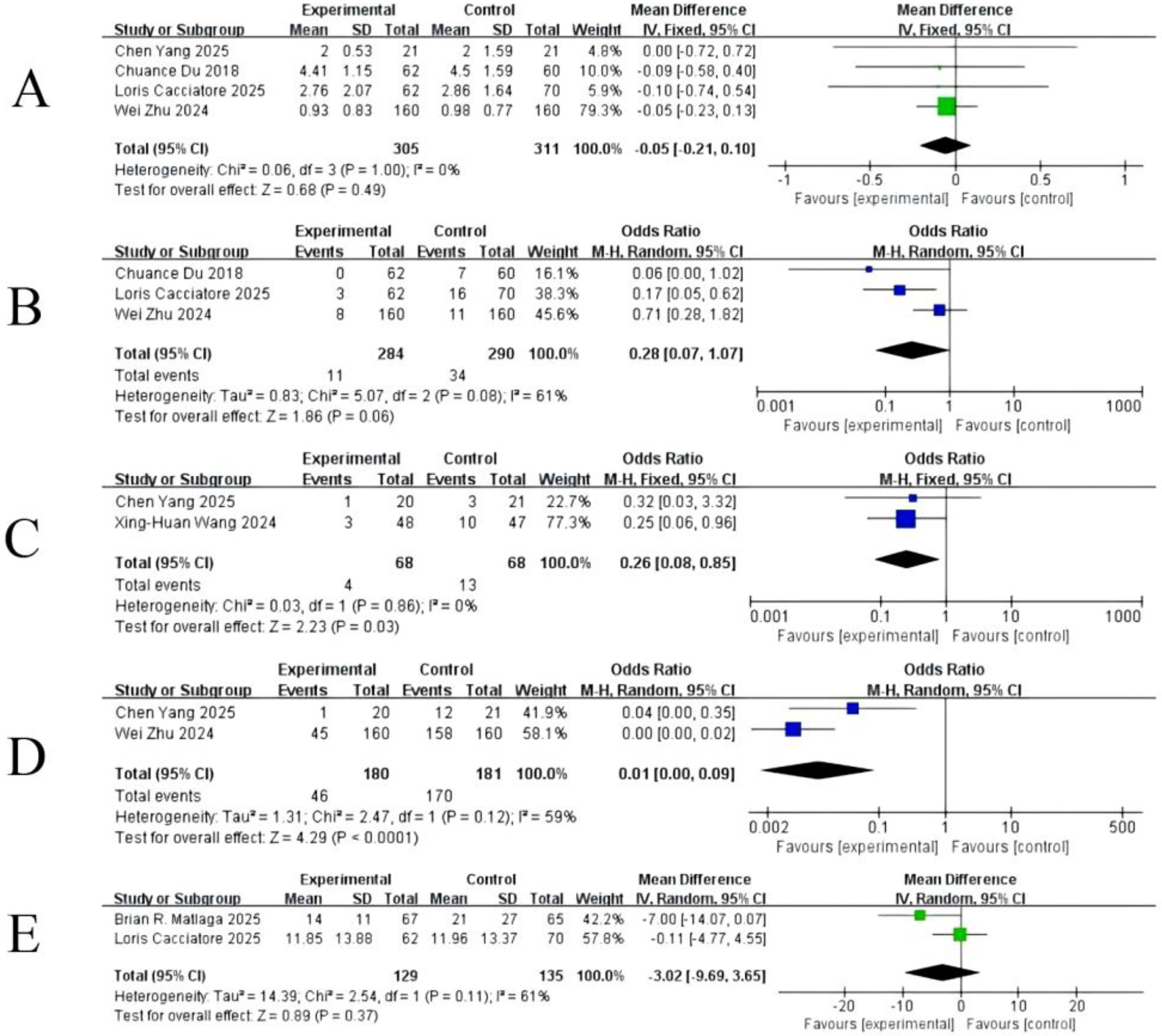
Forest plot of secondary outcomes.
GRADE evidence assessment
The certainty of evidence was rated high for all outcomes (Table 2). No downgrading was applied for RoB, as performance bias was unavoidable because of device visibility, whereas other domains were low or unclear risk. Inconsistency was explainable by differences in device type and stone burden. Indirectness was minimal, as all studies involved RIRS-eligible stones (≤2 cm). Imprecision was not a concern, with adequate sample sizes and CIs that did not cross the null for key outcomes such as SFR, complications, and retropulsion.
GRADE Evidence Profile for Key Outcomes of Suction-Assisted Retrograde Intrarenal Surgery vs Conventional Retrograde Intrarenal Surgery for Upper Urinary Tract Stones (≤2 cm)
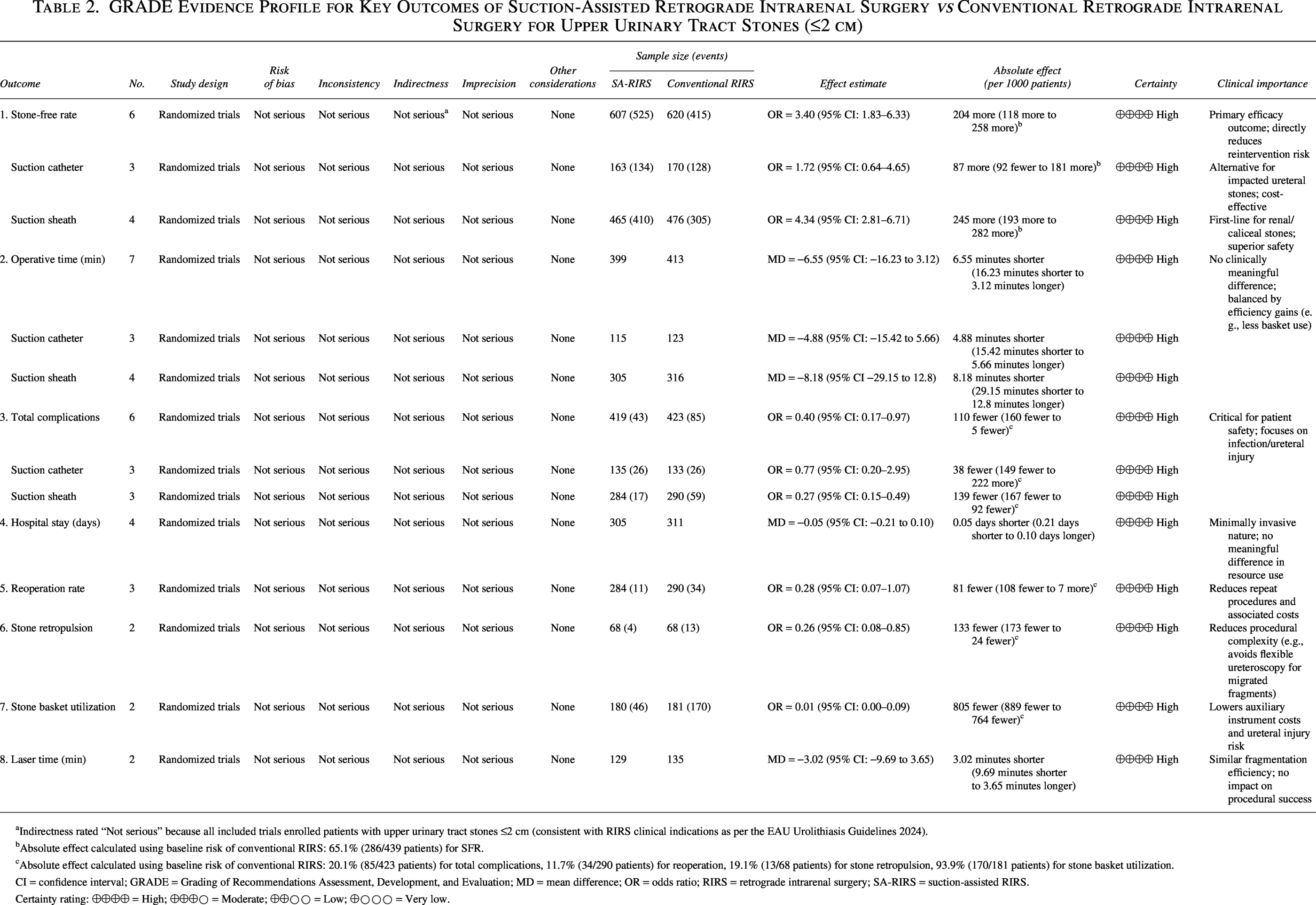
aIndirectness rated “Not serious” because all included trials enrolled patients with upper urinary tract stones ≤2 cm (consistent with RIRS clinical indications as per the EAU Urolithiasis Guidelines 2024).
bAbsolute effect calculated using baseline risk of conventional RIRS: 65.1% (286/439 patients) for SFR.
cAbsolute effect calculated using baseline risk of conventional RIRS: 20.1% (85/423 patients) for total complications, 11.7% (34/290 patients) for reoperation, 19.1% (13/68 patients) for stone retropulsion, 93.9% (170/181 patients) for stone basket utilization.
CI = confidence interval; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; MD = mean difference; OR = odds ratio; RIRS = retrograde intrarenal surgery; SA-RIRS = suction-assisted RIRS.
Certainty rating: ⨁⨁⨁⨁ = High; ⨁⨁⨁○ = Moderate; ⨁⨁○○ = Low; ⨁○○○ = Very low.
Publication bias
Publication bias was assessed using funnel plots for all analyzed outcomes. Visual inspection of the funnel plots for the primary outcomes, including SFR and operative time, revealed a roughly symmetrical distribution of the data points around the effect estimate lines, suggesting no obvious publication bias among the included studies. The funnel plots for all outcome indicators are available in Supplementary Material (Supplementary Figures S1, S2, S3, S4, S5, S6, S7, and S8).
Discussion
This meta-analysis of six high-quality RCTs confirms that SA-RIRS improves key clinical outcomes in the treatment of urolithiasis, with notable differences between suction catheters and suction sheaths.7–12 Overall, SA-RIRS significantly enhanced SFRs and reduced complication rates compared with traditional RIRS, addressing the most pressing limitations of the conventional approach. The 4.0-fold higher odds of achieving SFR with SA-RIRS are largely attributable to continuous debris clearance, which maintains endoscopic visibility and prevents fragment migration—an important clinical benefit given that RFs >2 mm increase the risk of reintervention by 9-fold. 6 Safety benefits were also evident, with a 60% reduction in complication odds (OR = 0.40), primarily because of improved IRP control. Elevated IRP (>30 mm Hg) is a well-established driver of postoperative urosepsis, 5 and suction devices—particularly sheaths—maintain IRP below 20 mm Hg.11,12 Although operative time did not differ significantly overall, SA-RIRS reduced stone basket use (OR = 0.01) and stone retropulsion (OR = 0.26), both of which simplify procedures and reduce surgeon fatigue.
Subgroup analysis revealed that although both devices significantly improved clearance, suction sheaths outperformed suction catheters in both SFR (OR = 4.46 vs 2.64) and complication reduction (OR = 0.27 vs 0.77). This superiority is explained by their design: larger lumens (10–14F) enable continuous negative pressure (−80 to −120 mm Hg), preventing pyelovenous backflow and endotoxin translocation; tip-bendable designs allow access to lower and middle calices, which is critical for stones in hard-to-reach locations; and compatibility with flexible ureteroscopes permits simultaneous lithotripsy and suction without repeated scope removal. In contrast, catheters have smaller lumens (1.2–11.9F) that are prone to clogging, limited caliceal access because of semirigid construction, and often require alternating scope removal for fragment extraction, which increases IRP variability. Nevertheless, suction catheters retain value in specific scenarios, such as impacted upper ureteral stones, where targeted suction can yield high early clearance rates, as demonstrated by Wang et al. 7 (1-day SFR 91.7% vs 74.5%). Device selection should therefore be tailored to stone location, with sheaths preferred for renal and caliceal stones and catheters for ureteral stones.
A critical factor in interpreting these results is the heterogeneity in imaging modalities used to determine SFR across the trials. To address this limitation, we conducted a subanalysis specifically evaluating studies that utilized noncontrast CT—the gold standard for detecting RFs.8–11 This subanalysis confirmed that even under the strictest imaging criterion, suction-assisted devices maintained superior clearance efficacy (OR = 3.39).
Furthermore, it is important to highlight that suction-assisted endourology is a rapidly evolving field. New suction-assisted ureteral access sheaths are continuously becoming available in a variety of diameters and lengths, alongside the advent of novel digital ureteroscopes. 21 Consequently, future studies will need to move beyond simple efficacy comparisons and investigate the ideal combinations of specific ureteroscopes and suction sheaths to optimize IRP, flow dynamics, and stone clearance.
In addition, readers—particularly those outside of North America—should note a critical distinction regarding the devices analyzed in this review. The trials included in our meta-analysis evaluated the first-generation CVAC aspiration system, 8 which is a stand-alone steerable suction catheter. Recently, the second-generation CVAC 2.0 system has been introduced. 22 Unlike its predecessor, the CVAC 2.0 is a single-use flexible ureteroscope (11.9F) that features integrated, simultaneous irrigation and aspiration channels. Recent prospective multicenter studies (e.g., Ballantyne et al. 22 and Cabo et al. 23 ) have demonstrated that the CVAC 2.0 system is highly effective for high-volume stone disease, achieving over 98% relative stone volume reduction. Because the currently available data on CVAC 2.0 consist of prospective observational cohorts rather than RCTs comparing it with conventional RIRS, it was not included in our primary meta-analysis. However, this second-generation technology represents a significant leap forward by merging the benefits of direct vision with continuous suction, and it will likely play a major role in the future standard of care for complex urolithiasis.22,23
Cost-effectiveness is a critical consideration for clinical adoption. Although SA-RIRS requires upfront investment in suction devices, long-term savings are substantial. Reduced auxiliary instrument use—particularly stone baskets, which cost $500–$1000 per case—can yield savings of approximately $450 per procedure, 7 with Zhu et al. 11 reporting basket use in only 28.1% of S-UAS cases vs 98.6% in traditional RIRS. Lower reoperation rates further contribute to savings, as repeat procedures cost around $5000 each; Du et al. 12 reported no reoperations in SA-RIRS compared with 11.7% in traditional RIRS. In addition, reductions in postoperative fever and urosepsis—conditions that increase hospital costs by roughly $3000 per case—translate into meaningful economic benefits.11,12 Although suction sheaths are slightly more expensive per unit ($100–$200) than catheters ($100–$150), their higher efficacy offsets this difference, making them the preferred choice for renal stones.7,12 In resource-limited settings, catheters may represent a cost-effective alternative for ureteral stones.
Several limitations should be acknowledged. Although the overall heterogeneity for SFR was low in the updated analysis (I2 = 12%), high heterogeneity remained in operative time (I2 = 96%), which was driven by differences in device design, learning curves, and initial stone burden. This underscores the need for standardized reporting according to the Journal of Endourology guidelines (Grade A: no RFs; Grade B: RF ≤2 mm; Grade C: RF 2.1–4 mm). 24 Most included studies had short follow-up periods (≤1 month), limiting assessment of long-term complications such as ureteral stricture and stone recurrence. Generalizability is constrained by the absence of trials from low-income countries, where device availability and cost may hinder adoption. Economic outcomes were reported in only three studies, restricting the robustness of cost-effectiveness analyses.7,11,12
Future research should prioritize head-to-head RCTs directly comparing suction sheaths and catheters for specific stone locations, long-term safety, and recurrence data with follow-up beyond 5 years, and studies evaluating the integration of novel laser technologies such as TFL, which produces finer dust (<150 μm) and may enhance suction efficiency. 23 Moreover, cost-effectiveness analyses in low-resource settings are essential to guide device selection and optimize global accessibility, with potential emphasis on reusable suction catheters.
Clinical Implications
The findings of this meta-analysis provide clear guidance for clinical practice. SA-RIRS should be considered the preferred approach for upper urinary tract stones ≤2 cm, particularly when using suction sheath systems for renal and caliceal stones, as they deliver the highest clearance rates and lower complication risks. Suction catheters also significantly improve clearance and remain a valuable option for impacted ureteral stones, offering targeted aspiration in anatomically constrained settings. Incorporating SA-RIRS into routine practice can reduce reliance on costly auxiliary instruments, minimize postoperative complications, and potentially shorten the learning curve for complex stone cases. Widespread adoption, guided by stone location and resource availability, has the potential to improve patient outcomes while optimizing health care resource utilization.
Conclusions
This meta-analysis of six high-quality RCTs demonstrates that SA-RIRS offers clear clinical advantages over conventional RIRS for upper urinary tract stones ≤2 cm. By integrating active aspiration, SA-RIRS significantly increases SFRs and reduces complications. Both suction sheaths and catheters improve clearance outcomes, with suction sheaths providing superior overall results for renal and caliceal stones, and suction catheters serving as an efficacious, cost-effective option for impacted ureteral stones. These benefits—driven by improved IRP control, enhanced fragment clearance, and reduced auxiliary instrument use—translate into meaningful economic savings and support broader adoption across diverse health care settings. Future studies should prioritize standardized outcome definitions, long-term safety and recurrence data, and direct head-to-head comparisons of sheath- and catheter-based systems to refine patient selection and optimize global accessibility. Our findings support the integration of SA-RIRS, particularly sheath-based systems, into routine endourological practice as a standard of care for appropriately selected patients.
Authors’ Contributions
Y.L.: Conceptualization (equal), data curation (lead), formal analysis (lead), writing—original draft (equal), and writing—review and editing (equal). H.W.: Conceptualization (equal), data curation (lead), formal analysis (equal), writing—original draft (equal), and writing—review and editing (equal). Z.Z.: Data curation (equal), methodology (supporting), and writing—review and editing (supporting). Y.Z.: Methodology (equal), supervision (equal), and writing—review and editing (equal). H.Z.: Conceptualization (supporting), supervision (lead), and writing—review and editing (equal). All the authors read and approved the final article.
Footnotes
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
No external funding was received for this study.
Availability of Data and Materials
The datasets used are available from the corresponding author upon reasonable request.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.