
Abstract
Purpose:
To evaluate the clinical impact of the ratio of endoscope–sheath diameter (RESD) on postoperative infectious complications after retrograde intrarenal surgery (RIRS) and to assess whether a prespecified RESD threshold of 0.85 provides better risk discrimination than the conventional target (<0.75).
Materials and Methods:
We retrospectively evaluated consecutive adults who underwent RIRS at two academic institutions. The RESD was defined as the outer diameter of the ureteroscope divided by the inner diameter of the ureteral access sheath (UAS). The primary outcome was postoperative infectious complications graded according to the Clavien–Dindo classification. Infection rates were assessed across ordered RESD categories (<0.75, 0.75 to <0.85, and >0.85), with a p for trend from ordinal logistic regression, and compared using prespecified dichotomous thresholds (0.75 and 0.85). Predictors of infectious complications were assessed using univariable and prespecified multivariable Firth’s penalized logistic regression.
Results:
Among the 243 patients, 20 (8.2%) experienced infectious complications. Infection rates increased stepwise across RESD categories (<0.75, 0.75 to <0.85, and >0.85; 2.6%, 4.6%, and 14.6%, respectively; p for trend = 0.009). Using the prespecified 0.85 threshold, infection occurred in 14.6% (14/96) of patients with RESD >0.85 vs 4.1% (6/147) with RESD ≤0.85 (p = 0.007), whereas dichotomization at 0.75 did not significantly discriminate infection risk (2.6% [1/39] vs 9.3% [19/204]; p = 0.214). In multivariable Firth’s penalized logistic regression, both RESD >0.85 (adjusted odds ratio [aOR] 3.73, 95% confidence interval [CI] 1.41–9.88; p = 0.008) and positive stone culture (aOR 3.50, 95% CI 1.33–9.22; p = 0.011) remained independently associated with infectious complications.
Conclusions:
RESD >0.85 was independently associated with post-RIRS infectious complications. A threshold of 0.85 provided more clinically useful risk stratification than the conventional RESD <0.75 target, while highlighting the importance of infected stone assessment.
Introduction
Retrograde intrarenal surgery (RIRS) is routinely performed to manage renal and proximal ureteral stones, and is supported by advancements in the flexible ureteroscopy, laser technology, and ureteral access sheath (UAS) systems. 1 Although RIRS is generally safe, postoperative infectious complications, ranging from febrile urinary tract infection (UTI) to sepsis, remain a common, clinically significant problem.2,3 Risk factors for post-RIRS infection include stone burden, operative time, preoperative urine culture, comorbidities, and intrarenal pressure (IRP).4,5 In addition to these established factors, a recent comprehensive machine-learning-based study by Senel et al. has highlighted that the presence of hydronephrosis, a history of postureteroscopy UTI, and an elevated preoperative urine leukocyte count are also significant independent predictors of febrile UTI following RIRS. 6 IRP is notable because it is intraoperatively modifiable. Continuous irrigation is required for visualization and can improve efficiency and shorten operative time, which may reduce infection risk; however, it potentially increases IRP and facilitates bacterial translocation. 7 Balancing efficiency and pressure control is critical, and this is mediated by the outflow resistance from the collecting system. 8
In current practice, UAS provides a dedicated outflow pathway and may mitigate IRP elevation; however, effective drainage depends on the annular space between the ureteroscope and the sheath. 9 The ratio of endoscope–sheath diameter (RESD) is a simple, clinically applicable metric that reflects this relationship and can be adjusted by selecting different scope–sheath combinations. 10 Although lower RESD thresholds (e.g., RESD <0.75) were proposed in ex vivo and in vivo animal studies,10,11 such thresholds may be difficult to achieve in clinical practice, particularly in cases with complex stones in which visualization, maneuverability, and scope–sheath selection must be balanced.
Clinically applicable thresholds are required to guide intraoperative outflow-resistance management. In this two-institution, retrospective cohort study, we evaluated the association between RESD and post-RIRS infectious complications. Considering the limited feasibility of extremely low RESD targets (e.g., <0.75) in routine practice, we examined whether a prespecified RESD <0.85 was clinically informative for intraoperative decision-making.
Materials and Methods
Ethics statement
This study adhered to the principles set forth in the Declaration of Helsinki and was approved by the institutional review boards of Kangdong Sacred Heart Hospital (2025-12-008) and Gangneung Asan Hospital (2021-08-001), with a waiver of informed consent owing to the retrospective design and use of deidentified data.
Participants
Patients (≥19 years) undergoing RIRS at two institutions between June 2020 and December 2024 were enrolled. To standardize fluid dynamics and minimize intersurgeon variability, the cohort was strictly limited to procedures performed by a single experienced endourologist using an automated irrigation pump. The exclusion criteria included the following: (1) failure of UAS insertion, (2) kidney transplant, (3) active preoperative infection refractory to appropriate antibiotics, (4) use of suction UAS, and (5) incomplete records.
Clinical parameters
The clinical variables included demographics, perioperative factors, and stone characteristics. Outflow resistance was assessed using the RESD, which was calculated as the outer diameter of the ureteroscope divided by the inner diameter of the UAS. RESD was analyzed using prespecified thresholds (≤0.75 vs >0.75 and ≤0.85 vs >0.85). The primary endpoint was the incidence of postoperative infectious complications. Events were assessed during the postoperative hospital stay (most patients were discharged on postoperative day 1 [POD 1]) and at the first postoperative outpatient visit (PODs 7–21), which served as a predefined surveillance window. Overall complications were graded using the Clavien–Dindo classification. 12
Postoperative infectious complications were defined by the occurrence of at least two of the systemic inflammatory response syndrome (SIRS) criteria: (1) temperature >38.0°C or <36.0°C, (2) leukocyte count >12,000 or <4000 cells/μL, (3) heart rate >90 beats/minute, or (4) respiratory rate >20 breaths/minute. Urosepsis was defined as the presence of a UTI together with SIRS, or the presence of at least two criteria of the quick sepsis-related organ failure assessment: (1) respiratory rate ≥22 breaths/minute, (2) systolic blood pressure ≤100 mm Hg, or (3) altered consciousness (Glasgow Coma Scale score <13). 13
Stone-free status was assessed using kidney, ureter, and bladder radiography and noncontrast CT at 3 months (2-mm slices) and reported according to the Journal of Endourology criteria (Grade A: no stone; Grade B: Grade A plus ≤2-mm fragments; Grade C: Grade A and B plus 2.1–4 mm fragments; not stone free: >4-mm fragments). As residual stones were recorded as none, ≤4 mm, or >4 mm in our database, Grades B (≤2 mm) and C (2.1–4 mm) were indistinguishable and therefore reported as “≤4-mm residual fragments (B/C combined).” Patients without 3-month imaging findings were excluded from the residual stone analyses.
Preoperative urine cultures were routinely obtained for all patients. Preoperative urine culture status was classified based on the initial culture obtained before a procedure; patients with an initially positive culture were categorized as culture-positive, even if subsequent cultures became sterile following appropriate antibiotic treatment. In cases of a positive urine culture, patients were treated with culture-specific susceptible antibiotics for 1 week before the operation. If susceptible oral antibiotics were not available, culture-directed parenteral antibiotics were administered via outpatient clinic visits or hospital admission before proceeding with the operation. In addition, a standardized perioperative prophylactic antibiotic regimen (e.g., intravenous third-generation cephalosporin) was uniformly administered to all patients approximately 30 minutes before surgical intervention, in accordance with the European Association of Urology guidelines. 14
Operative technique
All procedures were performed under general anesthesia by a single experienced endourologist (H.K.C.). RIRS was conducted using single-use digital flexible ureteroscopes (LithoVue™ [Boston Scientific, Marlborough, MA, USA] or L-scope [SEPLOU MEDICAL, Hangzhou, China]) with a UAS (10/12–14/16F) when feasible; the UAS size was selected intraoperatively based on retrograde pyelography (RGP). Continuous irrigation was delivered using an automated irrigation pump (IP-2000; Lagis®, Taichung, Taiwan), with settings adjusted according to intraoperative visibility and ensuring adequate outflow through the UAS. The baseline pump pressure was set at 50 mm Hg. To compensate for the decreased irrigation flow rate when instruments (e.g., laser fiber or stone basket) occupied the working channel of the ureteroscope, the pressure was transiently increased up to a maximum of 150 mm Hg to maintain adequate visibility. This pressure titration protocol was uniformly applied by a single surgeon across all cases. Holmium:YAG laser lithotripsy was performed using 200-μm fibers. A Double-J ureteral stent (4.8–6 F) was placed at procedure completion and typically removed on PODs 7–10 in routine practice; stenting was extended for up to 3 weeks in cases of clinically relevant ureteral injury.
To minimize IRP and enhance safety, a standardized irrigation protocol was used: (i) Outflow was confirmed as continuous and unobstructed through the UAS before laser activation; (ii) whenever endoscopic signs of outflow restriction (e.g., calyceal distention or mucosal whitening/petechiae) were observed, irrigation was stopped, and the scope was partially withdrawn to allow complete drainage; and (iii) prolonged working channel occupancy was avoided by timely fragment evacuation and basket retrieval.
Statistical analysis
Continuous variables are reported as mean ± standard deviation or median (interquartile range), and categorical variables as n (%). Between-group comparisons were performed using the Student’s t-test or Mann–Whitney U test for continuous variables, and the chi-square or Fisher’s exact test for categorical variables. For ordered categories (RESD group and 3-month residual stone burden), the p-value for trend was obtained by modeling the category as an ordinal variable in the logistic regression. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using logistic regression. To ensure a parsimonious multivariable model and prevent overfitting given the limited number of infectious events, the model was restricted to the two most critical predictors: RESD >0.85 and positive stone culture. Firth’s penalized logistic regression was then consistently used across all analyses to further correct for potential small-sample bias. Analyses were performed as complete case analyses, with additional adjustments for the study center in sensitivity analyses. All tests were two-sided, and p < 0.05 was considered statistically significant. Analyses were conducted using R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics and infectious complications
Among the 243 participants, 20 (8.2%) had postoperative infectious complications. Baseline characteristics are summarized in Table 1. Compared with the no-infection group, patients with infectious complications had a larger cumulative stone diameter (median 28.0 vs 15.0 mm; p = 0.009), were more likely to have multiple stones (100.0% vs 70.9%; p = 0.003), and tended to have a lower body mass index (median 23.1 vs 24.9 kg/m2; p = 0.050). The other baseline variables did not differ significantly between groups.
Baseline Characteristics of Patients with or without Infectious Complications after Retrograde Intrarenal Surgery (n = 243)
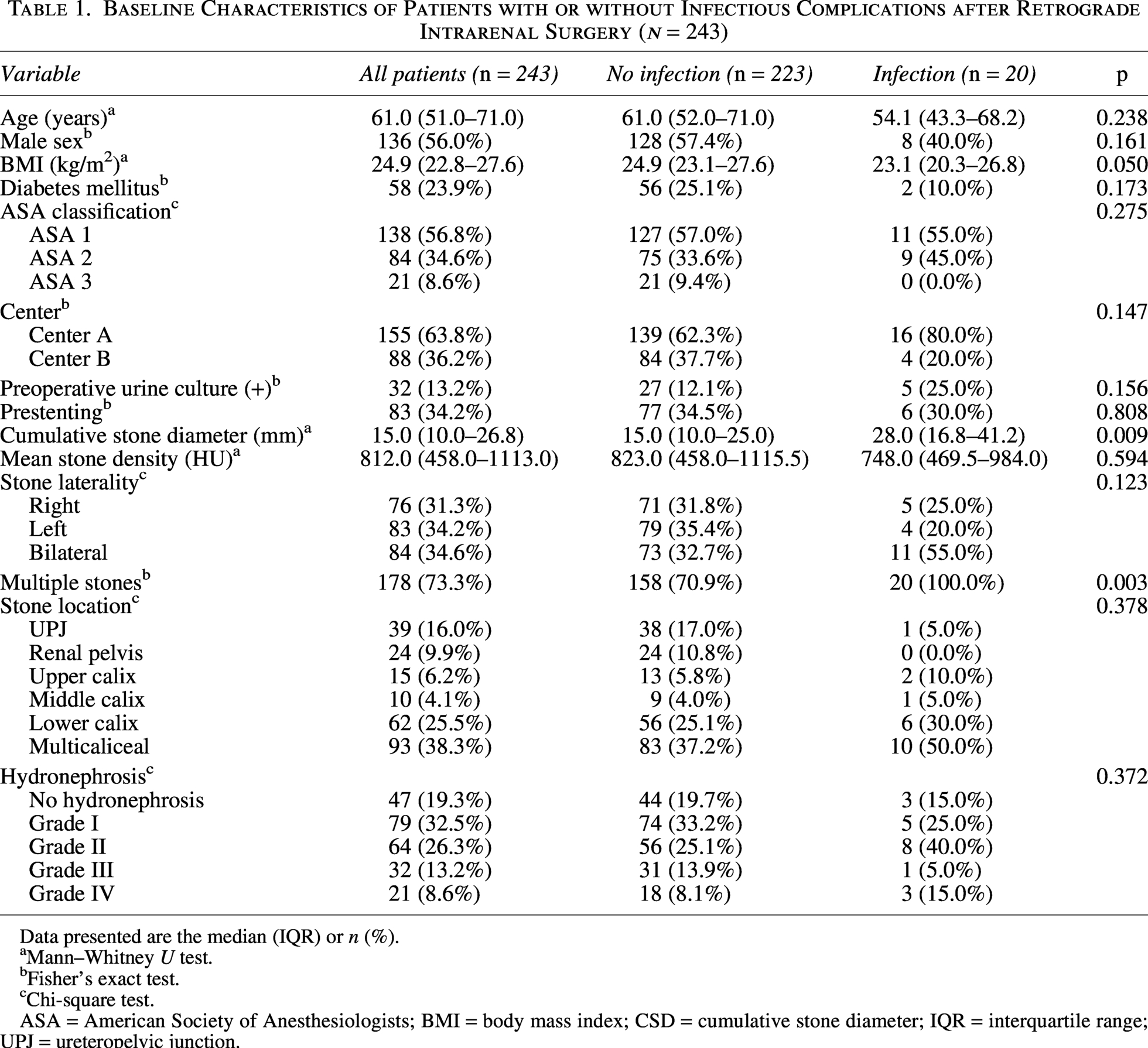
Data presented are the median (IQR) or n (%).
Mann–Whitney U test.
Fisher’s exact test.
Chi-square test.
ASA = American Society of Anesthesiologists; BMI = body mass index; CSD = cumulative stone diameter; IQR = interquartile range; UPJ = ureteropelvic junction.
Table 2 presents perioperative and postoperative data. Among the 20 infectious events, 2 (10.0%) resolved without antibiotics (Grade I), whereas 16 (80.0%) required antibiotics (Grade II). Two patients (10.0%) experienced septic shock requiring intensive care unit admission and vasopressor support (Grade IVa) but recovered and were discharged after clinical stabilization. Infectious complications increased stepwise across RESD categories (<0.75, 0.75 to <0.85, and >0.85; 2.6%, 4.6%, and 14.6%, respectively; p for trend = 0.009). Stone culture and composition differed between the groups, with higher positive culture rates (40.0% vs 15.7%, p = 0.012) and a higher proportion of struvite stones (55.0% vs 27.4%, p = 0.029) in the infection group. Three-month imaging data were available for 222 patients (21 [8.6%] were lost to follow-up) in the imaging-assessed cohort; infection rates increased with the residual stone burden (4.4% with Grade A, 11.5% with Grade B/C, and 23.1% without stone-free status; p for trend = 0.012). Additional analysis revealed no significant association between the size of the UAS and the incidence or grade of ureteral injury (p = 0.599).
Perioperative Data and Postoperative Complications
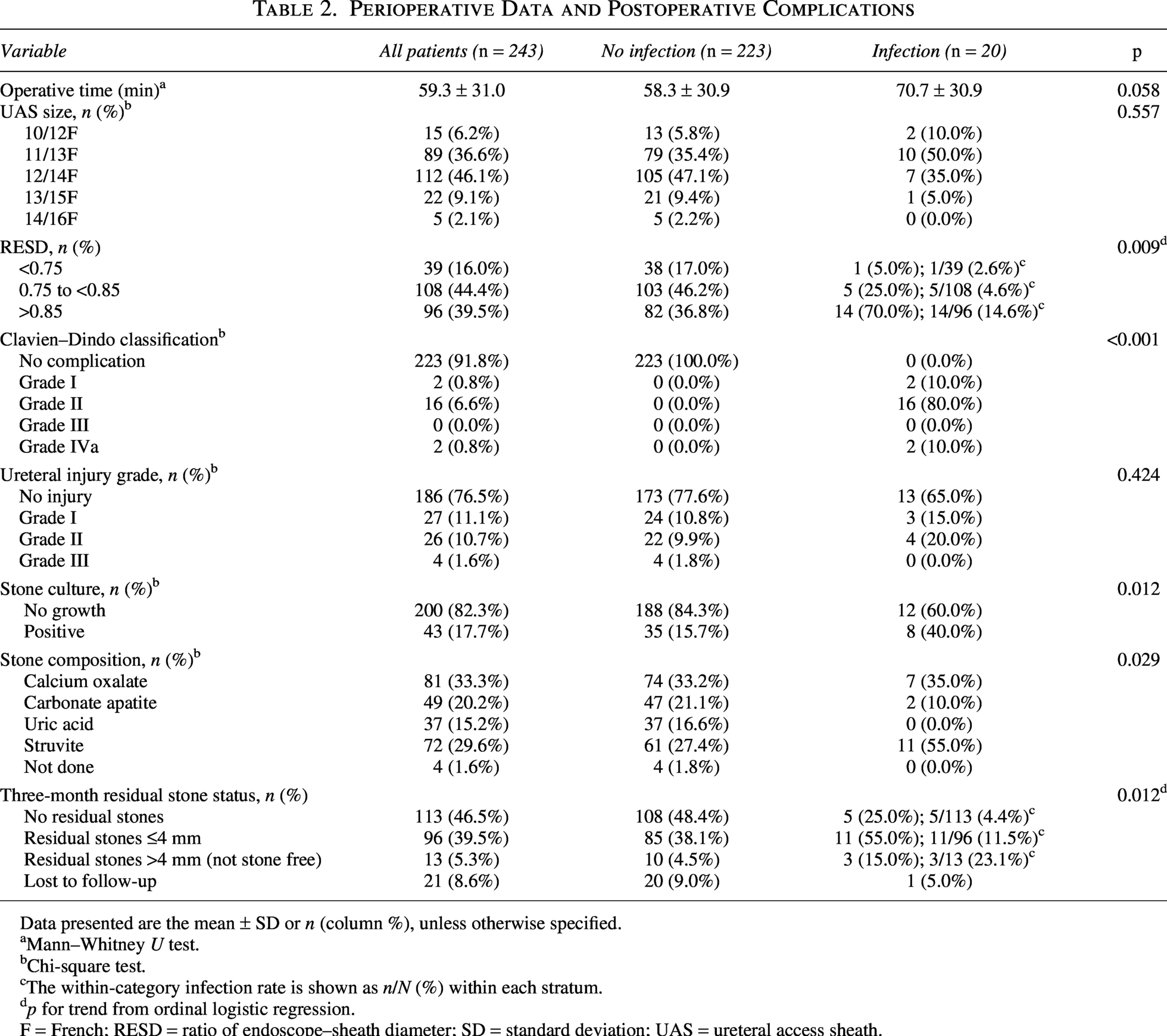
Data presented are the mean ± SD or n (column %), unless otherwise specified.
Mann–Whitney U test.
Chi-square test.
The within-category infection rate is shown as n/N (%) within each stratum.
p for trend from ordinal logistic regression.
F = French; RESD = ratio of endoscope–sheath diameter; SD = standard deviation; UAS = ureteral access sheath.
Comparison of RESD thresholds (0.85 vs 0.75)
Infection rates differed across prespecified RESD cutoff values (Table 3). When dichotomized at 0.85, infection occurred in 14.6% (14/96) and 4.1% (6/147) of those with RESD >0.85 and ≤0.85, respectively (Fisher’s exact p = 0.007). In contrast, when dichotomized at 0.75, infection occurred in 2.6% (1/39) and 9.3% (19/204) with RESD <0.75 and ≥0.75, respectively (Fisher’s exact p = 0.214); the <0.75 subgroup was small with only one event, which limits precision.
Infection Risk by Ratio of Endoscope–Sheath Diameter Thresholds (0.85 and 0.75)

CI = confidence interval; OR = odds ratio.
Univariable and multivariable Firth logistic regression analyses
Table 4 presents the results of the univariable and multivariable Firth logistic regression analyses for postoperative infectious complications. In the univariable analysis, RESD >0.85 (OR 3.83, 95% CI 1.45–10.07, p = 0.007), positive stone culture (OR 3.61, 95% CI 1.40–9.34, p = 0.008), and struvite stone composition (OR 3.20, 95% CI 1.28–7.97, p = 0.013) were significantly associated with infectious complications in the overall cohort (n = 243). In the imaging-assessed cohort (n = 222), 3-month residual stone status (non-Grade A) was also significantly associated with infectious complications (OR 3.00, 95% CI 1.08–8.34, p = 0.036).
Univariable and Multivariable Firth Logistic Regression Analyses for Infectious Complications
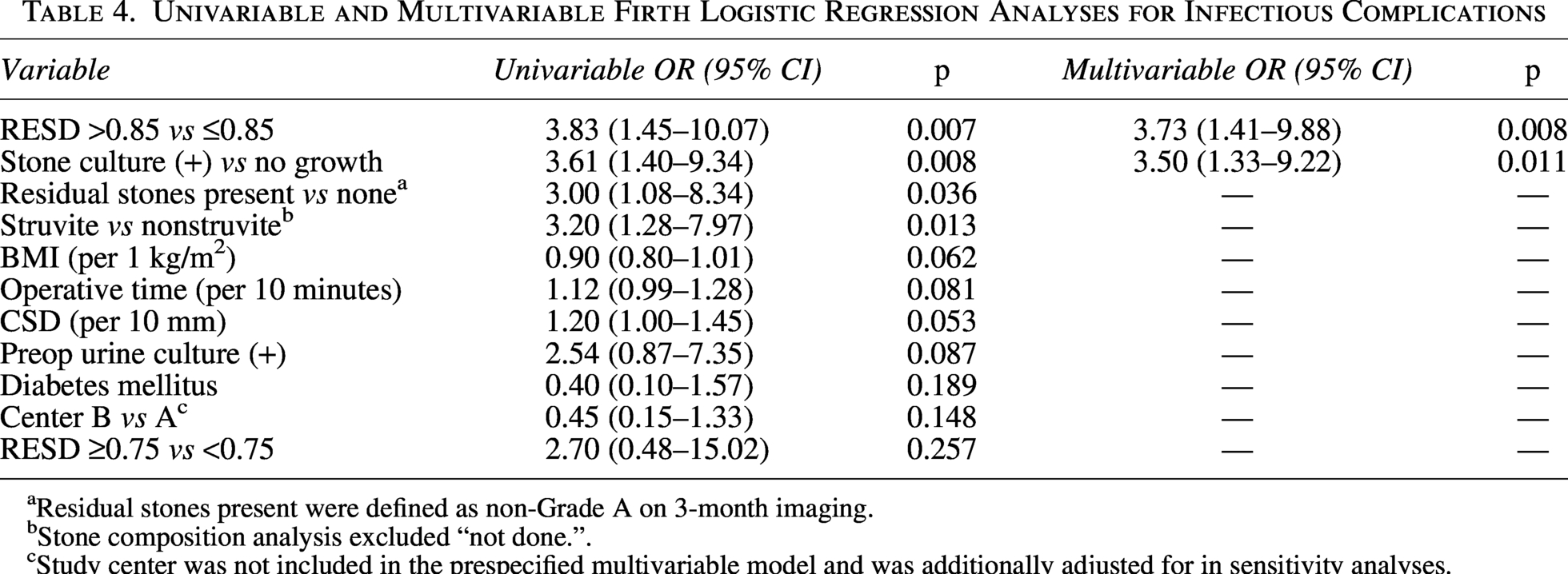
Residual stones present were defined as non-Grade A on 3-month imaging.
Stone composition analysis excluded “not done.”.
Study center was not included in the prespecified multivariable model and was additionally adjusted for in sensitivity analyses.
In the revised parsimonious multivariable model, both RESD >0.85 and positive stone culture remained independently associated with infectious complications (adjusted OR [aOR] 3.73, 95% CI 1.41–9.88, p = 0.008 and aOR 3.50, 95% CI 1.33–9.22, p = 0.011, respectively). In a sensitivity analysis additionally adjusting for the study center, these associations remained materially unchanged (aOR 3.80, 95% CI 1.44–10.03, p = 0.007 for RESD >0.85; aOR 3.19, 95% CI 1.21–8.44, p = 0.020 for positive stone culture).
Discussion
In this two-institution retrospective cohort, the 8.2% incidence of infectious complications was consistent with the previously reported range. 15 We demonstrated that a higher RESD was significantly associated with increased risk of postoperative infectious complications. An RESD threshold of 0.85 remained independently associated with infection after multivariable adjustment, which supports its utility as an intraoperatively modifiable surrogate of outflow resistance. However, the lower RESD target proposed in experimental settings (e.g., <0.75) lacked clear risk discrimination in this real-world cohort, likely reflecting limited feasibility and sparse events in the lowest RESD group.
Prior experimental work has frequently advocated extremely low RESD targets (e.g., ≤0.75) to preserve outflow and limit pressure elevation10,11; however, our findings suggest that clinically meaningful risk stratification may occur at a higher, more attainable threshold. A possible explanation is that intra-RIRS IRP is not a static consequence of the scope–sheath gap alone but is actively influenced by intraoperative maneuvers. We hypothesize that this compensatory mechanism creates a “clinical buffer zone” in which modest increases in outflow resistance are offset by dynamic decompression maneuvers. Our standardized irrigation workflow underscores the maintenance of unobstructed outflow and intermittent decompression, which potentially mitigates the pressure-related infection risk. Accordingly, a strict RESD <0.75 target showed limited discriminatory value, whereas an RESD <0.85 provided more clinically useful separation of infectious complications.
This interpretation is supported by a physical/simulation model by Oratis et al., who showed that IRP during ureteroscopy is governed not only by outflow resistance (related to the scope–sheath gap) but also by the frequency of ureteroscope withdrawal. 16 Their simulation demonstrated that the active removal of the endoscope constitutes a critical regulator of IRP. This plausibly explains why the slightly higher RESD of 0.85 remained clinically safe in our study. Clinically, the RESD potentially serves as a simple, intraoperatively modifiable indicator of outflow limitation to guide scope–sheath selection and outflow-oriented workflow. When a higher RESD is anticipated or encountered, intermittent decompression and avoidance of prolonged working channel occlusion may help balance visualization/efficiency with pressure control.
Although suction UAS was not used in our cohort, recent in vitro studies have provided a conceptually relevant framework for interpreting RESD. In an in vitro model using a suction UAS, Shi et al. reported that effective active drainage lowers IRP and recommended an RESD <0.85 to maintain a safe pressure range, suggesting the nonuniversality of the “≤0.75 rule” derived from passive outflow conditions. 17 Madden et al., in an in vitro evaluation of flexible vacuum-assisted UAS, reported that RESD alone does not predict aspiration/stone clearance performance and that outcomes depend on the aspiration technique (continuous in-sheath suction vs pull-out with suction). 18 Our clinical data extend these in vitro observations, in which an RESD threshold of 0.85 remained clinically informative even without a suction UAS.
These findings have practical implications for urologists. Using smaller caliber flexible ureteroscopes to satisfy a low RESD potentially reduces the working channel capacity and limits the use of ancillary devices, which could challenge lower pole access and fragment extraction in certain anatomies, 19 or larger access sheaths, conferring increased ureteral injury risk. 20 Our data suggest that an RESD threshold of 0.85 may be clinically useful when combined with an outflow-oriented intraoperative workflow. Therefore, a more attainable RESD threshold may reduce the tendency to overemphasize RESD reduction by either upsizing the UAS, potentially increasing the ureteral injury risk, or downsizing the ureteroscope, which can compromise the working channel function and make fragment handling more challenging. Overall, this threshold may facilitate a more practical scope–sheath selection that balances technical feasibility with ureteral safety in routine practice. Furthermore, we found no significant correlation between larger UAS sizes and ureteral injury rates in our cohort. This lack of correlation likely reflects our protocol of tailoring the UAS size to each patient’s ureteral anatomy assessed via RGP. Thus, our findings suggest that a pragmatic 0.85 RESD threshold, when combined with RGP-guided UAS selection, may serve as a safe clinical target without the unnecessary injury risk of forced sheath upsizing.
Another critical observation was the independent association between positive stone culture and infectious complications. In our parsimonious multivariable model, stone culture positivity remained a predictor of infection, alongside an RESD >0.85. This is consistent with previous reports suggesting that stone-level infection contributes meaningfully to postoperative risk, beyond intraoperative fluid dynamics alone.5,21 It is well established that urinary stones constitute a nidus for bacteria and endotoxins, and the fragmentation process releases these trapped pathogens. 22 Clinically, our findings suggest that intraoperative stone culture may help identify high-risk patients for whom close postoperative monitoring and culture-guided antimicrobial management are warranted.
Furthermore, the role of residual stones should not be overlooked. In our univariable analysis (and subset analysis of the imaging-assessed cohort), the presence of residual stones was significantly associated with higher odds of infection. Any remaining fragments can perpetuate the inflammatory process and serve as a reservoir for persistent bacteriuria. 22 Therefore, infection prevention should focus on a dual strategy: maintaining optimal outflow conditions through an appropriate RESD and achieving maximal stone clearance to eliminate the infectious nidus.
In our cohort, 10% of the infectious events (Clavien–Dindo Grade I) resolved with antipyretics alone. These self-limiting febrile episodes may represent transient endotoxin-mediated inflammatory responses related to stone manipulation and irrigation-driven backflow/absorption, rather than culture-proven bacterial infection. 23 We conservatively included these to capture all post-RIRS febrile events, underscoring the need for stricter microbiologic criteria in future studies.
This study had some limitations. First, the retrospective design and small sample size may reduce statistical precision. However, this limited volume reflects our strict criteria—restricting the cohort to single-surgeon, automated-pump, and nonsuction cases—designed to eliminate significant confounders related to fluid dynamics. Second, although a standardized surgical and perioperative protocol was applied, unmeasured interinstitutional differences may remain. However, additional adjustments for the study center in the sensitivity analyses did not materially change the conclusions. Third, residual stone status was determined on 3-month imaging, and incomplete follow-up required complete case analyses for models that included residual burden, which may introduce selection bias. Finally, although the irrigation pump pressure was strictly titrated (50–150 mm Hg) according to our protocol, we did not directly measure IRP during RIRS. Therefore, our explanations regarding the pressure-relieving mechanisms of dynamic scope maneuvers remain fundamentally speculative and rely on extrapolations from existing in vitro models. Further in vivo studies with real-time IRP monitoring are necessary to confirm these dynamics.
In an era of rapid technologic advances, we acknowledge that the clinical impact of RESD may diminish with the advent of suction access sheaths, real-time IRP monitoring system, or direct in-scope suction technology. 24 In these systems, active aspiration effectively manages fluid outflow, reducing the functional reliance on the passive scope–sheath gap. Nevertheless, as these advanced suction systems are not yet universally accessible because of economic constraints and varying institutional availability, the conventional UAS remains widely used. Therefore, our findings suggest a potential “surgeon factor”—indicating that postoperative infection risk may be influenced by outflow-oriented intraoperative decision-making. By considering a pragmatic 0.85 RESD threshold for scope–sheath selection and utilizing timely intermittent decompression, surgeons may further mitigate infection risks even when using conventional setups.
Conclusion
In this two-institution retrospective cohort study, RESD was associated with post-RIRS infectious complications. Compared with the conventional RESD <0.75 target, an RESD threshold of 0.85 provided a more clinically useful discrimination of infection risk. RESD >0.85 and positive stone culture were independently associated with infection, which underscores the need for outflow-oriented intraoperative management and clinical vigilance regarding stone-bound pathogens to reduce infectious complications.
Data Access Statement
All relevant data are within the article and its supporting information files.
Authors’ Contributions
H.K.C. contributed to the conceptualization and study design, and wrote the article. D.S., H.C.J., J.-Y.H., and D.Y.Y. contributed to the data acquisition, analysis, and interpretation. K.K. provided technical support, revised the article, conceived the original idea, supervised the project, and critically reviewed the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Research Foundation of Korea (NRF) funded by the Korean government (MSIT; grant no. RS-2023-00211456).