
Abstract
Background
Peritoneal dialysis (PD) and hemodialysis (HD) are both widely used as sole therapies for end-stage renal disease (ESRD). There is still controversy over which (if either) is superior in terms of patient outcomes. Peritoneal dialysis offers the advantages of long, slow, continuous ultrafiltration and potentially enhanced protection of residual renal function (RRF). In contrast, HD offers superior solute removal at the cost of undesirable cardiovascular tolerance of high rates of sodium and water removal. The aim of this study was to investigate the clinical feasibility of offering a combined treatment of both modalities [bimodal dialysis (BMD)] to incident patients reaching ESRD. We set out to investigate if it might be possible to utilize the intrinsic advantages of both modalities within a setting of good patient acceptability.
Methods
We prospectively studied 8 patients. They were recruited in the pre-ESRD phase from a specialist low clearance clinic. An arteriovenous fistula was formed and peritoneal catheters were inserted. The BMD consisted of 2, 3-hour, high efficiency, euvolemic HD sessions per week in combination with 2 PD exchanges per day to provide a degree of solute clearance and all of the ultrafiltration. Adequacy was measured independently for each modality. Patients were followed using the standard range of evaluations in addition to RRF (by creatinine clearance and EDTA clearance), echocardiography (left ventricular mass and ventricular performance), treatment outcomes, patient symptoms, and complications.
Results
Mean time on BMD was 346 ± 74.9 (range 245 – 431) days. Peritonitis rate was 21 months per episode (mean 0.6 ± 0.9, 0 – 2 episodes per patient). Mean peritoneal ultrafiltration volume was 1.58 ± 0.32 (1.3 – 2.1) L per day. Delivered Kt/V and weekly PD Kt/V did not change significantly. Patients’ RRF was maintained over the study period, as were serum albumin and control of serum phosphorus. Blood pressure was controlled with a reduction in the number of antihypertensive agents. Left ventricular mass index reduced over the treatment period, from a mean of 194 ± 31.2 (161 – 265) to 156 ± 21.2 (138 – 189) g/m2 (p = 0.05). Ventricular performance remained unchanged over the study [ejection fraction 50.4 ± 11.1 (38 – 67) % to 48 ± 8.0 (48 – 67) %]. Mean time during BMD spent on HD alone was 4.2 ± 6.9 (0 – 16) days, and on PD alone 9.2 ± 10.6 (0 – 25) days.
Conclusion
This study suggests that BMD is a feasible treatment for ESRD. It is associated with adequate solute removal and good hemodynamic/volume control, and allows increased treatment flexibility for coping with complications normally requiring recourse to unplanned HD with temporary central venous access.
Uncertainty exists concerning which mode of dialysis is associated with the best overall outcomes. There is considerable debate as to whether or nor there is a survival difference between hemodialysis (HD) and peritoneal dialysis (PD). In nondiabetic patients, mortality rates are similar for HD and PD (1,2), particularly in studies where mortality rates are adjusted to take into account the degree of comorbidity (3,4). Peritoneal dialysis does seem to confer a survival advantage for diabetic patients (1), although this benefit is not seen in elderly diabetics (2). Peritoneal dialysis may be preferred in the subgroup of patients with left ventricular ejection fractions of less than 35% (5).
Underdialysis has been established as a major predictor of reduced survival for both HD and PD (6). It is of concern that, in the absence of residual function, only a minority of PD patients are capable of reaching adequate levels of small molecule clearance, without the use of automated PD (7). The role of residual function, allowing both continuous solute clearance and fluid removal, is increasingly recognized to be of utmost importance. As a technique, PD allows slow continuous ultrafiltration, but less efficient solute removal. In contrast, HD allows highly efficient solute removal, but at the expense of interdialytic fluid overload and precipitous ultrafiltration. At present, most current innovations are directed at addressing these inadequacies by increasing the amount of the individual modality: increasing the amount of PD delivered to address its shortfall in solute removal, and increasing time on HD to partially replicate the slow ultrafiltration that PD allows. There are concerns regarding the escalating burden of therapy that such increasingly intensive treatments place on the patient.
The use of both modalities at the same time, which we term bimodal dialysis (BMD), allows partial separation of the two essential components of effective renal replacement therapy (RRT), fluid removal and solute clearance. Fluid removal is performed by PD. Solute removal can then be enhanced by the addition of high efficiency, euvolemic, short-time HD sessions. The total treatment load is similar to that experienced by a patient on a single modality as there is a reduced amount of each dialysis type. The only previous application of a combination of therapies has been in PD patients who have partially failed on that modality. The only published study, by Kawanishi (8), used combination therapy for a variety of indications (failure of both solute clearance and ultrafiltration), with the addition of HD to a continued full PD regime.
Bimodal dialysis aims to use both PD and HD in an optimized fashion, exploiting each technique's particular strengths within a setting of good patient acceptability. The potential benefits of such therapy might include good control of blood pressure, minimization of the increase in left ventricular mass (LVM), reduced need for potentially harmful antihypertensive medications, optimized preservation of residual renal function (RRF), all as a result of the maintenance of slow continuous peritoneal ultrafiltration. In addition to the increased flexibility in dialysis prescription, the seamless timeline can change, without the need to default to temporary central venous vascular access for HD, if problems with one modality are encountered, and there is increased patient acceptability (holidays, etc.). The aim of this study was to examine the feasibility of this approach in incident patients requiring dialysis.
Methods
Patients
The study was approved by the local Research Ethics Committee. Patients were recruited from an outpatient population approaching end-stage renal failure. Bimodal dialysis was offered to all patients meeting the inclusion criteria (all causes of ESRD, age 18 – 75 years, no transplant in situ) in predialysis counseling over a 6-month period in 2000. Eight patients elected to enter the study, giving informed consent. Initial consent was obtained well in advance of the dialysis commencing to allow time for formation of appropriate vascular access. The cohort of patients consisted of 1 female and 7 males, mean age 58.2 years (range 34 – 72 years). Five of the patients had diabetic nephropathy (4 type I, 1 type II diabetes), 1 patient had hypertensive nephrosclerosis, 1 patient had membranous glomerulonephritis, and 1 patient had small kidneys on presentation (presumed chronic glomerulonephritis). All patients had been under pre-end stage care with the nephrology service for at least 2 years prior to study. Patients were studied for at least a year.
Investigatory Protocol
Patients were followed in a specialist low clearance clinic and performed regular creatinine clearance measurements. Diabetic patients were commenced on RRT when creatinine clearance reached 15 mL/minute, and nondiabetic patients when it reached 10 mL/minute. This represents standard practice within our unit. All patients had had native arteriovenous fistulas fashioned prior to reaching end-stage disease. Hemodialysis was initiated first, with immediate insertion of the PD catheter. All catheters were inserted in the midline using a fluoroscopic percutaneous technique. Catheters were flushed immediately and PD commenced within 10 days.
Rrt Schedule
Hemodialysis was performed twice per week for 3-hour sessions. Hospal Integra dialysis monitors (Dasco, Mirandola, Italy) were used, with bicarbonate buffering. Dialysate sodium was set at 140 mmol/L and calcium at 1.25 mmol/L. Patients underwent high efficiency treatments using a dialysate flow rate of 750 mL/minute and a polysulfone high-flux dialyzer (Syntra 160; Baxter Healthcare, Thetford, Norfolk, UK). The treatments were euvolemic with no net ultrafiltration. All stations were connected to a central computer server. Dialysis prescriptions were held centrally and uploaded automatically on insertion of a patient-specific card into an appropriate reader on the Integra monitor. All monitors were equipped with on-line conductance monitoring (providing measurement of Kt/V and sodium flux), noninvasive blood pressure, and continual measurement of relative blood volume using a hemoglobin concentration-based system. These data, as well as standard “run sheet” type data, were downloaded at the end of each treatment to a patient-specific file for subsequent analysis.
Peritoneal dialysis was performed daily and consisted of 2 exchanges of 2 L to provide ultrafiltration and additional solute clearance. The strength of the bags was individualized as required to maintain desired weight. Initial prescription was two 1.36% glucose bags (Physioneal; Baxter), increasing to one 1.36% and one icodextrin bag (Extraneal; Baxter) and ultimately one 3.86% and one icodextrin bag, if necessary. Dwell times were also individualized to maximize overall ultrafiltration volumes. The PD schedule continued unchanged on HD days. Standard dietetic input was given to ensure a protein intake of 1 g/kg dry body weight/day and a daily sodium restriction of 100 mmol. Anemia was managed with subcutaneous epoetin and intravenous iron saccharate, aiming to maintain Hb > 10 g/dL.
Patient Monitoring
Patients underwent the standard monthly assessment of biochemical and hematological indices. Data were recorded on pre- and post-HD blood pressures, antihypertensive medication use, response to epoetin and doses, calcium/phosphate control, and hyperparathyroidism. In addition, RRF was followed by the use of creatinine clearance measurements (3 month intervals) and chromium EDTA radioisotope glomerular filtration rate (GFR) measurement at start of BMD, and at 6-month intervals thereafter. Transthoracic two-dimensional echocardiography was performed at 6-month intervals once target weight had been achieved with reference to clinical examination and relative blood volume monitoring. This was to provide information on both ventricular performance (ejection fraction) and ventricular dimensions, including LVM [calculated using the method of Devereux (9)]. All scans were performed on HD days, post treatment.
Dialysis adequacy was assessed by a variety of methods. Hemodialysis adequacy was measured monthly by the use of urea reduction. Postdialysis sampling took place 30 minutes after cessation of dialysis to allow for full urea rebound. Kt/V was calculated using the Daugirdas II method (10). Delivered Kt/V was also directly measured on each dialysis treatment using ionic dialysance measurements made automatically by the Diascan module installed in the dialysis monitor; V needs to be directly entered for this, and was calculated after Watson (11). Adequacy of PD was assessed every 6 months (starting 3 months after initiation). The PD Adequest 2.0 program (Baxter) was used to calculate the normalized protein catabolic rate, weekly Kt/V, weekly creatinine clearance, and RRF.
Patient symptoms were monitored by the use of a survey. This was administered at the start of BMD and at 6 and 12 months. Patients scored 9 questions from 0 – 5 (5 being best). These questions related to dyspnea at rest, dyspnea on exertion on the flat, fatigue, quality of sleep, appetite, dependent edema, cough, mood/depressed feelings, and overall level of well being / functional ability (maximum score 45).
Statistical Analysis
Paired observations were analyzed using the Wilcoxon rank sum test. All data were analyzed using GraphPad Prism, version 3.00, for Windows (GraphPad Software, San Diego, California, USA; www.graphpad.com). Where not otherwise stated, data are expressed as mean ± SEM (range).
Results
Clinical Course
Of the 8 patients recruited, only 6 were established on BMD (5 fully so). Two patients suffered initial drainage problems with their PD catheters and, despite a single attempt to reposition, both elected to remain fully on HD. One of the patients suffered thrombosis of his fistula after 2 months of combined treatment and, while awaiting further surgical access provision, chose to be established long term on continuous ambulatory PD (CAPD).
The mean time on combined treatment was 346.6 ± 74.9 (245 – 431) days for the remaining 5 patients. There were no other failures of vascular access within that time period. There was provision to spend time exclusively on one mode of dialysis for either medically imperative reasons or social choice (holidays, etc.). Three patients spent a period of time converted to full CAPD to allow foreign holidays without the restriction of attending a HD facility [mean 9.2 ± 10.6 (0 – 25) days on PD for the group as a whole]. Two patients spent time exclusively on HD. In both cases, this was a result of drainage problems with the PD catheter, pending successful reintroduction of the PD element of the BMD treatment [mean 4.2 ± 6.9 (0 – 16) days on HD for the group as a whole].
There were 3 episodes of peritonitis in 2 patients. Two of these were due to Staphylococcus epidermidis infection and one was a result of E. coli infection. They all resolved after treatment with intraperitoneal antibiotics and did not require removal of the PD catheters. This equated to a mean number of peritonitis episodes of 0.6 ± 0.9 (0 – 2) and a peritonitis rate of 1 per 21 months of treatment. These data are summarized in Table 1.
Time Spent on Bimodal Dialysis (BMD) and Peritonitis Rates
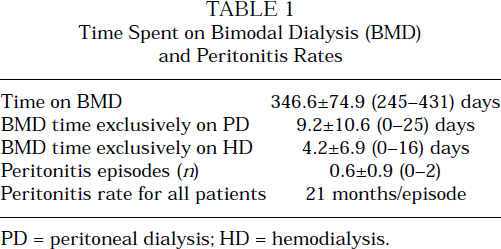
PD = peritoneal dialysis; HD = hemodialysis.
Patient symptoms improved over the study period. Mean score was 15.8 ± 0.95 at the start of the study, compared to 34.2 ± 2.6 (p = 0.002) at 12 months. Mean body weight did not increase significantly over the period of the study: 69.2 ± 5.5 (58 – 86) kg, and 70.4 ± 5.8 (57 –87) kg at the end of the study.
Dialysis Adequacy
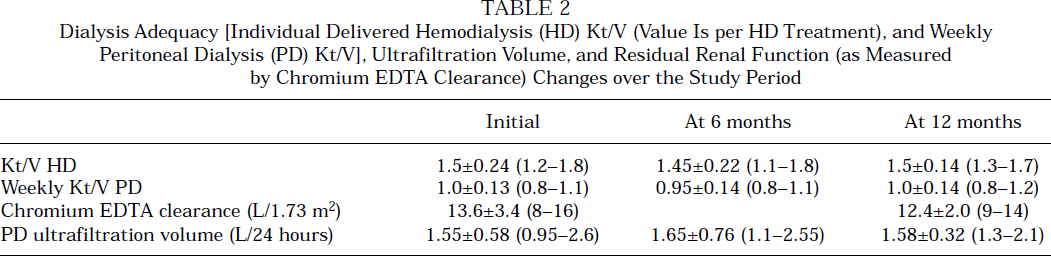
The mean delivered Kt/V on HD was 1.5 ± 0.24 (1.2 – 1.8) initially, and 1.45 ± 0.22 (1.1 – 1.8) and 1.5 ± 0.14 (1.3 – 1.7) at 6 and 12 months respectively. Two of the 6 patients who were established onto BMD required additional ultrafiltration during HD to reach and maintain their dry weight. Neither patient required this after the first 4 months of treatment. Only 2 patients required any additional ultrafiltration on HD, in less than 10% of treatments. Mean weekly Kt/V delivered by PD was 1.0 ± 0.13 (0.8 – 1.1) initially, and 0.95 ± 0.14 (0.8 – 1.1) and 1.0 ± 0.14 (0.8 – 1.2) at 6 and 12 months respectively. Four patients had high-average and 1 patient high peritoneal transport status. There was no significant change in peritoneal transport characteristics over the study period. All the patients achieved significant peritoneal ultrafiltration volumes. Mean daily volume was 1.55 ± 0.58 (0.95 – 2.6) L initially, and 1.65 ± 0.76 (1.1 – 2.55) L and 1.58 ± 0.32 (1.3 – 2.1) L at 6 and 12 months respectively. One patient achieved adequate ultrafiltration with the use of 1.36%-glucose bags alone. Three patients ultimately needed one 1.36% and one icodextrin exchange, and 1 patient required the addition of one 3.86% glucose exchange three times per week. All patients used an overnight dwell to achieve this level of ultrafiltration. The additional exchange used a mean dwell time of 7 ± 0.8 (5 – 10) hours. There was no statistically significant reduction in RRF over the study period, with mean EDTA GFR being 13.6 ± 3.4 (8 – 16) mL/minute at the start and 12.4 ± 2.0 (9 – 14) mL/minute at the end of the study period. These data are summarized in Table 2. Residual renal function contributed a significant degree of total clearance in all the patients: mean contribution by RRF (at the end of the study) was 50.7 ± 4.7 (37 – 68) %.
Dialysis Adequacy [Individual Delivered Hemodialysis (HD) Kt/V (Value Is per HD Treatment), and Weekly Peritoneal Dialysis (PD) Kt/V], Ultrafiltration Volume, and Residual Renal Function (as Measured by Chromium EDTA Clearance) Changes over the Study Period
Mean arterial blood pressure (MAP) control, although trending to a reduction over the study period, did not reach statistical significance. Mean MAP was 80.2 ± 9.4 (58 – 105) mmHg initially, and 74.8 ± 17.0 (55 – 94) mmHg and 72.6 ± 16.3 (56 – 91) mmHg at 6 and 12 months respectively. However, there was a reduction in antihypertensive medications required to achieve this: mean number of agents fell from 3.8 ± 0.8 (3 – 5) to 1.4 ± 0.5 (1 – 2), p = 0.04. Left ventricular mass index (LVMI) fell over the study period, from 194 ± 25.3 (161 – 265) g/m2 to 156 ± 21.2 (138 – 189) g/m2, p = 0.05. All the patients entering the study had left ventricular hypertrophy (LVH) (> 150 g/m2 adopted from the Framingham Study); at completion, only 2 patients met this criterion. There was no significant difference in mean hemoglobin concentration: from 11.3 ± 1.5 (9.7 – 13.4) g/dL to 11.4 ± 0.9 (9.9 – 12.1) g/dL. Ejection fraction was unchanged. Serum phosphate was also unchanged over the period; serum albumin was also largely preserved, with a mean of 27.4 ± 4.9 (21 – 33) g/L initially, and 28.0 ± 3.0 (24 – 32) g/L and 28.0 ± 2.8 (25 – 31) g/L at 6 and 12 months respectively (measured using a bromocresol purple-based method, normal range 30 – 38 g/L). These data are summarized in Table 3.
Cardiovascular and Biochemical Variables over Bimodal Dialysis (BMD) Study Period
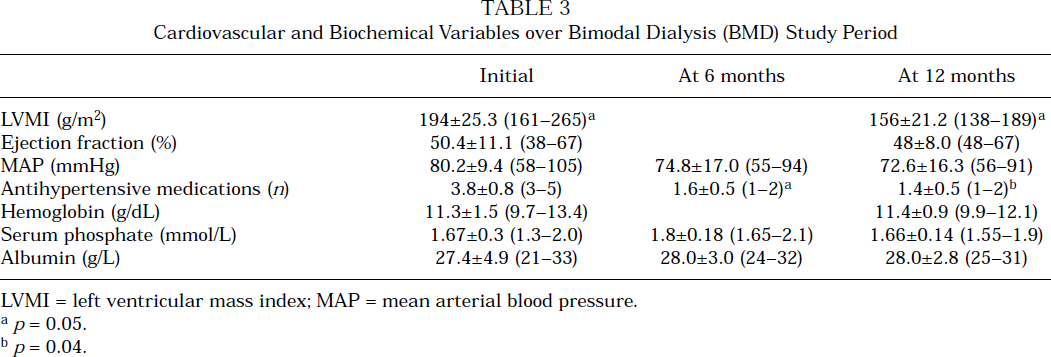
LVMI = left ventricular mass index; MAP = mean arterial blood pressure.
p = 0.05.
p = 0.04.
Discussion
This study demonstrates that BMD is a feasible form of RRT in patients new to ESRD. This is the first report of the use of combination therapy in incident patients. It appears to be capable of delivering adequate blood purification and control of blood pressure and LVH, and may be associated with preservation of RRF.
It was not possible to establish all of the initially enrolled patients onto BMD. The main barrier to this was complications with the access required for the dual therapy. The requirement for the formation of an arteriovenous fistula and insertion of a PD catheter is a potential shortcoming, exposing the patient to the possible complications of both. The scale of the difficulties encountered may in part have been related to the demographic characteristics of the patients in this initial pilot study, with the high proportion of diabetic patients. Highly dependent patients often lack the confidence to opt for community delivered therapy such as PD. The addition of a degree of hospital interaction with a reduced frequency of HD attendances might encourage a larger proportion to opt for a component of PD in BMD. This at least minimizes the impact of these patient numbers on often hard-pressed HD resources. The ability to convert between modalities is a potential benefit of BMD. The patients in this study did so, for both medical reasons (drainage problems) and social reasons (holidays without the need to be tethered to a HD unit). No patients in the study required temporary central venous access, with the attendant risks of line sepsis.
Peritonitis did not appear to be a significant problem. The peritonitis rate of 1 episode per 21 treatment months compares well with the standard set by the Renal Association of 1 episode per 18 months of treatment, although this was associated with half the normal number of daily PD exchanges. There were no confirmed episodes of sterile peritonitis associated with icodextrin use.
The only other published study of combination therapy was in patients who had failed PD and were then augmented with a degree of HD (1 HD treatment per week and continued on a full CAPD regime). The study by Kawanishi et al. contains no data on the proportional success of combining the therapies in these patients, but does describe 31 patients over a number of years (8). This implies that longer-term use is feasible. This is further backed up by two other small-scale studies (12,13) that were retrospective in nature and effectively surveyed patients who had been exposed to some form of combined dialysis treatment (again, all patients were converted from an initially established single treatment modality). Patient symptom scoring did demonstrate a marked improvement over the study period. Clearly, this was a somewhat limited assessment and did not have any controlled observations with patients on either modality alone to compare with.
The assessment of blood purification presented some difficulty. There are no data to determine what an adequate small molecule clearance would be with reference to currently accepted thresholds for the reduction of long-term mortality. We chose to assess the delivery of both modalities separately to provide a transparent picture of the relative contributions achievable with BMD. A further caution in an attempt to combine the adequacy measurements is that, during HD, patients were also receiving PD. This is in addition to the difficulty in robustly converting the high level of RRF into an equivalent degree of dialysis-achieved solute removal. The high RRF seen was a reflection of standard practice within our department for commencing RRT. Such an early start is a practice that is far from universal. However, it did provide significant RRF to meaningfully study the effect of BMD on this important determinant of overall patient outcome.
Delivery of solute clearance remained constant over the study period and would seem broadly comparable with current standards. Obviously, all of these patients retained a considerable degree of RRF, and it remains to be seen if the dialysis schedule (as delivered) would still be adequate in the anephric patient (RRF contributed about 50% of the calculated PD clearance over this study period). Obviously, the above methods consider only small molecule clearance. The combination of high-flux HD and PD should be associated with an attractive profile of middle molecule clearance, although this was not formally studied. Data were not collected on serum β2-microglobulin levels.
The PD component of BMD appeared capable of maintaining adequate ultrafiltration. Mean daily ultrafiltration volumes were around 1.5 L throughout the study period. The majority of patients achieved this without recourse to excessive exposure to hypertonic PD solutions. Only 1 patient needed intermittent combination of 3.86% glucose with icodextrin to maintain his dry weight. This requirement was largely in response to suboptimal compliance with prescribed limitation of fluid intake. In a CAPD regime alone, it is reasonable to expect the use of icodextrin would provide a sufficient degree of ultrafiltration in the majority of patients. However, with longer-term BMD treatment (associated with failing RRF) and the limitation of single daily icodextrin use, it is likely that additional high glucose concentration exchanges would be needed. This might require further adaptation of the PD and HD elements of BMD over the longer term to provide continued adequate ultrafiltration, potentially with the addition of some degree of ultrafiltration on HD. This would allow the possibility of enhancing long-term peritoneal function by reducing total glucose exposure with the possible effects on peritoneal membrane and structure.
Although the study was relatively short, there were no significant changes in peritoneal transport characteristics observed over the study period.
The apparent maintenance of RRF is of interest. In terms of maintenance of RRF, CAPD has been reported to be superior to HD using cuprophane-based dialysis membranes (14). This has been considered to be due largely to biocompatibility issues. Indeed, HD using synthetic dialysis membranes has been reported to be associated with a loss of RRF comparable to that seen with CAPD. In the present study, the apparent maintenance of RRF may be a consequence of both the biocompatible HD materials used and the euvolemic nature of the HD sessions. It could be speculated that a reduction in the hemodynamic insults associated with HD and ultrafiltration may assist in protecting RRF.
There is wide appreciation of the beneficial consequences of a continued degree of RRF (15). Patients treated with BMD certainly appeared to have good control of hypertension (with a reduction in the number of antihypertensive agents required) and improvements in LVMI as an index of longer-term salt and water overload. Clearly, it is difficult from this study to determine which of those benefits arose from the initiation of RRT, and which might be a more direct consequence of this particular dialysis strategy.
The limitation of glucose exposure compared to full PD may also have potential metabolic advantages by reducing exposure to high carbohydrate loading (with a reduction in the risk of obesity, poor glycemic control in diabetics, and hyperinsulinemia) (16,17). The typical systemic glucose exposure in this study was only around 25 g/day, compared to about 160 g/day for a CAPD patient performing only one in four exchanges with 3.86% glucose-containing fluid.
The issue of cost-effectiveness was not directly studied over the study period. However, cost analysis within the planning stage indicated that, in our institution, BMD was cost neutral. This was a result of flat-priced treatment costs between modalities and, roughly, a balanced cost implication of the additional HD time from the reduction in the cost of PD consumables. This neutrality, however, would depend very much on local pricing considerations and the possession of an adequate HD resource able to accommodate such nonstandard HD schedules.
In conclusion, BMD appears to be a feasible mode of RRT in the treatment of new onset ESRD. Bimodal dialysis appears to be capable of delivering adequate RRT, with levels of small molecule clearance, hypertension control, and modulation of volume status comparable to HD or PD alone. Furthermore, the technique may have the advantage of helping to maintain RRF and certainly increases flexibility of RRT, allowing default to either solo modality in response to medical or psychosocial imperatives. Patient groups in whom it might be considered would include those failing to maintain adequacy on PD alone (but without ultrafiltration failure), older or more dependent patients who might otherwise default to HD (due to being unable to consider being responsible for their dialysis on PD in solo), and, potentially, other patients at onset of ESRD in an attempt to provide them with the potential benefits of BMD to deliver improved overall outcomes. Clearly, further comparative study is required to investigate these potential applications.
Footnotes
Acknowledgment
The author thanks Baxter Healthcare for their financial support of this study.