
Abstract
Background
Continuous ambulatory peritoneal dialysis (CAPD) is an established treatment for end-stage renal disease (ESRD). We investigated the outcome of CAPD over a period of 25 years at our institution.
Methods
CAPD has been performed in 2301 patients in 25 years. After excluding patients with less than 3 months of follow-up and missing data, we evaluated 1656 patients who started peritoneal dialysis between November 1981 and December 2005. Data for sex, age, primary disease, co-morbidities, follow-up duration, cause of death, and cause of technique failure were collected. We also examined data for urea kinetic modeling (UKM), beginning in 1990, and peritonitis episodes, including causative organisms, starting in 1992.
Results
Compared to incident patients from 1981 – 1992, mean age and incidence of ESRD caused by diabetic nephropathy increased in patients from 1993 to 2005. Technique survival after 5 and 10 years was 71.9% and 48.1% respectively. Technique survival was significantly higher in patients who started CAPD after 1992 than in those who started before 1992. Peritonitis was the main reason for technique failure. Overall peritonitis rate was 0.38 episodes per patient-year, with a significant downward trend to 0.29 per patient-year over 10 years, corresponding to a decrease in gram-positive peritonitis. Patient survival after 5 and 10 years was 69.8% and 51.8% respectively. Patient survival improved significantly during 1992 – 2005 compared to 1981 – 1992 after adjustment for age, gender, diabetes, and cardiovascular comorbidities [hazard ratio (HR) 0.68, p < 0.01]. Subgroup analysis based on UKM revealed that dialysis adequacy did not affect patient survival. However, diabetes (HR 2.78, p < 0.001), older age (per 1 year: HR 1.06; p < 0.001), serum albumin level (per 1 g/dL: increase, HR 0.52; p < 0.05), and cardiovascular comorbidities (HR 2.32, p < 0.01) were identified as significant risk factors.
Conclusion
Technique survival has improved due partly to a decrease in peritonitis, which was attributed to a decrease in gram-positive peritonitis. Patient survival has also improved considering increases in aged patients and ESRD caused by diabetes. The mortality rate of CAPD is still high in older, diabetic, malnourished, and cardiovascular diseased patients. A more careful management of higher risk groups will be needed to improve the outcome of CAPD patients in the future.
Keywords
Patients and Methods
We considered a total of 2301 patients who started CAPD from 1981 to 2005. We then excluded patients that were younger than 15 years of age at initiation of CAPD, patients that had less than 3 months of follow-up, and patients that had been on hemodialysis (HD) or received a kidney transplant before CAPD. Patients that recovered kidney function or started CAPD for other reasons, such as acute renal failure or congestive heart failure, were also excluded from the analysis. Nephrologists performed all CAPD catheter insertions. On operation day, a prophylactic antibiotic (cefazolin sodium 1.0 g) was administered intravenously 2 hours before insertion of the Tenckhoff catheter; CAPD was then initiated incrementally with a starting volume of 500 mL per bag. The volume of PD was gradually increased by 500 mL over the next 3 – 4 days. If there was leakage, CAPD was started after a break-in period of 4 weeks following PD catheter insertion. A twin-bag system was employed in all patients starting in the early 1990s. Three different types of PD fluid (Baxter Healthcare, Deerfield, Illinois, USA; Fresenius Medical Care, Deutschland GmbH, Germany; Gambro, Lund, Sweden) have been used for 25 years.
For analysis of patient survival and technique survival during a period of 25 years, data for sex, age at the start of PD, underlying renal disease, comorbidities, follow-up duration, cause of death, and cause of technique failure were collected. For the assessment of comorbidities, history of cardiovascular disease, lung disease, liver disease, and malignancy were reviewed. Cardiovascular disease was defined as a history of coronary, cerebrovascular, or peripheral vascular disease. Coronary disease was defined as a history of angioplasty, coronary artery bypass graft, myocardial infarction, or angina. Cerebrovascular disease was defined as a previous transient ischemic attack, stroke, or carotid endarterectomy, and peripheral vascular disease was defined as a history of claudication, ischemic limb loss and/or ulceration, or peripheral revascularization procedure.
Technique failure was defined as transfer to HD due to peritonitis, ultrafiltration failure, inadequate dialysis, exit and tunnel infection, and mechanical problems. Ultrafiltration failure was defined as fluid overload associated with net ultrafiltration less than 400 mL after a 4 hour, 2 L, 4.25% dextrose dwell, and that was not related to dietary indiscretion or some other non-membrane-related causes such as heart failure or hernia. For peritonitis, data for causative organisms and incidence were collected starting in 1992. The urea kinetic model (UKM) was introduced in 1990. Subgroup analysis was performed in patients who undertook UKM within 6 months of CAPD commencement. Demographic and clinical data for sex, age, underlying renal disease, and follow-up duration were obtained. In addition, we examined hematocrit, serum albumin, and urea kinetics, including residual renal function, Kt/V urea as a measure of dialysis adequacy, normalized protein catabolic rate (nPCR), and percentage of lean body mass (%LBM). Residual renal function was assessed within 6 months after CAPD initiation by the measurement of urea and creatinine concentrations in urine samples collected over a 24-hour period. Residual glomerular filtration rate (GFR) was calculated as the average of 24-hour urinary urea and creatinine clearance (CrCl) (13). Kt/V urea was determined by standard methods (14), nPCR was calculated by the methods described by Randerson et al. (15), and %LBM was determined from creatinine kinetics according to the method of Keshaviah et al. (16).
Statistical Analysis
Statistical analysis was performed using SPSS version 13.0 (SPSS Inc., Chicago, Illinois, USA) for Windows operating system (Microsoft Corp., Redmond, Washington, USA). All data were expressed as mean ± SD. Data for transfer to HD or kidney transplantation, transfer to another center, and lost to follow-up were censored in the patient survival analysis. Patients who died within the first 3 months after transferring to HD or receiving a kidney graft were considered deaths related to CAPD. Data for death unrelated to technique failure, switch to kidney transplantation, and lost to follow-up were censored in the technique survival analysis. Patients that died due to peritonitis-induced sepsis were considered deaths related to technique failure. Patient and technique survival rates were determined using the Kaplan– Meier method. A log-rank test was used to compare patient and technique survival between subgroups. A multivariate Cox proportional hazards model was utilized to identify factors predicting patient mortality and to estimate and test the hazard ratio (HR) and associated 95% confidence intervals. We used the Student's t-test and chi-square test to compare the differences between survivors and nonsurvivors in the survival analysis based on UKM data. All probabilities were two tailed and the level of significance was set at 0.05.
Results
Patient Characteristics
Table 1 details the main patient characteristics. Following application of the exclusion criteria described above, a total of 1656 CAPD patients were analyzed, of which 912 were male (55.1%). Mean age at the start of CAPD was 48.9 ± 14.1 years and mean PD duration was 46.0 ± 40.4 months. Diabetes was the most common cause of ESRD (27.8%), followed by chronic glomerulonephritis (16.5%) and hypertension (13.0%).
Patient Characteristics
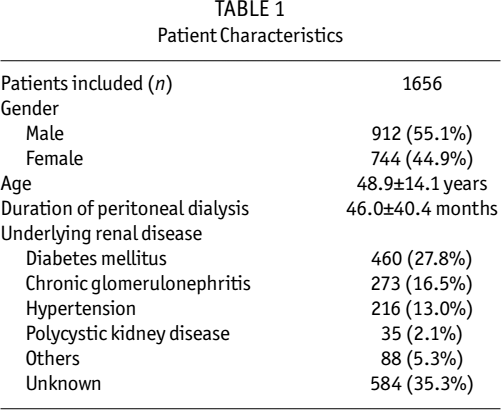
Table 2 details trends in the demographics of patients between the first half (1981 – 1992) and the second half (1993 – 2005) of the study period. Mean age at the start of CAPD increased from 44.2 ± 13.9 to 50.4 ± 13.9 years. Also, the proportion of patients over 60 years old at initiation of CAPD was double in the second period. The incidence rate of ESRD caused by diabetic nephropathy rose from 19.5% to 30.5% during the same period (Table 2).
Trends in Demographics Between the First and Second Halves of the Period

ESRD = end-stage renal disease; CGN = chronic glomerulonephritis; PKD = polycystic kidney disease; CV = cardiovascular.
p < 0.01 versus the first half of the period.
Peritonitis
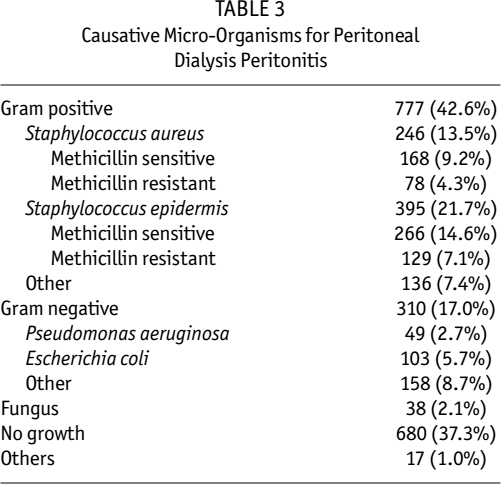
The overall peritonitis rate was 0.38 episodes per patient-year. The incidence of peritonitis decreased gradually, from 0.57 to 0.29 episodes per patient-year, over the 10 years surveyed (p < 0.01; Figure 1). Causative micro-organisms for PD peritonitis are described in Table 3. Gram-positive and gram-negative organisms caused most cases of PD peritonitis, and Staphylococcus epidermidis was the most common causative organism (21.7%). The incidence of gram-positive peritonitis decreased from the early 1990s, while gram-negative peritonitis did not change significantly (p < 0.01; Table 4). Methicillin-resistant staphylococci were increasingly prevalent in both Staphylococcus aureus and Staphylococcus epidermidis infections (p < 0.01; Table 5).
Causative Micro-Organisms for Peritoneal Dialysis Peritonitis
Changes in Peritoneal Dialysis Peritonitis Agents
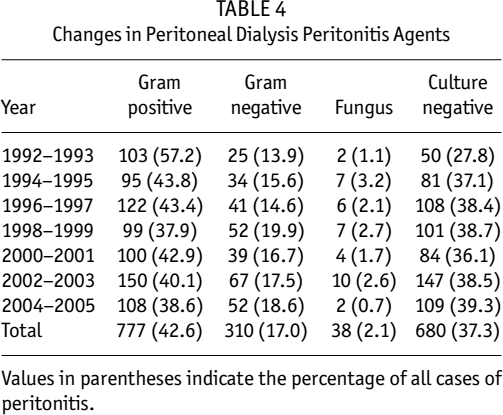
Values in parentheses indicate the percentage of all cases of peritonitis.
Changes in Peritonitis Rate Induced by Staphylococcal Pathogens
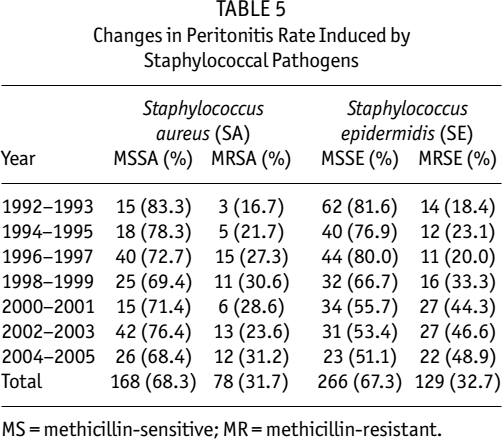
MS = methicillin-sensitive; MR = methicillin-resistant.
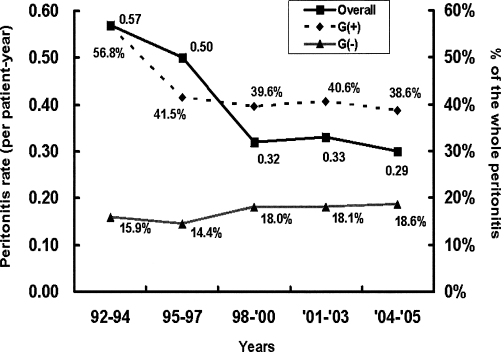
Peritonitis rates from 1992 to 2005. The overall peritonitis rate has decreased significantly, from 0.57 to 0.29 episodes per patient-year, for over 10 years (p < 0.01). The incidence of gram-positive peritonitis decreased (p < 0.01), while that of gram-negative peritonitis did not change.
Technique and Patient Survival
The 1-, 3-, 5-, and 10-year technique survival rates were 94.9%, 83.7%, 71.9%, and 48.1%, respectively. Technique survival rate increased in patients who started PD after 1993 compared to patients who started PD before 1992 (Figure 2; Table 6). There were no differences in technique survival rate according to sex, age, or dia-betes status. Technique failure resulted from peritonitis (72.3%), ultrafiltration failure (14.0%), mechanical malfunction and leakage (7.3%), and exit-site and tunnel infection (3.4%). The 1-, 3-, 5-, and 10-year patient survival rates were 93.4%, 81.5%, 69.8%, and 51.8%, respectively. The Kaplan–Meier plots for both patient survival and technique survival are shown in Figure 3.
Hazard Ratio (95% Confidence Interval) for Technique Failure and Mortality in Patients That Started CAPD During 1992–2005 Compared to Those That Started During 1981–1992
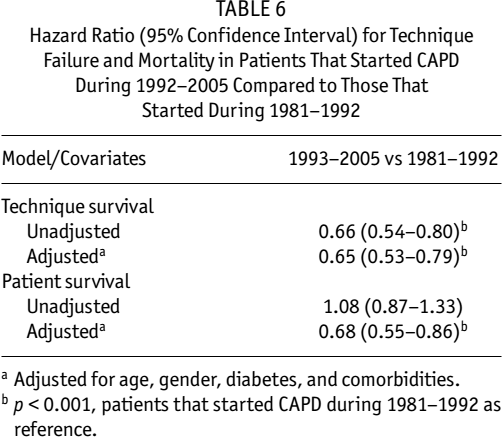
Adjusted for age, gender, diabetes, and comorbidities.
p < 0.001, patients that started CAPD during 1981–1992 as reference.
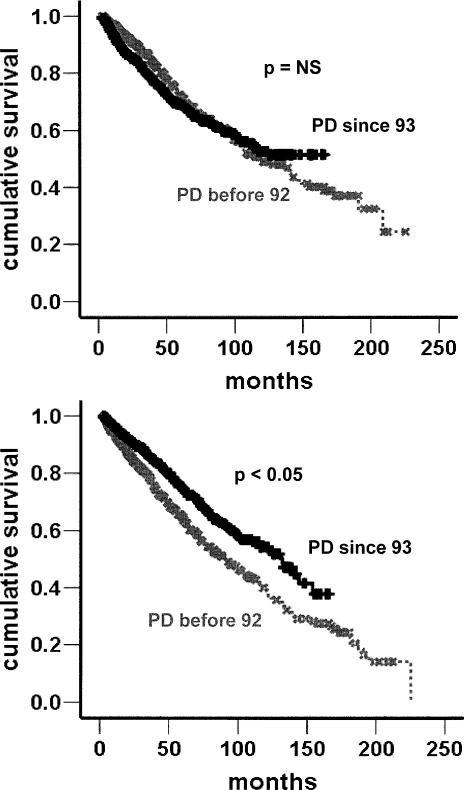
Kaplan–Meier survival plots for patient (upper) and technique (lower) survival before and after 1992. Technique survival rate was lower in patients that started peritoneal dialysis (PD) before 1992 than in those starting since 1993. Patient survival rate was not different between the two groups.
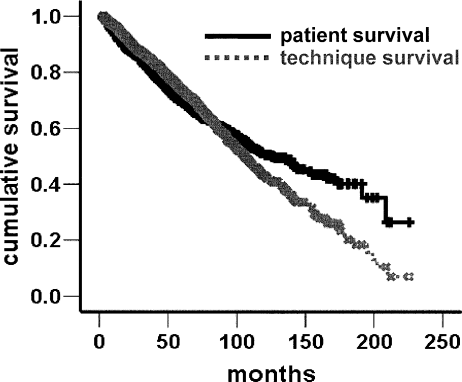
Patient and technique Kaplan–Meier survival curves. Patient survival after 5 and 10 years after CAPD was initiated 69.8% and 51.8% respectively. Five- and 10-year technique survival rates were 71.9% and 48.1%.
Most deaths were due to cardiovascular disease (31.8%) or infection (27.1%). Univariate analysis revealed greater patient survival in nondiabetic (p < 0.001), younger (p < 0.001), and female (p = 0.008) patients. The 5- and 10-year survival rates were 38.9% and 12.9% in diabetic patients, and 81.4% and 62.7% in nondiabetic patients. Also, the 5- and 10-year survival rates were 39.9% and 8.1% in patients that started CAPD while over 60 years old, and 78.1% and 59.2% in those less than 60 years old. In a multivariate Cox proportional hazards regression analysis (data not shown), female gender, younger age, and the absence of diabetes or cardiovascular comorbidities were independently associated with reduction in HR of death. Unadjusted univariate analysis showed no difference of mortality in patients who started CAPD in 1992 – 2005 compared to 1981 – 1992 (Figure 2; Table 6). However, multivariate Cox proportional hazards regression model revealed that patient survival increased significantly when adjusted for age, gender, diabetes, and comorbidities (Table 6; HR 0.68; p < 0.001).
Survival Analysis Based on Urea Kinetics
Urea kinetics was introduced in our institute during the early 1990s. Subgroup analysis was performed in 404 patients who undertook UKM within 6 months of CAPD initiation. Diabetes represented 19.6% of primary disease in the included patients. Mean age at the start of CAPD was 47.6 ± 12.8 years. Mean duration of PD was 47.2 ± 38.2 months. Baseline hematocrit and serum albumin were 28.0% ± 10.4%, and 36 ± 5 g/L (3.6 ± 0.5 g/dL) respectively. Baseline UKM data were as follows: Kt/V urea 2.3 ± 0.5; CrCl 86.3 ± 41.0 L/week/ 1.73 m2; nPCR 1.0 ± 0.2 g/kg/day; and %LBM 71.2 ± 14.4. Residual GFR was 2.6 ± 2.9 mL/minute/1.73 m2.
Patients were divided into survivor and non-survivor groups and compared based on baseline data. There were no significant differences in sex, hematocrit, Kt/V urea, CrCl, or residual GFR between the survivor and non-survivor groups at baseline. Survivors had a lower prevalence of diabetes, less cardiovascular comorbidity, younger age at the start of PD, and higher levels of serum albumin. No significant differences were seen between the two groups in longitudinal follow-up of Kt/V and CrCl. Patients with Kt/V urea ≥ 2.0 or CrCl ≥ 60 L/week/1.73 m2 showed no survival benefit compared to those with Kt/V < 2.0 or CrCl < 60 L/week/1.73 m2. Based on multivariate analysis, the independent factors for patient survival were diabetes, age at the start of PD, cardiovascular comorbidities, and serum albumin level (Table 7).
Multivariate Cox Proportional Hazard Ratio (HR) for Mortality a
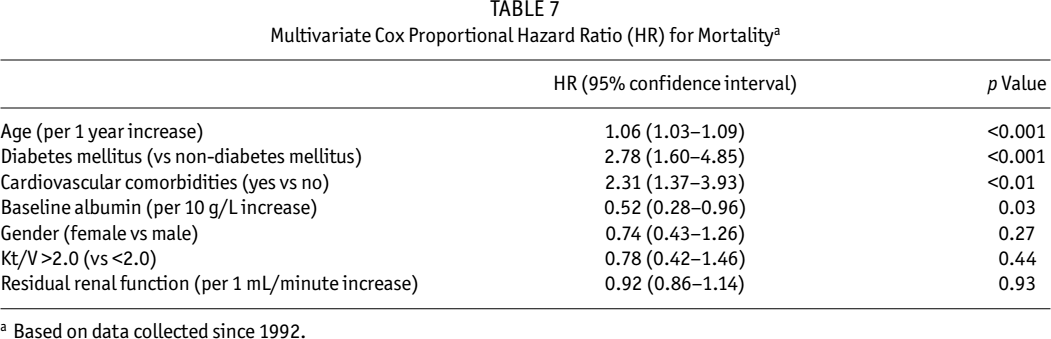
Based on data collected since 1992.
Discussion
There have been many reports on CAPD outcomes worldwide. USRDS data from 2003 reported a 5-year survival rate of 32.7% in PD patients that initiated treatment from 1994 to 1998, which was an increase of 7% over the previous period of 1989 – 1993 (4). Two-year survival rates in European prospective studies have been reported (17,18), but reports on long-term outcome on PD are scarce. Some centers have reported long-term CAPD experiences (5,7,8,19-23). Here, we report 25 years of experience with CAPD at our institute.
Five- and 10-year technique survival rates were 71.9% and 48.1% in our center, which were better than those reported in other countries. Technique survival was significantly improved in patients that started PD after 1992 compared to those that started before 1992. One of the reasons for improved technique survival was the decreased incidence of peritonitis. We could not collect data for peritonitis before 1992 due to lack of data, but the incidence of peritonitis has gradually decreased since the early 1990s, corresponding to a decreased incidence of gram-positive organisms as causative agents. The introduction of Y-set and double-bag systems greatly contributed to the reduction in peritonitis (24,25). Y-set and double-bag systems were applied to all patients in the mid-1990s, which might explain the rapid fall in the gram-positive peritonitis rate during the same period. Accordingly, we can speculate that technique failure decreased due to declining peritonitis and improvements in PD connection systems, which is consistent with worldwide trends (26). Our data revealed a lower rate of peritonitis compared to other countries. In addition, the prevalence of ultrafiltration failure was only 14.0% in our study, which is lower than in previous reports. These reductions might also explain the longer technique survival we observed. Sanitation and PD management education may play a role in better outcome based on technique, but the impact of those factors on PD outcome is difficult to prove. Although the peritonitis rate decreased, methicillin-resistant staphylococci have gradually increased. In addition, we experienced a few cases of vancomycin-resistant enterococcus-induced peritonitis. Treatment of antibiotic-resistant organisms will continue to be a challenge in the future.
Encapsulating peritoneal sclerosis (EPS) is a devastating complication of CAPD. We experienced 21 cases of EPS (0.90%) over 25 years. The overall mortality rate was 25.6%. Tamoxifen treatment was beneficial in some patients, but we could not suggest any specific treatment for EPS because there was no difference in survival rate according to different treatment modalities (data not shown).
Patient survival has been reported to be low in CAPD patients. However, a Japanese study reported surprising patient survival rates of 67.4% at 5 years and 48.6% at 10 years, which are greater than those in other countries (3,9). Our data were comparable to the Japanese findings. We found 5- and 10-year patient survival rates of 69.8% and 51.8% respectively. The patient survival rates on PD in Hong Kong were reported to be higher than those in Western countries. Five-year survival in Hong Kong was 47%, which is lower than that of Japan and our center. However, this should be interpreted with caution because more than 80% of new ESRD patients started with PD in Hong Kong. Interestingly, most data from East Asia showed that survival rates were much higher than those in Western countries. Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS) showed that the relative risk for death in HD patients was significantly higher in both Europe and USA compared to Japan (27). Further study is needed to investigate if patient survival on PD in the Asian population is better than in Western countries.
It is uncertain why the patient survival rates in our center are superior to those in Western countries. One of the possible explanations for this result is the relatively younger age of our patients at the start of CAPD. However, this figure was higher than that of the ADEMEX study (Adequacy of Peritoneal Dialysis in Mexico) subjects (28). CAPD has been favored especially in patients who are socially functioning. Therefore, a number of younger patients preferred CAPD in our study. Also, ESRD caused by diabetic nephropathy was 28%, which is relatively lower than in Western countries. This result is similar to those of East Asia. Reports from Hong Kong and Japan showed that only 22% of ESRD was caused by diabetes (6,9). Considering age and diabetes as significant determinants of death in CAPD patients, these factors combined together might contribute to superior survival in our center. However, the age of new ESRD patients at the start of CAPD and the proportion of diabetic ESRD patients have increased significantly as the incidence of ESRD has risen. As shown in Table 2, the mean age of patients during 1993 - 2005 was significantly higher than in the patients of 1981 - 1992. Also, the proportion of diabetic ESRD has increased from 19.5% in 1981 -1992 to 30.5% in 1993 - 2005. For the recent 5 years of 2001 - 2005, mean age at the start of CAPD was 53 years and diabetes comprised 39% of ESRD. Although patient survival was not different in 1993 - 2005 compared to that in 1981 - 1992 in the unadjusted model, patient survival is seen to improve significantly when adjusted for age, gender, diabetes, and cardiovascular comorbidities (Table 6).
With 1656 patients included, multivariate analysis revealed that female gender, diabetes, older age, and cardiovascular comorbidities were independent risk factors of death (data not shown). Careful consideration should be given to this result, however, because a lot of factors affecting mortality were excluded from the analysis. Therefore, we performed subgroup analysis to assess the risk factors of death in CAPD patients, in which other variables such as dialysis adequacy, laboratory findings, residual renal function, and baseline comorbidities were included. We found that diabetes, older age, lower levels of serum albumin, and cardiovascular comorbidities were significant determinants for death (Table 7).
Many reports have provided good evidence that a lower level of serum albumin is an independent risk factor for death (29-31). Serum albumin can represent not only nutritional but also inflammatory status (32), and hypoalbuminemia has been strongly associated with cardiovascular mortality (30). Our study revealed that hypoalbuminemia was an independent risk factor for death in CAPD patients.
Dialysis adequacy did not affect the outcome of CAPD in our study, which is consistent with results from the ADEMEX study (28) and Hong Kong (28,33). The European Automated PD Outcomes Study (EAPOS) group found that ultrafiltration of more than 750 mL per day was a better predictor for death than dialysis adequacy (18). We were unable to obtain ultrafiltration data due to the limitations of the retrospective study. Because most patients met the target Kt/V urea proposed by Dialysis Outcomes Quality Initiative (DOQI) guidelines, we could not conduct a comparative survival analysis in patients with a lower Kt/V urea. Unlike previous reports, residual renal function did not impact patient survival in our study (34-37). Baseline residual GFR was insignificantly higher in the survivor group (2.6 ± 2.7 vs 2.3 ± 3.5 mL/min). One of the possible explanations for this result is that baseline residual GFR was too low in both groups; therefore, the favorable effect of residual renal function would not be apparent. Unfortunately, many patients had to start dialysis treatment immediately after ESRD was diagnosed. As seen in Table 1, ESRD without definite causes comprised 35%. They were not aware that their kidney function had failed until they visited hospitals or emergency units, therefore resulting in too late diagnosis of chronic kidney disease. In addition, most patients needed a few sessions of HD before PD catheter insertion in order to reduce bleeding diathesis and improve uremic symptoms. The inclusion of data of residual renal function that were measured within 6 months of CAPD commencement might explain the low residual GFR at the start of CAPD in our patients.
We believe that this is one of the largest cohort studies of CAPD patients. Also, to our knowledge, 25 years is the longest range of experience in the literature. The size and breadth of our study are clear strengths. At the same time, our study is limited by the exclusion of factors that could influence survival, such as detailed comorbidities and peritoneal equilibration tests. For peritonitis analysis, we had a high incidence of culture-negative peritonitis. This result is difficult to explain in a retrospective study; however, it could be partly explained by the use of intraperitoneal antibiotics prior to visits at our PD unit. Even though the patients were instructed to bring the first cloudy dialysate, compliance was not good enough. In addition, this study is not a multicenter study, and a center-specific effect may exist (38,39): for example, Guo and Mujais found a significantly increased relative risk of death in patients at centers with fewer than 20 PD patients (39).
In summary, we found that patient and technique survival in our center was greater than previous reports from other countries. The improving technique survival of CAPD could be partly explained by the declining peritonitis rate, which is attributed to a decrease in gram-positive peritonitis. However, an increase in antibiotic resistance remains to be solved. Diabetes, old age, hypoalbuminemia, and cardiovascular comorbidities were independent risk factors for death. A more careful management of higher risk groups should be provided to further improve the outcome of CAPD in the future.
Footnotes
Acknowledgment
The authors thank Drs. T.H. Lee, D.K. Kim, S.J. Moon, H.S. Lee, S.Y. Park, H.J. Oh, D.E. Yoo, and S.J. Kim.