
Abstract
A simple, noninvasive method for removing peritoneal dialysis (PD) catheters, called the “pull technique,” has become popular in recent years. Physicians still worry, however, about the range of its application and possible complications such as infection of the retained cuff and breakage. We, therefore, applied this technique in patients and enriched its administration for removing PD catheters. Altogether, 24 PD catheter removals in 24 patients were reviewed during the period from July 2018 to October 2019 in our hospital. Using the pull technique, the PD catheter’s superficial cuff was dissected using an electronic knife, and the deep cuff was retained. All patients’ catheters were successfully removed with no breakage. No incision or retained cuff was infected during the follow-up period (1.1–15.6 months). The appropriate peak force of pull traction was approximately 12–13 pounds, not very different from the mean maximum tensile force of 21.48 pounds for silicone tube breakage. The use of intermittent (rather than sustained) traction may reduce the breakage risk of the silicone tube. This method is a safe, practical, minimally invasive method for removing PD catheters, and it is suitable for application on special patients with peritonitis or who are on an immunosuppressant.
Introduction
The standard technique for removing a peritoneal dialysis (PD) catheter is to surgically dissect the attached Dacron cuff and the silicone tube from the tissues to which it has become attached, 1,2 which requires one or two incisions. Since 1990, the ‘pull technique’ has been intermittently and sparsely reported on. It consists of pulling the catheter until the silicone tube detaches from the Dacron cuff, allowing the catheter to be pulled out while retaining the cuff in the abdominal wall. 1,3 –6 This technique has several advantages, including its noninvasiveness and that it is quickly accomplished at the bedside. Although it is recommended by an International Society for Peritoneal Dialysis (ISPD) guideline/recommendation (2019 update), 7 some physicians still worry about its range of application and accompanying complications, such as infection of the retained cuff or breakage. Since 2018, we have been using the pull technique for PD catheter removal and have enriched it. We have found it to be a safe procedure with many advantages. We review the pull technique for PD catheter removal both in our center and worldwide and discuss its complications and indications.
Methods
Data on the use of the pull technique were collected from July 2018 to October 2019 at our PD center. There were 24 PD catheter removals in 24 patients using the pull technique. All except one of the patients had undergone PD catheterization during open surgery. The other patient was catheterized using a laparoscopic technique. All catheters were double-cuffed Tenckhoff catheters (Covidien, Medtronic, Minneapolis, Minnesota, USA), 20 of which were swan neck and 4 straight. The deep cuff was embedded within the rectus sheath above the peritoneum, and the superficial cuff was positioned in subcutaneous tissue about 2–3 cm away from the exit site.
Patient characteristics were obtained from electronic medical records, including age, sex, causes of chronic kidney disease, indications for catheter removal, and duration of PD (Table 1). Surgery times and bleeding volumes were collected from the surgical records. The surgery time was calculated from the completion of administering local anesthesia to completion of skin suturing. The amount of bleeding was estimated by the operators. A tension meter was used to measure the appropriate peak force that could successfully remove the catheter using the pull technique and the maximum tensile force of the silicone tube for breakage. Ultrasonography was performed in patients with peritonitis the day after PD catheter removal by the pull technique and again 20 days later to determine the status of the retained deep cuffs and to see whether any complications had developed, such as bleeding or infection.
Characteristics of the study population.
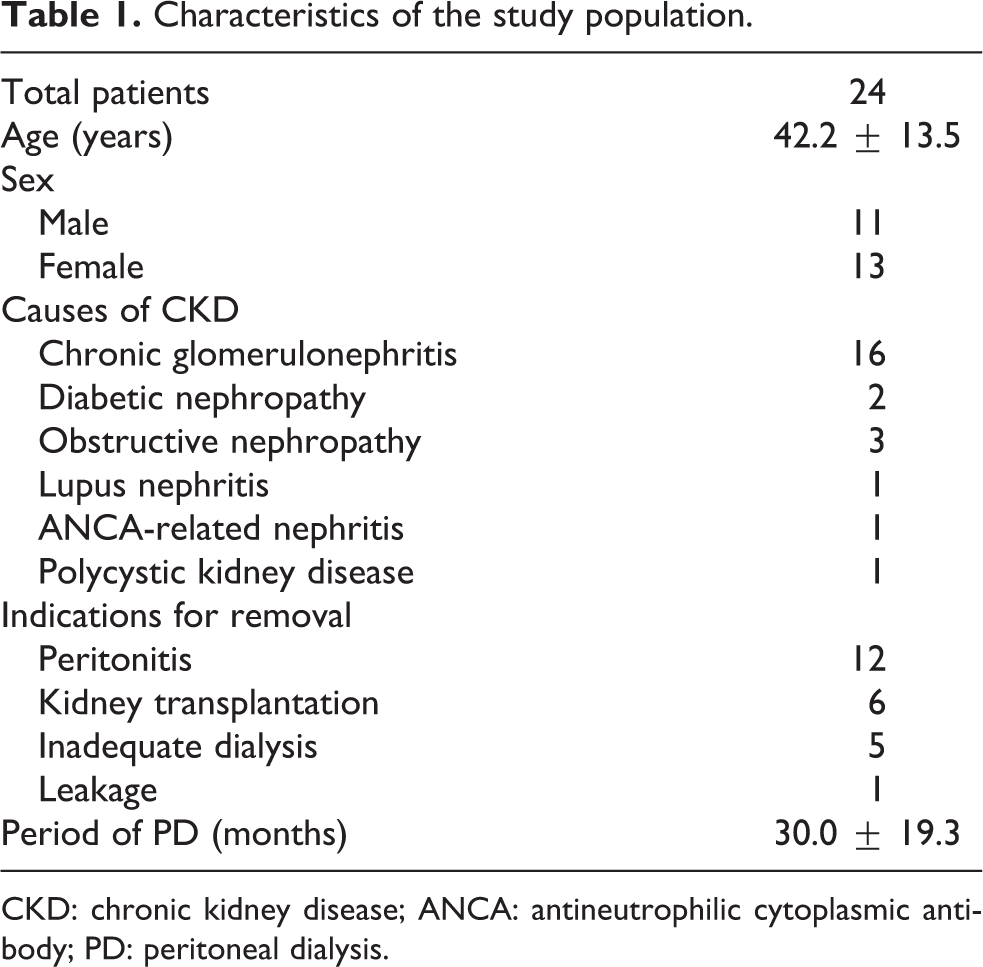
CKD: chronic kidney disease; ANCA: antineutrophilic cytoplasmic antibody; PD: peritoneal dialysis.
There are four major steps involved when removing the PD catheter using the pull technique. Local anesthesia is infiltrated around the superficial cuff, after which the external portion of the catheter is held firmly, while the electric knife separates a subcutaneous cuff (Figure 1(a)). The left hand then immobilizes the abdominal wall covering the exit site and primary incision site, while the right hand grasps and pulls on the silicone tube, applying gradual horizontal traction to stretch and shrink the tube until it cannot go any farther. Traction is maintained for several seconds until the tube loosens. If the silicone tube is stretched for too long, however, it should be coiled around the right-hand fingers, causing the hand to come closer to the skin to maintain the traction. This procedure is repeated several times (usually one to four times). After the catheter yields, the traction force is reduced or stopped (Figure 1(b)). The residual adhesive agent is visible at the deep cuff site of the catheter not far from the exit as the intra-abdominal catheter is slowly pulled out. The removed silicone catheter is then examined regarding its mechanical integrity. The exit site is sutured if the incision is large or there is obvious bleeding (Figure 1(d)).
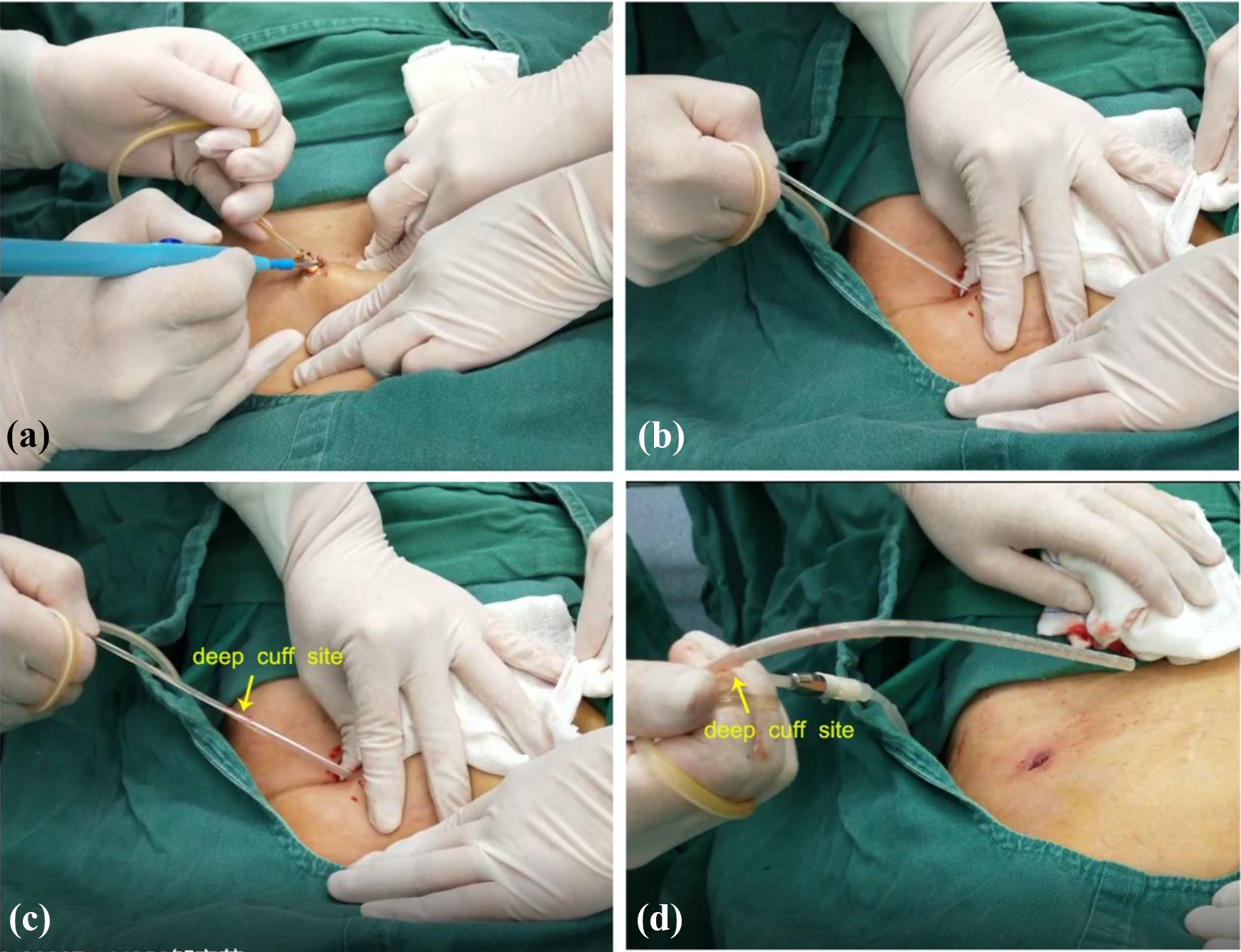
Procedure to remove a PD catheter using the “pull technique.” (a) An electric knife is used to separate the subcutaneous cuff. (b) The left hand fixes the abdominal wall, while the right hand pulls intermittently on the silicone tube. (c) After it yields, the intra-abdominal catheter is slowly pulled out. (d) The silicone tube is then examined for its mechanical integrity.
Results
Altogether, we studied 24 PD catheter removals and found no catheter breakage or conspicuous bleeding (>5 ml) during the operations. The average time for catheter removal was 4.13 ± 1.26 min. Only a tunnel opening of approximately 1 cm remained after the removal. Ultrasonographic images showed that the retained deep cuffs of two peritonitis patients were in the rectus sheath, with no obvious hemorrhage. On the 20-day follow-up, images showed that fibrous tissue had developed around the deep cuffs, with no obvious signs of infection. The overall follow-up for the 24 patients was 1.1–15.6 months (median 6.9 months). None of the patients exhibited abdominal wall pain, exit-site infection, or infection of the retained deep cuff. One straight Tenckhoff catheter was tested and was found to have a peak pull force of 12.21 pounds during the pulling procedure, and it took 12.85 pounds to detach the superficial cuff in vitro. Five other Tenckhoff catheters—three swan neck and two straight—were tested for maximum tensile force against breakage. The maximum tensile force of the silicone tube ranged from 18.20 pounds to 23.59 pounds (mean 21.48 pounds).
Discussion
The pull technique for PD catheter removal is currently attracting more attention. Although it is recommended by an ISPD guideline/recommendation (2019 update), 7 some physicians are still unwilling to accept it for fear of complications, such as retained cuff infections and/or catheter breakage. Elkabir et al. 1 reported a high infection rate (24.2%, 15 of 62 patients) for the retained cuffs, and Atkinson and Rubin 6 reported 29% (4 of 14) of the infected complications were related to the retained cuffs. Their findings may explain the unpopularity of the pull technique. With the positive results from subsequent studies, however, the technique has attracted a “second look.” Only one superficial cuff (of 57 retained cuffs) was infected in Quiroga et al.’s study, 3 and Grieff et al. 5 found that 2.2% (1 of 46) retained superficial cuffs that were infected with no deep cuff infections. Our study found no retained cuff infections, in accordance with the results in Nameirakpam et al.’s study. 4 Superficial cuff dissection and deep cuff retention during the pull technique is a highly practical method for reducing the infection rate of retained cuffs. This method is associated with minimal bleeding and leaves a tunnel opening of approximately 1 cm, which is greatly superior to that of the traditional surgical removal.
Four articles described the details of the ‘pull’ with sustained, smooth traction applied. 3 –5,8 Nameirakpam et al. 4 reported that, with sustained traction, the removal of 4 of 30 catheters resulted in failure (the reasons for which were not stated). Hakim et al. 9 pulled out the cuffs and the catheter together, and Shroff et al. 8 reported that 2 of 41 catheters snapped at the site of the deep cuff. Our tests showed that the peak pull traction was 12.21 pounds during the operation, which was not far from the maximum tensile force (mean 21.48 pounds) for catheter breakage. Sustained traction may cause excessive force and result in catheter breakage because the separation of the catheter from the cuff takes time. We experienced breakage with sustained traction during an experiment with a discarded catheter. We, therefore, changed the sustained traction to intermittent traction, with the result that there was no further catheter breakage in any of our patients.
It has been questioned whether the pull technique is suitable for peritonitis patients. The earlier study by Elkabir et al. 1 reported that 8 of 30 patients (26.6%) who underwent catheter removal for peritonitis developed a cuff-related infection, accounting for 53.3% of all 15 of those who became infected. They reported, however, that there was no correlation between the peritonitis and the local sepsis. Only 1 of 38 patients (2.6%) with peritonitis with a retained superficial cuff was infected in the studies by Nameirakpam et al. 4 and Grieff et al. 5 Our study showed no retained deep cuff infections in any of the 12 patients with peritonitis. We deem that the catheter removal by pull technique is suitable for patients with peritonitis, but still this view needs more studies to support as we have a limited number of patients with peritonitis.
Elkabir et al.’s article 1 reported that 7 of 15 patients whose retained cuff became infected had been given immunosuppressants. Atkinson and Rubin 6 believed that immunocompromised patients are at high risk for retained cuff infection. In contrast, Quiroga et al. 3 removed PD catheters of 31 post-kidney transplant patients, with only one case of an infected retained subcutaneous cuff. Our data showed that there was no deep cuff infection after PD catheter removal in six kidney transplant patients. The improvements in immunosuppressive agents and medical technology may have diminished the infection rate of retained cuffs in patients taking an immunosuppressant in recent years. The pull technique method may also be safe for the patients who are under antithrombotic agents, as we noticed no bleeding complication in 22 patients taking antithrombotic agents, such as aspirin, clopidogrel, and warfarin from Grieff’s study 5 and three patients taking clopidogrel from our study.
In addition, pull technique method may increase the risk of hemorrhage, while removing the PD catheter in patients whose intra-abdominal catheter was wrapped with omentum or fixed with thread. Similarly, it should not be applied in the presence of a tunnel infection, when catheters are extended with a titanium connector or when catheters are equipped with a bead and flange beneath the deep cuff.
Conclusions
Using pull technique to remove implanted PD catheters from patients who have undergone superficial cuff dissection and have retained deep cuffs is safe, practical, and minimally invasive. Superficial cuff dissection may reduce the infection risk, and intermittent (rather than sustained) traction may reduce the incidence of catheter breakage. The pull technique can be suitably applied on special patients with peritonitis or on those who are taking an immunosuppressant. We recommend that the technique be used routinely to remove PD catheters.
Footnotes
Acknowledgements
Author contributions
JW, X-SL, and F-XZ completed the surgery operations, researched literature, and conceived the study. R-XW, FC, and X-HT involved in protocol development and data analysis. X-QC and BH participated in patient follow-up and data collection. JW wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was waived by the Ethics Committee of the First Affiliated Hospital of Gannan Medical University because it is a retrospective study and the ‘pull’ technique is recommended by ISPD guideline/recommendations (2019 Update). This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Written informed consent was obtained from all subjects before the study, and every patient has signed a surgical consent form.
Informed consent to publish
Informed consent was not sought for the present study because it is a retrospective study and some patients lost contact.