
Abstract
Mycobacterium tuberculosis (MTB)-related peritonitis is a rare but serious complication in patients receiving maintenance peritoneal dialysis (PD). Early diagnosis is difficult due to the low sensitivity and delayed results of conventional microscopy and culture methods. MTB polymerase chain reaction (PCR) testing in PD effluent is recommended as a diagnostic adjunct, but real-world data remain limited. We conducted a 20-year single-centre retrospective study in a tuberculosis-endemic region to evaluate the diagnostic accuracy and clinical utility of MTB-PCR in PD effluent. Among 372 tests, MTB-PCR demonstrated sensitivity 50%, specificity 100%, negative-predictive value 94.6% and positive-predictive value 100%, using diagnoses based on a composite of clinical and laboratory criteria as the reference standard. Sensitivity showed a numerical trend of improvement from 33.3% with earlier assays to 50–85.7% with newer assays. Of 72 patients with culture-confirmed MTB-PD peritonitis, 13 (18.1%) were diagnosed via MTB-PCR. Compared to those diagnosed by non-PCR methods, MTB-PCR-diagnosed patients had shorter time to anti-tuberculosis treatment initiation (median 8 vs. 22 days, p ≤ 0.001) and shorter hospital stay from presentation to treatment (median 8 vs. 17 days, p = 0.008). They also had a numerically lower rate of PD catheter removal prior to treatment initiation [0/13 (0%) vs. 9/53 patients (17.0%), p = 0.186]. Rates of permanent transfer to haemodialysis and all-cause mortality at 1 year were similar among the two groups. These findings suggest a role for early MTB-PCR testing in suspected MTB-PD peritonitis. Further studies are needed to confirm the findings and optimize diagnostic strategies.
Keywords
Introduction
Peritoneal dialysis (PD)-associated peritonitis is a major complication in patients receiving maintenance PD. 1 Mycobacterium tuberculosis (MTB)-PD peritonitis, though uncommon, is associated with significant morbidity and mortality. 2 Early diagnosis is difficult due to clinical overlap with bacterial peritonitis, the low sensitivity of Ziehl–Neelsen smear microscopy and the delayed results from acid-fast bacilli (AFB) culture. While newer tools like adenosine deaminase assay, 3 gamma interferon enzyme-linked immunospot assay, 4 neutrophil-to-lymphocyte ratio 5 and pathogenic microorganism DNA high-throughput genetic sequencing 6 have been explored, the International Society for Peritoneal Dialysis (ISPD) has suggested MTB-polymerase chain reaction (PCR) tests as a diagnostic adjunct since 2010.7,8 However, real-world data on diagnostic accuracy and clinical value of MTB-PCR in PD effluent remain limited. To address this, we conducted a 20-year single-centre retrospective study in a tuberculosis-endemic region.
Methods
Inclusion and exclusion criteria
This single-centre retrospective study was approved by the local Research Ethics Committee (approval number: KC/KE-22-0194/ER-3). It comprised of two parts. First, we evaluated the diagnostic accuracy of MTB-PCR in PD effluent. All MTB-PCR performed in PD effluent for suspected MTB-PD peritonitis at United Christian Hospital from January 2002 to July 2022 were included. We excluded tests from patients with known MTB-PD peritonitis on anti-tuberculosis treatment and repeated tests within the same peritonitis episode. Second, we reviewed the clinical value of MTB-PCR. All patients diagnosed with MTB-PD peritonitis in United Christian Hospital from January 2002 to July 2022, identified from registry data, were included.
Microbiological tests
MTB-PCR were ordered at the treating clinicians’ discretion for suspected MTB-PD peritonitis. Multiple assays were used during the study period. From 2002 to 2009, AMPLICOR™ MTB test was used. From 2009 to 2013, COBAS® TaqMan® MTB test became the standard. From 2014 to June 2021, all PD effluent specimens sent for MTB-PCR underwent parallel testing with COBAS® TaqMan® MTB test and an in-house assay targeting insertion sequence 6110, except for one specimen from the intensive care unit that underwent only Xpert® MTB/RIF test. From July 2021 onwards, Xpert® MTB/RIF Ultra test replaced all previous assays as the standard. Details regarding AFB culture and MTB-PCR are provided in Online Supplemental Tables 1 and 2.
Data collection
Chart review was performed via electronic patient records. Collected data included age, sex, date of presentation, laboratory results, diagnosis, date of anti-tuberculosis treatment initiation, length of hospital stay (LOS) from presentation to treatment initiation, LOS from presentation to death in those not treated, PD catheter removal before treatment initiation, permanent transfer to haemodialysis and all-cause mortality within 1 year of treatment initiation. The diagnosis of MTB-PD peritonitis was based on a composite of clinical and laboratory criteria, independent of MTB-PCR, as outlined in Online Supplemental Table 3.
Outcomes and statistical analysis
Primary outcomes included sensitivity, specificity, positive-predictive value (PPV) and negative-predictive value (NPV) of MTB-PCR in PD effluent, using criteria-based diagnoses from chart review as the reference standard. Secondary outcomes included time from presentation to anti-tuberculosis treatment initiation, LOS from presentation to treatment initiation, LOS from presentation to death in those not treated, rates of PD catheter removal before treatment initiation, permanent transfer to haemodialysis and all-cause mortality at 1 year of treatment initiation. Chi-square test, Fisher's exact test, Mann–Whitney U test and Kruskal–Wallis test were used as appropriate. A p value <0.05 was considered statistically significant. Missing data were excluded by pairwise deletion. Analyses were performed by R version 4.5.0 and IBM SPSS Statistics 29.
Results
Diagnostic accuracy
Of 387 MTB-PCR performed in PD effluent during the study period, 372 were included for analysis (Figure 1, Online Supplemental Figure 1). Using criteria-based diagnoses from chart review as the reference standard, there were 19 true positives, 334 true negatives and 19 false negatives; no false positive was identified. All positive MTB-PCR results were confirmed by positive AFB culture in PD effluent. Pooled sensitivity was 50.0% [95% confidence interval (CI): 33.4–66.6%], specificity 100% (95% CI: 98.9–100%), PPV 100% (95% CI: 82.4–100%) and NPV 94.6% (95% CI: 91.7–96.7%). Diagnostic performance varied among assays. Xpert® MTB/RIF Ultra test had a numerically higher sensitivity (85.7%) compared to earlier tests (33.3–50.0%, Table 1).
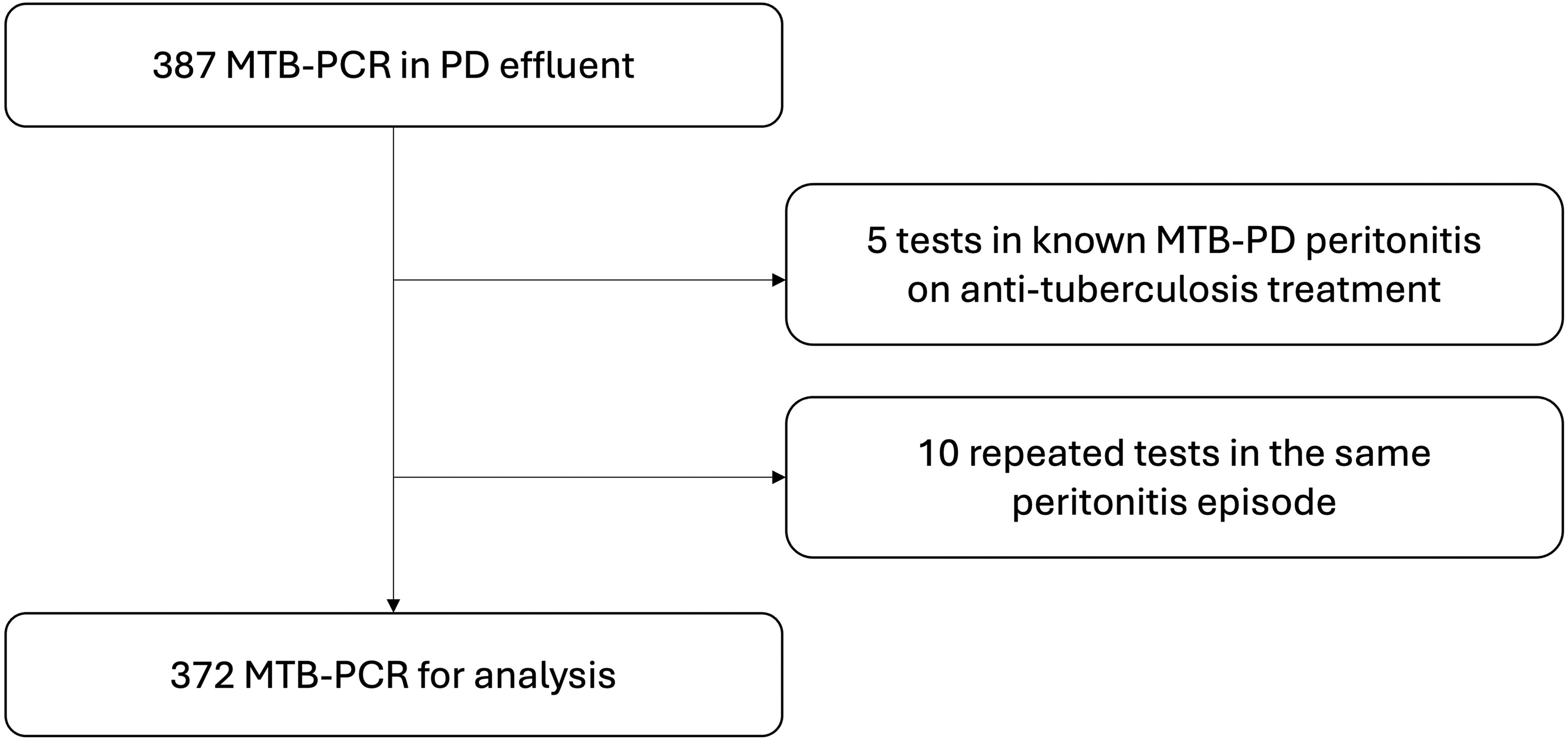
Inclusion and exclusion of MTB-PCR for analysis in the present study.
Analysis of MTB-PCR performance using diagnoses based on a composite of clinical and laboratory criteria as reference standard.
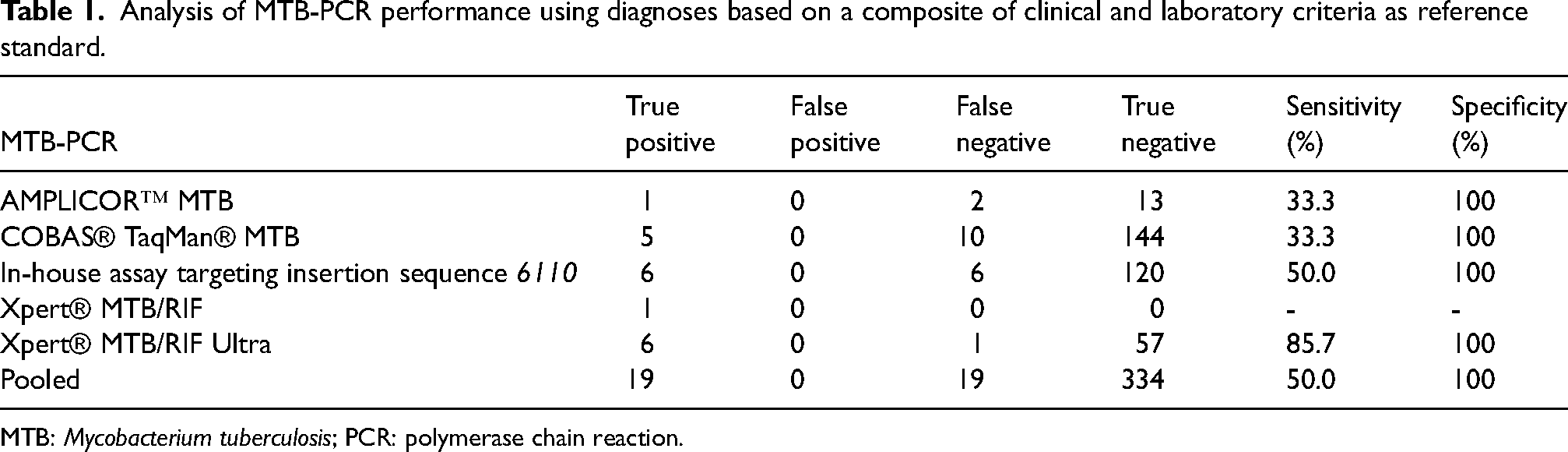
MTB: Mycobacterium tuberculosis; PCR: polymerase chain reaction.
Clinical value
Seventy-two patients were diagnosed with MTB-PD peritonitis during the study period; all had positive AFB culture in PD effluent. Their clinical features and outcomes are summarized in Tables 2, 3 and 4.
Clinical features and outcomes of MTB-PD-related peritonitis, by performance and result of MTB-PCR. a
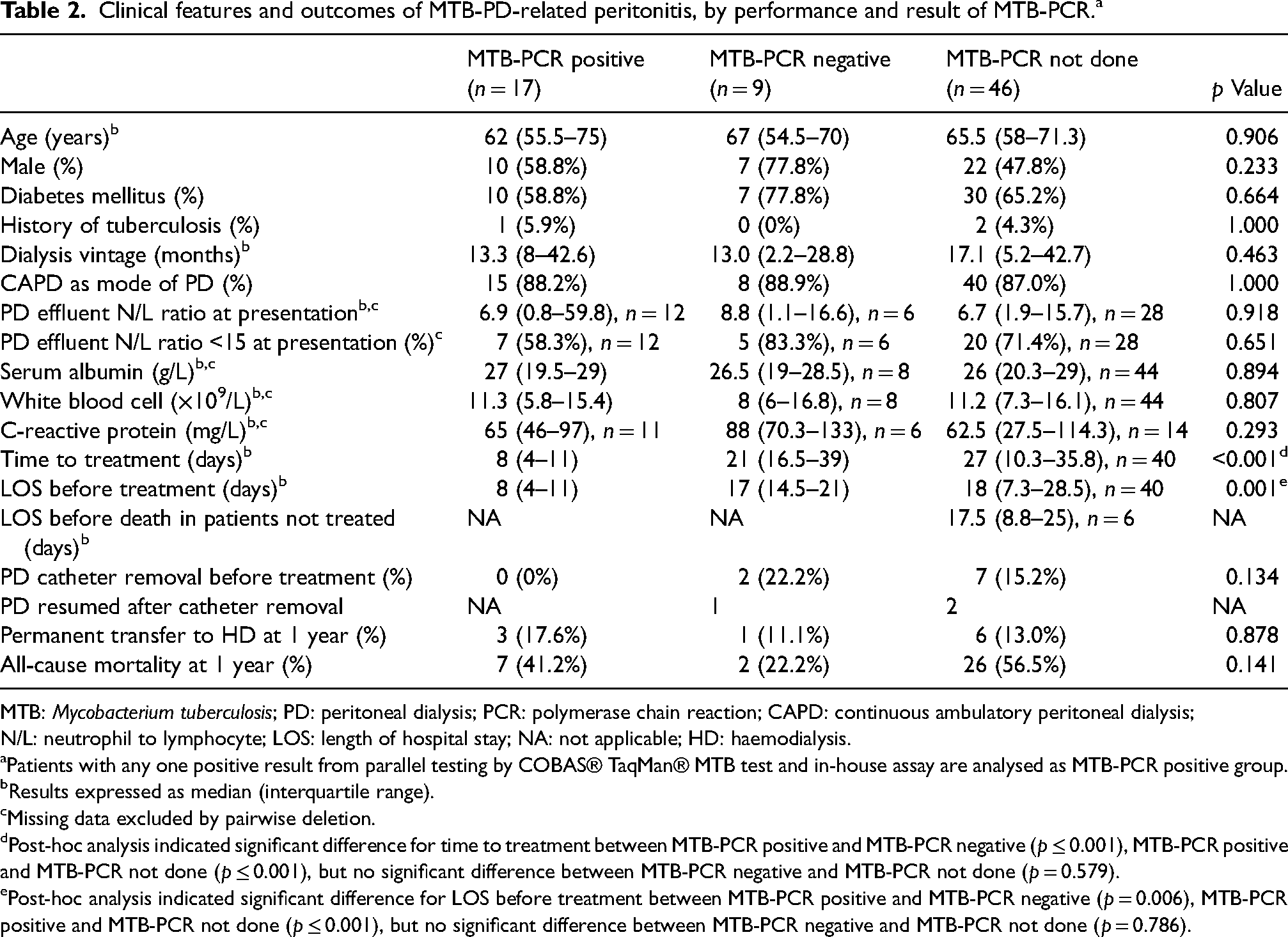
MTB: Mycobacterium tuberculosis; PD: peritoneal dialysis; PCR: polymerase chain reaction; CAPD: continuous ambulatory peritoneal dialysis; N/L: neutrophil to lymphocyte; LOS: length of hospital stay; NA: not applicable; HD: haemodialysis.
Patients with any one positive result from parallel testing by COBAS® TaqMan® MTB test and in-house assay are analysed as MTB-PCR positive group.
Results expressed as median (interquartile range).
Missing data excluded by pairwise deletion.
Post-hoc analysis indicated significant difference for time to treatment between MTB-PCR positive and MTB-PCR negative (p ≤ 0.001), MTB-PCR positive and MTB-PCR not done (p ≤ 0.001), but no significant difference between MTB-PCR negative and MTB-PCR not done (p = 0.579).
Post-hoc analysis indicated significant difference for LOS before treatment between MTB-PCR positive and MTB-PCR negative (p = 0.006), MTB-PCR positive and MTB-PCR not done (p ≤ 0.001), but no significant difference between MTB-PCR negative and MTB-PCR not done (p = 0.786).
Clinical features and outcomes of MTB PD-related peritonitis, by basis of diagnosis.
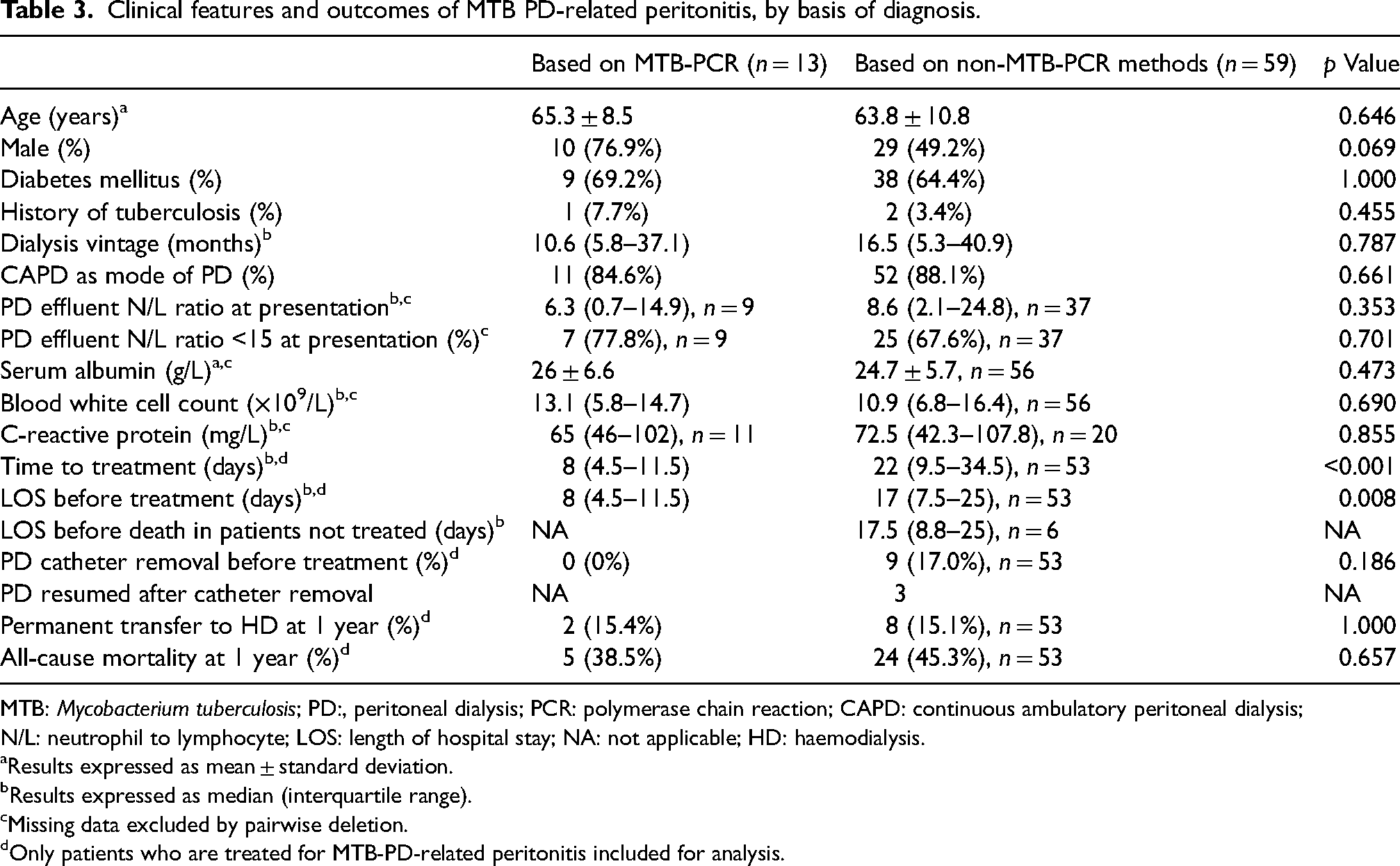
MTB: Mycobacterium tuberculosis; PD:, peritoneal dialysis; PCR: polymerase chain reaction; CAPD: continuous ambulatory peritoneal dialysis; N/L: neutrophil to lymphocyte; LOS: length of hospital stay; NA: not applicable; HD: haemodialysis.
Results expressed as mean ± standard deviation.
Results expressed as median (interquartile range).
Missing data excluded by pairwise deletion.
Only patients who are treated for MTB-PD-related peritonitis included for analysis.
Clinical features and outcomes of MTB-PD-related peritonitis, MTB-PCR positive versus false negative. a
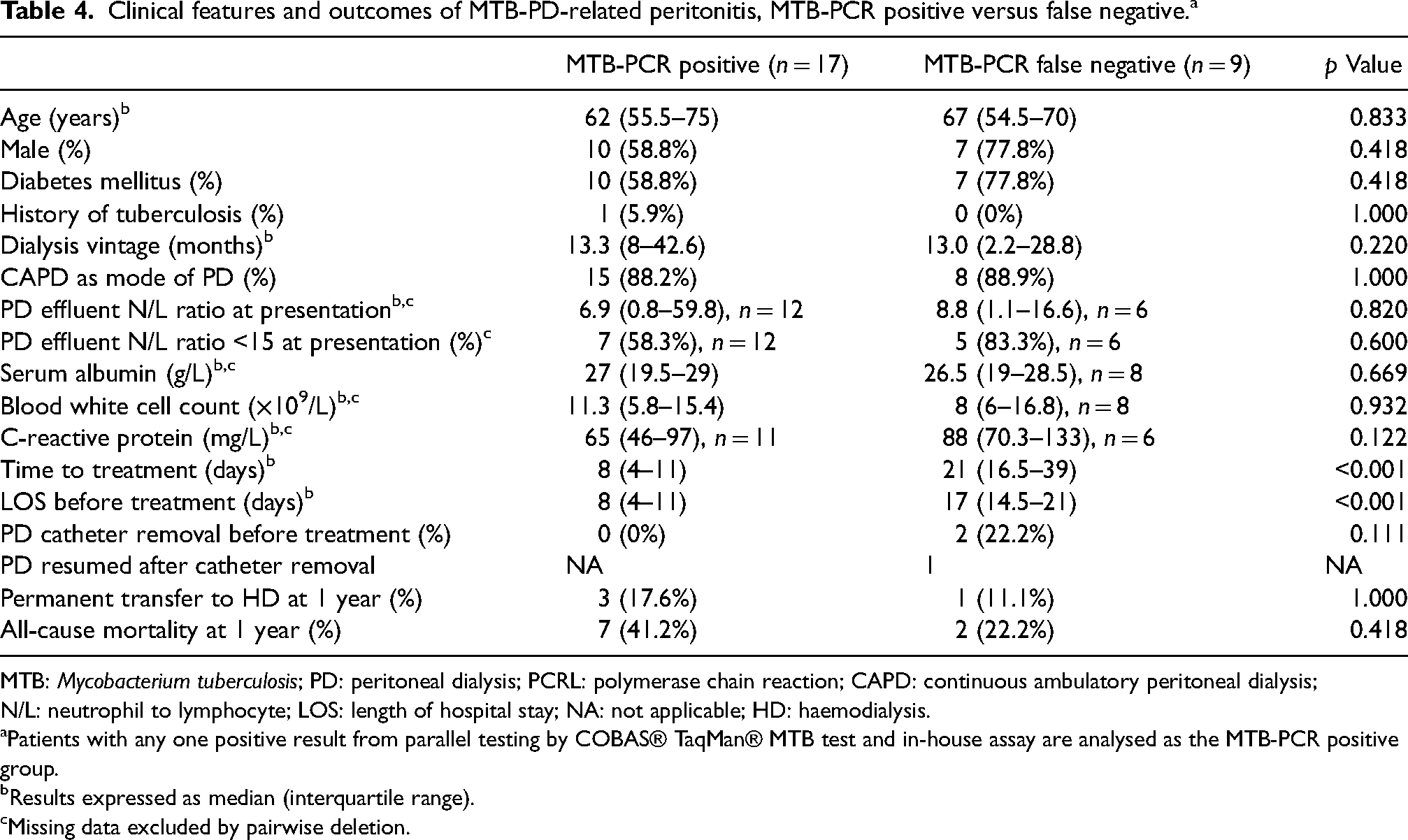
MTB: Mycobacterium tuberculosis; PD: peritoneal dialysis; PCRL: polymerase chain reaction; CAPD: continuous ambulatory peritoneal dialysis; N/L: neutrophil to lymphocyte; LOS: length of hospital stay; NA: not applicable; HD: haemodialysis.
Patients with any one positive result from parallel testing by COBAS® TaqMan® MTB test and in-house assay are analysed as the MTB-PCR positive group.
Results expressed as median (interquartile range).
Missing data excluded by pairwise deletion.
Six patients died before anti-tuberculosis treatment could be started and were retrospectively diagnosed by AFB culture. Among the 66 treated patients, 13 (19.7%) were diagnosed by MTB-PCR. The remaining 53 patients had diagnoses first suggested by non-MTB-PCR methods: empirical in six, Ziehl–Neelsen smear microscopy in eight, AFB culture in 31 and concurrent MTB infection at another site in eight.
Median time from presentation to anti-tuberculosis treatment initiation was shorter in patients diagnosed by MTB-PCR compared to those diagnosed by non-MTB-PCR methods [8 (interquartile range (IQR) 4.5–11.5) vs. 22 days (IQR 9.5–34.5), p ≤ 0.001]. Median LOS from presentation to treatment was also shorter [8 (IQR 4.5–11.5) vs. 17 days (IQR 7.5–25), p = 0.008]. Median LOS from presentation to death in the six patients not treated, all of whom did not undergo MTB-PCR, was 17.5 days (IQR 8.8–25).
None of the 13 patients diagnosed via MTB-PCR underwent PD catheter removal before treatment, versus 9 of 53 (17.0%) diagnosed by non-MTB-PCR methods (p = 0.186). One year after treatment initiation, there was no significant difference in the rates of permanent transfer to haemodialysis [2/13 (15.4%) vs. 8/53 patients (15.1%), p = 1.000] and all-cause mortality [5/13 (38.5%) vs. 24/53 patients (45.3%), p = 0.657].
Discussion
Our data suggest a role for early MTB-PCR testing in suspected MTB-PD peritonitis. MTB-PCR demonstrated modest sensitivity (50%) and excellent specificity (100%). Patients diagnosed by MTB-PCR had shorter time to treatment, shorter LOS before treatment, and a trend towards a lower rate of PD catheter removal before treatment.
MTB-PCR is known to have high specificity but modest sensitivity in extrapulmonary tuberculosis, as reflected in our findings, likely due to lower bacterial load and PCR inhibitors.9–11 While meta-analyses have evaluated the accuracy of MTB-PCR in abdominal tuberculosis,12,13 data specific to PD effluent is limited. PD effluent differs from ascitic fluid in composition and undergoes continuous exchange, potentially affecting diagnostic yield. Although MTB-PCR diagnosed 9.3% of reported MTB-PD peritonitis cases in a scoping review, 14 most case series included no more than six tests.15–17 A recent study reported a sensitivity of 32% with conventional PCR assay among 37 AFB culture-positive cases; specificity, PPV and NPV were not reported. 18 Our present data showed comparable sensitivity (33.3%) with earlier assays, and numerically higher sensitivity (50.0–85.7%) with newer assays, suggesting improved performance over time. It is important to note that given MTB-PCR's high rate of false negative and its inability to identify non-tuberculosis mycobacteria or provide sensitivity results, MTB-PCR should not replace AFB culture.
The rapid turnaround time of MTB-PCR likely contributed to the shorter time and LOS till treatment observed in our MTB-PCR-diagnosed patients. Since current ISPD guidelines do not recommend routine PD catheter removal in MTB-PD peritonitis, 1 timely diagnosis may prevent unnecessary catheter removal for presumed refractory culture-negative bacterial peritonitis. In our cohort, patients diagnosed by MTB-PCR had a numerically lower rate of PD catheter removal before treatment; this difference did not reach statistical significance, possibly due to a relatively small sample size.
Limitations of this study include retrospective design, single-centre setting, relatively small sample size and varied PCR assays over the 20-year study period. MTB-PCR being ordered at clinicians’ discretion might have increase the pre-test probability and overestimated the PPV. Nonetheless, this remains one of the largest studies of MTB-PCR in PD effluent to date. Prospective, multi-centre studies utilizing standardized PCR assays are needed to confirm our findings and optimize diagnostic strategies.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608251371954 - Supplemental material for Diagnostic accuracy and clinical value of polymerase chain reaction tests for Mycobacterium tuberculosis in peritoneal dialysis effluent: A 20-year single-centre retrospective study
Supplemental material, sj-docx-1-ptd-10.1177_08968608251371954 for Diagnostic accuracy and clinical value of polymerase chain reaction tests for Mycobacterium tuberculosis in peritoneal dialysis effluent: A 20-year single-centre retrospective study by Wai Lun Will Pak, Kin Chung Wong, Sandy Ka Yee Chau, Ka Lok Chan, Zi Chan, Yick Hei Wong, Wai Ping Law, Chi Kwan Lam and Sze Ho Sunny Wong in Peritoneal Dialysis International
Supplemental Material
sj-jpg-2-ptd-10.1177_08968608251371954 - Supplemental material for Diagnostic accuracy and clinical value of polymerase chain reaction tests for Mycobacterium tuberculosis in peritoneal dialysis effluent: A 20-year single-centre retrospective study
Supplemental material, sj-jpg-2-ptd-10.1177_08968608251371954 for Diagnostic accuracy and clinical value of polymerase chain reaction tests for Mycobacterium tuberculosis in peritoneal dialysis effluent: A 20-year single-centre retrospective study by Wai Lun Will Pak, Kin Chung Wong, Sandy Ka Yee Chau, Ka Lok Chan, Zi Chan, Yick Hei Wong, Wai Ping Law, Chi Kwan Lam and Sze Ho Sunny Wong in Peritoneal Dialysis International
Footnotes
Acknowledgments
None.
Author contributions
Conceptualization: WLWP; data curation: WLWP, CKW, SKYC, KLC, ZC, WPL, YHW, CKL; formal analysis: WLWP; methodology: WLWP, SKYC, SHSW; writing: WLWP, SKYC, SHSW.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent to participate
Informed consent was not sought for the present study because this study was conducted in accordance with the Declaration of Helsinki and was approved by Research Ethics Committee (Kowloon Central / Kowloon East), with the need for written informed consent waived.
Informed consent to publish
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.