
Abstract
Background:
Fatalities from opioid overdose have risen by 117% over the past 10 years. Increasing access to the opioid antagonist, naloxone can combat this trend and saves lives. This study investigates the various routes of naloxone administration for opioid reversal in the prehospital setting.
Methods:
PubMed, Ovid, and Google Scholar were searched for references that included the words naloxone and prehospital. Inclusion criteria were peer reviewed publications after 1995, English language, studies conducted in an outpatient setting, and intramuscular, intranasal, intravenous, or subcutaneous formulations; exclusion criteria were review articles or editorials.
Results:
8 articles met the inclusion criteria: intramuscular, intranasal, intravenous, and subcutaneous dosage forms of naloxone were analyzed to compare their time to administration, time to efficacy, financial impact, administrator safety, and administrator preference.
Conclusion:
There is little consensus on the optimal route of naloxone administration in the prehospital setting. Little training is required for proper administration of the intramuscular auto-injector; however, the high price of this device is a barrier to access. Intranasal naloxone appears to be the optimal dosage form when considering cost, effectiveness, and administrator safety. Pharmacists must be aware of trends in naloxone use, dosage forms, and administration when caring for patients and their communities.
Introduction
In the United States alone, an average of 46 individuals die from prescription opioid overdose each day. 1 Fatalities from opioid overdoses have risen by 117% over the past 10 years. 1 The variety of initiatives attempting to curb the current opioid epidemic is diverse and an increasing number of groups and agencies are working to combat the epidemic of opioid misuse, overdoses, and addictions. The Department of Health and Human Services supports a multipronged initiative that involves “actions to improve opioid prescribing and risk mitigation strategies, increase the dissemination of overdose prevention education, and expand use of naloxone (a prescription drug that reverses opioid overdoses) as well as access to substance use disorder (SUD) treatment, including medication assisted treatment for opioid use disorders.” 2(p 13)
Naloxone (Narcan®) is an opioid antagonist that was first approved in 1971 by the Food and Drug Administration (FDA) for use in opioid overdose reversals as an intravenous product. 3,4 Naloxone has a high affinity for the mu opioid receptor and antagonizes opioid effects through competition with opioids. Naloxone acts rapidly to temporarily reverse the effects of opioids to treat overdose; however, in patients who are not taking opioids, naloxone’s action at the opioid receptor has no clinical effect. New formulations of naloxone have been developed since 1971, including subcutaneous, intramuscular, and intranasal.
Naloxone distribution programs exist in many states to provide resources and training to medical professionals, as well as laypersons, for use. 5,6 This may include first responders such as police officers and other emergency personnel. In many circumstances, family or friends of an individual at high risk for opioid overdose may obtain the naloxone, as the product is not intended to be self-administered. 5,6 New Mexico was the first state to legally allow naloxone to be administered by an individual other than the person for whom it was prescribed. 7 Since New Mexico began this initiative in 2001, 24 other states and the District of Columbia have adopted similar changes in law protecting liability of administrators. 7
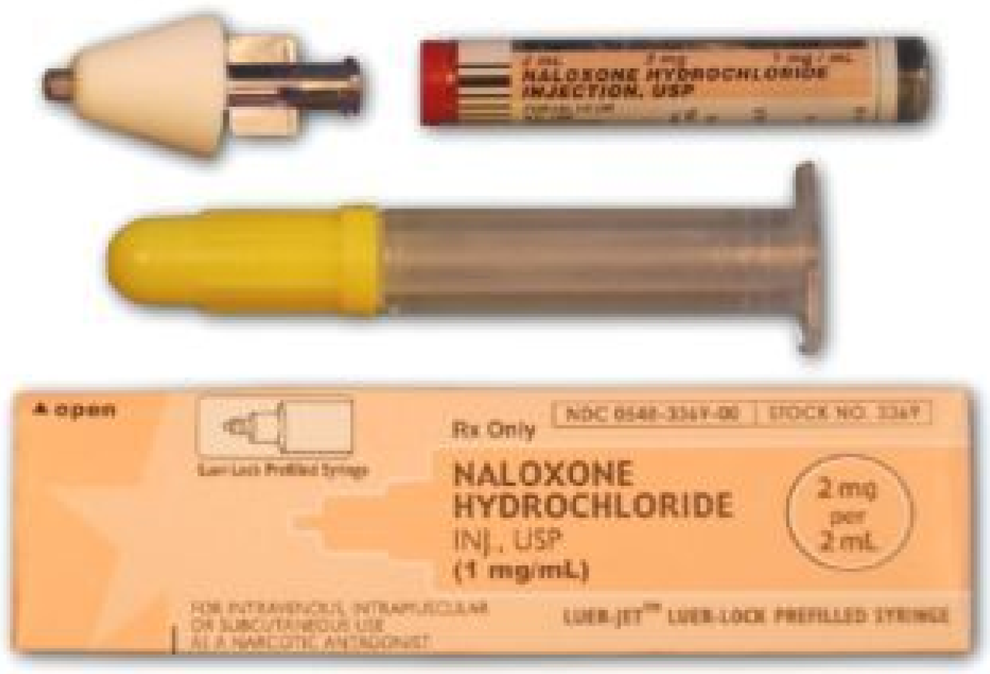
Common symptoms of an opioid overdose include pinpoint pupils, unconsciousness, and respiratory depression. Upon identification of an individual in respiratory distress from overdose, naloxone administration allows for a quick response from equipped bystanders and enables valuable extra time for emergency medical personnel to arrive on the scene to provide further care and deliver the overdose patient to the hospital for treatment. Many naloxone distribution programs have adopted the intranasal route for use in overdoses. 8 Approximately, 67 organizations reported to the Harm Reduction Coalition that they distributed intranasal naloxone to laypersons in 2013. 8 To create an intranasal spray, an atomizer adapter is placed on the end of an intravenous naloxone syringe (Figure 1). 8 Emergency medical service programs have now moved toward intranasal administration of naloxone since many of the patients needing naloxone are injection drug users; 80% of the injection drug user population in large metropolitan areas is hepatitis C positive or HIV positive. 9 Relative to intravenous administration, intranasal naloxone reduces the risk of exposure to blood-borne pathogens for both the patient and the person administering the medication.
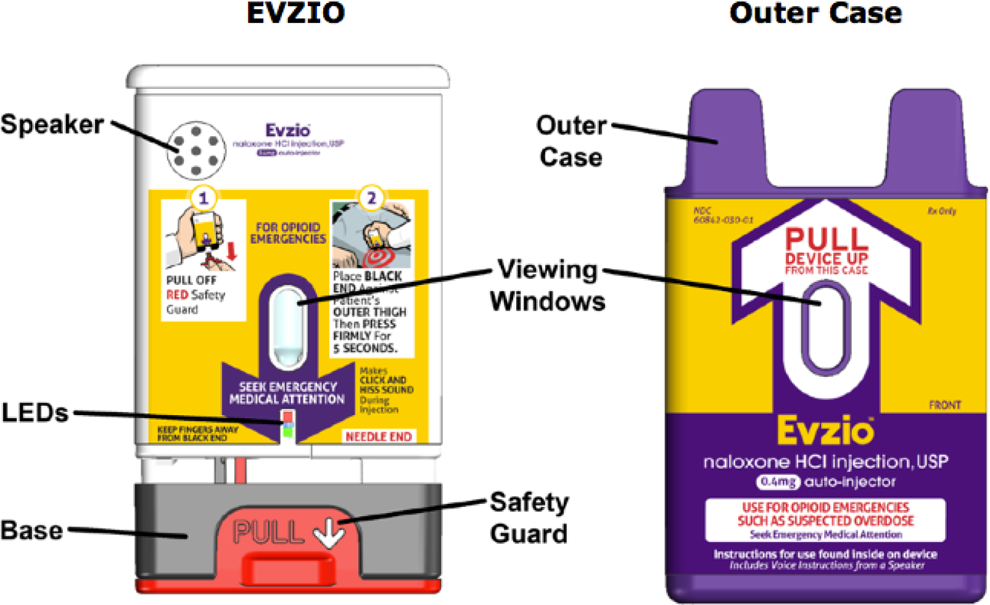
New formulations of naloxone continue to be introduced; in August 2014, the FDA approved a new formulation of naloxone for use as an intramuscular auto-injector known as Evzio® (Figure 2). 3 A newly designed nasal formulation that does not require assembly received FDA approval in November 2015. 4 The dose of naloxone administered is dosage form-dependent. The auto-injector can be administered intramuscularly or subcutaneously with an initial dose of 0.4 mg. 3 The nasal spray dose is 4 mg administered intranasally into 1 nostril. 4 If there is no response, additional doses can be administered every 2 to 3 minutes until emergency services arrive or a response is elicited and applies to both the auto-injector and intranasal products. 3,4
Methods
A literature review using the search engines Ovid, PubMed, and Google Scholar was performed using the following search terms: opioids, overdose, naloxone, Narcan, intranasal, intravenous, prescription pain killers, drug abuse, drug misuse, drug misadventures, hydrocodone, oxycodone, hydromorphone, morphine, fentanyl, heroin, Evzio, autoinjector, atomizer, first responders, and emergency medical technician. There were several inclusion criteria, which were publication in a peer-reviewed journal after 1995, articles published in the English language, studies conducted in an outpatient setting, as well as intramuscular, intranasal, intravenous, or subcutaneous dosage forms. The exclusion criteria for this search were review articles or editorials. This article compares the various routes of administration of naloxone in an attempt to determine the optimal route in the prehospital setting and later explores implications of this study for pharmacy practice.
Results
Based on the search criteria, 8 articles comparing the routes of administration of naloxone for opioid reversal were identified. The routes of naloxone administration compared in these studies include intravenous, intranasal, subcutaneous, and intramuscular. New naloxone dosage forms continue to be developed as the need for the drug continues to rise. Although new dosage forms offer additional portability and convenience, they may not always be the most affordable or available option; therefore, pharmacists must be familiar with all dosage forms. For this reason, the results of the literature search are presented in chronological order that allows practicing pharmacists to gain an appreciation for the development of various dosage forms and the advantages that each offers. A summary of the articles identified in the literature search is illustrated in Table 1.
Naloxone Route of Administration Results.a
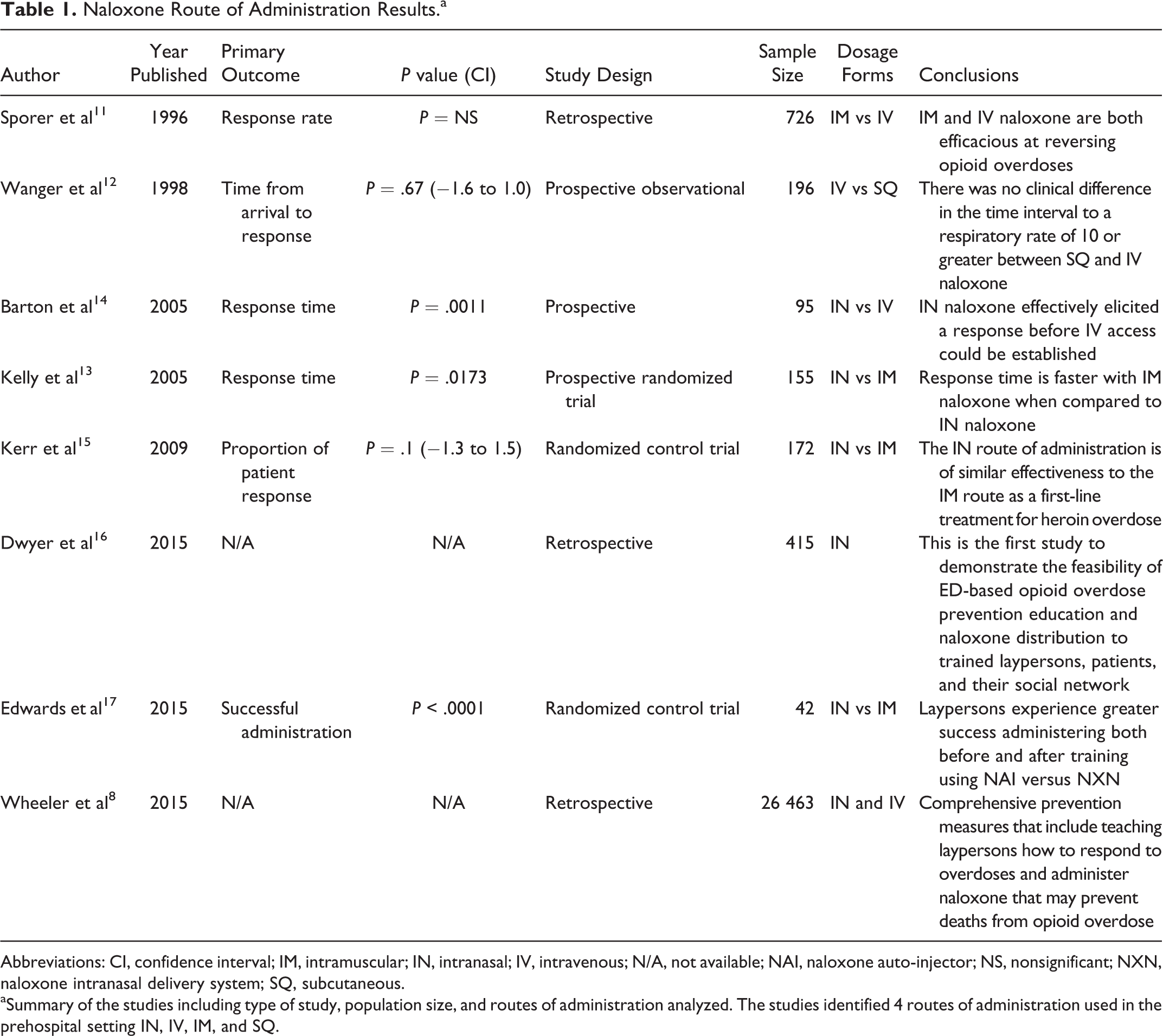
Abbreviations: CI, confidence interval; IM, intramuscular; IN, intranasal; IV, intravenous; N/A, not available; NAI, naloxone auto-injector; NS, nonsignificant; NXN, naloxone intranasal delivery system; SQ, subcutaneous.
aSummary of the studies including type of study, population size, and routes of administration analyzed. The studies identified 4 routes of administration used in the prehospital setting IN, IV, IM, and SQ.
One of the earliest studies comparing the routes of naloxone administration in the prehospital setting came from Sporer and colleagues in 1996. The authors compared the use of intravenous to intramuscular naloxone; in this study, all patients were treated by county paramedics. The study found that intramuscular naloxone was effective at reversing opioid overdoses in 94% of patients treated, compared to the 90% effectiveness observed in intravenous administration. Reversal was considered effective if an improvement in respiratory rate greater than or equal to 10 breaths per minutes was found and if a Glasgow Coma Scale (GCS) greater than or equal to 14 was observed within 5 minutes of administration. The GCS is a method used to assess consciousness by evaluating motor response, verbal responses, and eye opening. 10 In noncardiac arrest patients, intramuscular naloxone was preferentially selected 80% of the time. Intravenous naloxone was utilized in 11% of noncardiac patients, and the remaining 9% of noncardiac patients used a combination of both intramuscular and intravenous naloxone. 11
A publication from 1998 compared intravenous to subcutaneous naloxone in the prehospital setting. 12 In this study, the authors focused on the time needed for naloxone to take effect. Response was measured as the time to reach greater than or equal to 10 breaths per minute. A response was elicited at 3.8 minutes after the administration of intravenous naloxone. Subcutaneous administration produced a response at 5.5 minutes. The authors also analyzed the time from initial contact of the first responder to response; for intravenous naloxone, 9.3 minutes elapsed before response was seen, compared to 9.6 minutes for subcutaneous naloxone. However, the difference in time from contact between intravenous naloxone and subcutaneous naloxone was not found to be statistically significant. In this study, a second dose was administered if symptomatic improvement was not noted within 5 minutes of administration. In the intravenous group, 35% of patients required 2 doses for response compared to 15% in the subcutaneous group. It should be noted the dose was 0.4 mg for intravenous compared to 0.8 mg for subcutaneous. Administrators of the naloxone reported a preference for the subcutaneous formulation due to perceived decrease risk of exposure to patient blood.
In an article from Kelly and colleagues published in 2005, intranasal naloxone was compared to intramuscular naloxone when used by paramedics in the prehospital setting. 13 The primary outcome measure was the time for response of a patient to achieve greater than or equal to 10 respirations per minute. Patients in the intramuscular group achieved response quicker with a mean time of 6 minutes compared to 8 minutes for intranasal. A secondary outcome was achieving a GCS score over 11 within 8 minutes. There was no statistical difference in the time to respond based on the GCS between intranasal and intramuscular naloxone. Although not statistically significant, 74% of patients responded after 1 dose in the intranasal naloxone group compared to 87% response in the intramuscular naloxone group. Adverse effects of each route were also analyzed; in the intramuscular naloxone group, 13% of patients reported agitation and/or irritation compared to the 2% in the intranasal route.
An article from 2005 by Barton and colleagues compared intranasal naloxone to intravenous naloxone. 14 In this study, intranasal naloxone was merged into their standard protocol. If patients responded to intranasal naloxone before intravenous access could be established, then no further naloxone was administered. Once venous access was established, the patient’s response was reassessed. If response was not noted, then a second dose of naloxone was administered via the intravenous route. The authors found that 83% of individuals responded to intranasal naloxone alone. A limitation of this study was that intravenous naloxone was administered immediately upon gaining access. Intranasal naloxone was not provided with adequate time to take full effect in all cases. The median response time for intranasal naloxone alone was noted to be 4.2 minutes following administration. The response time for a dose of intranasal followed by intravenous naloxone was 3.7 minutes. The patients who received intranasal followed by intravenous naloxone essentially received a double dose before response was noted. However, there was a larger discrepancy in the time to response from initial contact by a first responder. The mean response time for intranasal naloxone was 9.9 minutes, whereas for intravenous naloxone was 12.8 minutes.
In 2009, Kerr et al compared intranasal to intramuscular naloxone for the reversal of opioid overdose when used by paramedics in the prehospital setting. 15 Response in this study was defined as spontaneous respiration at a rate of greater than or equal to 10 per minute and/or GCS greater than or equal to 13. Intranasal naloxone was successful in reversing overdose in 82% of patients. The difference in time from ambulance call to administration of naloxone was comparable, with 13.1 minutes for patients treated intranasally and 13.4 minutes for those treated intramuscularly. No statistical difference was noted in the efficacy. 15 Patients responded within 10 minutes in 72.3% of cases for the intranasal group compared to 77.5% in the intramuscular group. Additionally, there was no statistically significant difference in response time reported between the intranasal and intramuscular, which were 8.0 and 7.9 minutes, respectively.
A study published in 2015, conducted by Dwyer et al, analyzed the impact of naloxone distribution at the time of discharge from the emergency department. 16 Conducted in Boston, Massachusetts, between 2011 and 2012, 415 patients were studied. The subjects were split into 2 groups: overdose education only and overdose education and naloxone distribution groups. Patients in the overdose education and naloxone distribution group were given nasal naloxone kits with 2 atomized 2 mg naloxone vials at no cost. Roughly 16% of the individuals provided intranasal naloxone reported use for reversing an opioid overdose. Interestingly, subjects in the overdose education and naloxone distribution group reported increased rates of dialing emergency services, administering naloxone, and observing the patient until emergency services arrived compared to those in the overdose education only group.
The usability of naloxone in the intranasal and intramuscular auto-injector form was compared in an article by Edwards and colleagues. 17 The authors found that without training, 90.5% of users could properly administer naloxone via the auto-injector. Of 42 participants, none were able to correctly administer naloxone via the intranasal route; this was due to the necessity for the atomizer needing to be attached to the syringe prior to use. Participants were properly instructed on how to use the auto-injector or assemble the nasal formulation and tested 7 to 8 days post instructions. One week after instruction, 100% of participants could accurately use the auto-injector compared to 57.1% for intranasal administration. It was noted that the time to complete administration was different between groups: prior to training, the average time to administer naloxone was 0.9 minutes for the auto-injector compared to 6 minutes for assembly and administration of the intranasal formulation. With proper instruction, these times were reduced to 0.5 and 2 minutes for auto-injector and intranasal, respectively. The difference in time until complete administration was statistically significant.
A study conducted by Wheeler and colleagues analyzed the distribution of naloxone across several states. 8 There were 136 organizations surveyed regarding their distribution of naloxone for opioid reversals. Approximately 152 283 individuals were reportedly dispensed naloxone in either intravenous or intranasal formulation. There were 26 463 opioid reversals reported between 1996 and June 2014. This is an indication that widespread use of naloxone for opioid overdose reversal is a more recent development. Of the organizations studied, injectable naloxone was utilized 79.7% of the time, whereas intranasal naloxone was used 20.3% of the time.
Discussion
Several of the studies demonstrated the near-equal efficacy of the 4 dosage forms of naloxone used in the prehospital setting and all of the dosage forms were capable of reversing the effects of an opioid overdose. Intramuscular and intranasal formulations were specifically compared for efficacy in 2 studies with differing conclusions. Kerr et al concluded that the intramuscular and intranasal formulations have equal time in response for respiratory depression. 15 Kelly et al found that although both dosage forms are capable of reversing respiratory depression, the intramuscular dosage form is more effective. 13 This conclusion was based on the observation that intranasal naloxone had a slower response time as well as a higher proportion of patients requiring an additional dose compared to the intramuscular form. Both of these studies used trained paramedics as administrators. The studies demonstrate the efficacy of naloxone in the prehospital setting but may not apply when used by laypersons for opioid overdose reversals. Any dosage form is capable of reversing overdose when administered correctly, so other factors should be considered. These include adverse effects of different dosage forms, the response time from administrator arrival, response time from naloxone administration, the administrator’s preference, and the financial impact.
In general, adverse effects of naloxone are expected to be similar across the dosage forms. However, differences may arise from the route of administration. Only 1 study analyzed the differences in adverse events among dosage forms. The side effects of the intramuscular and intranasal formulations included agitations/irritation, nausea/vomiting, headache, tremor, and sweating. 13 The side effects described are expected to be observed in all dosage forms. There were less notable side effects associated with the use of intranasal naloxone compared to intramuscular. Patients receiving the intramuscular form were noted to have significantly higher levels of agitation/irritation. 13 Kelly et al suggest this may be due to more rapid response and absorption with the intramuscular dosage form. They also suggest the increased agitation/irritation may be advantageous for the intranasal formulation. 13 Overall, there appears to be little difference in the dosage forms with regard to side effects.
The response time from administrator arrival is an important factor to consider. The findings by Wanger et al support the notion that intravenous and subcutaneous have similar response times when considering the arrival of help from first responders until response. 12 The study by Barton et al further demonstrated that the time from arrival until response between the intravenous and intranasal formulation was not statistically significant. 14 The intravenous, subcutaneous, and intranasal dosage forms are equal when considering their time from arrival until response. However, there were no studies identified that analyzed the time from arrival until response for the intramuscular dosage form. The subcutaneous and intranasal dosage forms can be administered much more quickly because intravenous access does not need to be established. In the studies evaluated, several minutes typically elapsed prior to the use of intravenous naloxone. 12,14
The response time from naloxone administration until improvement in overdose symptomology is important to consider. The different dosage forms had varying reported times to take effect. The benefit of a more rapid response with intranasal compared to intravenous naloxone can be lifesaving in practice. 14
Administrator preference should also be taken into consideration when selecting the optimal dosage form of naloxone in the prehospital setting. There is a higher risk of exposure to blood-borne pathogens when intravenous access needs to be established. The intranasal and intramuscular auto-injector formulations provide a safer alternative for the administrator by minimizing the risk of exposure to blood-borne pathogens. 14 Although intravenous use is associated with the highest risk of blood-borne pathogens, it is overwhelmingly the most common dosage form of naloxone utilized as of June 2014. 8 With regard to administrator safety, intranasal and intramuscular naloxone are underutilized in the prehospital setting.
There is a disparity in the amount of training required to properly administer naloxone. Intravenous administration would require extensive training in order to be used properly in the general public, making it a less than ideal dosage form. Minimal training is required for proper use with the intranasal and intramuscular formulations. No studies identified analyzed the training required for subcutaneous use. Instructions regarding the attachment of the atomizer to the syringe are necessary to prepare the dosage form for intranasal use. Additionally, the technique for intranasal delivery is an essential component. The FDA approved a nasal formulation of naloxone that does not require an assembly in November 2015. 4 This should improve the ability of laypersons to administer intranasal naloxone correctly. A preference by administrators for intramuscular over intravenous naloxone was observed in the article by Sporer et al. 11 Furthermore, Edwards et al demonstrated that the intramuscular auto-injector requires almost no training to be used properly. Over 85% of laypeople are capable of administering the auto-injector correctly with no prior training. 17 This high percentage is likely due to the auto-injector providing audio instructions on proper administration technique. The intramuscular dosage form is superior to the intranasal and intravenous formulations when considering the amount of training required.
Finally, the financial impact of each dosage form should be considered. The difference in cost is significant between dosage forms. Intravenous and subcutaneous were noted to be the least expensive costing around US$9 per dose. 18 An intranasal naloxone kit was valued at US$55 mainly due to the cost associated with acquisition of the atomizer. 16 The intramuscular auto-injector was reported with the highest cost, in the range of US$400 to US$600. 19
The article by Wheeler et al analyzed naloxone distribution for out-of-hospital use for nearly the last 20 years; however, half of the organizations studied began their distribution of naloxone after January 2013. This is an indication that widespread use of naloxone for opioid overdose reversal in the prehospital setting is a more recent development. Laws related to limiting liability for administration from bystanders have also gained momentum in the past 5 years. Nearly half of the United States now have Good Samaritan laws for naloxone administrators when used in good faith. 7
Pharmacies throughout the United States are working to make naloxone more accessible to the public through the use of collaborative practice agreements. As of August 2016, CVS Corporation, retail pharmacies in 30 states have the ability to dispense naloxone to patients without a prescription. 20 On August 10, 2016, the FDA announced they are “exploring options to make naloxone more available to treat opioid overdose” and stated they intend to facilitate the development of over-the-counter naloxone. 21 The major barrier to transition from prescription to over-the-counter naloxone lies in creating a consumer-friendly Drug Facts Label (DFL). 21 The DFL is intended to aid patients in the correct administration technique without the help of a health-care professional. 2
There are several limitations of this literature review. There is a limited amount of randomized controlled trials analyzing the different routes of naloxone administration in the prehospital setting. More research is needed in the area of naloxone distribution to identify which dosage form is optimal for treatment prior to arrival to the hospital. Studies comparing the various routes head-to-head would provide guidance in future practice. Factors such as response time from first responder arrival, response time from administration, administrator preference, adverse events, and financial impact need to be taken into consideration.
As discussed previously, there are a variety of strategies being utilized with naloxone to address the issue of opioid abuse. In the United States, the use of rescue naloxone for opioid overdose in the prehospital setting has gained momentum in recent years. However, due to varying positive and negative attributes involved with administration route, there is little consensus on naloxone delivery in the prehospital setting. Little training is required for proper administration of the intramuscular auto-injector. However, the high price is a barrier to access and widespread adoption. Intranasal naloxone appears to be the optimal dosage form when considering cost, effectiveness, and administrator safety.
Implications for the Practice of Pharmacy
Opioid overdose is a serious public health threat that affects not only the individuals at risk of overdose but also their families, friends, and communities. As access to naloxone in the community increases across the United States, pharmacists must be prepared to address concerns about naloxone use, promote naloxone availability, speak to the Good Samaritan laws that protect caregivers and bystanders who may administer naloxone, and educate on the proper use of naloxone delivery methods. Proper training on the use of various naloxone administration devices can mean the difference between life and death for an individual suffering from an opioid overdose. Pharmacists must seek ways to ensure that their pharmacy can provide patients and community members with the most affordable and most user-friendly naloxone dosage form available, with individual pharmacists as well as the profession seeking to explore avenues for reimbursement of dispensing costs. Pharmacists must be willing to provide training on not only the use of the dosage form but also the importance of seeking medical assistance after using naloxone. Because it has been shown that speaking with someone about treatment after a nonfatal overdose is associated with treatment seeking, 22 a pharmacist who is able to refer patients and/or their families to SUD treatments may be able to offer assistance in helping a patient on the path to recovery and long-term sobriety.
Pharmacists must also assess each patients risk for opioid overdose, mitigate that risk whenever possible, and provide thorough patient counseling on the risk factors for opioid abuse and what patients’ can do to lower their risk. 23 Pharmacists must remain vigilant in reminding themselves of the risk factors for opioid overdose, including high doses of opioid therapy, opioids used concomitantly with other sedating medications, and known or suspected opioid dependence, in particular following reduced tolerance after detoxification, release from incarceration, or cessation of treatment. 24,25 An awareness of medical conditions that may put patients at a higher risk of opioid overdose, including depression and HIV, 26 will also help pharmacists to provide proper individualized counseling and screening.
It has been demonstrated that in the emergency department setting, counseling can reduce risky opioid use among certain patients. 27,28 Although pharmacist patterns in screening and discussing opioid misuse with patients has been explored, the role that counseling provided by a pharmacist might provide in reducing opioid misuse has not been adequately studied. 23
Green and colleagues have explored the advantages of various models of community pharmacy–based naloxone distribution, comparing the case of a collaborative pharmacy practice agreement model in Rhode Island with a standing order model in Massachusetts. 29 In their manuscript, Green and colleagues provide state-specific examples that are immediately implementable within existing regulatory frameworks of many US states. 29
To effectively combat the opioid abuse epidemic, pharmacists should be open to the opportunity for engagement within their communities. Pharmacists must be willing to partner with their communities, collaborating with other professionals and other agencies to find community-specific solutions to the opioid crisis. 30 This could include planning forums to address community needs, serving on established drug abuse task forces and coalitions, advisory boards, drug court teams, and other partnerships with public health, local community members, health-care organizations, and schools. All pharmacists, regardless of practice setting or location, can collaborate with prescribers and other health professionals to formulate policies and protocols for dispensing naloxone, help train providers and patients, and aid in circulating information throughout the community and the profession. 31 Although naloxone distribution can save the lives of individual patients, community and population-based interventions are needed if the opioid abuse epidemic is to be properly addressed and resolved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
{kind=link}
{kind=link}