
Abstract
Nationally, the prescription of opioids for acute and chronic pain is increasing. As opioid use continues to expand and become of increased concern for health-care practitioners, so do the adverse effects and long-term management of those effects. Opioid-induced constipation (OIC) presents a unique challenge because tolerance does not develop to this particular adverse effect, making chronic pain management a delicate balance between relieving pain and preventing long-term adverse effects such as constipation and dependence. Several agents have been developed for the treatment of OIC in patients with chronic noncancer pain on the basis of short-term studies of 12 weeks or less. However, chronic pain management often extends beyond this 12-week boundary, resulting in health-care professionals questioning the safety and efficacy of continued treatment with OIC agents. This review evaluates available literature on long-term treatment of OIC in patients with chronic noncancer pain with lubiprostone, naloxegol, and methylnaltrexone as well as preliminary results of the recently completed naldemedine long-term trial, COMPOSE-3.
Introduction
Approximately 20% of patients who present with noncancer acute or chronic pain receive an opioid prescription, resulting in 259 million prescriptions for opioid pain medications in the United States in 2012 alone. 1 Furthermore, the Centers for Disease Control reports that the prescription of opioid medications is increasing in the United States. 1 The increase in use of opioids carries with it an inherent increase in the potential for adverse events. Common adverse effects of opioids include constipation, dry mouth, nausea, vomiting, drowsiness, confusion, and the potential for physical dependence and withdrawal symptoms when discontinued. 1 Recent clinical guidelines have refocused efforts on evaluating ongoing need for long-term opioid therapy and minimizing opioid use to reduce adverse events, including the possible development of psychological dependence and addiction. 1 In those patients for whom long-term therapy is deemed appropriate, management of the adverse effects may require additional medications or nonpharmacologic therapies.
Opioids act on the opioid receptor, a G-protein-coupled receptor distributed throughout the body with the highest distribution in the central nervous system. The opioid receptor has 3 main subtypes—μ, δ, and κ. Within the gastrointestinal (GI) tract, the μ-opioid receptor remains the predominant receptor subtype. 2,3 Activation of opioid receptors in the GI tract leads to constipation through multiple mechanisms, with the overarching themes of decreased bowel secretions and decreased peristaltic movements with increased sphincter tone. 4
Opioid-induced constipation (OIC) is unique from other opioid adverse effects in those patients who rarely develop tolerance, 4 which has implications for patients on long-term opioid therapy for chronic pain management. Because of varying definitions, there are a wide variety of reports on the true incidence rate for OIC; however, it has been reported to affect between 30% and 57% of patients taking opioids for chronic noncancer pain. 5 -7 Wherever the true incidence lies within the reported range, it is clear that a large proportion of patients prescribed opioids are affected and have a potential need for long-term OIC therapy. The objective of this review is to examine available evidence on the long-term safety and efficacy of Food and Drug Administration (FDA)-approved OIC agents and to identify any factors that may influence a patient-specific therapy decision.
Effects on Quality of Life and Pain Management
OIC is reported as the most common and bothersome adverse effect by patients and negatively impacts health-care resource utilization, work productivity, and quality of life. 8,9 Patient perception of OIC and the associated responses to it can affect and complicate pain management. In 1 international survey, 1 in 3 patients reported missing or decreasing their opioid medications to relieve constipation. 8 Furthermore, a vast majority (86%) of those patients who self-adjusted their opioid therapy due to constipation experienced increased pain that produced a patient-reported moderate-to-great or great impact on quality of life. 8
Despite the consequences of OIC, it often goes unrecognized or underestimated by health-care providers. In the delicate balance of relieving pain and preventing constipation, health-care providers were shown to be more aware of patients’ pain than constipation. 10 When providers and patients were simultaneously surveyed, they were in agreement on average pain scale scores but vast discordances in OIC treatment and relief were discovered. While about half (49%) of patients surveyed reported moderate to complete interference with pain management, a majority (73%) of health-care providers reported pain was mostly or adequately managed. Furthermore, when the majority of patients (73%) reported little or no benefit of laxative therapy, over half (53%) of health-care providers were reporting moderate to complete patient satisfaction with constipation relief. 10 These discordances highlight the need for a greater awareness of OIC to allow more systematic treatment.
Approaches to Treatment
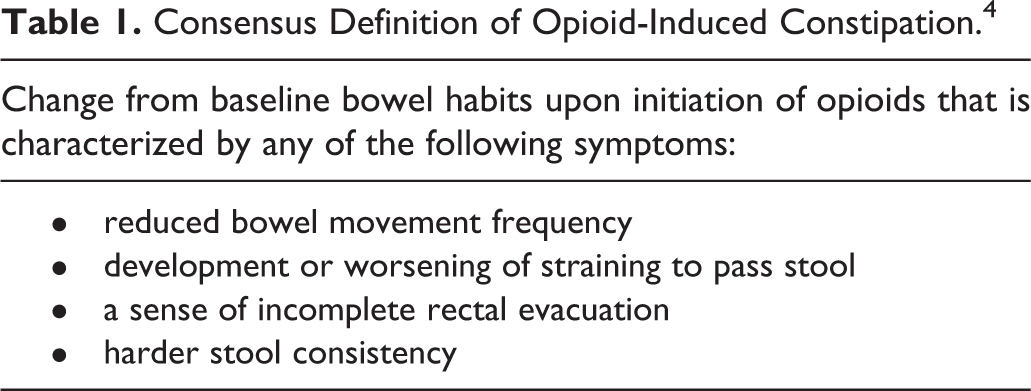
Fundamental to greater awareness and systematic therapeutic approaches are standardized definitions of the disease and implementation of validated assessment tools. A multidisciplinary consensus panel formed by the American Academy of Pain Medicine and endorsed by the American Gastroenterological Association convened in 2015 to address the assessment of OIC and an appropriate threshold to advance therapy. 11 The panel adopted a definition put forth by Camilleri et al in their proceedings, which incorporates both patient-reported subjective and objective measures (Table 1). 4 The Bowel Function Index (BFI) was recommended as the primary assessment tool for OIC on the basis of validation and practicality. The BFI is a 3-item questionnaire administered by a health-care provider to determine patient assessment of ease of defecation, incomplete bowel evacuation, and constipation rated on a scale from 0 to 100 over a 7-day recall. Patients are instructed to consider a score of 0 equivalent to an assessment of no symptoms and a score of 100 to be very strong symptoms. The scores for each component are then averaged to produce a BFI score, with the minimum possible score being 0 and the maximum 100. The panel recommends a threshold score of 30 or greater after optimization of prophylactic and first-line therapy to consider therapy intensification with a novel prescription agent. However, due to the high cost and limited experience with novel agents, the panel continues to recommend traditional first-line approaches for patients with BFI scores <30. When appropriate, additional assessment tools such as changes from baseline bowel movement frequency or the visual Bristol Stool Form Scale can be employed. 11
Consensus Definition of Opioid-Induced Constipation. 4
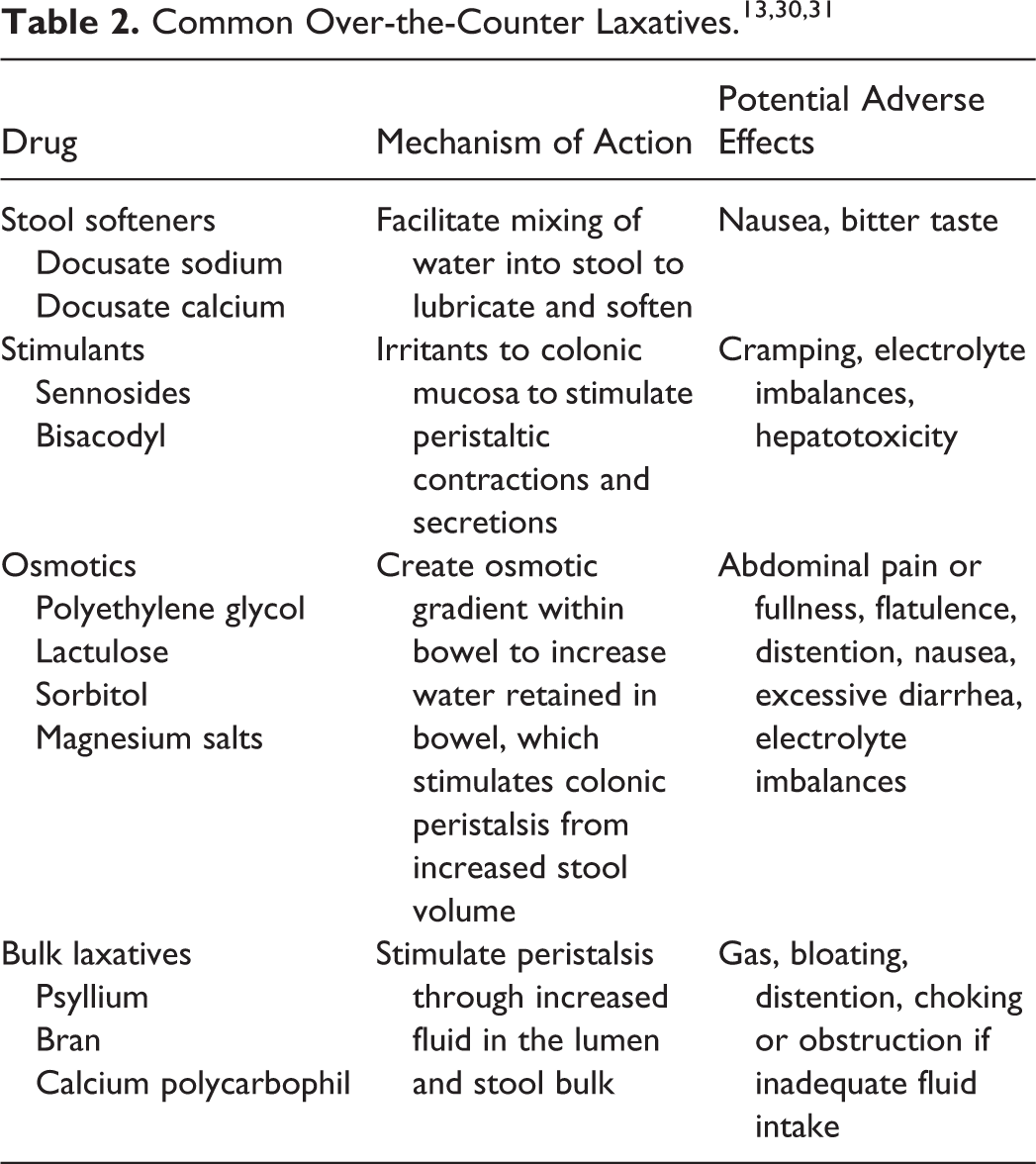
Clinical guidelines for the use of chronic opioid therapy in noncancer pain recognize the risk of OIC and recommend prophylactic nonpharmacological and pharmacological therapy. 1,12 Nonpharmacological measures should include counseling to increase dietary fiber, fluid intake, and physical exercise. 13 It is widely recognized that the evidence behind traditional prophylactic therapy is largely anecdotal; in fact, surveyed patients with sufficient laxative use, defined as using laxatives at least 4 days out of a 14-day period, reported some benefit but remaining dissatisfied with their therapy. 14 However, due to low cost and vast experience, coupled with relatively advantageous safety profiles, over-the-counter laxatives continue to be considered first-line agents for OIC. Available agents are summarized in Table 2. No over-the-counter agents target the underlying pathophysiology of OIC, but it may be possible to mechanistically address OIC with a combination of a stool softener targeting decreased bowel secretions and a stimulant laxative to address decreased peristalsis. For this reason, a combination of a stool softener and stimulant is commonly prescribed in clinical practice for OIC.
Advances in Pharmacotherapy—Short-Term Use of Novel Agents
While nonprescription therapies remain first-line for prophylaxis and treatment, novel prescription therapies for OIC are also available. A brief review of each of these agents is available in Table 3. The first novel agent approved for OIC in patients with noncancer pain, lubiprostone, targets chloride channels to increase intestinal fluid secretion. 15,16 Lubiprostone is orally active and was originally approved for use in chronic idiopathic constipation before its efficacy in OIC was demonstrated. Lubiprostone does not interact with the cytochrome P450 system, greatly reducing the number of expected drug interactions. 15 However, in vitro studies have revealed that methadone may interfere with the action of lubiprostone on chloride channels, indicating concomitant use of methadone may attenuate the clinical impact of lubiprostone. 17 Metabolites of lubiprostone are primarily excreted in the urine, although there is no dosage adjustment required for renal dysfunction. 15
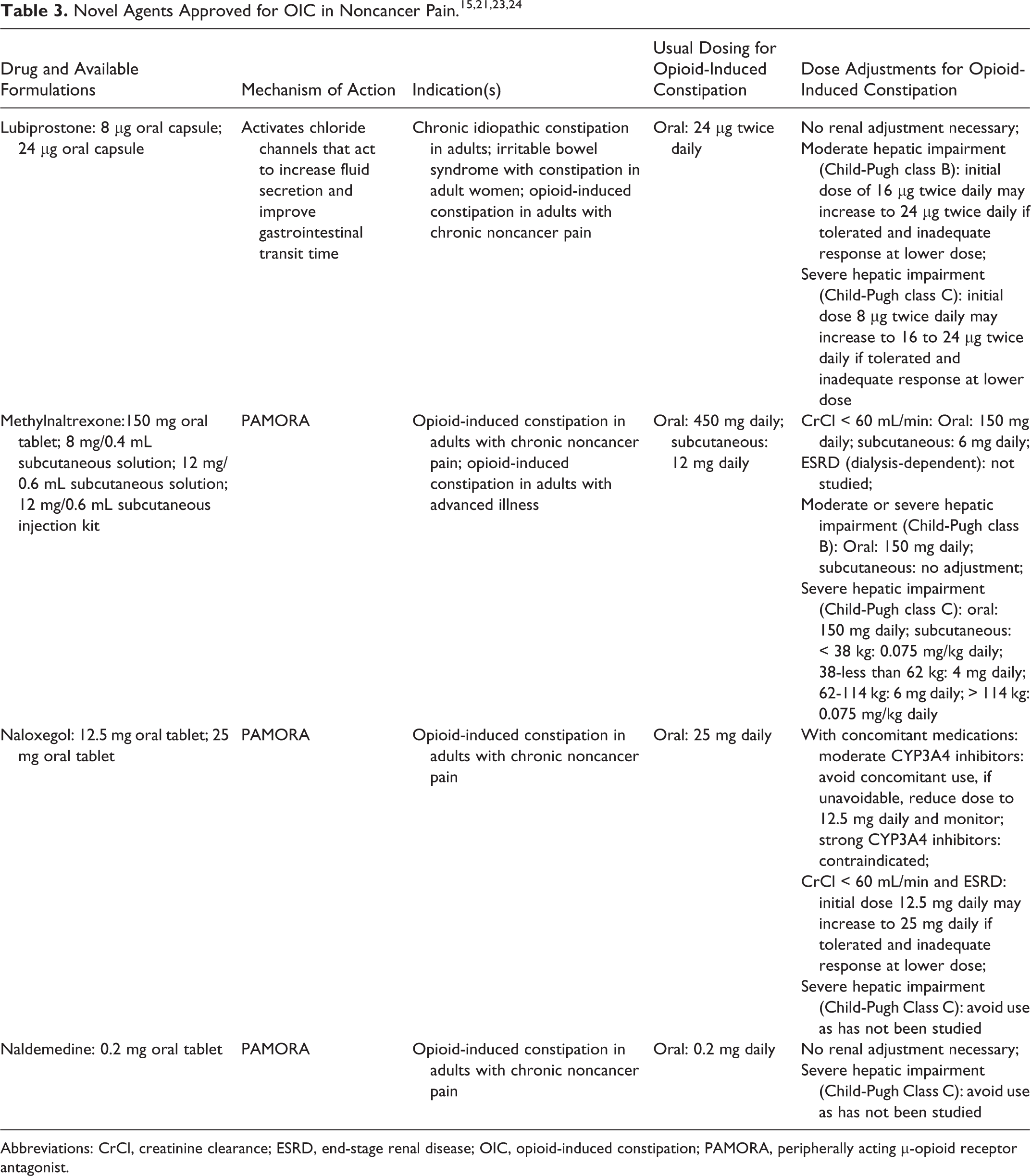
Abbreviations: CrCl, creatinine clearance; ESRD, end-stage renal disease; OIC, opioid-induced constipation; PAMORA, peripherally acting μ-opioid receptor antagonist.
Two 12-week trials were conducted to assess the safety and efficacy of lubiprostone in comparison to placebo in patients with OIC treated for noncancer pain. In a study of 418 patients, Cryer et al demonstrated an increase in spontaneous bowel movement frequency after 8 weeks of lubiprostone 24 μg by mouth twice daily (3.3 vs 2.4; P = .005). The increase was also present at week 12 of treatment (2.2 vs 1.6; P = .004). 18 Similarly, Jamal et al showed an increase in spontaneous bowel movement frequency from 2.4 to 3.2 per week (P = .001) in a study of 431 patients randomized to either lubiprostone 24 μg or placebo. 16 They also demonstrated an overall response characterized by increase in spontaneous bowel movements by ≥1 over baseline each week and a sustained rate of ≥3 spontaneous bowel movements per week in at least 9 of the 12 study weeks (27.1% vs 18.9%; P = .030). 16 Jamal et al also demonstrated a significantly shorter median time to spontaneous bowel movement following administration of lubiprostone over placebo (23.5 hours vs 37.7 hours; P = .004). The decreased time to bowel movement correlated with significantly more patients having spontaneous bowel movements within 4, 8, 12, 24, and 48 hours of lubiprostone administration (P ≤ .009 for each comparison to placebo). 16 Cryer et al also demonstrated shorter median times to a spontaneous bowel movement following lubiprostone compared to placebo (28.5 vs 46.0 hours), but the result did not reach statistical significance. 18 Safety analyses in both trials were similar, with diarrhea, nausea, and abdominal pain or distention being significantly more common in the lubiprostone treatment groups. There was some variation in the rates of each of these adverse effects, with nausea being more common in the Cryer et al study (15.4%) than in the Jamal et al (8.5%). Diarrhea, abdominal pain, and distention had similar rates. 16,18
More recently approved OIC agents are the peripherally acting μ-opioid receptor antagonists (PAMORAs). Alvimopan is a PAMORA that is indicated only for short-term use in hospitalized patients to relieve postoperative ileus; it carries a warning for potential risk of myocardial infarction with long-term use and would not be expected to be used for OIC. 19 However, there are 3 other agents in the class that have been studied and approved for OIC.
Naloxegol is an orally active derivative of naloxone that contains a polyethylene glycol moiety to confer peripheral selectivity (as a P-glycoprotein substrate) and increased bioavailability. 20,21 Because it relies upon P-glycoprotein to maintain peripheral selectivity and is also a substrate of the CYP3A enzyme system, naloxegol has numerous drug interactions to consider. It is contraindicated with strong CYP3A4 inhibitors, and a reduced dose is recommended for patients concomitantly prescribed a moderate CYP3A4 inhibitor due to the possibility of increased naloxegol levels and potential adverse events. 21 Naloxegol metabolites are excreted primarily in the feces, with minor amounts of renal excretion.
Short-term studies of naloxegol were performed in 2 identical 12-week trials to establish its safety and efficacy in the patient population with noncancer pain. 20 Although there were discordant results between the 2 trials on the efficacy of naloxegol 12.5 mg by mouth daily, each trial showed a response rate that was significantly higher with naloxegol 25 mg daily than with placebo (44.4% vs 29.4%, P < .05 and 39.7% vs 29.3%, P < .05). Responsive patients were those that had ≥3 spontaneous bowel movements per week and an increase in 1 spontaneous bowel movement per week over baseline for at least 75% of the study period. Importantly, this efficacy was maintained in a subgroup analysis of patients who were previously deemed unresponsive to laxative treatment. Furthermore, both trials showed a significantly shorter median time to spontaneous bowel movement following the administration of naloxegol 25 mg when compared to placebo (12.0 hours vs 37.2 hours, P < .001 and 5.9 hours vs 35.8 hours, P < .001). Mean opioid daily doses and pain scores remained relatively stable and similar to placebo in both studies, and only 1 of the 4 reported cardiovascular events was considered related to study drug. The related cardiovascular event occurred in the placebo group. GI adverse events were the most common in the two 25 mg studies, with abdominal pain (12.6% and 19%), diarrhea (9.3% and 9.1%), and nausea (7.5% and 9.6%) reported most often.
Methylnaltrexone bromide is a PAMORA with peripheral selectivity due to a quaternary amine group that prevents its passage across the blood–brain barrier. It was first approved for OIC in patients with cancer and later gained approval for patients without cancer; although originally developed and approved only as a subcutaneous injection, an oral methylnaltrexone bromide tablet was approved by the FDA in 2016. 22,23 Methylnaltrexone is excreted primarily as the parent drug in the urine, with a secondary minor excretion pathway in the feces. The subcutaneous injection bypasses first-pass hepatic metabolism, and thus patients using this dosage form are exposed to lower concentrations of active metabolites than those receiving the oral tablets. The oral dosage form requires dose adjustments at lower levels of hepatic impairment than the subcutaneous injection due to the possibility for overexposure to methylnaltrexone when the first-pass effect is diminished due to hepatic dysfunction following oral administration. 23
The efficacy and safety of methylnaltrexone in patients with noncancer pain was demonstrated in a 12-week trial that randomized 469 patients to either subcutaneous methylnaltrexone 12 mg daily, every other day, or placebo for 4 weeks. The first dose of methylnaltrexone was more likely to produce a bowel movement within 4 hours than placebo (34.2% vs 9.9%; P < .001), and similar results were seen in the daily and every other day dosing groups. Additionally, 28.9% of injections in the daily dosing group and 30.2% in the every other day dosing group produced a bowel movement within 4 hours, which was significantly higher than the placebo group in both instances (P < .001). Almost half of patients in the methylnaltrexone treatment groups experienced a treatment-emergent adverse event (49.3% in daily group, 45.3% in every other day), compared to 38.3% in the placebo group. Events were most often GI, and abdominal pain (19.3% in daily group, 15.5% in every other day group), diarrhea (6.0% in daily group, 11.5% in every other day group), and nausea (8.7% in daily group, 11.5% in every other day group) were all more common in the treatment groups than placebo. There was little reported difference in pain scores and opioid withdrawal assessments with no statistically significant findings. 22
Naldemedine was approved in 2017, making it the newest commercially-available member of the PAMORA class, and is a derivative of naltrexone with peripheral selectivity that also acts as a P-glycoprotein substrate. 24 Naldemedine is metabolized primarily by the CYP3A enzyme system, which introduces the possibility of many drug interactions. Furthermore, it is a substrate of P-glycoprotein and thus interacts with P-glycoprotein inhibitors with the potential for increased naldemedine-mediated adverse effects. 24 Naldemedine metabolism forms 2 primary active metabolites with lesser potency than the parent drug, which are then excreted in the urine and feces. 24
Two identical 12-week randomized, controlled trials (COMPOSE-1 and COMPOSE-2) were completed to assess the efficacy and safety of naldemedine. 25 Patients were randomized to receive either naldemedine 0.2 mg orally daily or placebo and were not permitted to use other laxatives during the trial outside of rescue medications after 3 days without a bowel movement. In both trials, the naldemedine group was more likely to respond to therapy (COMPOSE-1 47.6% vs 34.6%, P = .002 and COMPOSE-2 52.5% vs 33.6%, P < .0001). Furthermore, naldemedine treatment resulted in a greater increase in weekly spontaneous bowel movements, presented as least square mean difference between naldemedine and placebo, despite similar frequencies in all groups at baseline (COMPOSE-1 1.30 spontaneous bowel movement/week, P < .0001 and COMPOSE-2 1.40 spontaneous bowel movement/week, P < .0001). Naldemedine did result in higher rates of adverse effects, most commonly GI in nature and reported as abdominal pain (5%-6% vs 1%-2%), diarrhea (7%-9% vs 2%-3%), and nausea (5% vs 3%). There were events of possible opioid withdrawal in all groups, but rates were low (1%-2% in naldemedine groups) and not supported by changes in pain intensity scores or opiate withdrawal scale scores.
Each OIC agent has been shown to be safe and efficacious in short-term trials of up to 12 weeks, and their proposed place in therapy using the BFI was described by the OIC consensus group. In 2005, an estimated 9.6 to 11.5 million adults were prescribed long-term opioid therapy, 1 and with increases in opioid prescribing nationally, this number is expected to have grown considerably. With the rise in opioid use and the knowledge that OIC is an adverse effect to which patients do not develop tolerance, the question of long-term safety and efficacy arises. Examining available long-term data could aid in selecting OIC therapy for patients remaining on long-term opioid medications.
Literature Review
A search of the literature using the MEDLINE database (1946-June 2017) with the search terms “opioid,” “constipation,” and “noncancer” revealed 91 publications. The search was not limited by publication date or language. Sixteen trials regarding the treatment of OIC were identified. Trials examining treatment periods of 12 weeks or less were excluded. Three trials were included in the analysis evaluating the long-term use of lubiprostone, naloxegol, and methylnaltrexone for patients with noncancer pain and OIC (see Table 4). However, this literature search did not identify any trials of naldemedine studied for >12 weeks.
Summary of Literature Examining Long-Term Use of Novel Agents in OIC.
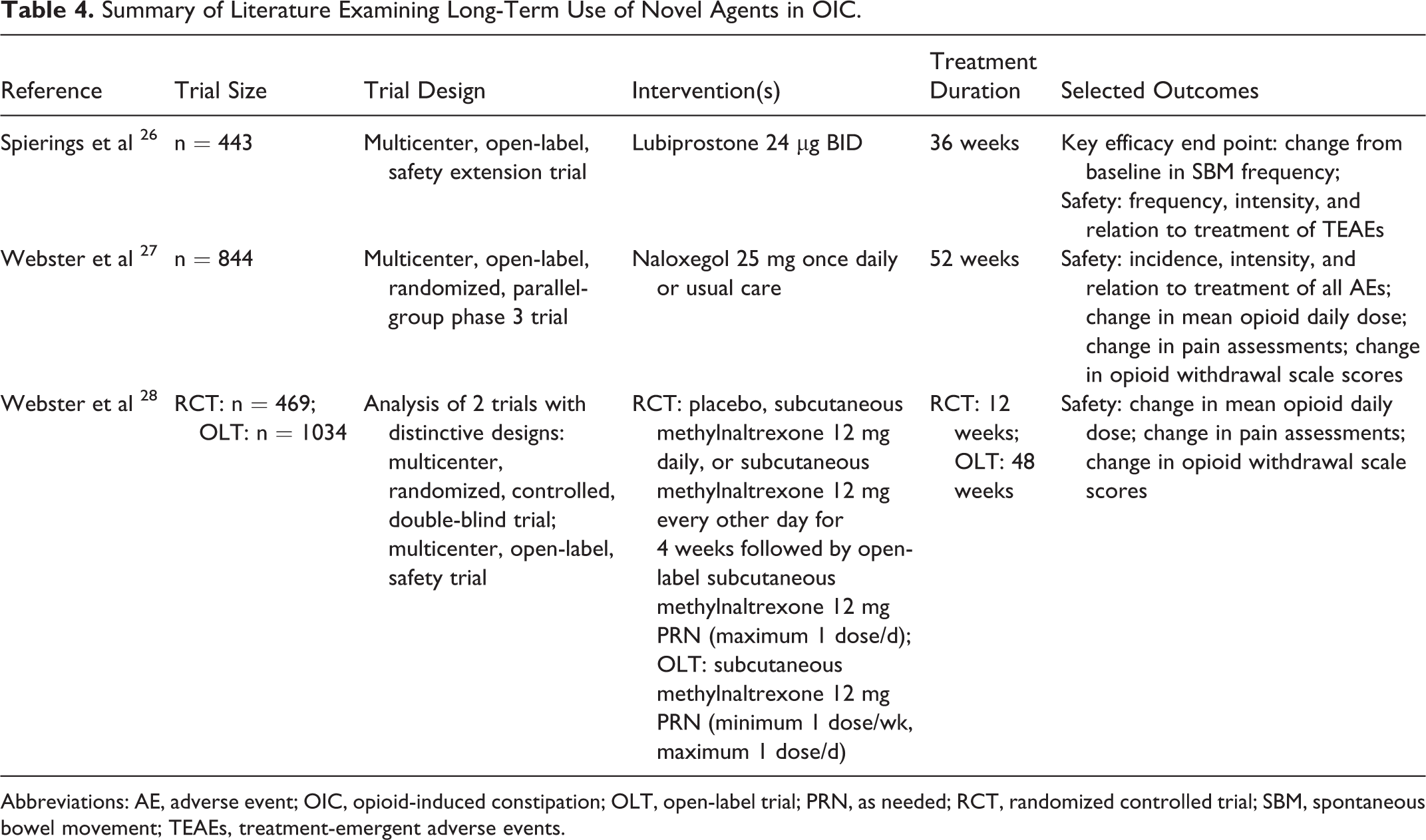
Abbreviations: AE, adverse event; OIC, opioid-induced constipation; OLT, open-label trial; PRN, as needed; RCT, randomized controlled trial; SBM, spontaneous bowel movement; TEAEs, treatment-emergent adverse events.
Lubiprostone
Spierings et al designed an open-label extension study to examine the long-term safety and efficacy of lubiprostone. 26 Patients were enrolled from previous 12-week phase 3 trials, and all patients received lubiprostone 24 μg twice daily without a comparator group. The rollover design introduces the potential for selection bias when analyzing safety outcomes, as patients who previously discontinued lubiprostone due to adverse effects would have been excluded from the long-term analysis. Rescue medication was available at the investigator’s discretion if there was no bowel movement for 3 days. Patients were prohibited from using any other laxative or stool softener during the trial other than rescue therapy. Patients were allowed to decrease therapy from the protocol-specified 2 capsules/d to 1 capsule/d with investigator approval.
A total of 443 patients were enrolled, with a baseline median morphine equivalent daily dose of 300 mg. The average lubiprostone daily dose was 1.4 capsules/d, reflecting that many patients did in fact decrease their dose as the protocol allowed. Additionally, missed doses were common, with 95% of patients missing at least 1 dose. These dose adjustments and missed doses reflect real-world patient circumstances and increase external validity in applying results to patient populations. Notably, a significant portion (20.3%) of the study population was treated with methadone, which has a known mechanistic interaction with lubiprostone that could potentially have skewed efficacy results. 17
The long-term efficacy data mirror that found in short-term lubiprostone trials in patients with noncancer pain. Spontaneous bowel movement frequency increased from 1.4/wk at baseline to 4.9 to 5.3 per week at the conclusion of the study, and this increase from baseline was significant (P < .001) at each monthly evaluation. Echoing this increase in spontaneous bowel movement frequency was a significant decrease in rescue medication use from baseline (59.9% vs 18.6% at month 9). Differences in other common patient-reported measures of constipation—straining, abdominal bloating, abdominal discomfort, stool consistency—were all significantly improved (P < .001) at each month as well.
Adverse events were common; almost 1 in 4 patients experienced at least 1 treatment-related adverse event that was generally mild or moderate. Most common adverse events were nausea (5.0%), diarrhea (4.6%), headache (1.6%), and vomiting (0.9%). Overall event rates were similar between patients previously exposed to lubiprostone or placebo. The observation that patients who were previously exposed to lubiprostone had a later onset (88 days vs 60 days) and shorter duration (7 days vs 38 days) of nausea than those previously exposed only to placebo raises the question of developing tolerance to GI adverse effects with prolonged exposure to lubiprostone. The same trends held true with diarrhea, a later onset (58 days vs 152 days) and duration (8 days vs 11 days) were observed in patients previously treated with lubiprostone over placebo. Although the authors point out that low event rates make it difficult to draw conclusions from these data, it would be an interesting consideration for future studies.
Without new safety concerns arising from long-term use, Spierings et al demonstrated continued benefit of lubiprostone in patients with chronic noncancer pain for up to 1 year. 26 Adverse effects remained consistent with short-term trials, and there may be a potential for these effects to be somewhat transient in patients treated for longer periods, although this requires further exploration. 16,18 Additionally, the long-term data allow for a dose reduction to accommodate patients who may experience these adverse effects without an apparent sacrifice in efficacy. Lubiprostone can be considered safe in patients with noncancer pain and OIC for up to 9 months to a year, and the efficacy data are reassuring despite the lack of a comparator group.
Naloxegol
Webster et al explored the safety and tolerability in adult patients with chronic noncancer pain and OIC compared to usual care in a 52-week open-label randomized controlled trial. 27 For this phase 3 trial, usual care was defined as any laxative regimen, excluding opioid-antagonist therapy, chosen by the investigator. Patients were randomized in a 2:1 fashion to receive naloxegol or usual care; those receiving naloxegol were prohibited from all other laxative use during the study with the exception of rescue medication use after 72 hours without a bowel movement. There was no defined rescue therapy for patients receiving usual care.
A total of 844 patients were enrolled, with 84 patients enrolled from previous naloxegol trials. At baseline, patients were prescribed a wide range of opioid medications with the most common being hydrocodone/acetaminophen (32.3%), morphine (27.9%), oxycodone as a single agent (25.0%), and in combination with acetaminophen (19%) and tramadol (14%). Baseline breakthrough opioid medication use was similar between the 2 groups, and the most commonly used breakthrough medications were hydrocodone/acetaminophen (9.8%), oxycodone (9.6%), and oxycodone/acetaminophen (8%). The mean morphine equivalent daily dose was 136.7 mg in the usual care group and 151.5 mg in the naloxegol treatment group. The use of partial opioid agonists was prohibited and use of methadone, buprenorphine, and pentazocine/naloxone were each reported in <1% of patients. About two-thirds of patients were taking a laxative in the 2 weeks before the screening period, with stimulants (54.4%), stool softeners (30.5%), and polyethylene glycol (14.7%) most commonly used. However, most patients (72.4%) were only taking a single laxative class.
The majority of patients randomized to receive usual care were taking laxatives at baseline with no change to their pretrial regimen (73%). Twenty-five patients were on no laxative at baseline and were not started on any medication for their OIC. The most common laxatives used by usual-care patients were bisacodyl (38%), polyethylene glycol (14.1%), and docusate sodium (10%).
Treatment-emergent adverse events were common in both groups (naloxegol 81.8%, usual care 72.2%). Abdominal pain (17.8% vs 3.3%), diarrhea (12.9% vs 5.9%), nausea (9.4% vs 4.1%), headache (9.0% vs 4.8%), flatulence (6.9% vs 1.1%), bronchitis (5.6% vs 4.4%), and upper abdominal pain (5.1% vs 1.1%) were all more common in the naloxegol group than in the usual care group. Of these, abdominal pain was the most common adverse effect with naloxegol, ranging in severity between mild (9.9%), moderate (5.6%), and severe (2.2%). Abdominal pain was also reported with usual care but was less prevalent (3.3%) and ranged between mild (0.7%), moderate (1.5%), and severe (1.1%). Interestingly, in patients experiencing abdominal pain on naloxegol, the majority reported an onset within the first week of therapy and a total duration of <2 weeks. No patients in the usual care group reported abdominal pain within the first week, and onset varied over the study period.
Discontinuation rates were higher with naloxegol (10.5%) than usual care (1.8%) and most commonly associated with diarrhea, abdominal pain, and vomiting. Importantly, only 2 deaths occurred throughout the trial, neither of which was attributed to study medications. Additionally, adverse events prespecified as being of special interest such as major cardiovascular events, heart failure, blood pressure changes, and opioid withdrawal were not more common in the naloxegol group. No bowel perforations were reported, and GI serious adverse events were not more common in the naloxegol group. Mean changes in pain scores were ≤0.4 and can be considered clinically insignificant. Also, mean opioid daily doses remained stable throughout the study with an overall minimal decrease in daily morphine equivalent requirements in both groups.
The long-term data published by Webster et al are reassuring and in alignment with short-term studies of naloxegol. 20,27 Unfortunately, because the study was focused primarily on safety, it is difficult to assess whether naloxegol provides ongoing benefit past the initial 12-week study period seen in phase 3 trials. However, the data allow for a conclusion that naloxegol is safe for use up to 52 weeks for patients with noncancer pain.
Methylnaltrexone Bromide
Webster et al described the effects of methylnaltrexone on pain management long-term by analysis of a phase 3 randomized placebo-controlled trial and a phase 3 open-label trial. 28 Patients in the randomized controlled trial received 4 weeks of blinded therapy with subcutaneous methylnaltrexone 12 mg daily, 12 mg every other day, or placebo. All patients were then eligible for inclusion in an 8-week open-label period during which they received subcutaneous methylnaltrexone 12 mg as needed (maximum 12 mg daily). In the separate, open-label trial, patients received subcutaneous methylnaltrexone 12 mg as needed (maximum 12 mg/d, minimum 12 mg/wk) for 48 weeks. There was no comparator group in either the open-label period of the randomized controlled trial or the phase 3 open-label trial.
A total of 469 patients were enrolled in the randomized controlled trial, with 364 moving on to the open-label period to receive methylnaltrexone as needed. In the open-label trial, 1034 patients were enrolled. Baseline median morphine equivalent daily doses varied between the 2 trials, with the randomized controlled trial having a median range of 154.8 to 163.4 mg across groups and phases, and the open-label trial having a median morphine equivalent daily dose of 120 mg. The most commonly prescribed opioids at baseline in the randomized controlled trial were oxycodone (20.2%), methadone (18.7%), and hydrocodone (14.3%). In the open-label trial, the most commonly prescribed opioids were morphine sulfate (22.4%), oxycodone (20.7%), and methadone (14.8%). The prevalence of methadone use in this trial without an underlying concern for mechanistic interactions, as with lubiprostone, can be considered an advantage when managing patients treated with methadone.
There was very little fluctuation in morphine equivalent dose requirements throughout the randomized controlled trial, with 1 exception. The methylnaltrexone 12 mg every other day group showed a significant decrease in the requirements for opioids when compared to placebo (P < .02). However, a decrease in opioid requirements would be unexpected and clinical significance can be questioned. Both open-label periods demonstrated little variation in opioid requirements (randomized control trial open-label period range 144-180 mg morphine equivalents/d, open-label trial 117.3-121.1 mg morphine equivalents/d).
Pain scores were assessed on an 11-point scale (0 = no pain, 10 = worst possible pain) and remained stable throughout all phases of both trials. Changes in pain scores from baseline in the randomized controlled trial ranged from −0.3 to 0.0 with consistently nonsignificant P values (P > .05 in all cases) when compared to baseline. The open-label trial revealed a mean change from baseline of −0.1 to 0.1; although there was no inferential statistical analysis performed on these data, these would not relate to clinically significant findings even if found to be statistically significant. Opioid withdrawal scores were also relatively stable throughout all phases of the trials, with small changes on the Objective Opioid Withdrawal Scale and the Subjective Opioid Withdrawal Scale that are not clinically different.
The long-term safety data with subcutaneous methylnaltrexone correlate well with short-term data. 22,28 Furthermore, the opportunity to use a medication only as needed, rather than committing a patient to the daily or twice daily oral OIC medications is appealing. Although there is no indication that the beneficial bowel effects would be expected to wane, without long-term efficacy data it is difficult to assess whether as-needed methylnaltrexone would continue to provide benefit past the initial short-term 12-week trial periods. The available long-term safety analyses focus on pain management and opiate withdrawal, and subcutaneous methylnaltrexone can be considered safe for up to 48 weeks from this vantage point. Additional data on other adverse effects of interest, including cardiovascular and GI safety, could provide further safety assurances for long-term use.
Emerging Therapy
Naldemedine
A 52-week study on the safety of naldemedine in which patients were randomized to receive naldemedine 0.2 mg daily or placebo ended in January 2016. The long-term data on naldemedine are not yet published and thus were not yielded in the results of the literature search previously described. However, preliminary results available from ClinicalTrials.gov indicate that in the 1240 enrolled patients, naldemedine had a significantly higher increase in the number of bowel movements per week (P < .0001 at weeks 12, 24, and 36; P = .0001 at week 52). 29 Correspondingly, naldemedine patients were less likely to require rescue laxatives regardless of frequency of laxative use prior to study entry. Preliminary results also indicate that naldemedine may improve constipation symptoms and quality of life. Patients in the naldemedine group were more likely to experience an adverse drug reaction (24.0% vs 19.5%), with abdominal pain, diarrhea, nausea, and vomiting being the most common. Although unpublished, it appears that naldemedine will have both safety and efficacy data in the long-term treatment of OIC, making it only the second agent that can provide this level of reassurance of ongoing benefit to health-care practitioners.
Discussion
This literature review reveals that long-term data are limited in the treatment of OIC and primarily focused on safety rather than efficacy. The inclusion of efficacy end points in long-term studies of lubiprostone and naldemedine lends weight to the choice of these agents, although naldemedine data are still unpublished and difficult to analyze within this review. Lubiprostone has the theoretical advantage of being unlikely to cause opioid withdrawal since it is not an opioid antagonist and was studied in patients taking median daily opioid doses almost twice that of patients in naloxegol and methylnaltrexone long-term studies. Although safety analyses of PAMORAs long-term have not raised concerns about changes in opioid requirements or opioid withdrawal, it may be prudent to consider lubiprostone for those patients that require higher morphine equivalent daily doses than those studied with either naloxegol or methylnaltrexone (120 - 160 mg morphine equivalents/d).
There are significant differences in formulation, drug interactions, and cost between the available OIC agents. Although patient-specific therapy should be the cornerstone of any therapy decision, the limited available data on long-term use of OIC agents reinforce the importance of incorporating these elements into shared decision-making with the patient. Methylnaltrexone was shown to be safe with as needed dosing, perhaps with as little as 1 dose/wk. However, the distinct disadvantage is the requirement for subcutaneous dosing. Although oral methylnaltrexone is now available, it does not have long-term evidence and there is relatively little experience with this dosage form. In contrast, naloxegol, lubiprostone, and naldemedine are all orally active but would require patient persistence to gain the benefits seen in long-term trials, which may be a treatment burden some patients are unwilling to accept.
Drug interactions, although relatively infrequent, must be considered with OIC agents. Naloxegol and naldemedine depend upon P-glycoprotein to aid in maintaining peripheral selectivity. Furthermore, naloxegol studies excluded patients who were using strong P-glycoprotein inhibitors. 27 Concomitant administration of naloxegol and naldemedine with P-glycoprotein inhibitors could result in higher levels of naloxegol and naldemedine, 21,24 potentially leading to increased opioid withdrawal symptoms. Methadone presents another interesting drug interaction challenge, as there is a known reduction in lubiprostone action on chloride channels in vitro that could translate to decreased clinical efficacy. Furthermore, naloxegol studies excluded patients with concomitant methadone use. 27 For these reasons, methylnaltrexone may be the best option for patients using methadone for chronic noncancer pain.
Conclusion
There are significant gaps in the long-term data available, most notably the lack of data on the use of novel therapies in combination with standard first-line therapy for OIC. It remains unclear if continuing nonprescription therapy when initiating a prescription OIC agent would provide additional benefit. Additionally, the new methylnaltrexone oral formulation may provide an attractive long-term treatment option, especially if studied with an as needed long-term dosing protocol. As long-term data and clinical experience accumulate with OIC agents, the treatment of OIC will continue to evolve. As it stands, treatment remains very patient-specific, with a stronger recommendation for lubiprostone, and tentatively naldemedine, without any other compelling patient factors such as drug interactions, route of administration, and cost to drive the decision due to proven efficacy past the 12-week study periods from short-term trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.