
Abstract
Background:
Currently, no consensus approach exists for optimal venous thromboembolism (VTE) prophylaxis in obese (BMI ≥30 kg/m2) patients. Time to development of in-hospital VTE is not well studied.
Objective:
This study evaluates time to in-hospital VTE in obese patients.
Methods:
A single-center, retrospective study evaluated obese patients that developed an in-hospital VTE. Patients were categorized into 3 BMI groups: 30 to 34.9 (group 1), 35 to 39.9 (group 2), and ≥40 (group 3) kg/m2. The primary end point compared time to VTE between the groups.
Results:
A total of 246 patients were included, and time to VTE was similar between the groups, 8 (group 1) versus 8 (group 2) versus 9 days (group 3); P = .38. Secondary outcomes showed time to VTE was shorter in acute care versus ICU patients (7.5 vs 10 days; P = .01), nonsurgical versus surgical patients (6 vs 9 days; P = .004), and no prophylaxis versus mechanical plus pharmacologic prophylaxis (4.5 vs 9 days; P < .001).
Conclusions:
BMI category did not significantly impact time to in-hospital VTE. This study provides insight into the timing of in-hospital VTE in obese patients. The differences in prophylactic strategies highlight the importance of optimized prophylaxis.
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a significant cause of morbidity and mortality in both medical and surgical patients. 1 –3 It has been estimated that approximately 900 000 patients develop a VTE in the United States each year, with half of these events being hospital acquired. 4,5 A number of risk factors for the development of VTE have been identified, including obesity. 6 Current data suggest that the incidence of VTE increases as body mass index (BMI) increases. 7 –10
In-hospital VTE is associated with health-care costs of US$10 billion or more per year in the United States. 4 Due to this significant cost burden on health care, these events are the focus of many patient safety quality and performance measures developed and promoted by agencies such as the Agency for Healthcare Research and Quality and Centers for Medicare and Medicaid. 11,12 The Centers for Disease Control and Prevention have also identified the need for strategies to address the use of VTE prophylaxis and improved tracking of these events. 12
Although appropriate prophylactic measures have been shown to prevent up to 70% of hospital-acquired events, fewer than half of hospitalized patients receive appropriate prophylaxis. 13,14 The American College of Chest Physicians (CHEST) provide recommendations for VTE prophylaxis in medical, orthopedic surgery, and nonorthopedic surgery patients with options including pharmacologic and mechanical methods. 15 –17 Unfortunately, there is no consensus recommendation or guidance for an optimal prophylactic strategy in obese patients. Given the lack of guided prophylaxis strategies in obese patients, a better understanding of the time which an in-hospital VTE occurs could lead to the development of more timely and aggressive preventative measures. As a result, complications resulting from in-hospital VTE could potentially be reduced (ie, length of stay [LOS] and hospital cost). The objective of this study is to determine the impact of BMI on time to in-hospital VTE in obese patients.
Methods
Study Design and Setting
A retrospective, observational, cohort study was performed for obese patients (BMI ≥ 30 kg/m2) aged 18 years or older admitted to Houston Methodist Hospital in Houston, Texas, from September 1, 2011, to June 30, 2015, who developed a VTE during their hospital admission. Patients were identified using the VizientTM database with diagnosis codes for upper extremity DVT, lower extremity DVT, and PE not present on admission. Patients were excluded if there were incomplete data points (ie, missing height or weight and no VTE documented). Patients were separated into 1 of 3 World Health Organization obese classes, class 1 (BMI 30-34.9 kg/m2), class 2 (BMI 35-39.9 kg/m2), or class 3 (BMI ≥ 40 kg/m2). This study was provided a letter of exemption from the Houston Methodist Research Institute Institutional Review Board after being deemed nonhuman subject research.
VTE events were defined as an acute DVT in the upper or lower extremities, diagnosed by venous doppler ultrasound, or an acute PE diagnosed by computed tomography or ventilation/perfusion (V/Q) scan. Tests were ordered by providers upon clinical suspicion of a possible VTE event. At our institution, a modified Caprini risk assessment tool is used to assess thrombotic risk in patients (Table A1). The assessment tool assigns various point values depending on the risk factor to provide a risk score. Patients were classified into 4 risk levels based on their total risk score: low (0-1), moderate (2), high (3-4), and highest (≥5).
Risk factors were retrospectively identified at the time of admission using provider-documented history and physical.
VTE preventative measures were collected for all patients. Mechanical prophylaxis was defined as orders placed for sequential compression devices (SCDs), compression stockings, or SCDs plus compression stockings prior to VTE event. Pharmacologic prophylaxis was defined as receiving anticoagulation or aspirin prior to VTE as recommended by the CHEST guidelines. 15 –17 Prophylaxis was ordered at the discretion of the physician’s leading variability in agent of choice, dose, and dosing interval. Prophylactic doses were defined as unfractionated heparin (UFH) 5000 or 7500 units subcutaneously every 8 to 12 hours, enoxaparin 30 mg (if creatinine clearance [CrCl] <30 mL/min] or 40 mg subcutaneously every 24 hours, fondaparinux 2.5 mg subcutaneously daily, and aspirin 161 mg orally daily. Alternative doses of enoxaparin were considered prophylactic if they did not exceed 1 mg/kg per day. All other dosing strategies used for these agents were considered treatment doses. Nonsurgical patients could have received prophylaxis with enoxaparin, UFH, or fondaparinux, while surgical patients (hip or knee replacement) could have received these agents or apixaban 2.5 mg orally twice daily, aspirin 161 mg orally daily, rivaroxaban 10 mg orally daily, or warfarin. 17 The use of warfarin, dabigatran, rivaroxaban, apixaban, or edoxaban in nonsurgical patients were considered treatment doses. Patients with contraindications to pharmacologic prophylaxis received only mechanical prophylaxis (Table A2). Patients in the low-risk group were eligible for early and aggressive mobilization or mechanical prophylaxis, the moderate- and high-risk groups were eligible for pharmacologic prophylaxis with or without mechanical prophylaxis, and the highest risk group were eligible for both pharmacological and mechanical prophylaxis.
End Point Measures
The primary end point of the study was time to in-hospital VTE based on BMI category. Secondary end points evaluated differences in time to VTE between acute care and intensive care unit (ICU) patients, nonsurgical and surgical patients, and differences in time to VTE between prophylactic strategies such as no prophylaxis, mechanical prophylaxis alone, pharmacologic prophylaxis alone, or pharmacologic plus mechanical prophylaxis. The determination of acute care or ICU was based on the initial admission location. The determination of surgical patient was based on the patient receiving a surgical procedure at any point during the hospitalization.
Statistical Analysis
The Ryan-Joiner normality test was used to determine normality. Baseline characteristics were summarized using descriptive statistics, including median and minimum–maximum for continuous variables and frequency and percentage for categorical variables. Kruskal-Wallis test was used to evaluate the primary end point. Mann-Whitney U test was used to evaluate acute care versus ICU and nonsurgical versus surgical patients, and Kruskal-Wallis test was used to evaluate the different prophylactic strategies. A post hoc analysis using Mann-Whitney U test was performed to determine true significant differences between the 4 different prophylactic strategies. To evaluate for differences between BMI categories, a post hoc analysis was performed for all secondary end points using Kruskal-Wallis test, and a further post hoc analysis using Mann-Whitney U test was performed to determine the significant difference between BMI categories. All primary and secondary end points were represented as median (min-max). A Kaplan-Meier product-limit method curve along with log-rank test was used to analyze time to VTE for primary and secondary end points. The relationship between end points (independent variable), covariates, and time to VTE was assessed using the Cox proportional hazard model. The following covariates used in our analysis were age, gender, race, hospital LOS, days receiving prophylaxis, heart failure exacerbation on admission, previous history of DVT/PE, and history of malignancy. An alpha value of less than .05 was considered statistically significant, and statistical tests were conducted using Minitab statistical software (v. 16; Minitab Inc, State College, Pennsylvania) and SAS Version 9.3 (SAS Institute, Inc, Cary, North Carolina).
Results
Overall, 246 patients met inclusion criteria during the study period, 146 in BMI class 1, 55 in BMI class 2, and 45 in BMI class 3. Patients were primarily white (66%), male (52%), and surgical patients (65%) with a median age of 63 years (Table 1). Median LOS in class 1 and class 2 were shorter than class 3 (20 vs 25 days), although this was not statistically significant. Upon admission, class 1 and class 3 had a higher median VTE risk score than class 2 (highest risk vs high risk). VTE events that occurred during hospitalization were lower DVT (64%), PE (15%), upper DVT (11%), and combined PE plus DVT (10%).
Baseline Demographics.
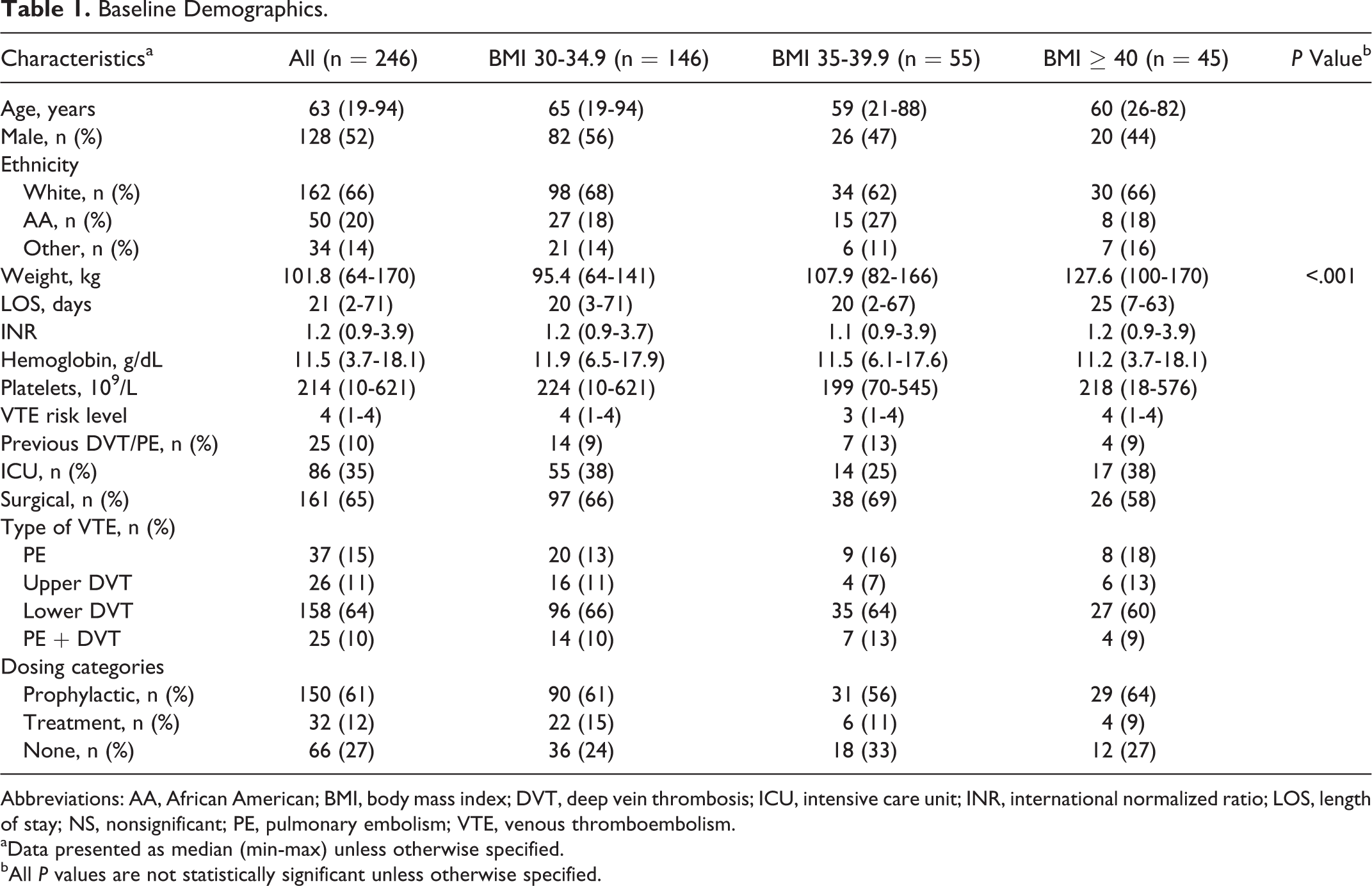
Abbreviations: AA, African American; BMI, body mass index; DVT, deep vein thrombosis; ICU, intensive care unit; INR, international normalized ratio; LOS, length of stay; NS, nonsignificant; PE, pulmonary embolism; VTE, venous thromboembolism.
aData presented as median (min-max) unless otherwise specified.
bAll P values are not statistically significant unless otherwise specified.
VTE prophylactic strategies utilized were mechanical prophylaxis alone (n = 48, 22%), pharmacologic prophylaxis alone (n = 45, 21%), pharmacologic plus mechanical prophylaxis (n = 105, 48%), and no prophylaxis (n = 19, 9%). Prophylactic pharmacologic agents used were enoxaparin (n = 117, 78%), UFH (n = 30, 20%), and aspirin (n = 3, 2%). The doses of prophylactic agents are listed in Table 2.
VTE Prophylactic Dosing.

Abbreviations: BMI, body mass index; q8h, every 8 hours; q12h, every 12 hours; q24h, every 24 hours; UFH, unfractionated heparin.
a5 in class 1, 5 in class 2, and 2 in class 3 were adjusted for a creatinine clearance <30 mL/min.
b1 received 300 mg rectally.
There was no difference in the primary outcome of median time to in-hospital VTE between the 3 groups (8 days in class 1, 8 days in class 2, and 9 days in class 3; P = .38). Kaplan-Meier curve of the culminated probabilities of VTE events by primary and secondary end points is displayed in Figure 1. At hospital day 20, approximately 80% of patients experienced VTE; however, after hospital day 20, patients in groups 1 and 2 had prolonged time to VTE (∼50 days) compared to the patients in group 3 (28 days). Patients who received no prophylaxis all experienced a VTE by day 15 (Figure 1C).
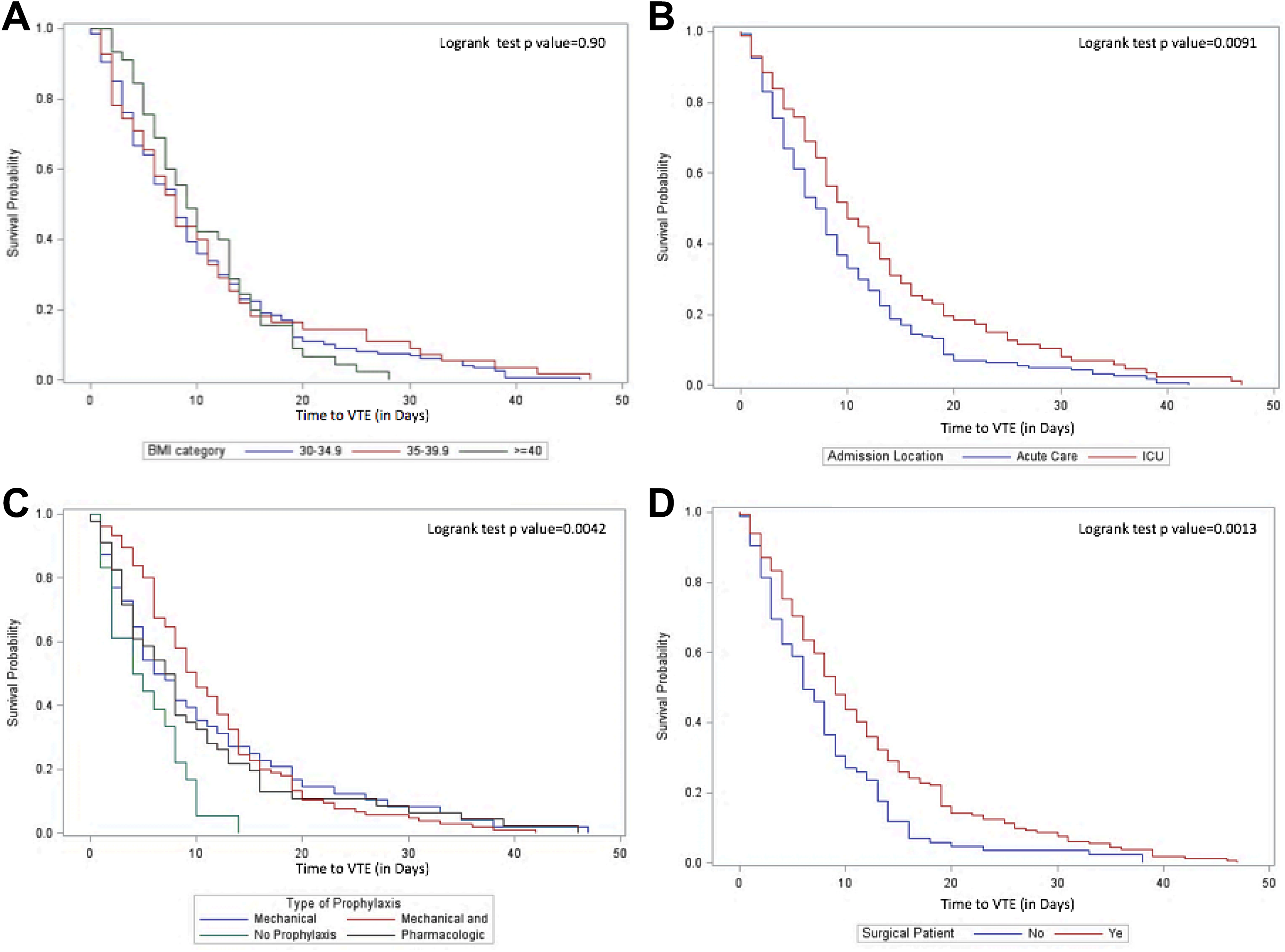
Kaplan-Meier curve of time to VTE: primary and secondary end points. The primary end point of time to VTE compared between BMI categories, 30 to 34.9, 35 to 39.9, and ≥40 kg/m2 (A). The secondary end points of time to VTE compared between admission location of ICU versus acute care (B), type of prophylaxis (C), and surgical versus nonsurgical patients (D). BMI indicates body mass index; ICU, intensive care unit; VTE, venous thromboembolism.
Patients in the acute care setting (n = 160) compared to ICU (n = 86) had a shorter median time to in-hospital VTE (7.5 days [0-42] vs 10 days [0-47]; P = .01), and nonsurgical patients (n = 85) compared to surgical patients (n = 161) had a shorter time to in-hospital VTE (6 days [0-38] vs 9 days [0-47]; P = .004). Also, as prophylactic strategies were escalated, time to VTE was subsequently prolonged (Figure 1C). Patients received pharmacologic prophylaxis a median of 5 days and mechanical prophylaxis a median of 8 days prior to the development of VTE. The time to VTE in patients receiving no prophylaxis was 4.5 (1-14) days, whereas patients receiving mechanical alone, pharmacologic alone, and pharmacologic plus mechanical were 6.5 (0-47), 7.5 (0-46), and 9.5 (1-42) days, respectively (P = .003). A post hoc analysis evaluating the true differences between prophylactic strategies only found that no prophylaxis compared to pharmacologic plus mechanical prophylaxis had a shorter time to VTE (4.5 vs 9.5; P < .001). A post hoc analysis exploring the differences between BMI and secondary outcomes is shown in Table 3. Acute care patients in class 1 had a shorter time to VTE compared to ICU patients in class 1 (7 vs 9 days; P = .04; Figure 1B), and nonsurgical patients in class 1 also had a shorter time to VTE compared to surgical patients in class 1 (5 vs 9 days; P = .003; Figure 1D).
BMI and Secondary End Points—Post Hoc Analysis.
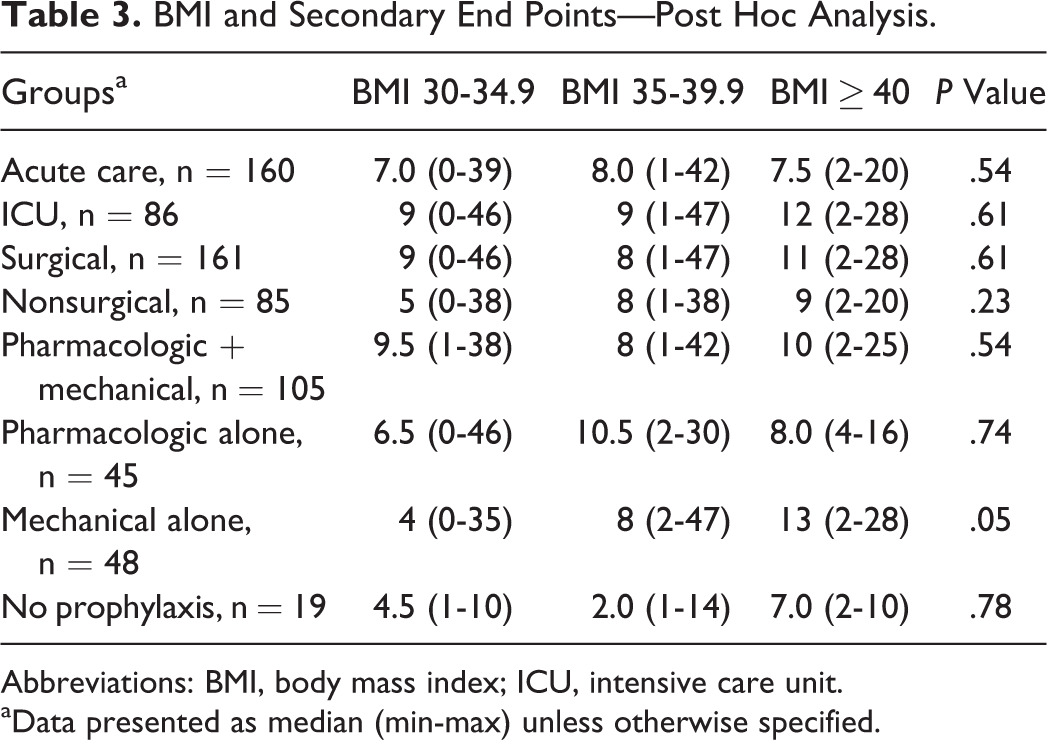
Abbreviations: BMI, body mass index; ICU, intensive care unit.
aData presented as median (min-max) unless otherwise specified.
Cox proportional hazard results evaluating primary and secondary end points adjusting for confounders are shown in Table 4. Consistent with the bivariate analysis, there was no difference in time to VTE between BMI categories. There were differences noted in the adjusted analysis when evaluating our secondary outcomes. There was no difference in time to VTE between acute care and ICU patients, but acute care patients with BMI class 3 had VTE prolonged by 73% compared to ICU patients (hazard ratio [HR] = 0.27, 95% confidence interval [CI]: 0.12-0.62). Mechanical prophylaxis statistically significantly prolonged the time to VTE by 46% compared to patients who did not receive prophylaxis (HR = 0.54, 95% CI 0.30-0.96). Unlike our bivariate analysis, there was no difference between surgical and nonsurgical patients in the cohort (HR: 1.14, 95% CI: 0.87-1.5). Confounders significantly associated with time to VTE included LOS, days received prophylaxis prior to VTE, and previous history of VTE (Table 4).
Cox Proportional Hazard Model Regression Coefficient Time to VTE.
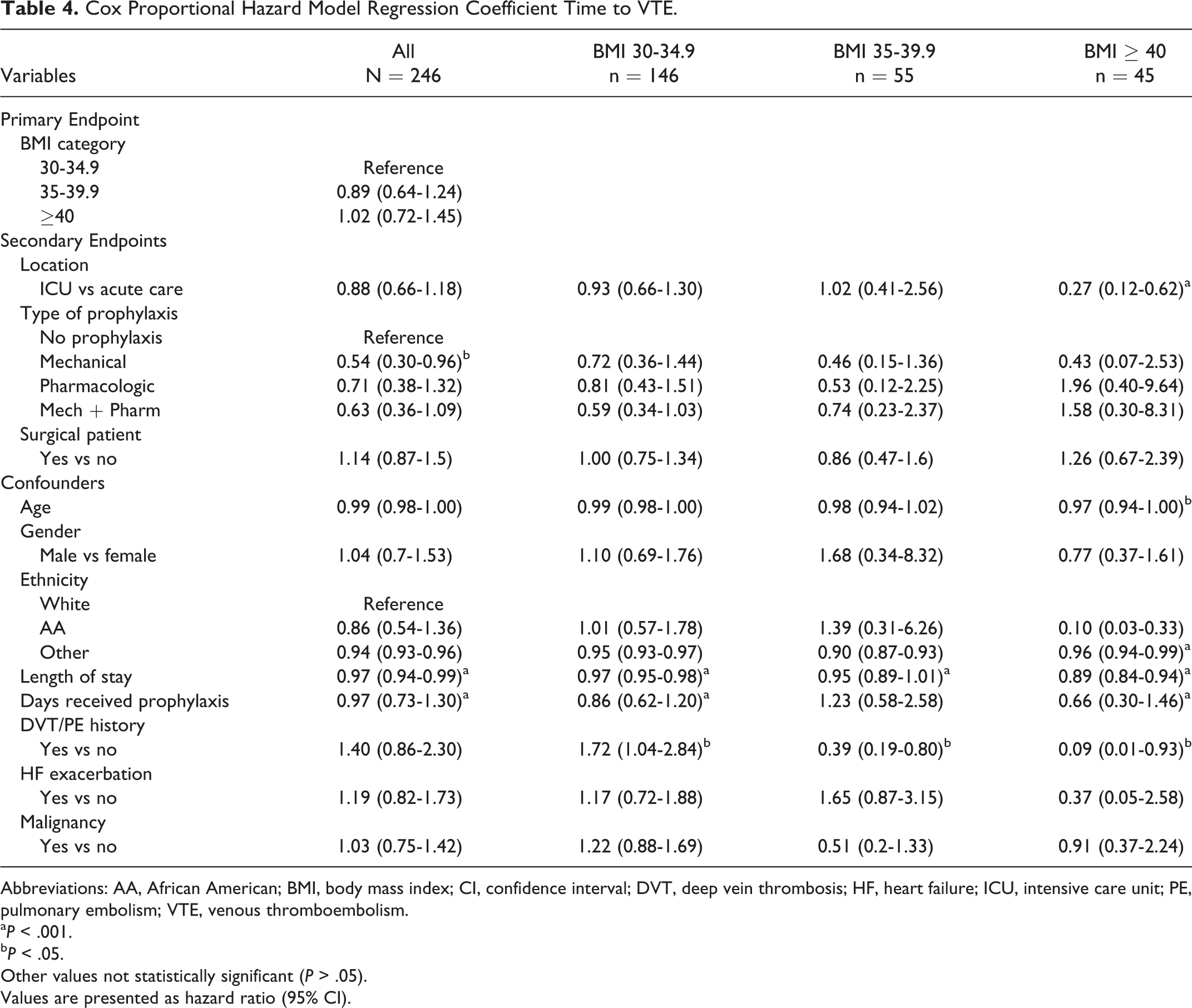
Abbreviations: AA, African American; BMI, body mass index; CI, confidence interval; DVT, deep vein thrombosis; HF, heart failure; ICU, intensive care unit; PE, pulmonary embolism; VTE, venous thromboembolism.
a P < .001.
b P < .05.
Other values not statistically significant (P > .05).
Values are presented as hazard ratio (95% CI).
Discussion
The prevention of hospital-acquired VTE is of increasing importance within health care. 18 Given the lack of optimal guidance for VTE prevention in obese patients, understanding the time to development of in-hospital VTE can provide valuable information on appropriate and timely prophylaxis. Our study showed that there was no difference in time to VTE based on different BMI categories. To our knowledge, only one study has been published evaluating time to in-hospital VTE, which exclusively evaluated spinal surgery patients. 19 The median time to VTE in this study was 9.5 days, while our study showed an overall median of 8 days. Only 7 spinal surgery patients were represented in our study population with a median time to VTE of 9 days, similar to what was reported by McClendon and colleagues. The use of VTE prophylaxis differed between the studies as well. McClendon et al initiated mechanical prophylaxis in all patients and pharmacologic prophylaxis was started a median of 6.5 days after surgery. In our study, the use of both mechanical and pharmacologic prophylaxis was under the discretion of the provider. Only 62% of patients in our study received mechanical prophylaxis, and 76% were started on pharmacologic prophylaxis with 48 hours of admission. Unfortunately, weight was not reported in the study by McClendon et al.
Extended length of hospitalization is a known risk factor for the development of in-hospital VTE. Our cohort had an overall median LOS of 21 days, and a Cox proportional hazard model found that 80% of our cohort developed a VTE by day 20 of hospitalization. The average hospital LOS in the United States in 2013 was approximately 5.4 days. 20 Because of the impact LOS has on the development of in-hospital VTE, it should be considered in VTE prevention strategies.
Although we did not find a difference in the primary end point, there were differences in our secondary end points. The location and patient type had a significant influence on time to VTE. Interestingly, acute care and nonsurgical patients experienced shorter times to VTE compared to ICU and surgical patients which was an unexpected finding in our study. Critically ill and surgical patients are at an increased risk of developing VTE mostly due to prolonged immobility, mechanical ventilation, vascular injury, and trauma. 21 Our findings could be explained by the heightened awareness of VTE in ICU and surgical patients, as these patients require higher care, although this is purely theoretical.
The type of prophylaxis patients received also had a significant impact on time to VTE. According to current CHEST guidelines, moderate- to high-risk patients should receive pharmacologic with or without mechanical prophylaxis. Although not specified in guidelines, obese patients are thought to have at least a moderate increased risk for VTE with other comorbidities factoring into this as well. Based on their risk, obese patients need pharmacologic prophylaxis with or without mechanical prophylaxis unless contraindications to one or both of these are present. 22 Of those receiving prophylaxis in our study, 70% were receiving a pharmacologic agent, and time to VTE was subsequently prolonged in these patients compared to those only receiving mechanical or no prophylaxis (Figure 2). Enoxaparin was the most commonly used agent (76%; Table 2). Of the 29 who received enoxaparin 30 mg every 24 hours, 13 were appropriately dosed reduced due to renal insufficiency (CrCl < 30 mL/min).
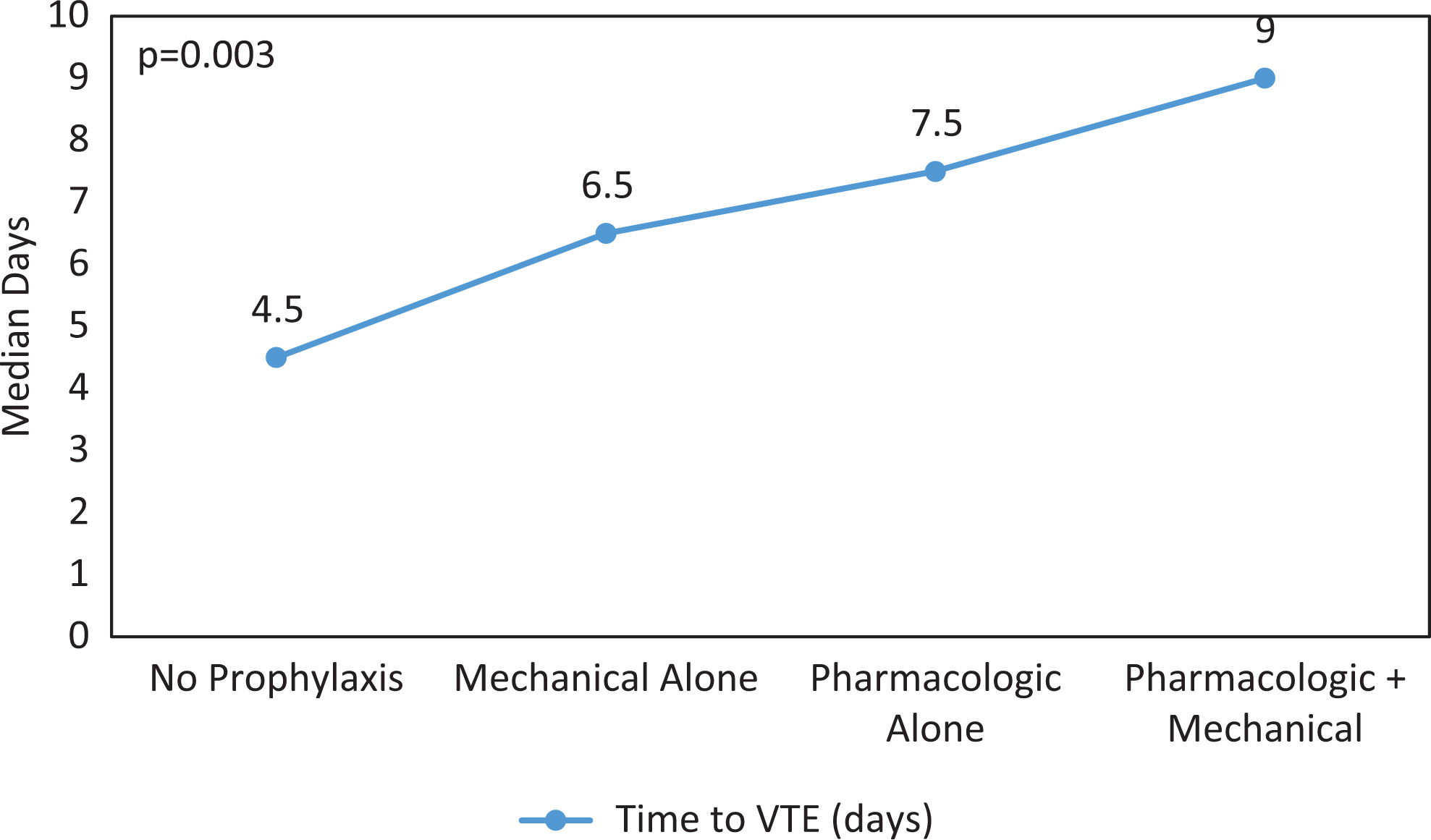
Prophylactic strategies and time to VTE. VTE indicates venous thromboembolism.
Despite the CHEST guideline recommendation that prophylaxis in obese patients should be weight based, limited data exist studying this approach. There have been some studies comparing standard to nonstandard doses in a broad, obese patient population. 23,24 One study evaluated the incidence of VTE in obese patients (>100 kg) using standard prophylactic dosing versus high-dose prophylactic dosing. 23 High dose was defined as UFH 7500 units every 8 hours and enoxaparin 40 mg twice daily. The study found no difference in the incidence of VTE between high-dose and standard-dose groups, 1.18% versus 1.52% (P = .22), respectively. However, patients with BMI ≥ 40 kg/m2 had a lower incidence of VTE if they received high-dose prophylaxis, 0.77% versus 1.48% (odds ratio: 0.52, 95% CI: 0.27-1.00; P = .05). Although this was not statistically significant, the authors concluded that there was a difference between the 2 groups as the logistic regression analysis showed the interaction between BMI and high-dose prophylaxis was significant (P = .047) after accounting for known VTE risk factors (ie, age, gender, cancer, and recent surgery) and since prior studies had shown benefit with high-dose prophylaxis in obese patients. The authors also commented that the utilization of high-dose prophylaxis was low compared to standard prophylaxis (1159 patients vs 2369 patients) due to physician’s prescribing patterns and could have impacted the power of the study. Notably, there was also no difference in bleeding between the 2 groups, 7.18% in the high-dose group versus 8.44% in the standard group (P = .15). Another study evaluated high-dose UFH to standard-dose UFH and showed no difference in incidence of VTE but more bleeding in the high-dose group. 24 In our study, there was minimal use of alternative prophylactic dosing.
Despite the limited benefit shown with alternative prophylactic dosing in a general, obese patient population, there has been benefit shown in bariatric surgical patients. A few studies have evaluated the incidence of VTE as the primary end point. 25,26 Scholten and colleagues compared enoxaparin 30 mg every 12 hours to enoxaparin 40 mg every 12 hours in bariatric surgery patients and found that incidence of VTE was higher in the 30 mg group compared to the 40 mg group (5.6% vs 0.6%; P < .01). 25 One major bleeding event occurred in both groups. The authors noted that the results could have been skewed due to patients in the enoxaparin 30 mg group having longer hospital stays (5.6 vs 3.8 days; P < .05) and procedure times (213 vs 175 minutes; P < .05). Another study evaluated the use of enoxaparin 40 mg every 12 hours after bariatric surgery in 451 patients. 26 Unfortunately, this study did not have a control group; however, there was only 1 VTE event and no major bleeding was noted. Although high-dose prophylaxis was not compared to standard doses in these studies, they do provide data that higher doses can be both effective and safe.
There were several limitations to our study. Although BMI class 1 included 146 patients, BMI class 2 and 3 included only 55 and 45 patients, respectively, which could have caused higher variability and potential sample bias possibly not allowing us to see a true difference between the groups. Our study was retrospective which could introduce a potential for recall bias. In addition, doses of prophylactic agents varied due to prescriber preference which could have had an impact on time to VTE. Also, patients were categorized into acute care or ICU groups on admission and did not account for changes in clinical status throughout hospital stay. Although acute care and nonsurgical patients experienced shorter times to VTE compared to ICU and surgical patients, we did not evaluate and compare prophylactic strategies between the groups. We did not assess and collect data on compliance of prescribed prophylaxis strategies which is an important factor to consider in patient developing in-hospital VTE. Our study contained a large portion of surgical patients; however, we did not stratify patients based on the complexity of the procedures. We also did not have a control group to compare our results to such as nonobese patients who developed an in-hospital VTE or obese patients who did not develop a VTE. Lastly, we were unable to assess patients receiving early ambulation in our study. Early ambulation is recommended in current CHEST guidelines for prevention of VTE, although this is not well defined. 15 –17 We initially evaluated physical therapy notes to assess ambulation in our patients, but documentation was erratic, poor, and was deemed unusable. Despite these limitations, our study provides valuable clinical information. Time to in-hospital VTE has not been well studied. Understanding this variable provides clinicians with information that could potentially lead to the initiation of institutional protocols for early and appropriate VTE prophylaxis in patients, especially high-risk patients (ie, obese). These protocols would be helpful in targeting high-risk patients who have not received appropriate prophylaxis after a period of days into hospitalization (ie, 48-72 hours).
Conclusion
Although in-hospital VTE is a preventable complication, these events can still occur despite best efforts to prevent them. Understanding the time to these events may provide clinicians better insight into the importance of timely and proper prophylaxis. Our study showed there was no difference in time to VTE based on BMI; however, patient location, patient type, and the prophylactic strategy used had significant impact on time to VTE. This study offers valuable insight into obese patients and highlights the need for more well-designed studies evaluating optimal VTE prevention strategies and patient type.
Footnotes
Appendix A
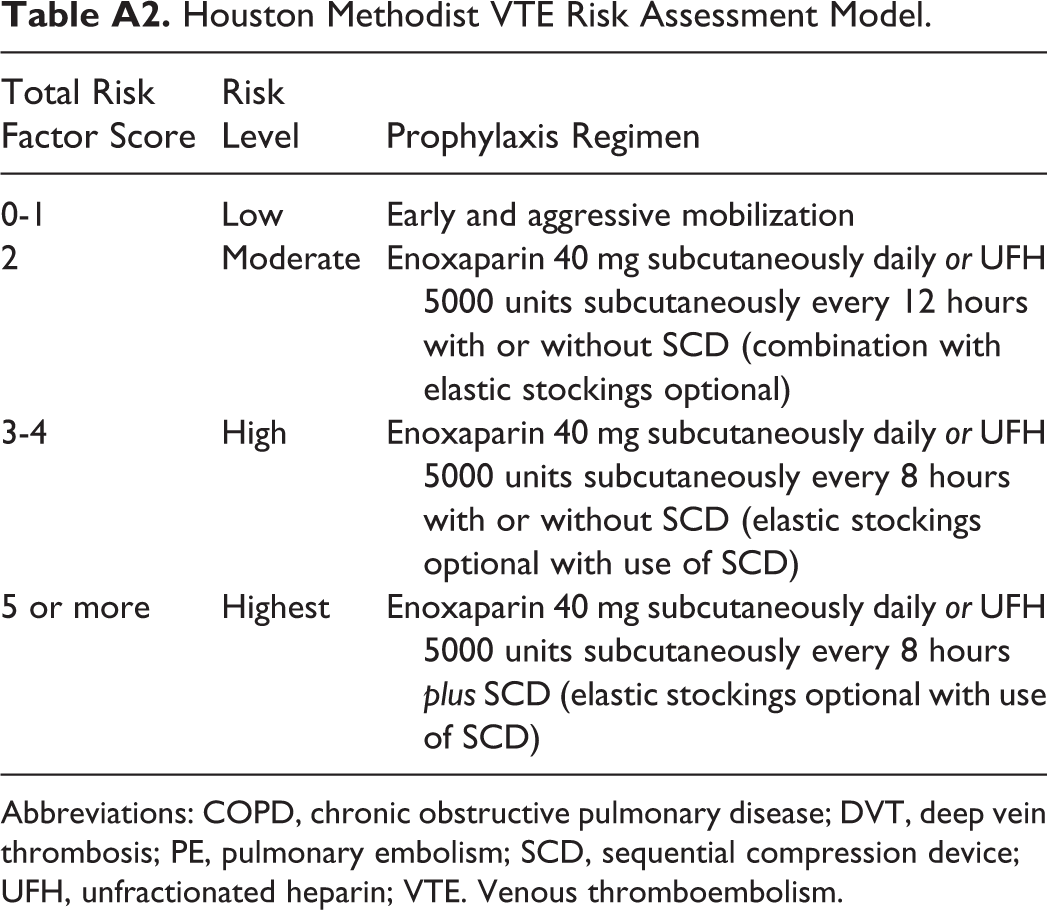
Houston Methodist VTE Risk Assessment Model.
| Total Risk Factor Score | Risk Level | Prophylaxis Regimen |
|---|---|---|
| 0-1 | Low | Early and aggressive mobilization |
| 2 | Moderate | Enoxaparin 40 mg subcutaneously daily or UFH 5000 units subcutaneously every 12 hours with or without SCD (combination with elastic stockings optional) |
| 3-4 | High | Enoxaparin 40 mg subcutaneously daily or UFH 5000 units subcutaneously every 8 hours with or without SCD (elastic stockings optional with use of SCD) |
| 5 or more | Highest | Enoxaparin 40 mg subcutaneously daily or UFH 5000 units subcutaneously every 8 hours plus SCD (elastic stockings optional with use of SCD) |
Abbreviations: COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; PE, pulmonary embolism; SCD, sequential compression device; UFH, unfractionated heparin; VTE. Venous thromboembolism.
Acknowledgments
The authors thank Dr Meena Mabbu for assistance with data collection for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.