
Abstract
Venous thromboembolism (VTE), including both pulmonary embolism (PE) and deep vein thrombosis (DVT), is the leading cause of maternal death in developed countries. Pregnancy is associated with an increased risk of VTE due to physiologic changes during the obstetric period that promote a hypercoagulable state. Appropriate use of prophylactic anticoagulants can decrease the event rate of thrombus formation in at-risk patients. In the United States, there is not a validated risk-assessment tool for VTE in obstetric patients or a clear consensus on initiation and optimal dosing strategy for the prophylactic use of anticoagulants. This article reviews the mechanism of coagulation disturbance that leads to an increased risk of VTE in obstetric patients, as well as the available literature surrounding pharmacologic prophylaxis.
Background
Venous thromboembolism (VTE) is five times more likely to occur in pregnant women compared to the nonpregnant population. 1 VTE accounts for approximately 10% of maternal deaths annually.1,2 While VTE is associated with significant maternal morbidity and mortality, the overall incidence is low, approximately 1-2 per 1000 pregnancies. 3 There are no validated VTE risk-assessment tools for the obstetric population in the U.S., and the available literature surrounding this topic is generally of low quality. Therefore, it is critical to stratify patients by risk early and to identify those who may benefit from VTE prophylaxis. Additionally, individual patient risk factors should undergo thoughtful consideration to weigh bleeding risk, cost, administration burden, and birth implications of anticoagulation in pregnancy. This aids in identification of those most likely to benefit from pharmacologic prophylaxis. This article reviews the hypercoagulable state induced by pregnancy, outlines modifiable and nonmodifiable risk factors for VTE, summarizes the available literature regarding agent selection, dosing, and monitoring, and compares published guideline recommendations from The American College of Obstetricians and Gynecologists (ACOG), The American College of Chest Physicians (ACCP), and the American Society of Hematology (ASH) for VTE prophylaxis in obstetric patients.
Pathophysiology
Hemorrhage can complicate 3%–5% of pregnancies with postpartum hemorrhage remaining a leading cause of maternal mortality, accounting for 11%–12% of maternal deaths in the United States.4-7 Due to the hemorrhage risk, there is an evolutionary benefit for the coagulation cascade to shift toward a hypercoagulable state during pregnancy. In addition to changes in the coagulation cascade, physiologic changes related to endothelial damage and venous stasis combined with patient-specific risk factors contribute to an increased risk of VTE during the obstetric period.
Hypercoagulability
Modifications in the concentration of coagulation factors that occur during pregnancy contribute to the increased risk of thrombus formation. Throughout the course of pregnancy, concentrations of the procoagulants fibrinogen, Von Willebrand factor (VWF), factor VII, factor VIII, and factor X increase. 8 The concentrations rise throughout pregnancy and return to normal range by eight weeks postpartum. 9 Additionally, the concentration of natural anticoagulants decreases during the obstetric period. Protein S levels decrease significantly while resistance to activated protein C increases. 9 The higher concentration of circulating coagulation factors, and reduction of endogenous anticoagulants, promotes clot formation and activation of the coagulation cascade.
A reduction in fibrinolysis also occurs due to a decrease in tissue plasminogen activator (tPA). 9 This decrease in tPA is caused by increased plasminogen activator inhibitors 1 and 2 (PAI-1 and PAI-2). Levels of PAI-1 are threefold higher compared to nonpregnant levels. 10 PAI-2 comes from villous cells of the placenta; therefore, concentrations are dependent on placental size. 11
These changes shift the balance in the coagulation cascade toward clotting to protect women from hemorrhage during miscarriage and birth. The average volume of blood loss is less than 500 mL for vaginal births and less than 1000 mL for cesarean deliveries. 4 Blood volume loss could be commonly higher in the event of complications, such as postpartum hemorrhage or placental abruption, if these coagulation changes did not occur.
Endothelial Injury and Dysfunction
Endothelial dysfunction and injury contribute to the risk of thrombosis during pregnancy and the postpartum period. Tissue damage during both vaginal and cesarean delivery triggers the extrinsic coagulation cascade. 12 Besides the inherent tissue damage associated with labor and delivery, increases in the incidence of obesity, sedentary lifestyles, and rising maternal age has contributed to an increase in the rate of hypertension.8,9 Hypertension causes thickening of the arterial wall leading to endothelial dysfunction. It can also initiate the production of reactive oxygen species and a subsequent decrease in nitric oxide, a vasodilator produced by the endothelium. 13
Venous Stasis
Pregnancy is associated with both venous distension and insufficiency. 14 There is a complex interplay between hormonal changes, increased plasma blood volume, obstruction from the expanding uterus, and decreased mobility that promotes blood stasis. 14 The expanding uterus causes a 50% reduction in venous flow in the deep leg veins by 25-29 weeks of gestation which lasts until six weeks postpartum. 15 In addition, the left lower extremity is the site of 82% of DVTs in pregnant and postpartum women due to uterine compression of the left common iliac vein by the right common iliac artery. 16
Risk-Assessment
The risk of VTE exists throughout each trimester and is highest in the first six weeks postpartum. 17 One meta-analysis compared the event rate of VTE throughout each trimester and the postpartum period. This review pooled data from 14 studies between 1966-1998. The trimester in which a VTE event occurred was reported in 12 of the 14 studies. The event rate across these studies was 21.9% (95% CI 17.4-27.3) during the first trimester, 33.7% (95% CI 28.1-39.8) during the second trimester, and 47.6% (95% CI 39.2-56.2) during the third trimester. Heterogeneity testing was not significant. An event rate during the antepartum and postpartum period was reported in 9 of the 14 studies. Of these events, 65.5% (95% CI 58.1-72.1) occurred during pregnancy and 34.5% (95% CI 27.9-41.9) occurred during the postpartum period (P = 0.08). This result was also not heterogeneous. There was no significant difference in event rates across these periods, but the length of the antepartum period (280 days) is much longer than the postpartum period (42 days). The estimated distribution of 100 VTE events during the antepartum period is 0.23 per day compared to 0.82 per day in the postpartum period.
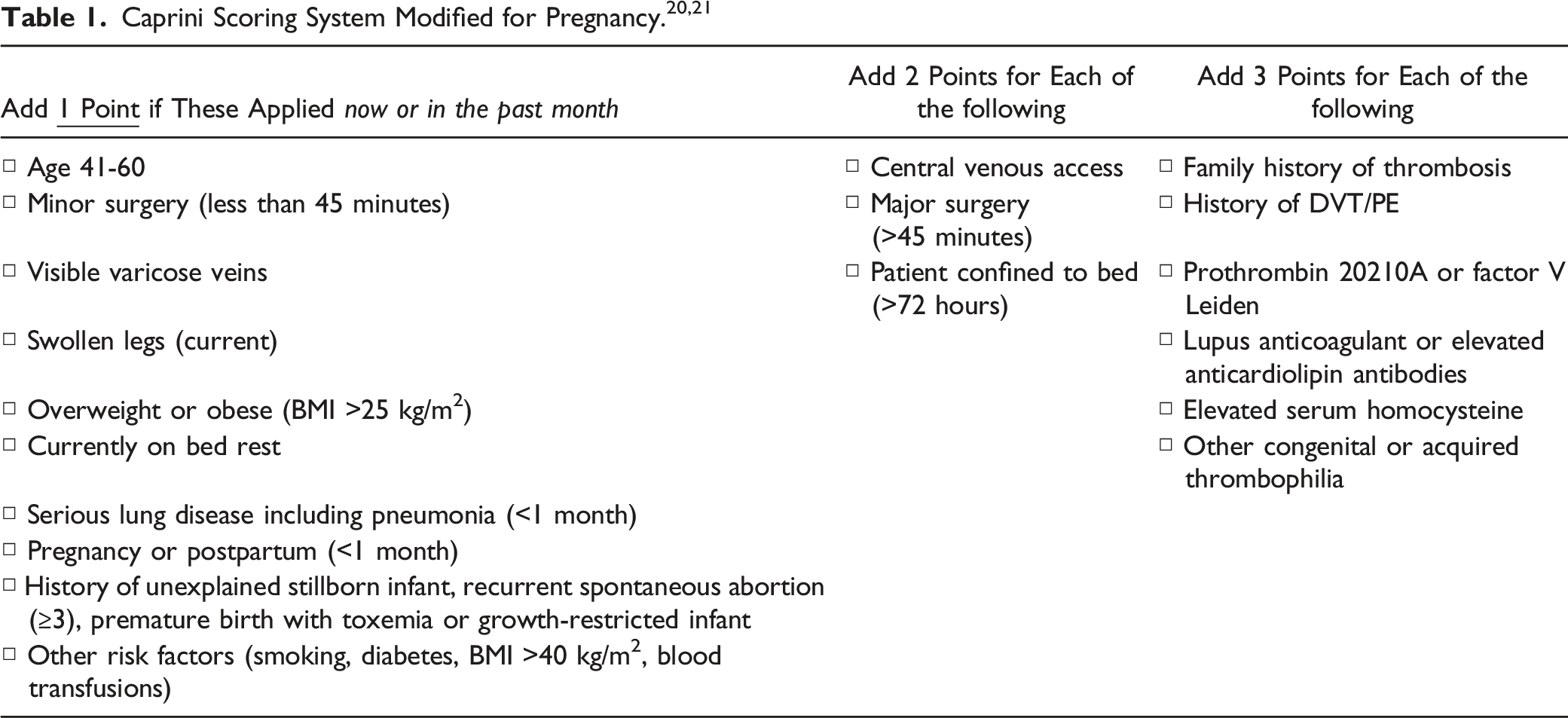
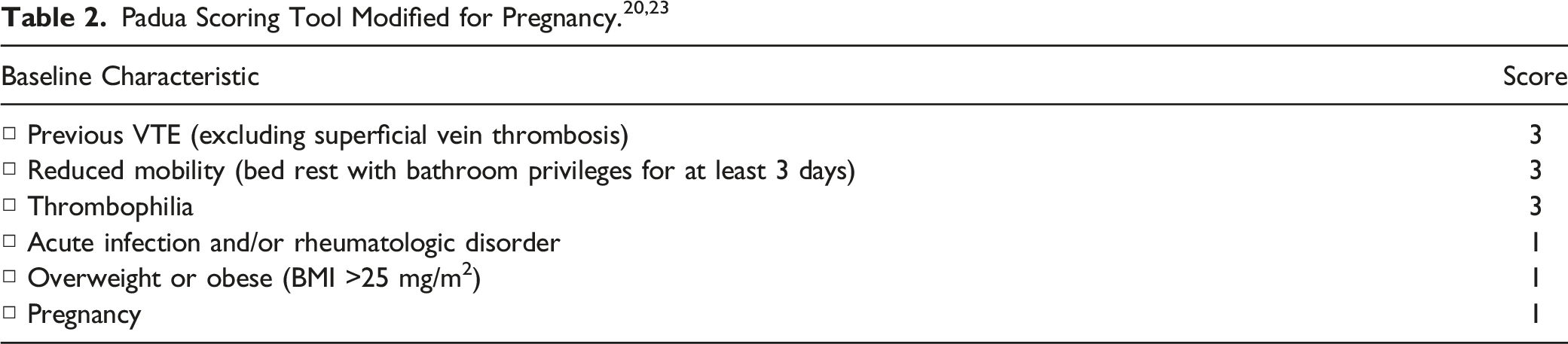
Despite the increased risk of VTE in pregnancy, most patients do not require pharmacological prophylaxis due to a low overall incidence of VTE and uncertainty in data about the benefits of chemoprophylaxis in women without additional risk factors. 18 A thorough review of individual risk factors should be conducted to weigh the benefits of VTE prophylaxis against the financial cost, administration burden, and bleed risk. The National Partnership for Maternal Safety (NPMS) was formed in recognition of the need to decrease maternal morbidity and mortality in the U.S. 19 They created three consensus bundles for preventable causes of maternal mortality: hemorrhage, hypertension, and VTE. In the consensus bundle for VTE, completion of a VTE risk-assessment is recommended for all obstetric patients during their first prenatal visit, during all antepartum admissions, immediately postpartum, and upon discharge after delivery. 20
Risk Factors
Given the overall low incidence but high morbidity and mortality, individual patient risk factors should be carefully considered to identify those most likely to benefit from pharmacological prophylaxis. 3 Potential indications for pharmacological prophylaxis include personal history of VTE, inherited or acquired thrombophilias, cesarean section delivery, and use of assisted reproductive technology.
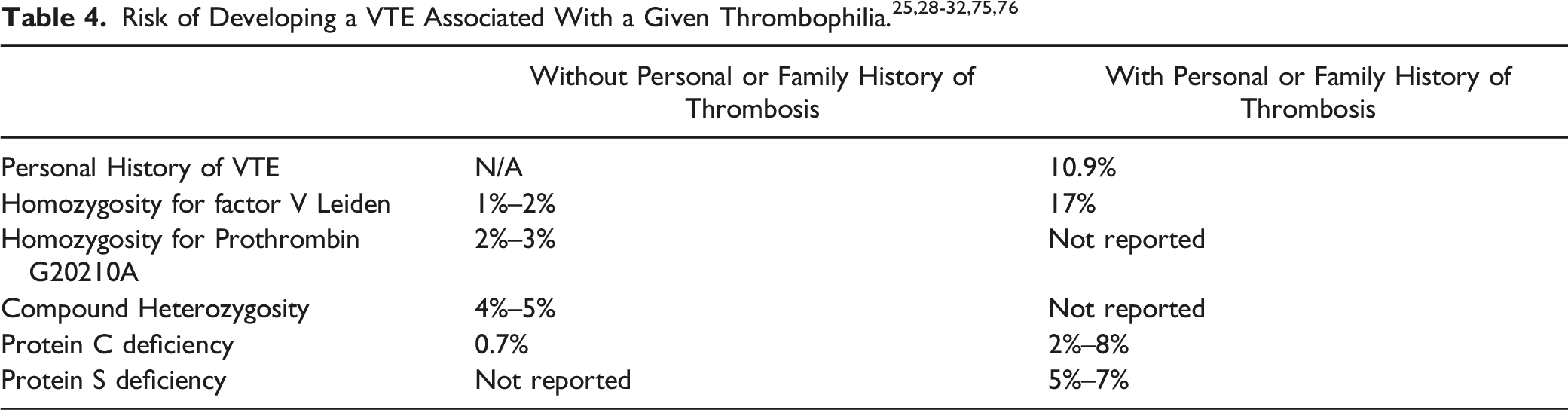
Prothrombin G20210A is present in 17% of women who develop VTE during pregnancy. 30 Women who are homozygous for prothrombin gene mutation without a personal or family history of VTE have a 2%-3% risk for VTE. Women can also be heterozygous for both factor V Leiden and prothrombin gene mutation. This compound heterozygosity has a synergistic effect leading to a 4%–5% risk of VTE in the absence of personal or family history of VTE (Table 4).
Two other types of thrombophilias include protein C deficiency and protein S deficiency. Women without a personal or family history of VTE in the setting of protein C deficiency have a risk of ∼0.7% of developing a VTE during pregnancy. 26 Women with a positive personal or family history have an estimated risk of 2%-8%. 31 Women with a positive personal or family history of VTE in the setting of protein S deficiency have a risk of 5%-7% for developing VTE during pregnancy (Table 4). 32
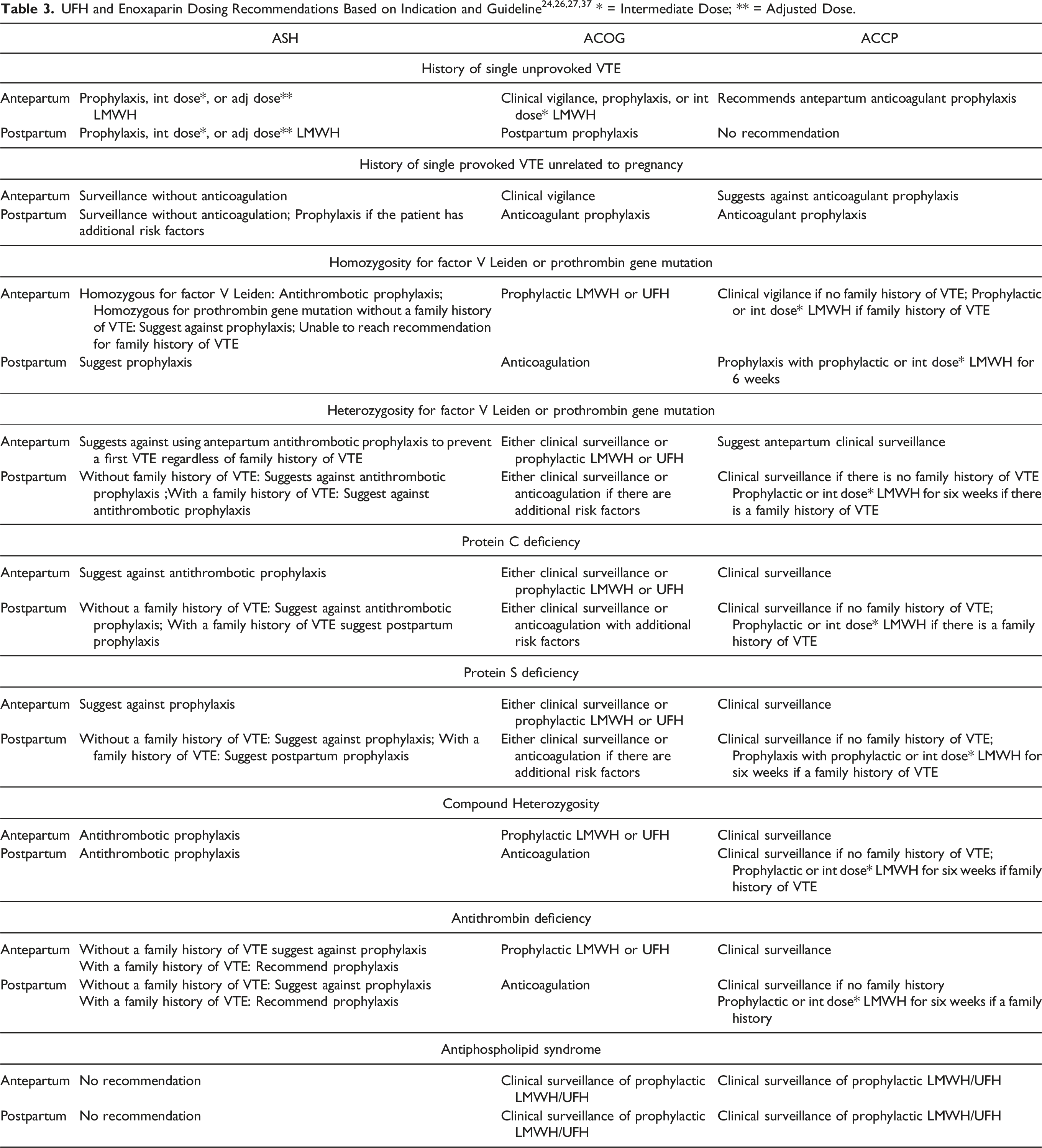
Examples of acquired thrombophilias include antiphospholipid syndrome (APS) and human immunodeficiency virus (HIV). 33 The most common acquired thrombophilia in pregnancy is APS which is characterized by circulating antibodies such as anticardiolipin antibodies (aCL) or lupus anticoagulant (LA). 34 Women with APS have a 5%-12% risk of VTE during pregnancy.35,36 Due to an overall lack of data, ACOG and ACCP state that clinical surveillance, prophylactic unfractionated heparin (UFH), or prophylactic low-molecular-weight heparin (LMWH) may be warranted both antepartum and postpartum (Table 3).26,37
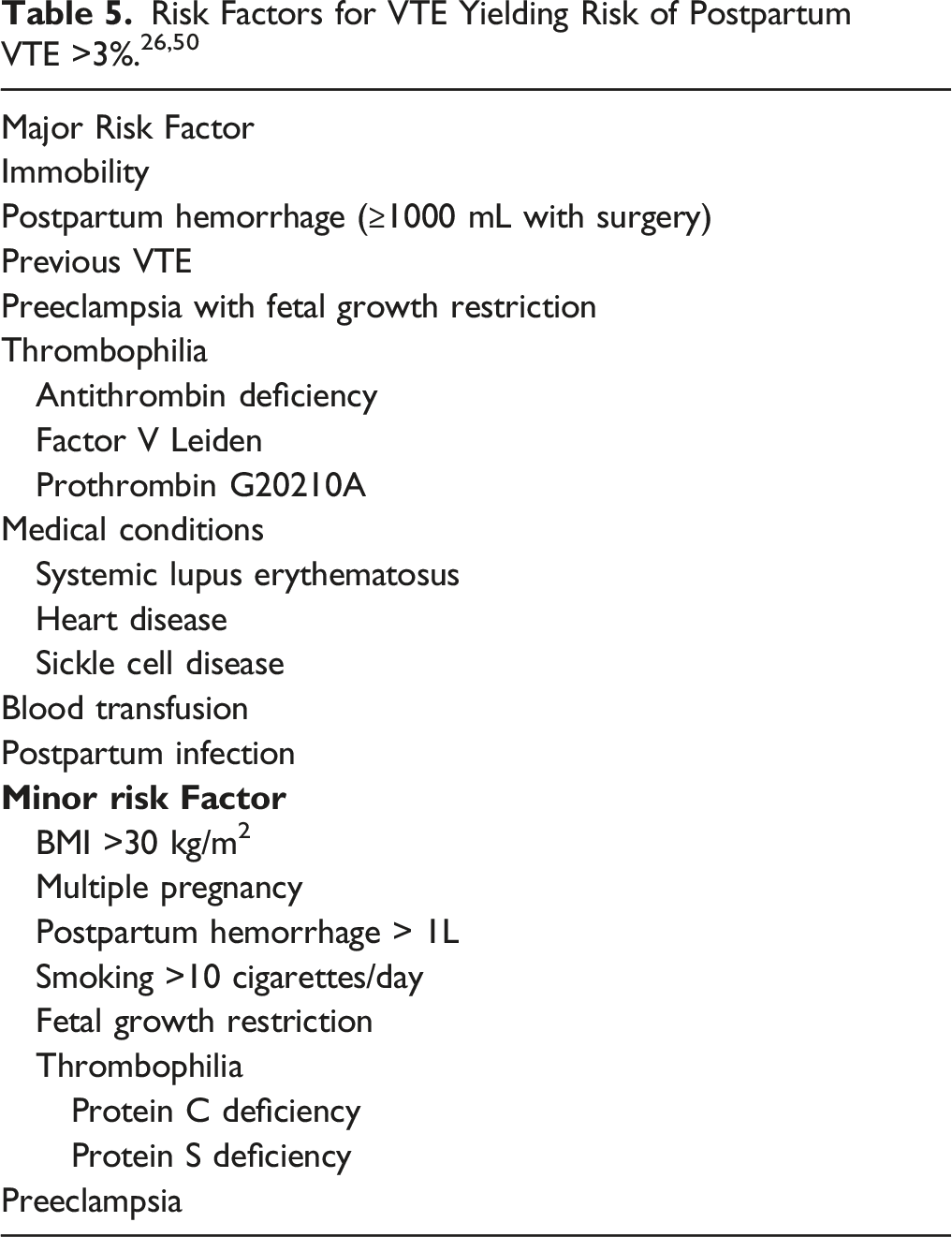
ACCP also recommends the use of mechanical prophylaxis in place of, or in addition to, pharmacologic prophylaxis. 26 When used in place of pharmacologic prophylaxis, mechanical prophylaxis had less major bleeding (RR, 0.51; 95% CI, 0.40-0.64) but a higher risk of VTE (RR, 1.8; 95% CI, 1.2-2.8). 50
Assisted reproductive technology (ART) includes treatment and procedures where oocytes or embryos are handled (i.e., in vitro fertilization-embryo transfer, gamete intrafallopian transfer, zygote intrafallopian transfer, and frozen embryo transfer). 55 ART has been associated with a low increased risk of VTE (0.1%). 56 A higher incidence of VTE has been observed in patients who experience ovarian hyperstimulation syndrome (OHSS), a complication of ART therapy. OHSS is characterized by third space fluid accumulation, respiratory dysfunction, and renal impairment often requiring intensive care hospitalization. 57 When OHSS develops, the absolute risk of VTE increases to 4%. 56 There is limited data regarding the use of VTE prophylaxis in both the ART and OHSS populations. ACCP estimated the effect of LMWH prophylaxis in women undergoing ART by extrapolating data from patients who underwent hip arthroplasty.26,58 In the presence of severe OHSS, prophylaxis with enoxaparin may result in a reduction of 26 VTEs per 1000 women treated (NNT is 39), without increased risk of significant bleeding. In the absence of OHSS, the NNT is 781. For women undergoing assisted reproduction who develop severe OHSS, ACCP recommends VTE prophylaxis for 3 months following resolution of OHSS. 26
VTE Prevention With Medication
Agents used in the general adult population for VTE prophylaxis include UFH, LMWH, direct thrombin inhibitors (DTI), factor Xa inhibitors, and vitamin K antagonists (VKA). Of these agents, DTIs and factor Xa inhibitors, such as dabigatran, apixaban, and rivaroxaban, should not be used antepartum due to their potential ability to cross the placenta and their unknown impact on reproduction. 27 VKAs, such as warfarin, are also generally not recommended in pregnancy because they cross the placenta and can lead to warfarin embryopathy. 26 An exception is use of a VKA in a pregnant patient with a mechanical mitral valve. A systematic review found that the risk of thromboembolic complications was highest when UFH was used throughout pregnancy in women with a mechanical mitral valve. 59 In order to balance the risk of congenital anomalies and risk of VTE, UFH or LMWH is recommended in the first trimester followed by warfarin therapy in the second and third trimester for this indication. Overall, national guidelines recommend use of UFH or LMWH as preferred anticoagulants during the obstetric period.24,26,27
The benefits of UFH during pregnancy include its inability to cross the placenta, safety in renal failure, measurable effect with activated partial thromboplastin time (aPTT) and anti-factor Xa (anti-Xa), and availability of a reversal agent. 60 Disadvantages of UFH include its unpredictable pharmacokinetic profile, bruising at the injection site, frequency of injection, risk of heparin-induced thrombocytopenia (HIT), and the risk of major bleeding.
Compared to UFH, the benefits of LMWH include the inability to cross the placenta, dosing frequency, predictability of effect, lower incidence of HIT, and bleeding risk relative to UFH. 61 Disadvantages of LMWH include renal dose adjustment when creatinine clearance falls below 30 mL/min, injection site pain, cost, and longer half-life where consideration must be given to patients who receive neuraxial analgesia during labor.
A study by Casele et al. was performed that compared the incidence of VTE events with UFH and LMWH. 62 This study observed two VTEs in patients on LMWH (3%, n = 60) and four VTEs in patients on UFH (7%, n = 57). This corresponded to a risk ratio of 0.47 (95% CI 0.09-2.49) demonstrating noninferiority between the two agents further solidifying practitioners’ preference for LMWHs during pregnancy and postpartum. By consensus, LMWH is the preferred agent for VTE prophylaxis in obstetric patients.24,26,27
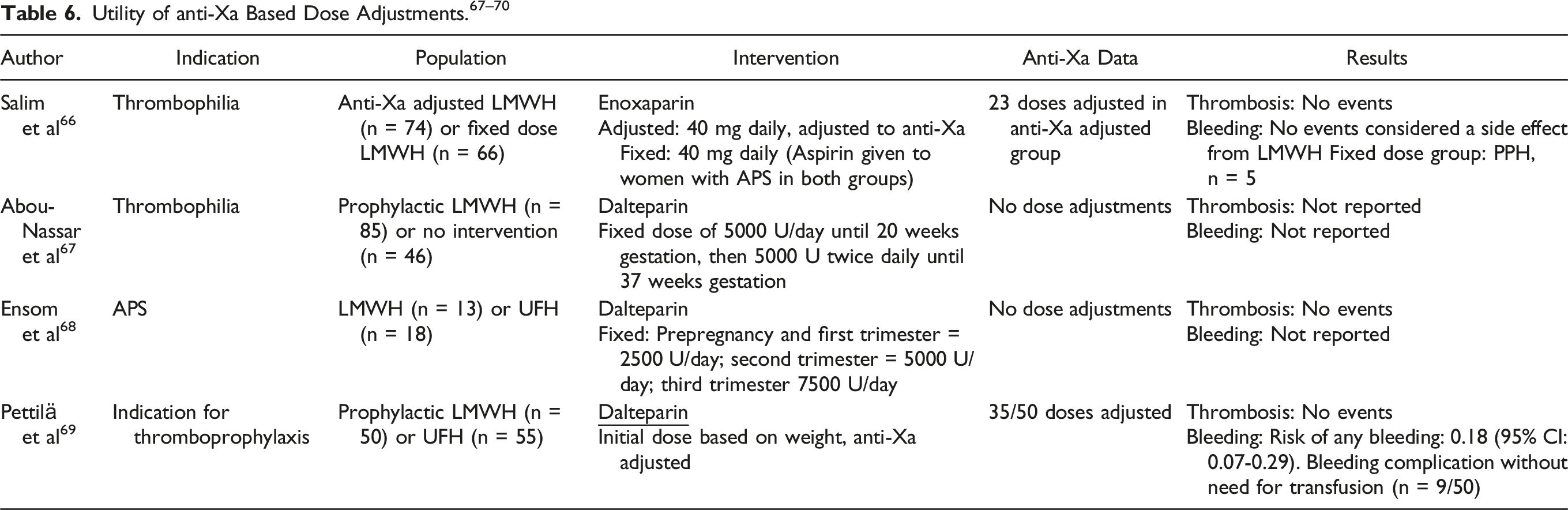
The physiologic changes associated with pregnancy have led to questions regarding optimal LMWH dosing. Beginning at 6-8 weeks of gestation, maternal blood volume begins to increase, and by 32 weeks of gestation, maternal blood volume will increase by 40%-50%. 63 Renal plasma flow also increases by 40%-65%, and glomerular filtration rate increases by 50%-85% compared to non-pregnant women due to renal vasodilation during pregnancy. Since a direct measure of LMWH levels does not exist, anti-Xa levels are measured as a surrogate marker of drug concentration. Anti-Xa level monitoring is not recommended in the general population given the predictable pharmacokinetic profile of LMWH. However, there may be utility in monitoring anti-Xa levels in certain populations such as patients with renal insufficiency or at the extremes of body weight. A study conducted by Lebaudy et al. evaluated the potential impact of the obstetric physiologic changes on the pharmacokinetics of enoxaparin. 64 They found that drug clearance increased throughout the initial trimesters of pregnancy and then stabilized around 20 weeks of gestation. In addition, the volume of distribution increased slowly throughout the first and second trimesters and then increased rapidly after 30 weeks of gestation. Based on a computed pharmacokinetics model, they found that with a prophylactic regimen of enoxaparin 40 mg subcutaneously once daily, the peak anti-Xa level decreased with pregnancy progression. In the first trimester, the mean anti-Xa level was 0.47 IU/ml compared to 0.32 IU/mL in the third trimester (P = 0.002). The goal peak enoxaparin anti-Xa level for VTE prophylaxis in pregnancy has not been determined; however, studies evaluating enoxaparin use in trauma or obese patients for VTE prophylaxis suggest a goal peak anti-Xa level of 0.2-0.4 IU/mL.65,66
The California Quality Improvement Toolkit Provides Dosing Recommendations Based on Available Data. 71
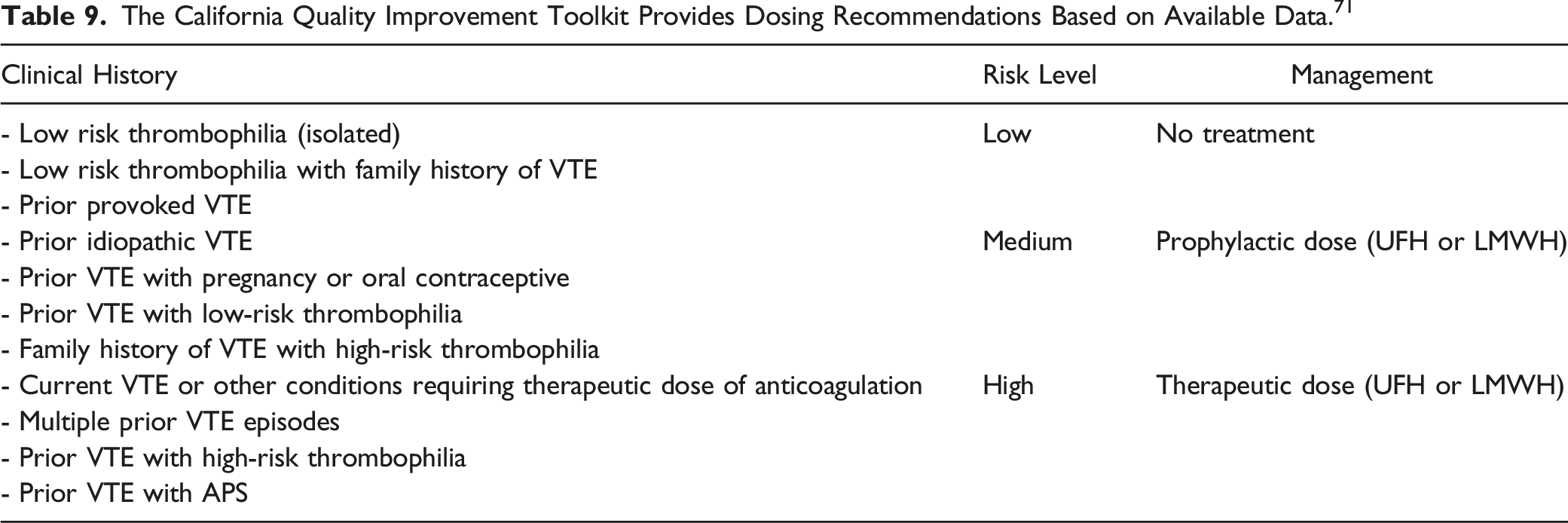
A retrospective cohort study completed in the Netherlands by Roeters van Lennep et al. evaluated LMWH dosing based on risk stratification. 72 The study extrapolated women into either intermediate-risk or high-risk groups. Women were stratified into the intermediate-dose group (n = 34) if they had a single episode of provoked VTE, low-risk thrombophilia and a first-degree family history of VTE, or VTE in first-degree family member without a thrombophilia. Women were stratified into the high-risk group (n = 57) if they had a high-risk thrombophilia, single episode of unprovoked VTE, single episode of VTE and thrombophilia, or greater than or equal to two episodes of VTE not on long-term anticoagulation. The intermediate-risk group received nadroparin 2850 IU subcutaneously once daily for 6 weeks postpartum. The high-risk group received nadroparin 2850 IU subcutaneously once daily during pregnancy and for 6 weeks postpartum. The primary outcome was pregnancy related symptomatic VTE, and the secondary outcome was postpartum hemorrhage defined as greater than 500 mL of blood loss. There was a total of seven VTEs in 126 pregnancies (5.6%, 95% CI [4.3-16.6]), all of which occurred in the high-risk group. Two of the seven VTE events occurred during the antepartum period, and five of the seven VTE events occurred during the postpartum period. 72 Postpartum hemorrhage occurred in 30.3% of patients in the intermediate-risk group and 16.4% of patients in the high-risk group (P = 0.12) demonstrating no statistically significant difference. Based on these results, researchers concluded that higher doses of LMWH may be needed in women at high-risk of VTE. However, two of the five VTEs that occurred in the postpartum period were after the 6-week postpartum study period and should not have been included in the analysis. The recommendation to increase the enoxaparin dose would increase the risk of hemorrhage. Additionally, providers would need to recognize the patient is receiving enoxaparin and hold the medication 12-24 hours prior to delivery for women who desire neuraxial analgesia.
The results of the Roeters van Lennep et al. study prompted a similar investigation to be conducted in New Zealand by Cox et al. 73 This retrospective cohort study analyzed patients from 1999-2014 who were at risk of pregnancy associated VTE. Patients were stratified based on the origin of their clot history. Women with a history of provoked VTE (n = 49) received enoxaparin 40 mg subcutaneously once daily for 6 weeks postpartum. Women with a history of idiopathic or hormone provoked VTE (n = 74) received enoxaparin 40 mg subcutaneously once daily during pregnancy and for 6 weeks postpartum. The primary outcome was breakthrough VTE, and the secondary outcome was postpartum hemorrhage defined as blood loss greater than 500 mL. There were two (1.2%) VTE events and both occurred antepartum in the idiopathic VTE group. Postpartum hemorrhage occurred in 27 of 73 (37%) patients in the provoked VTE group and 32 of 88 (36.4%) in the unprovoked VTE group (P = 0.93). 73 Based on the low overall event rate, researchers concluded that the failure rate of enoxaparin 40 mg subcutaneously once daily is acceptably low, and higher doses are unnecessary.
Dosing Regimen for the Highlow Trial. 74 Patients Were Randomized Before 14 weeks Gestation and Continued Therapy Until 6 weeks Postpartum.
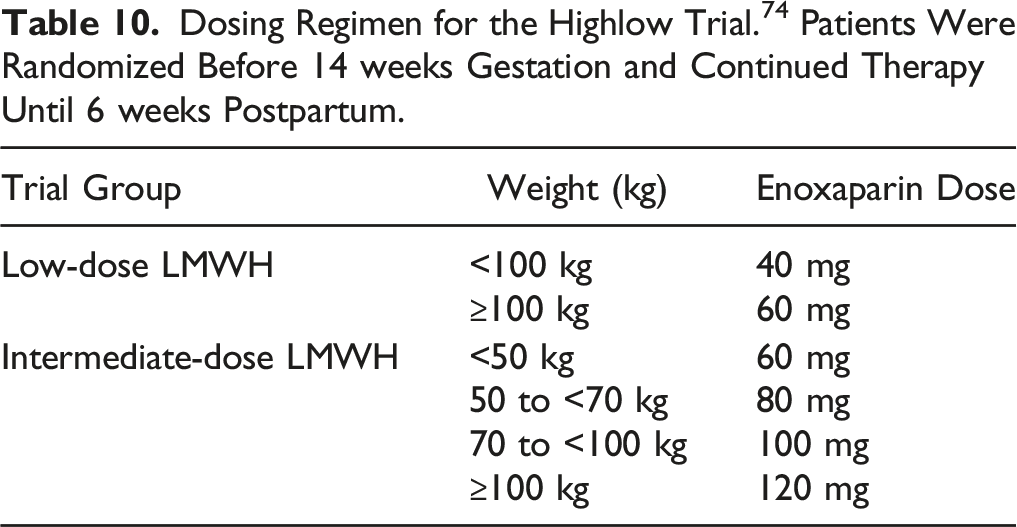
The efficacy outcome was recurrent VTE, and the safety outcomes included bleeding, blood transfusion, and mortality. 74 Recurrent VTE occurred in 16 of 555 (3%) subjects in the low-dose group and 11 of 555 (2%) subjects in the intermediate-dose group (RR 0.69 [95% CI 0.32-1.47]). For secondary outcomes, bleeding occurred in 23 of 520 (4%) subjects in the safety population (RR 1.16 [95% CI 0.65-2.09]). Intermediate-dose LMWH was not associated with decreased rates of VTE recurrence; therefore, the authors concluded that fixed low-dose LMWH is appropriate to prevent recurrent VTE during pregnancy and the postpartum period. Some limitations of the study included patient-reported adherence and deviations from the dosing protocol. Deviations from the dosing protocol likely occurred due to the open-label design and variation of individual provider’s practice.
Guidelines
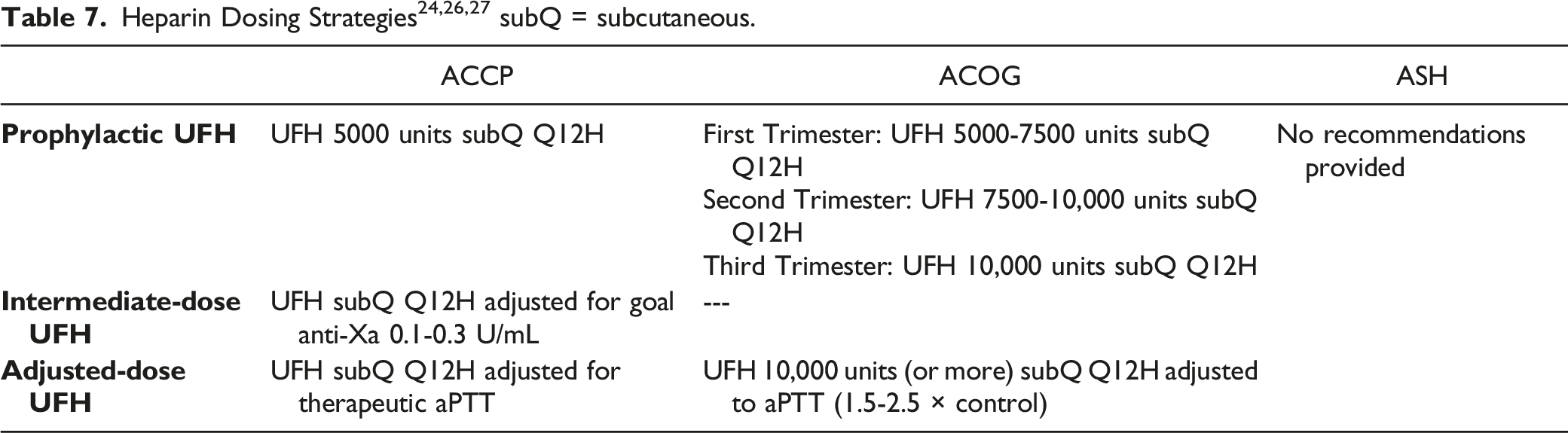
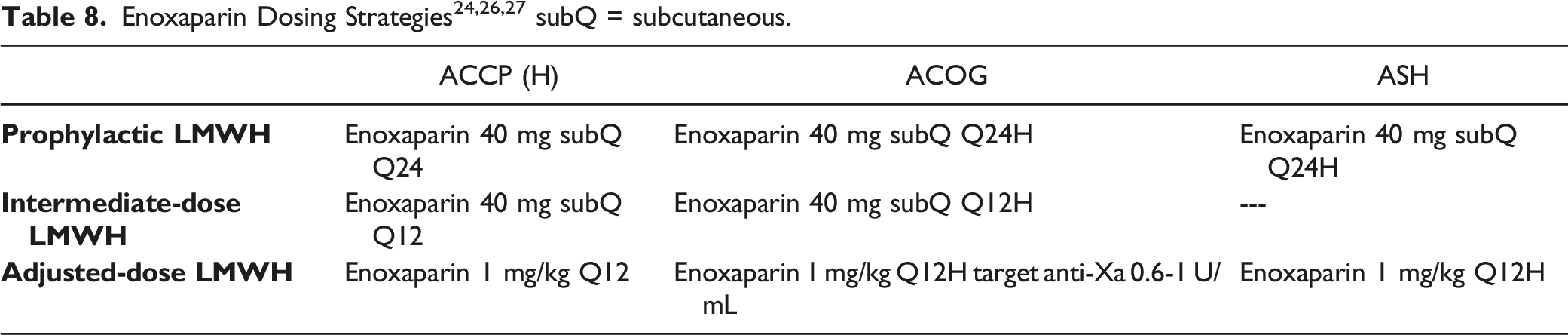
Three societies, ACOG, ACCP, and ASH, have developed national guidelines for managing obstetric patients at risk for VTE.24,26,27 The most recent of these guidelines was published in 2018 and does not reflect the most current literature available. As a result of the low quality and limited volume of available evidence, variation exists among national guidelines. Dosing recommendations for UFH and LMWH are shown in Tables 7 and 8. ACOG utilizes increasing doses of heparin throughout the pregnancy due to physiologic changes in blood volume and clearance while ACCP recommends the same dose throughout.24,26 The predictable profile of enoxaparin has created a consensus for dosing recommendations.
Dosage selection depends on the indication, interpretation of the associated risk of VTE, and the accompanying literature. Table 3 contains common indications for thromboprophylaxis and recommendations from national guidelines. In patients with a history of a single unprovoked VTE, there is a wide range of recommended doses. In the antepartum period, ACCP is the only guideline that provides the option of surveillance while ACOG and ASH recommend some degree of prophylaxis.24,26,27 All three recommend prophylaxis in the postpartum period. In patients with a history of a provoked VTE unrelated to pregnancy, there seems to be consensus among guidelines against prophylaxis in the antepartum period. However, in the 6 weeks postpartum, ACOG recommends surveillance while ACCP and ASH recommend prophylaxis. When considering thrombophilias, ACOG, ACCP, and ASH make varying recommendations with the available literature for the antepartum and postpartum period.
Conclusion
Pregnancy induces a hypercoagulable state that can lead to thrombosis in the presence of additional risk factors. When pharmacologic prophylaxis is indicated, LMWH is the preferred agent. However, there is a lack of high-quality data to guide initiation of thromboembolism prophylaxis which has led to variation among recommendations from national guidelines. Individual patient risk factors should undergo thoughtful consideration to weigh bleeding risk, cost, administration burden, and birth implications of anticoagulation in pregnancy. Additional prospective trials are needed to further elucidate optimal risk-assessment, dosing strategies, and duration of VTE prophylactic therapy in the obstetric population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.