
Abstract
Background:
A local health authority in Canada implemented its own Antimicrobial Stewardship Program (ASP) which provide guidelines to clinicians to utilize when treating infectious diseases such as community-acquired pneumonia (CAP). Objectives: The primary objective is to describe antibiotic usage patterns at the community hospital’s emergency department (ED) and to analyze the patterns in relation to ASP goals of reducing risk of infections, adverse drug events and antibiotic resistance, and to identify potential areas of improvement.
Methods:
This retrospective chart review included 156 adult patients with a diagnosis of CAP admitted to a community hospital ED from December 1, 2015 to November 30, 2016.
Results:
50.6% patients were prescribed moxifloxacin across all severity of CAP patients. Low and moderate severity CAP patients were most often prescribed antibiotic duration > 7 days. In low, moderate and high severity CAP patients who were treated using ceftriaxone, 100%, 88.9% and 66.6% patients were treated with ceftriaxone 2000 mg daily respectively.
Conclusions:
Antibiotic prescribing patterns suggest fluoroquinolones were frequently being over-prescribed, ceftriaxone dosages were often too high, and duration of antibiotics for low and moderate severity CAP were too long. More efforts are needed to promote appropriate antibiotic usage and optimize patient care.
Keywords
Introduction
Community-acquired pneumonia (CAP) is a common disease with a high incidence of morbidity and mortality, as well as a large economic burden. 1 In Canada, CAP has an annual incidence of 12 per 1000 adults and a 30-day in-hospital mortality of 14%. 1 Canadian emergency department (ED) treats approximately 126,000 patients each year for pneumonia, with approximately 30% of these patients getting admitted into the hospital. 2 Streptococcus pneumoniae is the leading bacterial cause of CAP; beta-lactams, macrolides and fluoroquinolones (FQ) are typical treatment options. 3 Resistant strains of S. pneumoniae to these drug classes are now noted in Canadians, especially in adults over the age of 65. 4 Worham et al. 5 observed an increase in FQ popularity among prescribers, perhaps due to their convenient dosing. However, this selective preference may lead to greater FQ resistance, especially for gram negative bacteria. 6 In addition, there is strong epidemiological association of FQ use with Clostridium difficile infection (CDI). 7 Moreover, the FDA has issued Box Warnings about the potential serious side effects of FQ, such as tendinitis, tendon rupture, confusion, hallucinations, and blood sugar disturbances. 8
IDSA and the American Thoracic Society (ATS) have created comprehensive guidelines for the management of CAP, which utilize risk stratification tools such as the Pneumonia Severity Index (PSI) and CURB-65 (confusion, uremia, respiratory rate, blood pressure, age 65 years or greater) score in addition to clinical assessment to help guide the appropriate CAP treatment. 9 At the local community hospital using the Antimicrobial Stewardship Program (ASP) guideline for CAP, CRB-65 (confusion, respiratory rate, blood pressure, age 65 years or greater) score is used instead of CURB-65 as a risk stratification tool. CRB-65 has been shown to correlate highly with CURB-65 and is more convenient as it doesn’t require blood work to be drawn. 10
In response to rising antimicrobial resistance, antimicrobial stewardship (AMS) initiatives have been implemented across the globe, driven by an ethical imperative to protect public health and improve patient care. 11 Accreditation Canada has also mandated AMS to be a component of all health care organizations that provide inpatient care and chronic, complex care. 12 A local health authority in Canada implemented an Antimicrobial Stewardship Program (ASP) with the primary goals of reducing risk of infections, adverse drug events and antibiotic resistance while reducing antibiotic costs. 13 The 3 main goals of the ASP include: 1. Optimize patient care through appropriate selection and use of antimicrobials, while minimizing adverse events, 2. To slow the emergence of antimicrobial resistance by limiting selection from antimicrobial misuse, and 3. To improve health care efficiency by reducing unnecessary antimicrobial use. 14 With this in mind, the team has identified specific items to address, including reduction of unnecessary FQ usage, lowering empiric dose of ceftriaxone from 2000 mg to 1000 mg, and decreasing the duration of antibiotics to 5 days in the low and moderate severity CAP categories. Thus, we sought to describe antibiotic use for CAP at a community hospital’s ED and analyze the pattern in relation to our goals and identify potential areas of improvement.
Methods
This was a retrospective chart review conducted at a community hospital ED in Canada. Our primary objective is to describe the antibiotics usage patterns for CAP treatment in ED. We identified the use of all antibiotics with their doses and durations. All-cause in-hospital mortality, hospital length of stay (LOS), and in-hospital CDI rates were collected as adverse events. A list of patients that were admitted through ED were generated by the health authority informatics department using ICD-9 codes. Patients were randomly selected using an online random number sequence generator. 15 In the case where the patient meets the exclusion criteria, the next patient on the list was assessed for eligibility. Electronic Medical Records (EMR) was used to obtain demographic and diagnostic information, allergy, medical history, clinical assessment notes (any presence of cough, sputum production, pleuritic chest pain or dyspnea), vital signs, laboratory and radiographic finding (chest x-ray), and prescribing data. The specific laboratory tests include white blood cell (WBC) count, neutrophil count, serum creatinine, estimated glomerular filtration rate (eGFR), blood urea nitrogen (BUN), C-reactive protein, blood culture, sputum culture, and procalcitonin level. Inclusion criteria were adults first admitted via the community hospital’s ED with a primary diagnosis of CAP between December 1, 2015 to November 30, 2016. Primary diagnosis of CAP is identified if the patients had CAP as part of their diagnosis on admission, even if the patients may have other diagnosis that does not require antibiotic treatment. Patients were excluded if they had other diagnoses that required treatment with antibiotics, who refused antibiotic treatment, who had a recent admission to a hospital within 10 days prior 1 to admission for pneumonia to exclude hospital acquired pneumonia (HAP), who had either empyema, pneumonitis due to food or emesis, or aspiration pneumonia, and who were considered immunocompromised with the following conditions: hematologic malignant disease, history of organ transplantation, tuberculosis, human immunodeficiency virus (HIV) infection, cystic fibrosis, or were on therapy with immunosuppressant drugs (long-term corticosteroids [i.e. > 10 mg daily or cumulative dose of > 700 mg equivalent dose of prednisone], 16 methotrexate therapy, chemotherapy, and radiation therapy). The study was approved by the health authority’s ethics board.
CRB-65 score is used to stratify severity (1 point is awarded to each of confusion, respiratory rate ≥ 30 breaths per minute, low systolic [< 90 mm Hg] or diastolic blood pressure [≤ 60 mm Hg] and age ≥ 65 years). 17 A patient with a CRB-65 score of 0 would be considered low severity, a CRB-65 score of 1-2 would be considered moderate severity, and a CRB-65 score of ≥ 3 or if the patient has respiratory failure or requiring ICU admission would be considered high severity.
Statistical Analysis
Based on an annual admission rate of 262 to ED for CAP, a sample size of 156 was deemed representative of the population. Qualitative variables were expressed as numbers and percentages while quantitative variables (age, hospital LOS) were expressed as mean, median and interquartile range.
Results
Of the 262 patients admitted via the community hospital’s ED for CAP from December 1, 2015 to November 30, 2016, 156 patients were included in the analysis (Figure 1). 15 Patients’ baseline characteristics and comorbidities are presented in Table 1. The most common allergy was penicillins (n = 21, 13.5%), followed by fluoroquinolones (n = 11, 7.1%) and cephalosporins (n = 9, 5.8%).
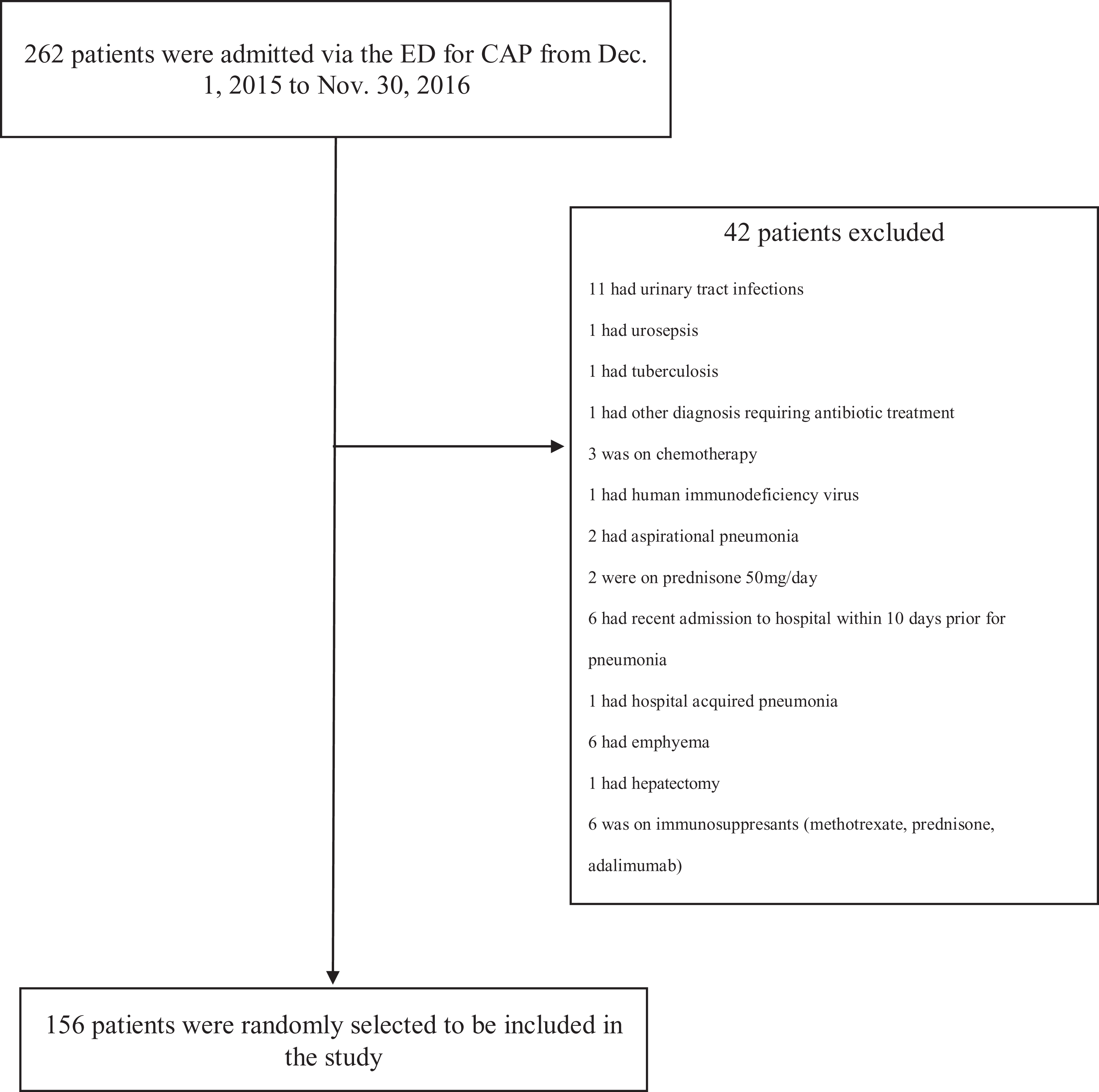
Study flow diagram.
Patient Baseline Characteristics.

Abbreviations: IQR, Interquartile range; eGFR, estimated glomerular filtration rate (mL per minute per 1.73 m2).
Patients with any of the comorbidities (diabetes, heart disease, liver disease, lung disease, renal disease) are at high risk for pneumonia according to the Pneumonia Severity Index (PSI).
The organisms found in blood and sputum cultures can be found in Figure 2. Not all patients had blood and sputum cultures available. There was 1 patient who had probable viral pneumonia based on clinical notes.
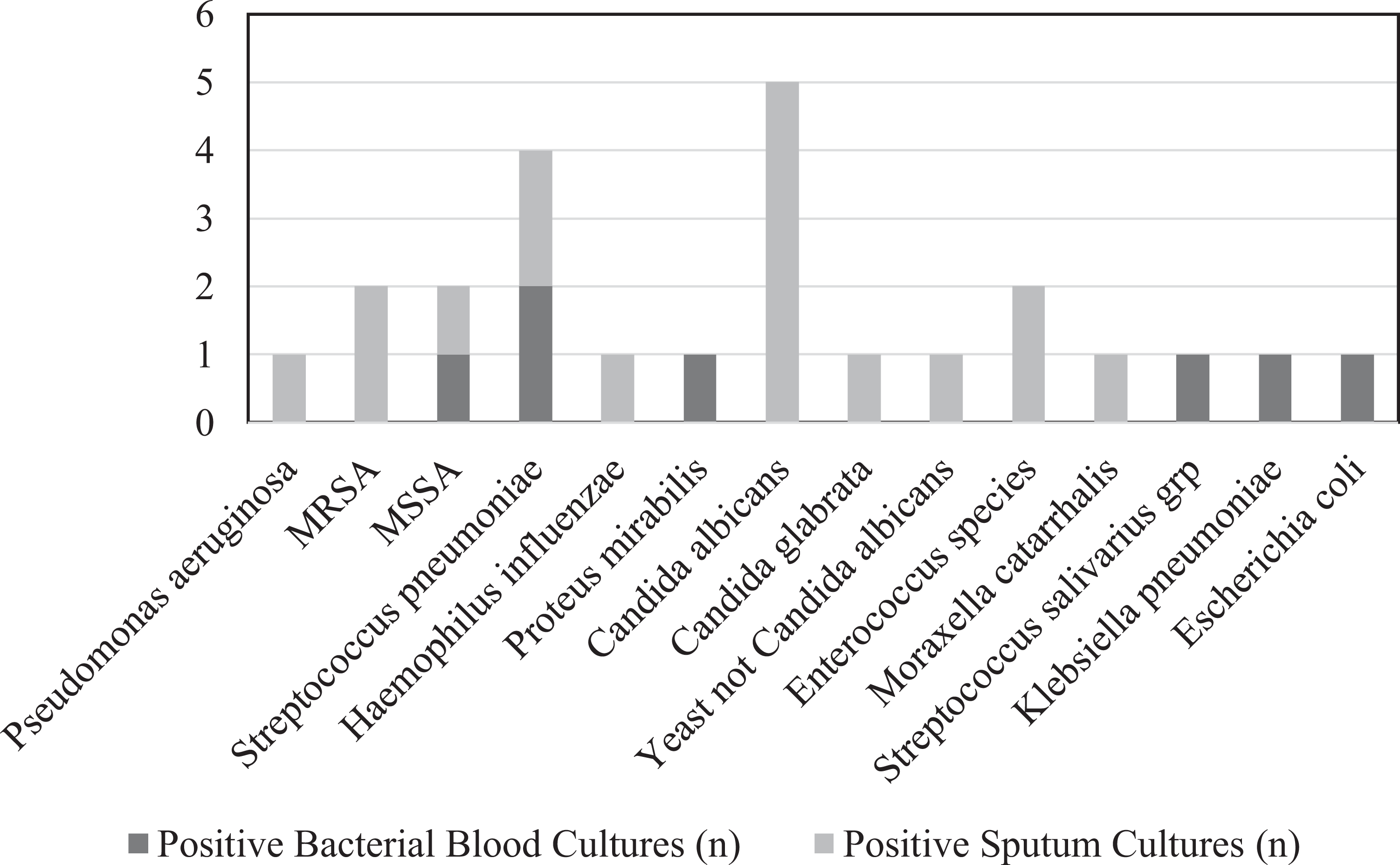
Summary of microbiology lab data from blood and sputum cultures. MRSA, Methicillin-resistant Staphylococcus aureus; MSSA, Methicillin-sensitive Staphylococcus aureus.
Procalcitonin level was ordered in 1 patient (0.6%). The 1 patient who got tested had a procalcitonin level of 0.25 μg/L with no follow-up testing.
A total of 28 patients (17.9%) had low severity CAP (Table 2). The most frequently prescribed antibiotic was ceftriaxone (n = 8, 28.6%), followed by azithromycin (n = 6, 21.4%) and moxifloxacin (n = 6, 21.4%). All the prescribed doses of ceftriaxone were 2000 mg. Low severity patients were most often prescribed total antibiotic duration >7 days (n = 19, 67.9%) (Table 3).
Summary of Antibiotic Usage With Drug, Dose and Frequency.
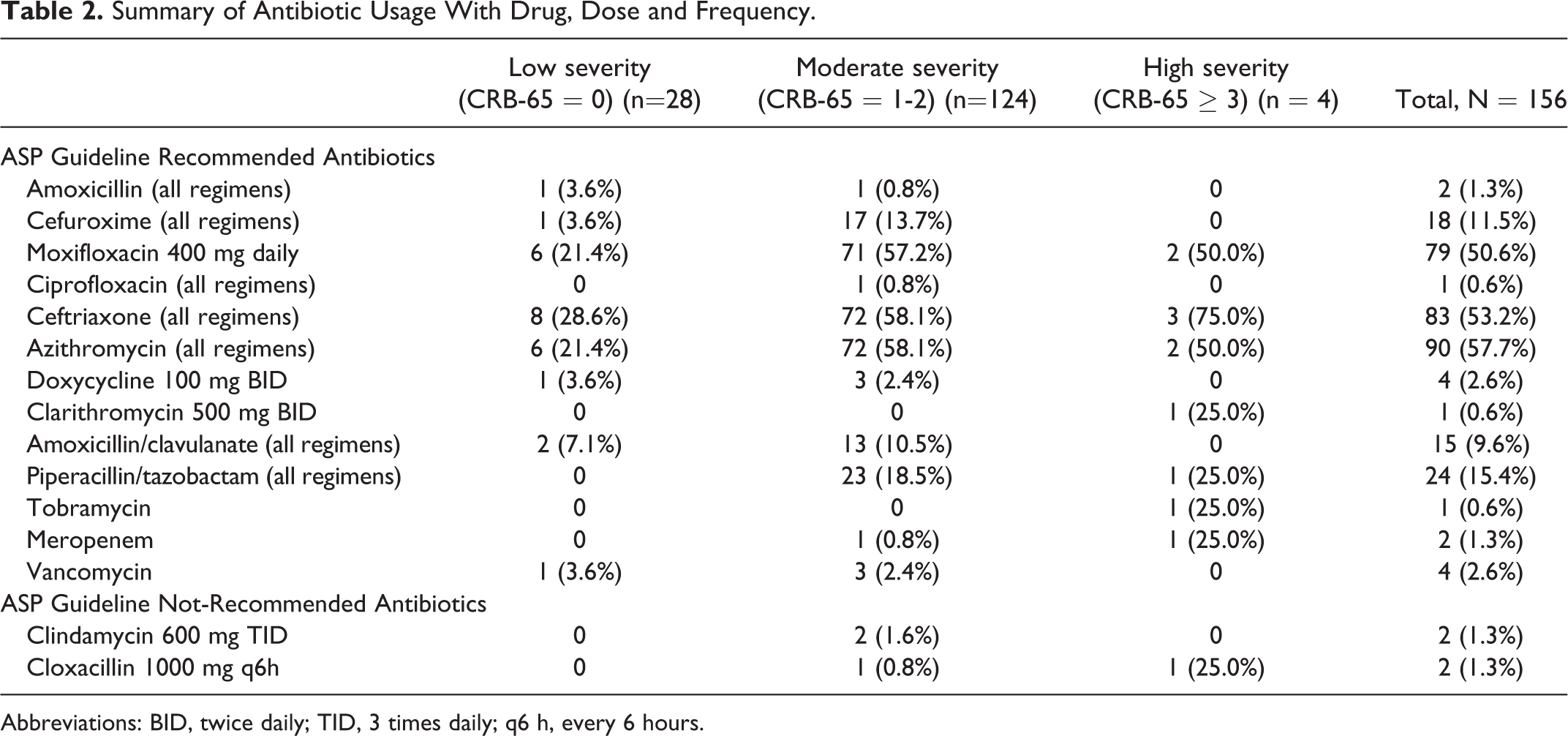
Abbreviations: BID, twice daily; TID, 3 times daily; q6 h, every 6 hours.
Duration of Antibiotics.

There were 124 patients (79.5%) who had moderate severity CAP (Table 2). The most frequently prescribed antibiotics among moderate severity CAP were ceftriaxone plus azithromycin (58.1%, n = 72), moxifloxacin (58.1%, n = 72) and piperacillin/tazobactam (18.5%, n = 23). Out of those who were prescribed ceftriaxone, 8 patients (11.1%) were given 1000 mg daily and 64 patients (88.9%) were given 2000 mg daily. Moderate severity patients were most often prescribed total antibiotic duration >7 days (n = 56, 45.2%) (Table 3). For patients who were prescribed azithromycin, 31 patients (43%) were given 500 mg daily for less than or equal to 4 days, 31 patients (43%) were given 500 mg daily for greater than 4 days, 6 patients (8.3%) were given only 250 mg daily, and 4 patients (5.6%) were given 500 mg once followed by 250 mg daily for 4 days.
There were 4 patients (2.6%) who had high severity CAP (CRB-65 ≥ 3) (Table 2). The most frequently prescribed antibiotics for high severity CAP were ceftriaxone with azithromycin (75%, n = 3), ceftriaxone alone (50%, n = 2), and moxifloxacin (50%, n = 2). Piperacillin/tazobactam (25%, n = 1) or meropenem plus tobramycin (25%, n = 1) were the third most frequently prescribed antibiotics. Out of those who were prescribed ceftriaxone, 1 patient (33.3%) was given 1000 mg daily and 2 patients (66.6%) were given 2000 mg daily.
Out of the 156 patients, there were 15 patients who were switched from ceftriaxone or moxifloxacin to piperacillin/tazobactam midway during treatment. Overall, the average in-hospital LOS was 8.6 days, median hospital LOS was 5.5 days, and in-hospital mortality rate was 6.4%.
Discussions
Based on our observations on antibiotics prescribing pattern, cephalosporins prescribing rates were similar across all severity of CAP. Ceftriaxone had a slightly higher prescribing rate than moxifloxacin (28.6% vs 21.4% in low severity patients, 58.1% vs. 57.2% in moderate severity patients, 75% vs. 50% in high severity patients). However, moxifloxacin is generally reserved for patients with severe beta-lactam allergies, 17 and given that 80.8% of our patients had no documented penicillin or cephalosporin allergies, moxifloxacin was overprescribed. Thiessen et al. found that fluoroquinolones were the most frequently overprescribed antibiotic in the low-risk group, according to the IDSA/ATS CAP Treatment Guidelines. 18 Overuse of fluoroquinolones is a concern due to the risk of serious disabling side effects, such as tendonitis, tendon rupture, peripheral neuropathy, and central nervous system side effects including anxiety, dizziness, and confusion.8,19,20 Both the U.S. Food and Drug Administration (FDA) and Health Canada have issued a black box warning on fluoroquinolones advising for judicious use of fluoroquinolones.19,20 In addition, the most recently published case-control study published in the Journal of the American College of Cardiology in 2019 found that current and recent use of fluoroquinolones had statistically significant higher risk for aortic and mitral valve regurgitation compared to amoxicillin and azithromycin. 21 The impact of the overuse of fluoroquinolones is especially problematic for our sampled patient population, which consists of mostly elderly patients with a mean age of 75 years as they are especially vulnerable to adverse reactions of the renal and central nervous system.22,23
In patients who were appropriately prescribed ceftriaxone, we observed that 2000 mg was more often prescribed than 1000 mg dose. A randomized double-blinded trial in 1995 found no significant difference in clinical outcome such as improvement rate and duration of therapy between patients who received ceftriaxone 1000 mg versus 2000 mg daily in the treatment of community-acquired infections including CAP. 24 In a more recent meta-analysis, it was found that ceftriaxone dose of 1000 mg daily is as safe and effective as other regimens (2000 mg daily, 1000 mg twice a day) and that dosages higher than 1000 mg daily did not show improved clinical outcomes for CAP. 25 Thus, ceftriaxone 2000 mg is unnecessary for the treatment of CAP and can contribute to antibiotic resistance. Our local guidelines now recommend ceftriaxone 1000 mg over 2000 mg dose for CAP. The impact of this change remains to be seen.
Although IDSA did not have a clear recommendation of optimal total duration of antibiotic use, our ASP guidelines recommended 5 days for low and moderate severity CAP and 7 days for high severity. 17 Urganda et al. compared patients who were treated based on clinical stability with antibiotics for a minimum of 5 days and patients who were treated with traditional durations prescribed by physicians found no difference in clinical success rate and symptoms at 10 and 30 days. 26 Low and moderate severity CAP patients were often prescribed antibiotic duration longer than 5 days (Table 3). Our ASP guidelines also recommended the azithromycin duration is either 500 mg for 3 days, or 500 mg for 1 day followed by 250 mg for 4 days, with longer durations only indicated in Legionella infection. 17 Longer durations of antibiotic treatment increases the risk of antibiotic resistance in subsequent infections, as well as poses higher risk for C. difficile infection.27,28 Azithromycin was often prescribed longer than 4 days with a total treatment dose greater than 1500 mg (38.8% patients had duration greater than 4 days with a total dose greater than 1500 mg), with the most common regimen being 500 mg daily for 5 days. This may be attributed to the automatic 5 days stop date policy within the health authority and physicians often do not specify treatment duration on the order. Due to the post-antibiotic effect of azithromycin and its prolonged half-life of 65 hours, the 3 or 5 day (1500 mg total) regimens provide equal serum concentration and efficacy against common CAP pathogens compared to the higher dosing regimens.29,30 Therefore, patients who received azithromycin 500 mg daily for 5 days or greater were overexposed to azithromycin and this can increase the risk of adverse events and resistance to macrolides. 31 The FDA warns that azithromycin use can lead to fatal irregular heart rhythm, particularly in patients who are at risk for cardiovascular events, those with existing QT interval prolongation or on medications that prolong QT interval and those with low potassium or magnesium. 32 It was found that during 5 days of therapy of azithromycin compare with patients who took no antibiotics, there was an increased risk of cardiovascular death. 33 In 2014, there were 35.2% of S. pneumoniae non-susceptible to erythromycin in British Columbia, although the resistance rate has remained stable since 2007, 34 globally, there has been an increasing trend of resistance of macrolides to not only S. pneumoniae, 35 but also H. influenzae 36 and Mycoplasma pneumoniae. 31 Resistance to macrolides has been found to be significantly associated with global macrolides consumption. 37 Macrolides resistance can also impact the treatment of infectious diseases other than CAP. In Canada, azithromycin resistance in Neisseria gonorrhoeae has doubled from 5% in 2015 to 7% in 2016. 38 It was found that macrolides resistance is a cause of outpatient pneumonia therapy failure. 36 Therapeutic failure to eradicate CAP can lead to bacteremia, empyema and death. 39 Therefore, it is important to continue following ASP guidelines to slow down or prevent further resistance to macrolides.
Another trend that we observed was for patients on ceftriaxone (with or without azithromycin) or moxifloxacin who had only laboratory worsening but showed no clinical evidence were often switched to piperacillin/tazobactam. We speculate that this was due to the clinical experience of prescribers and the broader-spectrum coverage of piperacillin/tazobactam, as in most cases, there were no microbiological evidence to support the broadening of antibiotic spectrum. 40 However, due to the retrospective nature of this study, we were unable to assess the clinical status of the patients and there may be signs and symptoms that led to the escalation of antibiotics by the physician.
Procalcitonin level was not readily utilized in our study. Procalcitonin level is a tool to help clinicians reduce unnecessary antibiotic use for possible non-bacterial pneumonia. 17 It is recommended that antibiotic therapy can be discontinued when procalcitonin is < 0.25 μg/L or reduced by ≥ 80% on follow-up testing. 17 The lack of procalcitonin testing and follow-up indicates there is potential for increased awareness, education and utilization of this tool.
There were a number of limitations in our study. Firstly, as a retrospective study, particularly for those with higher severity CAP and multiple comorbidities, it is difficult for us to get a complete picture of the patient’s clinical status and assess the appropriateness of the antibiotics given. As a result, we could only assess the appropriateness of empiric antibiotic therapy according to the CRB-65 score, which presents the limitation of not taking into consideration of the patient’s comorbidities, hypoxemia, and functional status. 41 In addition, we did not take into account any potential drug interactions, which could have led to the preference of one antibiotic over another. Ceftriaxone poses less potential for drug interactions than fluoroquinolones such as QTc prolongation so drug interactions in theory would not lead to the increased usage of fluoroquinolones over ceftriaxone. Unfortunately, this study was not designed to assess the potential resistance that may emerge from the extended duration of antibiotics. Finally, since our study was carried out in a single community hospital, the results may not necessarily be applicable to other clinical settings.
Some potential areas of improvement in the future include decreasing fluoroquinolones prescribing, reducing dosage of ceftriaxone from 2000 mg to 1000 mg, limiting azithromycin total dose to 1500 mg, and reducing the duration of total antibiotic therapy according to CAP severity. Physicians should be encouraged to indicate the duration of antibiotic therapy at the time of prescribing and utilize procalcitonin level to guide antibiotic therapy. Some barriers to physician adherence to guidelines include lack of familiarity, lack of awareness, lack of agreement with specific regimens, lack of outcome expectancy, lack of time and patient preference interfering with guideline recommendations. 42 Increased education may help to increase familiarity and utilization of the CAP pre-printed orders (PPO) and the ASP guidelines.
Conclusion
Our findings suggest that inappropriate antibiotic use for CAP remain an important problem in the ED. It is clear that the problem involves multiple components, not limiting to antibiotics choice. These patterns suggest more ASP efforts together with the cooperation of the local health authority to improve system-level issues, such as the incorporation of clinical decision support tools, are needed to promote appropriate antibiotic usage and optimize patient care.
Footnotes
Authors’ Note
The study was approved by the Fraser Health Research Ethics Board (FHREB approval number 2017-059).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.