
Abstract
Background:
Clopidogrel is the most commonly prescribed P2Y12 inhibitor for acute coronary syndrome (ACS) or stent placement, though ticagrelor or prasugrel may be preferred. Medication-related factors may influence selection of therapy.
Objectives:
To determine which factors most greatly influence cardiology-provider and patient selection of P2Y12 inhibitor to guide shared-decision making (SDM).
Methods:
Single-center study assessed survey responses from 32 cardiology-providers who prescribed and 105 patients who received clopidogrel, prasugrel, or ticagrelor for ACS or stent placement. Respondents ranked factors influencing P2Y12 inhibitor selection and reported preference of therapy. Patients reported experience with shared decision-making process.
Results:
Cardiology-providers ranked risk of bleeding, comfort/experience, and cost as most influential. Patients ranked risk of drug interaction, adverse effects, and reduction in myocardial infarction as most influential. Significant differences between cardiology-providers and patients were found for 5 of 8 factors. Cardiology-providers ranked once daily administration (p = 0.01), risk of bleeding (p = 0.002), and cost (p < 0.001) as more important than patients. Patients ranked risk of adverse effects (p = 0.007) and drug interactions (p = 0.005) as more important than cardiology-providers. Cardiology-providers prescribed ticagrelor 42.3% of the time following ACS, though 78.1% ranked it as their preferred agent. Patients were prescribed ticagrelor 9.3% of the time, though 55.7% ranked it as their preferred agent. Use of SDM was reported by 21.6% of patients and 88.5% were unaware that multiple P2Y12 inhibitors existed.
Conclusion:
Significant differences exist between cardiology-providers and patients regarding factors influencing P2Y12 inhibitor selection, specifically safety-related factors, once daily administration, and cost. Most patients were not involved in SDM.
Keywords
Introduction
Acute coronary syndrome (ACS) is a major cause of morbidity and mortality, estimated to affect one American every 42 seconds. 1 Advances in management strategies over the last 30 years have reduced post-ACS 1-year mortality rates more than 50%. 2 Antiplatelet therapy with P2Y12 inhibitors significantly reduces secondary risk of myocardial infarction (MI) when administered in combination with aspirin.3-5
Reduced incidence of MI associated with P2Y12 inhibitors was discovered in 2001 with clopidogrel. Since this discovery, additional P2Y12 inhibitors have gained FDA approval. Prasugrel gained approval after comparison with clopidogrel demonstrated an association with significantly lower risk of MI, though at the expense of increased major, life-threatening, and fatal bleeding. 4 Ticagrelor, the most recently approved P2Y12 inhibitor, was associated with a significantly lower risk of MI compared to clopidogrel. Additionally, ticagrelor is the only P2Y12 inhibitor associated with significant mortality reduction and was not associated with increased risk of major, life-threatening, or fatal bleeding compared to clopidogrel in the study that lead to its approval. However, ticagrelor increased the risk of non-CABG related major bleeding, dyspnea, and increased serum uric acid. 5 Prior to 2019, randomized controlled trials comparing prasugrel and ticagrelor did not find significant differences in safety or efficacy. 6 A recently published randomized controlled trial comparing prasugrel and ticagrelor found prasugrel significantly reduced the composite risk of death from any cause, myocardial infarction, or stroke. The composite endpoint was primarily driven by a reduction in myocardial infarction. 7 Genetic polymorphisms and drug interactions associated with clopidogrel, potentially reducing conversion of clopidogrel into an active metabolite, have led to hypotheses of efficacy advantages of prasugrel and ticagrelor over clopidogrel. These advantages remain a theoretical benefit but have not been supported by available literature.8,9
In addition to the benefits found in literature, the American College of Cardiology/American Heart Association (ACC/AHA) guidelines and European Society of Cardiology (ESC) guidelines state that it is reasonable to choose prasugrel or ticagrelor over clopidogrel in patients following ACS.10-12 Despite guideline recommendations supporting the use of ticagrelor and prasugrel, clopidogrel remains the most commonly prescribed P2Y12 inhibitor. 13 The cause for this mismatch between primary literature and practice patterns is unknown. Drug preferences are often multi-factorial, related to cost, efficacy, safety, ease of use, and comfort/experience contributing to selection. To our knowledge, no literature is available assessing factors that influence physician or patient preferences of P2Y12 inhibitors.
Though no data pertaining to P2Y12 inhibitor selection are available, literature has been conducted to assess factors that influence medication preference with other drug classes. In one study, values and preferences of providers and patients receiving oral anticoagulation for atrial fibrillation were assessed. 14 Participants favored safety and efficacy above other attributes; however, the order of attributes sorted in terms of perceived importance varied between providers and patients. When asked to select a preferred anticoagulant based on attribute profiles, providers selected apixaban; however, stated drug preferences and prescribing patterns found rivaroxaban and warfarin to be most commonly prescribed. This study highlights the discrepancy between which factors influence provider and patient preferences and between theoretically preferred medications and actual prescribing patterns.
Awareness of factors influencing provider and patient medication therapy preference facilitates shared decision-making (SDM). Shared decision-making is a process that allows providers and patients to work together to make decisions based on clinical evidence, balancing risks and expected outcomes with patient preferences and values. 15 Increased interest in SDM has emerged as literature reflects improvements in decision quality, patient knowledge, risk perception, and overall patient satisfaction with its use.16-18 The SDM approach is valuable but relies on appropriate patient disease-state and drug-therapy comprehension. A baseline assessment of patient values regarding antiplatelet drug-therapy for heart attack or cardiac stent placement is essential to developing educational tools necessary to facilitate SDM.
The purpose of this study was to survey cardiology-providers who recently prescribed and patients who recently received a P2Y12 inhibitor to identify factors influencing P2Y12 inhibitor preference and to assess patient experiences with this therapy. The goal of this study was to obtain information that could be used to guide cardiology providers in optimizing the SDM process in selection of antiplatelet therapy.
Methods
Study Design and Participants
We performed a single-center, survey study of cardiology-providers and patients affiliated with the academic medical center. Cardiologists or cardiology fellows actively practicing within the UT Health System were included as “cardiology-providers.” Patients registered in the UT Health System who received a prescription for clopidogrel, prasugrel, or ticagrelor between June of 2016 and June of 2017 and had ICD 9 or ICD 10 codes indicating ACS or cardiac stent placement were included as “patients.” Patients were identified using the Informatics for Integrating Biology and the Bedside (I2B2) Clinical Integrated Data Repositories (CIRD), a large-scale database allowing a patient search query that provided a data set limited to patients meeting inclusion criteria. Patients were excluded if they were not between 18 and 80 years of age or lacked an available mailing address. All cardiology-providers and patients who met inclusion criteria were contacted to participate. For cardiology-providers and patients, consent was determined based on survey completion and submission.
Cardiology-Provider and Patient Surveys
The 2 surveys evaluated: 1) which factors cardiology-providers felt influence prescribing, 2) which factors cardiology-providers believe patients valued, 3) which factors patients deemed most influential in selection of therapy, 4) cardiology-provider and patient experience with each therapy, and 5) P2Y12 inhibitor preference for cardiology-providers and patients. Eight factors of potential influence were assessed and included mortality reduction, MI reduction, risk of bleeding, risk of adverse effects, risk of drug interactions, once-daily administration, comfort/experience, and medication cost. Participants ranked factors in order of importance, with a score of 1 indicating the most important factor and a score of 8 indicating the least important. Of note, cardiology-providers were asked to first evaluate factor influence from the perspective of a provider (provider-perspective) and secondly based on what they perceived as most influential to their patients (patient-perspective). Patient experience with therapy was assessed based on perceived financial burden, adverse effects, use of other P2Y12 inhibitors and participation in SDM.
In assessing preferences of cardiology-providers, providers were asked to provide an evidence-based therapeutic preference and an actual preference in clinical practice. The evidence-based therapeutic preference of cardiology-providers was based on what P2Y12 inhibitor they felt most confident prescribing based on risks and benefits in the literature, following ACS with or without stent placement and stable ischemic heart disease (SIHD) with stent placement. Cardiology-providers were also asked to provide the primary reason for this preference. The actual preference in clinical practice of cardiology-providers was based on self-reported prescribing rates based on indication. Patient P2Y12 inhibitor preference was assessed by providing patients with a hypothetical scenario in which 3 medications, noted as “Medicine A,” “Medicine B,” and “Medicine C” were given attributes matching each P2Y12 inhibitor. For example, “Medicine A” which represented clopidogrel stated daily dosing of “one time a day” while “Medicine B” which represented ticagrelor stated daily dosing of “two times a day.”
As no validated surveys were available to meet the needs of this study, survey design was based on surveys used in a similar study. 14 Surveys were piloted and revised prior to being dispersed to their respective populations. Piloting was done by administering surveys to volunteers with educational backgrounds comparable to the intended populations. Comments from pilot testers were discussed by the authors and updates were made to enhance survey clarity. Cardiology-provider and patient surveys are provided in the supplemental materials of this article.
Study Procedures
Cardiology-provider surveys were administered in-person in paper format. Opportunities for in-person completion included department meetings, clinic days, cardiac catheterization lab days, and office hours. Additional contact attempts were made until either 4 contact attempts had elapsed or participation was declined.
Patient surveys and prepaid return envelopes were sent via the United States Postal Service (USPS) to home addresses. Surveys were confidential and included a de-identified tracking code to facilitate follow-up contact. Two weeks after initial survey mailing, a reminder postcard was sent to non-responders. Four weeks after initial survey mailing, a second survey was sent to remaining non-responders. Follow-up procedures were conducted in this manner to yield response rates approaching 50% based on estimates for mail-based surveys. 19 Funding for logistical costs associated with administration of patient surveys was provided by the Feik School of Pharmacy Competitive Intermural Scientific Research Award. Financial incentives were not used to increase response rates for cardiology-providers or patients.
Statistical Analysis
Analysis included all cardiology-providers and patients who met inclusion criteria. Participant demographics and experiences with P2Y12 inhibitor therapy were treated as parametric data using descriptive statistics. Ranking of factors of importance were analyzed between groups (patient perception, cardiology-provider perception, and cardiology-provider perception of patient beliefs) with the Kruskal-Wallis test. Factors demonstrating statistically significant differences were analyzed as matched cardiology-provider-patient comparisons with Dunn’s tests. The choice to use non-parametric tests aligned with the use of ranking within the surveys. The Kruskal-Wallis tests were used as omnibus tests to examine the differences between the 3 groups and post-hoc Dunn’s tests were used to pinpoint exact group differences. Results are reported in Mean Ranks, due to the ranked nature of the data and the subsequent non-parametric analysis. The congruity of the P2Y12 inhibitor desired by the patient, based on the hypothetical scenario response, and the P2Y12 inhibitor prescribed were measured using a non-parametric Chi-square test for independence.
Results
A total of 39 cardiology-providers met inclusion criteria, of which, 32 completed the survey (82.1%). Responses were evenly split between cardiologists (n = 16) and cardiology fellows (n = 16). Average time in specialty was 17.9 years for cardiologists and 2.6 years for cardiology fellows.
A total of 579 patients met inclusion criteria (Table 1). Following 3 contact attempts (the initial mailed survey, reminder postcard, and second mailed survey) a total of 105 completed surveys were received (18.1%). The patient population was predominantly male (61.4%) with an average age of 67.2 years. Indication for P2Y12 inhibitor therapy was balanced between ACS with or without stent placement (49.4%) and SIHD with stent placement (46%). A small percentage of patients were unsure of their indication (4.6%). Of the 75 patients (71.4%) who reported their prescribed P2Y12 inhibitor, 85.33% were prescribed clopidogrel, 5.33% were prescribed prasugrel, and 9.33% were prescribed ticagrelor. Most patients reported currently taking aspirin (90%) or had received aspirin in the past (5%).
Population Characteristics of Patients.
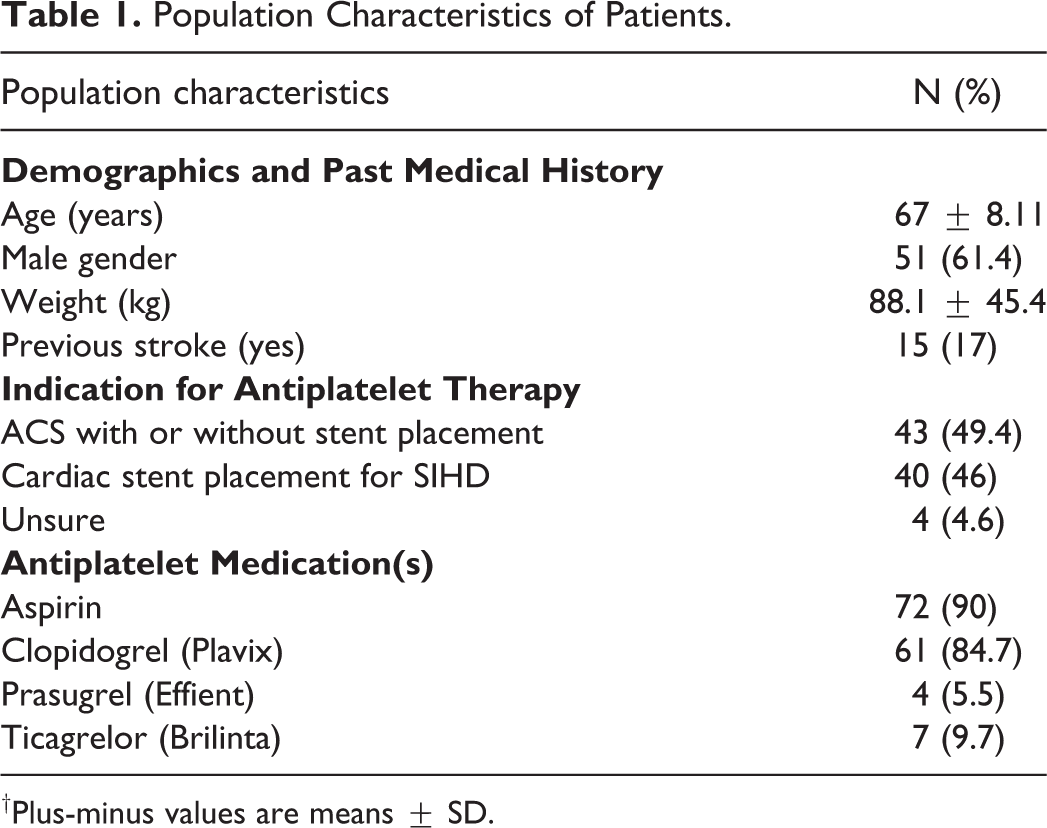
†Plus-minus values are means ± SD.
Ranking of Influential Factors for P2Y12 Inhibitors
Cardiology-provider (provider-perspective) ranking of factors from most to least influential were risk of bleeding, comfort/experience, medication cost, MI reduction, mortality reduction, risk of drug interaction, risk of adverse effects, and once daily administration. Cardiology-provider (patient-perspective) ranking of factors from most to least influential were medication cost, once daily administration, risk of bleeding, risk of adverse effects, mortality reduction, comfort/experience, MI reduction, and risk of drug interactions. Patient ranking of factors from most to least influential were risk of drug interactions, risk of adverse effects, MI reduction, mortality reduction, comfort/experience, once daily administration, risk of bleeding, and medication cost. Figure 1 provides the mean rank assigned scores for each factor.
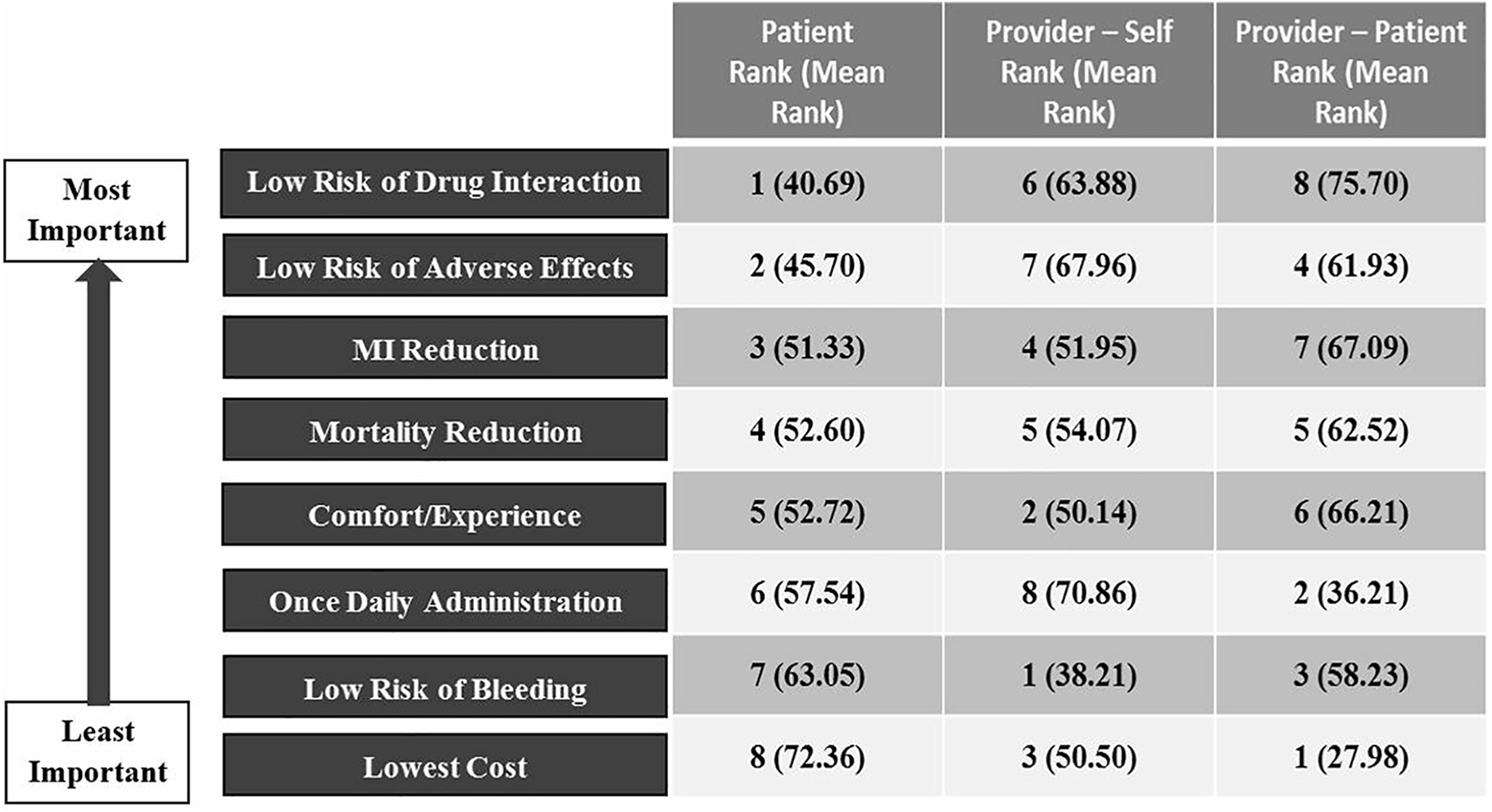
Ranking of influential factors for cardiology-providers and patients. MI indicates myocardial infarction. “Provider-Self” indicates cardiology-provider rankings based on their provider-perspective. “Provider-Patient” indicates cardiology-provider rankings based on their patient’s perspective.
Significant differences between cardiology-provider influential factors in prescribing and patient rankings were identified for 5 of the 8 factors. The factors that demonstrated differences between the mean rankings were: risk of adverse effects, risk of drug interactions risk of bleeding medication cost and once daily administration. Additional detailing of the numerical and statistical differences can be found in Table 2. Cardiology-providers (provider-perspective) ranked risk of bleeding and medication cost as more important than patients. Patients ranked risk of adverse effects and risk of drug interactions as more important than cardiology-providers (provider-perspective). Cardiology-providers (patient-perspective) ranked medication cost and once daily administration as more important than patients. Patients ranked risk of drug interactions as more important than cardiology-providers (patient-perspective).
Comparison of Rankings Between Cardiology-Providers and Patients.
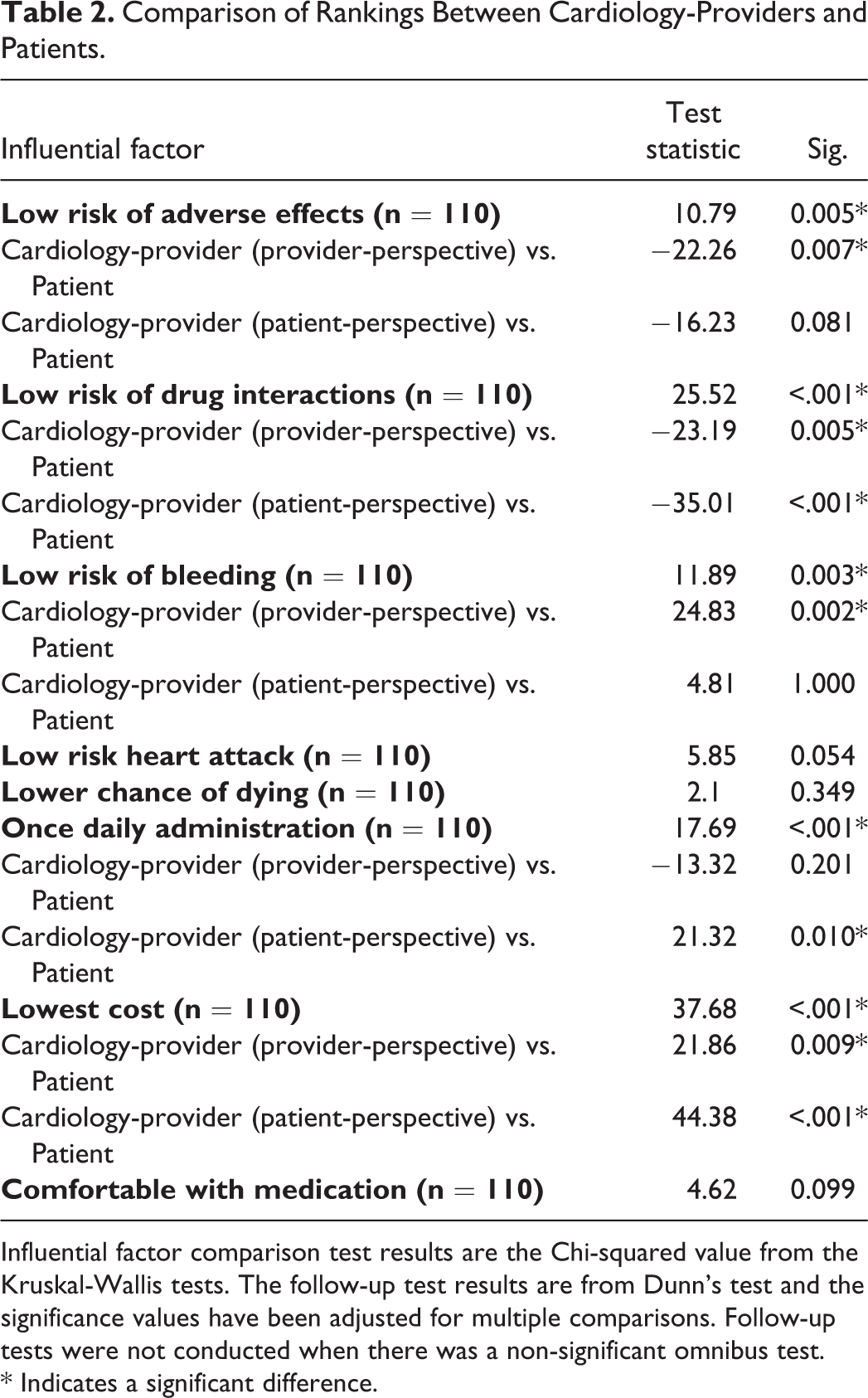
Influential factor comparison test results are the Chi-squared value from the Kruskal-Wallis tests. The follow-up test results are from Dunn’s test and the significance values have been adjusted for multiple comparisons. Follow-up tests were not conducted when there was a non-significant omnibus test.
* Indicates a significant difference.
Preference of P2Y12 Inhibitor Therapy
Evidence-based therapeutic preferences of cardiology-providers varied based on indication. For ACS with or without stent placement, most cardiology-providers preferred ticagrelor (78.13%) and selected efficacy (92.00%) as the primary reason for this preference. Greater variation was found for SIHD with stent placement, with preferences split between clopidogrel (60.00%) and ticagrelor (40.00%). Cardiology-providers that selected clopidogrel as their preferred medication, cited comfort/experience (56.25%), medication cost (22.22%), and safety (11.11%) as the primary reasons for preference. Cardiology-providers that selected ticagrelor as their preferred medication, cited efficacy (90.91%) as the primary reason for preference.
For cardiology-providers, the actual preference in clinical practice, based on self-reported prescribing patterns, was found to differ from the evidence-based therapeutic preference. For ACS with or without stent placement, though most cardiology-providers selected ticagrelor (78.13%) as their evidence-based therapeutic preference, clopidogrel (51.13%) was most frequently prescribed. For SIHD with stent placement, self-reported prescribing patterns more closely matched the evidence-based therapeutic preference. Clopidogrel was reportedly prescribed 62.50% of the time, ticagrelor 29.98%, and prasugrel 7.52%. Figure 2 summarizes findings of cardiology-provider medication preferences.
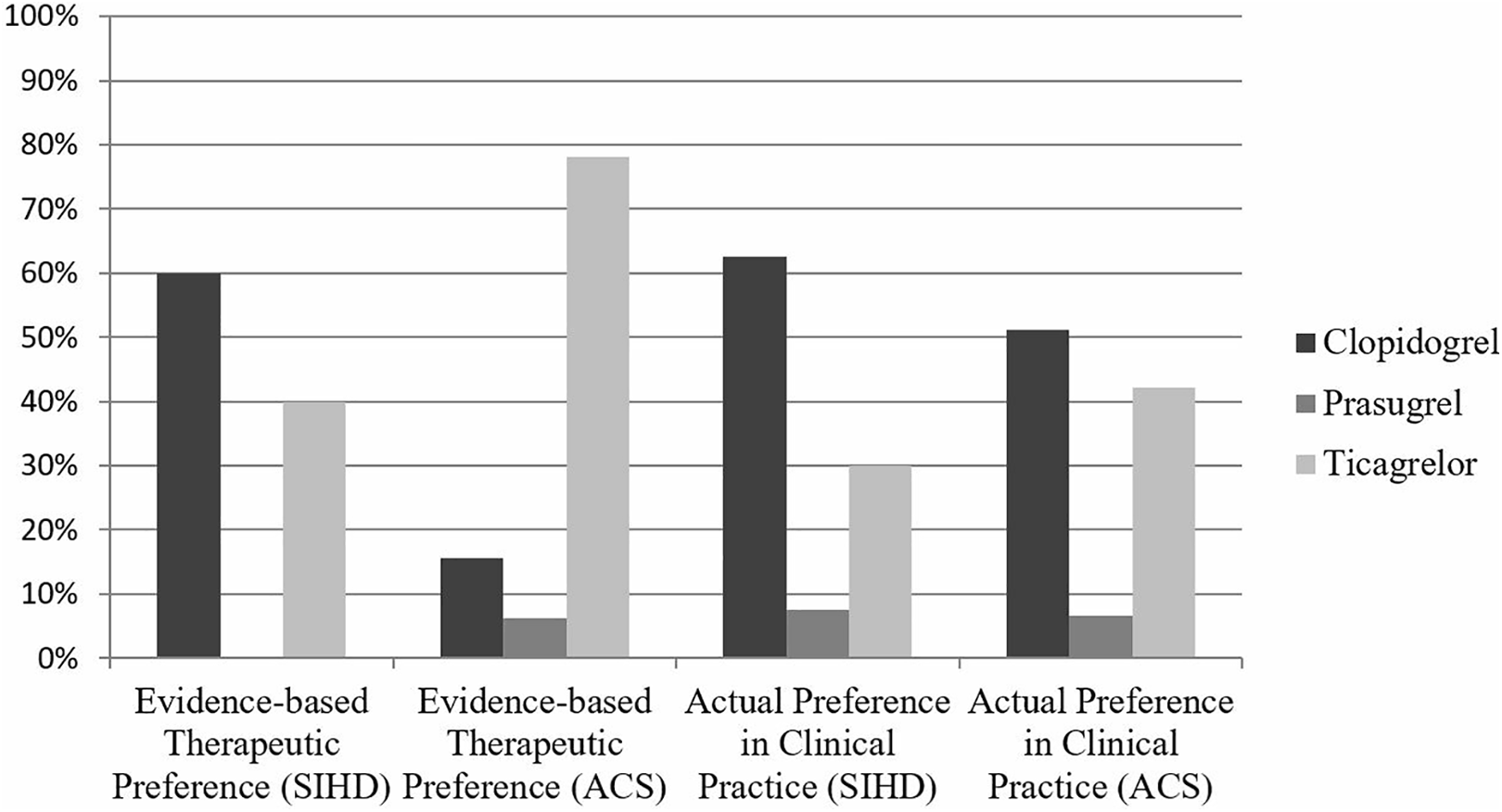
Cardiology-provider P2Y12 inhibitor preference percentages based on indication. SIHD notes responses by cardiology-providers for the indication of stable ischemic heart disease. ACS notes responses by cardiology-providers for the indication of acute coronary syndrome.
Regarding patient preference, most patients preferred “Medicine B” which matched attributes of ticagrelor, followed by “Medicine A” which matched attributes of clopidogrel (56% vs. 42.7%, respectively). Of patients currently prescribed clopidogrel, 46.9% of them preferred clopidogrel in the hypothetical scenario. Of patients currently prescribed ticagrelor, 85.7% of them preferred ticagrelor in the hypothetical scenario. None of the patients prescribed prasugrel selected it as their preferred P2Y12 inhibitor in the hypothetical scenario. Overall, there was a significant relationship between the medicine that the patients were taking and the medicine that the patients wanted to take (Χ2(n = 75) = 7.71, p = 0.021).
Financial Burden and Shared Decision-Making Experience
Based on pre-tax annual household income, 47.47% of patients reported earning less than $30,000, with 78.79% earning less than $75,000. Figure 3 depicts annual household income. Overall, 94.85% of patients reported having insurance coverage for their P2Y12 inhibitor. For clopidogrel, prasugrel, and ticagrelor individually, 94.4%, 100%, and 83.3% reported insurance coverage, respectively. The median cost of clopidogrel was lowest among the 3 medications at $6 per month. The median monthly costs of prasugrel and ticagrelor were $35 and $16.67, respectively. Most patients self-reported “affordable” monthly payments for all 3 P2Y12 inhibitors (87% clopidogrel, 85.7% prasugrel and 83.3% ticagrelor).
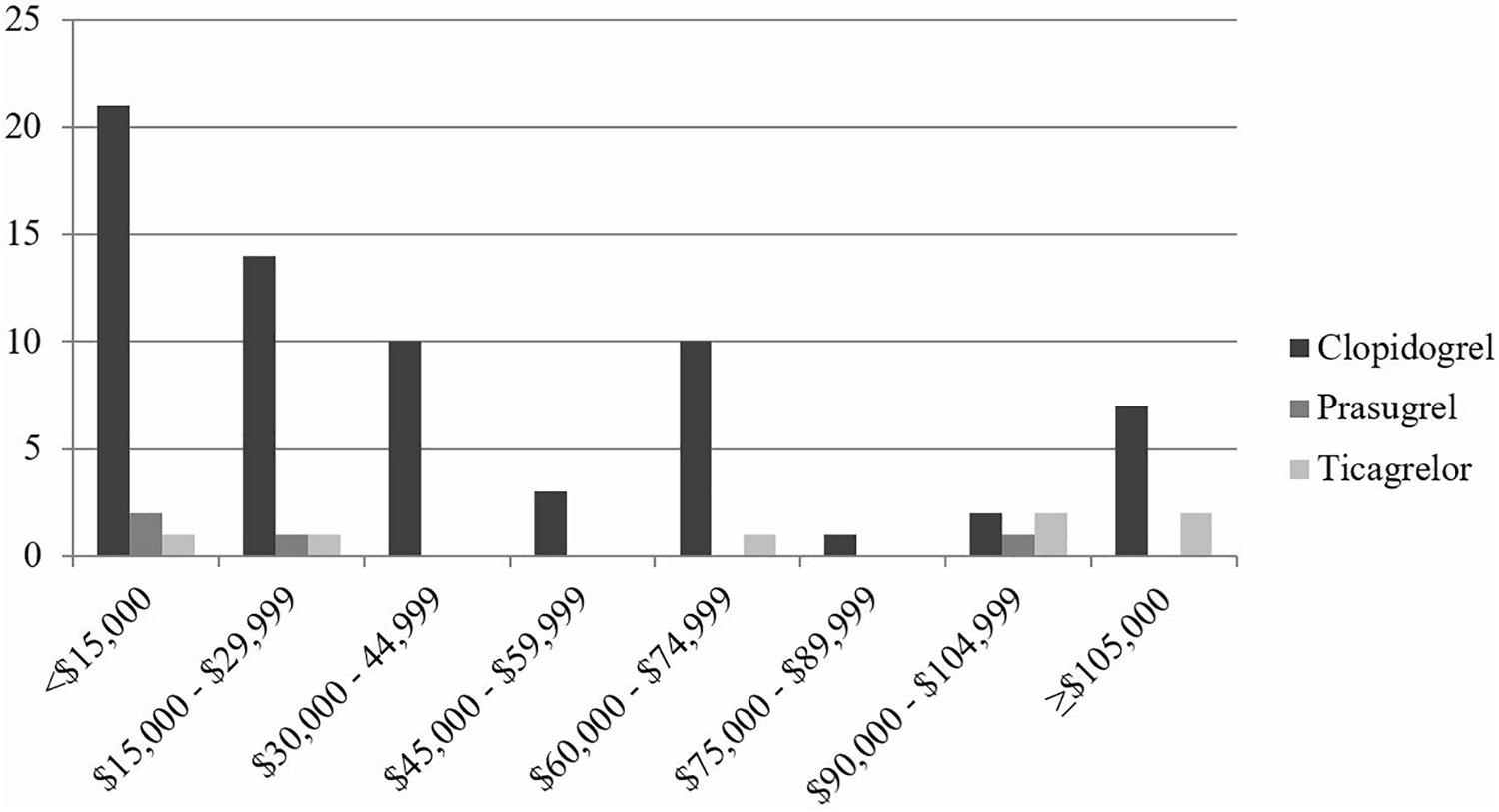
Count of participants by annual income among patients that reported taking clopidogrel, prasugrel, or Ticagrelor. Based on pre-tax annual household income. Majority of patient were prescribed clopidogrel (84.7%), among these patients, 94.4% reported insurance coverage of their medications.
Prior to being prescribed their current medication, 88.5% of patients were unaware that multiple P2Y12 inhibitors were available. During the appointment at which their current P2Y12 inhibitor was prescribed, 80.61% of patients discussed clopidogrel as a potential therapeutic option. Prasugrel and ticagrelor were discussed less frequently, with only 8.16% and 21.43% of patients reporting that these medications were discussed, respectively. Most patients (78.43%) reported that they did not help make the decision on which P2Y12 inhibitor would be prescribed.
Adverse Effects, Adherence, and Previous P2Y12 Inhibitor Use
When asked about adverse effects, 32 patients reported experiencing shortness of breath while receiving P2Y12 inhibitor therapy. Of these patients, 21 were receiving clopidogrel, 6 were receiving ticagrelor, 3 were receiving prasugrel, and 2 did not report which P2Y12 inhibitor they were receiving. Bleeding was experienced by 47 patients and most commonly resolved without medical attention (53.19%) or after a doctor’s office visit (8.51%) with only 8 patients required a visit to the emergency room. Of the patients that reported bleeding, 31 were receiving clopidogrel, 5 were receiving prasugrel, 4 were receiving ticagrelor, 4 did not report which P2Y12 inhibitor, and 3 reported receiving multiple P2Y12 inhibitors. When asked about medication adherence, 13 patients reported missing one or more doses. As shown in Figure 4 the most commonly reported reason for missing the dose was forgetting to take it, which was reported by 69.23%. Of the patients that reported missing medication doses, those receiving clopidogrel, ticagrelor, and prasugrel, were 84.62%, 7.69%, and 0%, respectively. One patient reported missing medication doses but did not report which P2Y12 inhibitor they were prescribed.
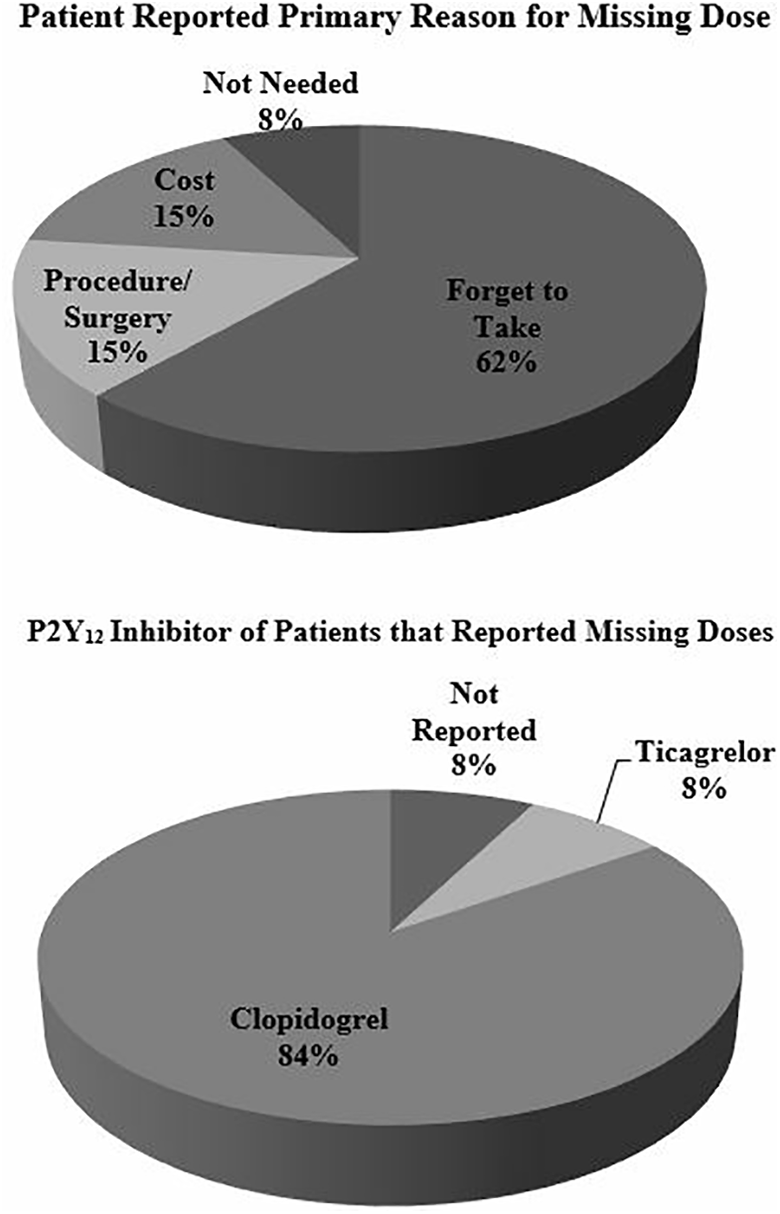
Adherence to P2Y12 inhibitor therapy. Thirteen patients reported missing one or more doses of their medication. Patients were asked to choose from a list of 9 potential reasons for missing a dose. Patients were given the option to select all that apply and then asked to narrow down their selection to a single primary reason.
Twelve patients reported taking a different P2Y12 inhibitor previously and provided information regarding previous therapy. Ticagrelor (9 patients) was most commonly reported, followed by prasugrel (2 patients) and clopidogrel (1 patient). For those previously receiving ticagrelor, the most frequent reason for switching was experiencing an adverse effect (4 patients). Other reasons included medication cost (1 patient), insurance coverage (1 patient), and transient ischemic attack (1 patient). Two patients did not provide a reason for switching therapy. For the 2 patients previously receiving prasugrel, primary reasons for switching therapy included cost and doctor recommendation. The patient previously receiving clopidogrel reported being unsure of the reason for switching therapy.
Discussion
The results of this study demonstrate significant differences in hierarchical rankings of the factors that influence selection of P2Y12 inhibitor therapy between cardiology-providers and patients. In assessing factors valued by patients, the most important factors were safety-related and efficacy-related. The factor most valued by patients was risk of drug interactions. In comparing P2Y12 inhibitors based on risk of drug interactions, the agent with the greatest risk is clopidogrel. Clopidogrel is inactive following administration and requires CYP2C19 mediated activation. 20 Given the need for activation, clopidogrel efficacy could potentially be reduced by genetic polymorphisms or drug interactions that inhibit CYP2C19. Many medications inhibit CYP2C19 including commonly used drug classes such as proton pump inhibitors. Studies assessing this interaction have found some measures of efficacy to be reduced, but no significant difference in rates of cardiovascular events. 21 Comparatively, prasugrel and ticagrelor have low risks of drug interactions. 20 Risk of adverse effects was the second most important factor to patients. In comparing P2Y12 inhibitors based on risk of adverse effects, ticagrelor has a greater number of associated adverse effects, including dyspnea, increased serum uric acid, and ventricular pauses. Of note, the adverse effects associated with ticagrelor have been shown to be reduced or eliminated with continued use. 5
Compared to patients, cardiology-providers (from a provider-perspective and/or patient-perspective) placed a higher value of importance on medication cost, risk of bleeding, and once daily administration. Prescribing rates could be explained by these provider values since clopidogrel is associated with comparatively lower risk of bleeding and administered once daily.4,5 Cardiology-providers ranked medication cost as the most important factor, when considering patient values, whereas patients ranked medication cost as least important. This marked one of the greatest contrasts between cardiology-provider and patient rankings. We also found that most patients considered their P2Y12 inhibitor to be affordable, regardless of the P2Y12 inhibitor prescribed. Clopidogrel is currently the least expensive P2Y12 inhibitor available. If cardiology-providers believe medication cost to be the most important factor to patients, it could explain why prescribing rates of clopidogrel exceed ticagrelor. During the SDM process, patient socioeconomic factors could be discussed to minimize the discrepancy between perceived and actual values.
The goal of this study was to provide information to enhance provider-patient communication and potentially allow cardiology-providers to more frequently prescribe medications that match their own values and the values of their patients. This study found that most cardiology-providers preferred ticagrelor following ACS but predominantly prescribed clopidogrel. As previously discussed, this could be attributed to cardiology-providers perceiving medication cost as most important to patients. Additionally, cardiology-providers and patients may not have discussed the factors of greatest value to patients. The extent of influence that patient education can have on prescribing patterns cannot be determined from our study. However, our study did find that after reading a hypothetical scenario providing education on key differences between P2Y12 inhibitors, patients preferentially selected ticagrelor. Though most patients had no prior knowledge of all 3 medications, a brief educational experience resulted in patient preferences that more closely aligned with cardiology-provider preferences.
There are many strategies for enhancing patient education of P2Y12 inhibitors in clinical practice. One strategy is incorporating the use of decision aids. Decision aids, which have been studied in multiple formats such as pamphlets, videos, or web-based tools, are designed to educate patients on risks and benefits when multiple therapeutic options are available. When compared to usual care, decision aids have been associated with patients feeling more knowledgeable about the available options, better informed, and clearer on what values matter most to them. 22 Decision aids have also been shown to increase the likelihood of patients and providers engaging in communication about the decision. 22 Incorporation of decision aids could increase patient-provider communication and facilitate SDM, which is associated with improvements in decision quality, patient knowledge, risk perception, and overall patient satisfaction.16-18 In this study, most patients did not participate in SDM and few patients discussed prasugrel or ticagrelor with their cardiology-provider. By using the data obtained in this study, cardiology-providers can engage in SDM with a better understanding of patient values.
Notable limitations of this study include the single-centered nature, making application to larger, more diverse populations of providers and patients unclear. Surveys being administered on paper format rather than electronically limited the ability to randomly order multiple response options. This may have led to order-effect bias as noted by the fact that the most influential factors for patients, risk of adverse effects and drug interactions, were also the first 2 influential factors listed. Additionally, the nature of administration of patient surveys via mail did not make supervision and response support possible, potentially contributing to missing or erroneous data points and low response rate. Our initial survey communication and planned follow up was designed to achieve an anticipated 50% response rate, though the actual rate was much lower (18%). 19 A contributing factor to low response rates could be that home addresses on file may not reflect current patient addresses. In addition, a health literacy assessment was not included in our patient survey, making it difficult to determine the level of patient understanding of survey questions. Patient level of understanding of influential factors is also difficult to determine, especially as it relates to cardiology-provider understanding. For example, when thinking about bleeding risk, a cardiology-provider may consider life-threatening bleeding while a patient may consider more familiar forms of bleeding like epistaxis. Lastly, as survey distribution began prior to the start of 2018, data published after this time would not be reflected in survey design or survey responses from cardiology-providers.
To our knowledge, this study is the first to examine factors influencing selection of P2Y12 inhibitors for cardiology-providers and patients. Opportunities for future research include repeating this assessment in a larger and more diverse patient population, possibly via an electronic format during office visits. Other opportunities include prospective studies examining whether incorporation of an SDM process or use of decision aids changes prescribing rates of P2Y12 inhibitors. These research opportunities may provide information to enhance provider-patient communication and allow cardiology-providers to more frequently prescribe their preferred P2Y12 inhibitor.
Conclusion
This study emphasizes the importance of recognizing the difference in values placed on drug therapy selection between patient and provider, thus highlighting the important role for shared decision making to occur in instances were multiple drug therapy options are available.
Supplemental Material
Supplemental Material, sj-pdf-1-jpp-10.1177_0897190020966174 - Factors Influencing Provider and Patient Choice of P2Y12 Inhibitor Therapy
Supplemental Material, sj-pdf-1-jpp-10.1177_0897190020966174 for Factors Influencing Provider and Patient Choice of P2Y12 Inhibitor Therapy by Rebekah M. Benitez, Kathleen A. Lusk, S. Hinan Ahmed, Stephanie A. Hartzell and Bethany A. Kalich in Journal of Pharmacy Practice
Footnotes
Author's Note
Stephanie A. Hartzell is now affiliated with College of Education, Concordia University Texas, Austin, TX, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. S. Hinan Ahmed discloses a modest relationship with the Speakers Bureau for AstraZeneca. Dr. Bethany A. Kalich discloses a modest relationship with the Speakers Bureau for Pfizer/Bristol-Myers Squibb and a significant relationship with the Speakers Bureau for Sanofi/Regeneron.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study provided by the Feik School of Pharmacy Competitive Intermural Scientific Research Award.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.