
Abstract
Introduction
Several studies have illustrated value in early patient contact following oral anticancer medication (OAM) initiation, particularly within the first 14 days of therapy, as adverse effects may lead to early discontinuation or poor adherence. Health-system specialty pharmacies (HSSPs) are optimally positioned to adopt this best practice through formalized protocols designed to identify and mitigate medication-related issues.
Objective
To outline an HSSP-led early check-in protocol for patients taking OAMs and to describe the subsequent interventions conducted by the HSSP team and their acceptance rate.
Results
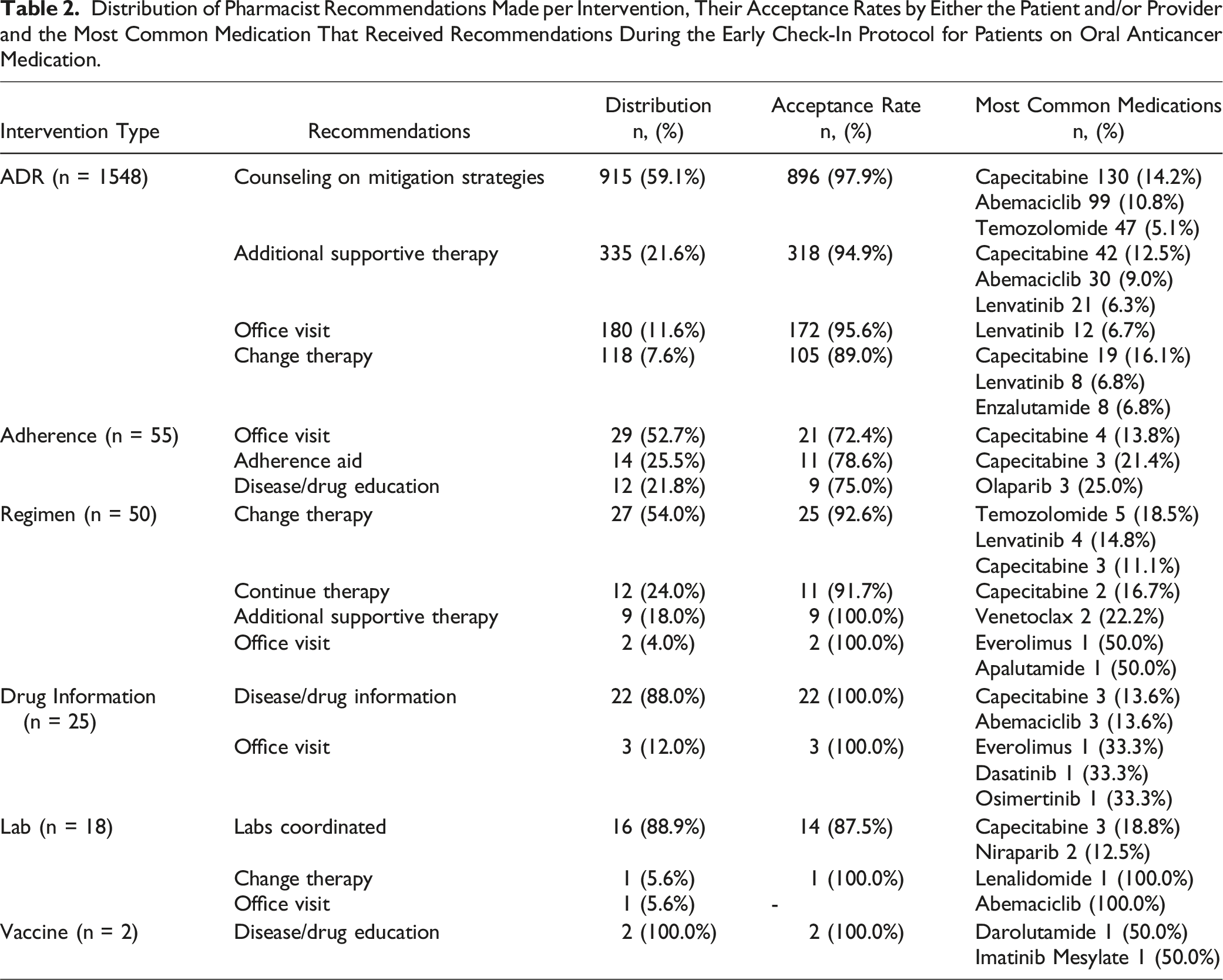
HSSPs enacted a protocol in January 2021 requiring oncology pharmacists - to contact patients within 14 days of OAM initiation, aiming to optimize adverse effect management, offer supportive care, address adherence, and provide education. To evaluate the impact of the early check-in protocol, we conducted a retrospective, multicenter, observational study across CPS’s health system clients from January 2022 to November 2023. HSSP pharmacists created 1698 interventions for 1184 patients from the early check-in. The cancer types most frequently associated with an intervention were breast (n = 431, 25.4%), gastrointestinal (n = 245, 14.4%), and prostate (n = 206, 12.1%). The most frequent intervention categories were adverse drug reactions (ADRs) (n = 1,548, 91.2%) and adherence (n = 55, 3.2%). Overall, 95.5% of pharmacist recommendations were accepted by patients and/or providers.
Conclusion
Implementing an early check-in protocol allows HSSP pharmacists to mitigate barriers to OAM adherence. This study emphasizes the importance of early check-in and illustrates the scope of the oncology pharmacist’s role by evaluating critically meaningful interventions and quantifying pharmacist recommendations and acceptance rate.
Keywords
Background
Oral anticancer medications (OAMs) have become a key component of many cancer regimens over the last two decades. 1 Although OAMs offer more convenience to patients compared to intravenous (IV) therapies, individuals prescribed an OAM may experience similar challenges to other oral medications, including poor adherence. As with many oral maintenance medications, OAMs rely on patients’ self-administration, often daily, whereas IV treatments are administered less often and require appointments with a healthcare provider. 2 Most often, this poor adherence results from patients taking medication less than the prescribed dose or frequency, with adherence rates to OAMs as low as 16% depending on the patient population, medication class, and cancer type. 3 Ensuring adherence to OAM regimens is crucial to achieving treatment goals, particularly in cases where treatment aims for curative outcomes. 4 One critical component of OAM adherence that can impact treatment outcomes is early discontinuation. Early discontinuation of an OAM leads to low therapeutic efficacy and an increased risk of relapse and mortality. 5 Factors contributing to early discontinuation include socioeconomic barriers, high medication costs, adverse drug reactions, and a lack of education about medications or disease states. 6 Given the prevalence of low adherence and early discontinuation among patients prescribed OAMs, comprehensive programs that target these issues may help improve overall treatment outcomes for these patients.
Pharmacists can play a crucial role in improving adherence to and decreasing early discontinuation of OAMs. Several pharmacist-led programs within community pharmacy settings have used various strategies to improve medication adherence, including comprehensive OAM education or medication management services that involve monitoring, follow-up, and collaboration with the patient and their other healthcare providers. 7 Medication access is another concern that can impact adherence and early discontinuation where pharmacists have a direct role. Many OAMs require insurance approval (i.e., prior authorizations), special storage and handling conditions, and considerable perpetual monitoring and coordination between providers, all of which lead to many being classified as specialty medications that must be obtained from a specialty pharmacy. 8 Health-system specialty pharmacies (HSSPs) are particularly well positioned to address these needs due to their patient- and provider-facing roles, which allow them a high level of involvement with direct patient care and access to electronic health records (EHRs). 9 Pharmacists in these settings specialize in assisting patients with insurance coverage, securing financial assistance to improve affordability, and ensuring safe and effective medication use. 10
HSSPs provide on-going clinical support for patients using evidence-based protocols, which affords them opportunities to improve adherence and reduce early discontinuation. One strategy that is not well-documented is the implementation of an early check-in protocol for patients who initiate an OAM. According to the Hematology/Oncology Pharmacy Association (HOPA), standardized protocols should include a proactive follow up to conduct initial monitoring after OAM initiation. 11 Therefore, the objectives of this study were 1) to outline an HSSP-led early check-in protocol for managing patients taking OAMs and 2) to describe the interventions conducted by the HSSP team and their acceptance rate.
Early Check-In Protocol
The early check-in protocol was implemented at CPS Solutions, LLC (CPS) in January 2021. Though some HSSPs embedded within CPS’s client health systems were already performing a check-in early in the course of OAM therapy, the oncology subcommittee at CPS decided to formalize and standardize this process across all sites. This standardization would allow for the patient management system to facilitate the scheduling of these check-ins and differentiate these touchpoints and associated interventions from other counseling sessions with patients. Thus, based on the HOPA best practice recommendations, 11 the subcommittee developed a standardized protocol by enabling the patient management system to differentiate this touchpoint, thereby facilitating scheduling, streamlining counseling, and creating a framework for clinical pharmacists to proactively check-in with patients within 14 days of OAM initiation. This protocol also provided structured guidance for those HSSP pharmacists that had not received advanced training in oncology pharmacy.
Prior to the early check-in protocol, existing processes involved establishing medication access (including insurance coverage and financial assistance) and providing the patient with a comprehensive counseling session before therapy initiation. In this session, HSSP pharmacists would review crucial information about the medication. Following OAM initiation, the updated protocol required pharmacists to conduct a follow-up within 14 days to assess common challenges in the early stages of treatment. (Figure 1) This included evaluations for medication schedule, proper administration, side effects, and any potential access challenges. Overview of the Early Check-In Protocol. This figure shows the general workflow for the early check-in protocol. After enactment of this protocol, pharmacists checked in with patients within 14 days of OAM initiation to evaluate for side effects, barriers to adherence, the need for supportive care, and if the patients had any questions for the pharmacist. If any of these were present, they documented these interventions in the patient management system by assigning an intervention type and recommendation outcome. If none were present, pharmacists documented the check-in with no additional interventions. In both cases, pharmacists then resumed normal monitoring and follow-up per protocols.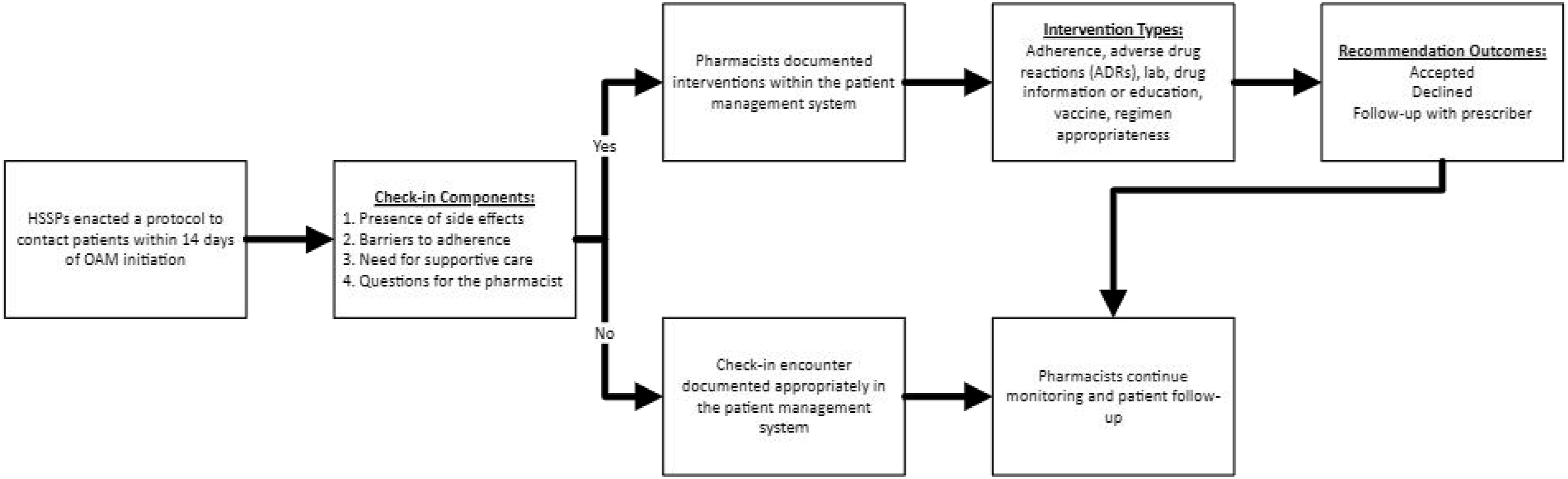
Each encounter was documented within a proprietary patient management system. 9 This platform, along with the EHR, facilitates the collection of clinical outcomes and quality measures. If the patient experienced a medication-related issue requiring intervention, the pharmacist documented the intervention in the patient management system. Each intervention was categorized based on the relevant medication-related issue identified, including: adverse drug reaction (ADR), adherence, regimen appropriateness (e.g., changes to the regimen), drug information, laboratory values, and vaccines. Depending on the intervention, pharmacists documented their actions taken or recommendations made to resolve the medication issue, including: 1) conduct patient counseling (e.g., on side effect mitigation strategies or medication adherence), 2) recommend a new therapy, change in therapy (e.g., dose changes or holding doses), or to continue a therapy, 3) recommend an office visit with a medical provider, 4) coordinate a laboratory test, or 5) provide general education on medication and disease state. For the severity of ADRs, pharmacists managed cases based on the Common Terminology Criteria for Adverse Events (CTCAE), issued by the U.S Department of Health and Human Services. 12 Pharmacists also have access to clinical resources that are compiled by the oncology subcommittee and are specific to the different types of cancer and medications used. Ultimately, clinical judgment, combined with guidance from these resources, was used to make recommendations and determine when to escalate care to the provider. After the pharmacist made their recommendations to either the patient or provider, they recorded the recommendation as accepted, declined, or required follow-up with the prescriber. For example, during an early check-in call with a patient diagnosed with breast cancer who was prescribed capecitabine, the patient reported tingling in their fingertips and soles of their feet. The pharmacist then created an intervention documenting their discussion with the patient on mitigation strategies, and they notified the oncologist about the ADR for further evaluation. The pharmacist documented the recommendation as requiring a follow-up appointment with the provider.
Following the initial check-in interaction with patients, pharmacists continued to monitor and follow up with them throughout the course of their OAM treatment based on existing protocols for each cancer type. In addition to disease-specific measures, a chart review was conducted for all patients 6 months after OAM initiation, with annual reassessments conducted at or after one year of therapy. The 6-month chart review assessed medication-related issues such as therapy interruptions or delays, non-therapeutic laboratory trends, or side effects. The annual reassessment was always interactive and included: updating the patient profile (e.g., medication list, allergies, and comorbid conditions), reviewing adherence, reviewing the dose and administration, assessing side effects, and assessing therapy appropriateness and effectiveness.
Evaluation of the Early Check-In Protocol
Methods
To evaluate the impact of the early check-in protocol, a retrospective, multicenter, observational study was conducted across CPS-managed HSSPs from January 2022 to November 2023. Interventions associated with OAMs were included if they were for a patient 18 years of age or older who was enrolled in clinical HSSP services. Interventions were excluded if they were for an OAM without a cancer diagnosis or had incomplete categorization or information.
All intervention recommendations were documented and categorized as one of the following: recommendation accepted, recommendation declined or recommendation required follow-up with the provider. Patients and/or providers determined the outcomes of an intervention recommendation by either accepting or declining it. Data was collected from the proprietary specialty pharmacy patient management system. Descriptive statistics were used for all measures, with data presented as counts (n) and percentages.
Results
Most Common Medications Associated With an Intervention During the Early Check-In Protocol for the Most Common Cancer Type.
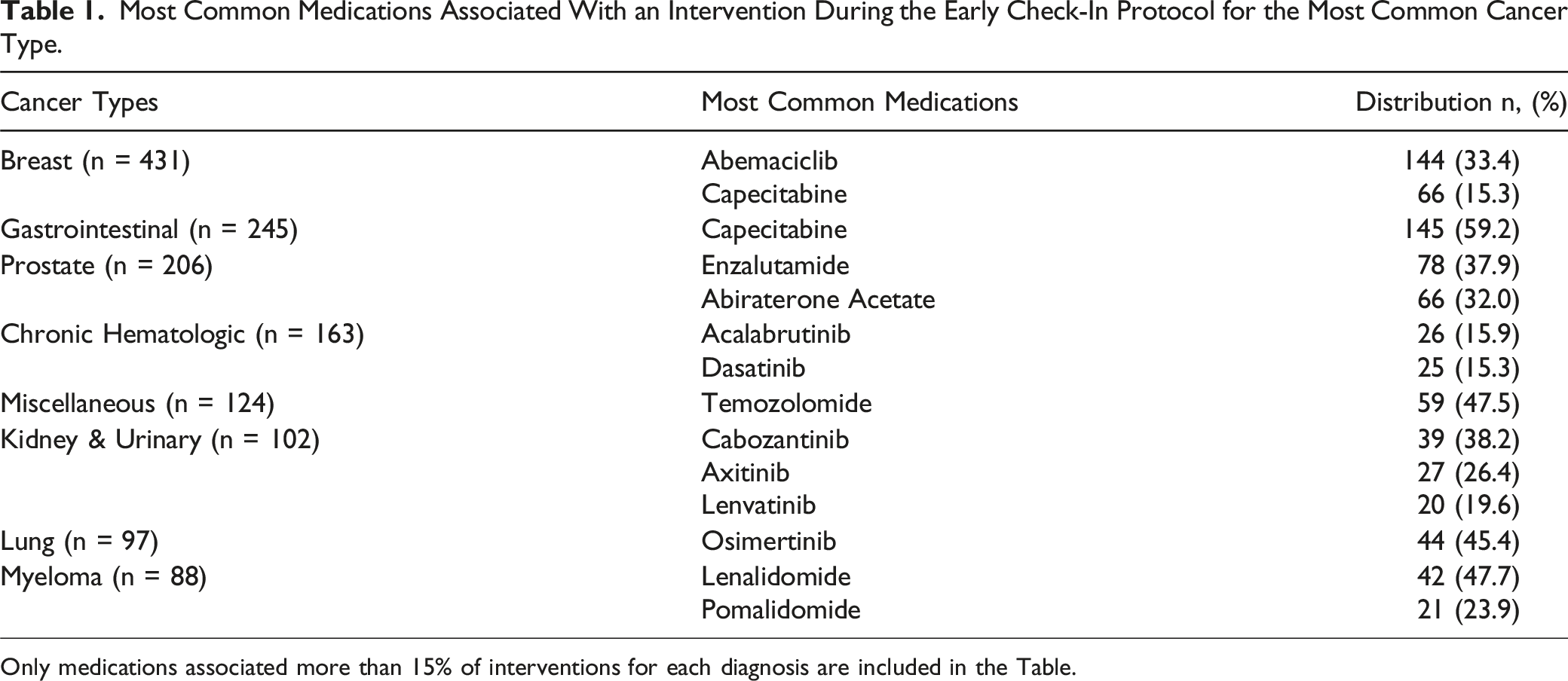
Only medications associated more than 15% of interventions for each diagnosis are included in the Table.
Distribution of Pharmacist Recommendations Made per Intervention, Their Acceptance Rates by Either the Patient and/or Provider and the Most Common Medication That Received Recommendations During the Early Check-In Protocol for Patients on Oral Anticancer Medication.
Clinical Implications
Early discontinuation and poor adherence to OAMs are challenges in cancer treatment that affect therapeutic efficacy and patient outcomes. This study introduces a novel approach to address these challenges through the implementation of an early check-in protocol within the HSSP setting. Implementation of an early check-in protocol allowed HSSP pharmacists to intervene early and address OAM-related issues. Additionally, this study highlights the value of HSSP pharmacists in optimizing the management of patients prescribed OAMs.
During the study period, the most common intervention conducted by pharmacists was related to ADRs. This is not surprising since OAMs have a high incidence of ADRs, which often cause moderate to severe symptoms in patients. 13 Studies indicate that approximately 70% of ADRs occur within the first 10 days of OAM initiation, often leading to early discontinuation and poor adherence. 14 The check-in protocol implemented in this study facilitated early identification of ADRs, allowing pharmacists to promptly intervene. After identifying ADRs, pharmacists provided counseling on mitigation strategies, enabling patients to increase the likelihood that they could remain on their prescribed therapy. They also provided additional supportive therapy or recommended a hold or change of therapy (e.g., adjusting dosage and/or frequency) by collaborating with prescribers to mitigate ADRs.
The disease states most commonly implicated in pharmacist-generated interventions were breast, prostate, and colorectal cancer, which aligns with the most common diagnoses seen in larger datasets such as the Surveillance, Epidemiology, and End Results Program (SEER) from the National Cancer Institute. 15 As patients live longer with certain cancer types, such as breast and prostate (5-year relative survival of 91.2% and 97.5%, respectively), it is inevitable that additional therapies may be added, which may have contributed to the frequency with which these disease states were seen during this initiative. The recommended modalities in treating cancers also vary depending on origin tissue. Lung cancer, for example, has limited OAM options as approved oral agents are almost exclusively targeted therapies, requiring evidence of specific mutations. Earlier-line drug therapies are predominantly intravenous, which are not generally managed at the HSSP level.16,17 In contrast, treatment guidelines for myeloma utilize OAM – primarily oral immunomodulators (e.g., lenalidomide and pomalidomide) – at every step. 18 Interestingly, despite the frequency with which pharmacists at all sites were intervening on lenalidomide and pomalidomide, only one client health system had access to dispense this medication. Our pharmacists still manage these patients based on evidence-based clinical protocols, and these interventions indicate that the pharmacists are still able to help patients work through early complications and offer clinical support for potentially unaddressed toxicities. Along similar volume trends, some medications would be more likely to be used than others, rendering them with more potential for intervention by volume. OAMs with multiple indications, such as capecitabine and lenvatinib, may see more interventions simply because of the higher volume associated with multi-use therapies. Additionally, many agents are known to carry more toxicity risk than others, which inherently renders them more likely to warrant intervention. Toxicities with cancer treatments are well documented, and clinical pharmacists, who are routinely speaking with patients, are well equipped to both predict some of these toxicities based on literature and patient-specific factors as well as mitigate or escalate problems as they arise. For example, knowing that hypertension can lead to therapy interruption with lenvatinib, pharmacists in clinics can help patients obtain a home blood pressure monitor and encourage patients to self-report measures. Then, a pharmacist proactively contacting a high-risk patient early in therapy can recommend an appropriate antihypertensive medication to the provider and ultimately alleviates the burden on the patient while optimizing patient care. Another area where pharmacists can be impactful is in patients with low health literacy. For patients new to cyclical chemotherapy, complex instructions such as “twice daily on days 1-5 and 8-12 of a 28 day cycle” as seen with tifluradine/tipiracil 19 may be overwhelming. Assessing patient understanding and supporting patients through their early days of treatment are critical to improving outcomes by ensuring optimal medication use.
The early check-in protocol presented in this study can serve as a framework for other institutions aiming to reduce ADRs and improve therapy outcomes. Based on these results and previous studies,10,20,21 HSSP pharmacists are in a unique position to play an important role in the oncology care team. In contrast to other pharmacy settings, HSSP teams are embedded within the clinic with direct access to patient’s EHRs and healthcare providers. This proximity enables them to actively manage OAMs and ensure therapy is precisely tailored to meet each patient’s individual needs. The high acceptance rate of pharmacists’ recommendations further supports the value of the HSSP model in oncology clinics. Collaboration between HSSP teams and other healthcare team members has been shown to improve patient outcomes in various disease states such as multiple sclerosis, 9 rheumatoid arthritis, 22 and HIV.23,24
This study has some limitations that should be considered. Since some site pharmacists were already performing check-ins prior to standardization of the check-in protocol, the ability to evaluate the impact on adherence and discontinuation rate using statistical analysis was limited. Additionally, we were unable to evaluate the long-term effect of the early check-in by measuring discontinuation rates, adherence, and persistence at 6 months or 1 year after therapy initiation. Future studies should focus on evaluating the impact of such programs using traditional measures of adherence and persistence and utilizing statistical analysis at different time periods Additionally, as a retrospective study, there may be biases in the data collection process (e.g., interventions with missing or incomplete data were not included in the analysis), which can impact the generalizability of the results.
Conclusions
The implementation of an early check-in protocol allowed HSSP teams to address OAM-related issues. This protocol placed pharmacists in an optimal position to perform patient-centered interventions aimed at increasing adherence, reducing early discontinuation rates, and improving patient outcomes. Additionally, this study highlights the positive impact of the protocol on the patient-pharmacist relationship and the collaborative dynamic of HSSPs within the oncology team.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.