
Abstract
Hypertension often remains inadequately controlled despite pharmacological therapy, indicating the influence of multidimensional factors on blood pressure regulation. Psychological and spiritual processes contribute to stress regulation and adaptive coping; however, quantitative synthesis of psychospiritual interventions within holistic nursing remains limited. This meta-analysis evaluated the effects of psychospiritual interventions on systolic blood pressure (SBP) and diastolic blood pressure (DBP) in adults with hypertension. A systematic review and meta-analysis of randomized controlled trials was conducted following PRISMA 2020 guidelines using databases covering 2000–2025. Twelve studies were included in the qualitative synthesis, with six studies analyzed for SBP and five for DBP. Psychospiritual interventions were associated with a significant reduction in SBP (SMD = −0.91; 95% CI: −1.54 to −0.29; p = .004), but not DBP (SMD = −0.20; 95% CI: −0.77 to 0.36; p = .48). Findings support psychospiritual interventions as complementary non-pharmacological strategies consistent with holistic nursing approaches to hypertension management.
Keywords
Background
Hypertension is one of the most prevalent chronic conditions globally and a major contributor to cardiovascular morbidity and mortality (Lu et al., 2025). Although pharmacological therapy and lifestyle modification have become the standard of care, long-term blood pressure control remains suboptimal (Edwards et al., 2022). In clinical nursing practice, nurses frequently encounter patients who have received adequate treatment yet continue to experience fluctuating or uncontrolled blood pressure (Edwards et al., 2022). This persistent instability indicates that hypertension is not solely a physiological disorder but a complex condition shaped by dynamic interactions among biological, psychological, social, and spiritual processes (Lasco et al., 2022; Magnani, 2023).
Within the holistic nursing paradigm, health is conceptualized as a multidimensional process in which physiological stability is interconnected with emotional balance, meaning-making capacity, relational experience, and spiritual well-being (Papathanasiou et al., 2013; Sassen, 2023). Holistic nursing emphasizes the unity of body, mind, and spirit as a guiding principle for understanding health and illness experiences (Papathanasiou et al., 2013; Sassen, 2023). From this perspective, blood pressure regulation may reflect not only cardiovascular functioning but also an individual's adaptive capacity to regulate stress, construct meaning in illness, and maintain internal coherence (Cilli et al., 2022; King, 2023; Sassen, 2023).
A growing body of evidence indicates that psychological conditions, such as chronic stress, anxiety, depression, and existential distress, play an important role in the pathophysiology and regulation of blood pressure (Chauvet-Gelinier & Bonin, 2017; Silverman et al., 2019). Sustained psychological stress is associated with increased sympathetic nervous system activity and dysregulation of the hypothalamic–pituitary–adrenal axis, which ultimately compromises blood pressure stability (Oei et al., 2025; Spruill, 2010). In addition to their physiological effects, these psychological conditions influence patient engagement in self-care behaviors and adherence to long-term treatment (Cilli et al., 2022; Rouhi et al., 2022). Blood pressure can therefore be understood as a biopsychophysiological indicator reflecting interactions among emotional experience, behavioral adaptation, and cardiovascular regulation (King, 2023; Sassen, 2023).
In addition to psychological influences, spiritual well-being and existential coping are increasingly recognized as important factors in chronic illness adaptation (Ghorbani et al., 2021; Papathanasiou et al., 2013). Spiritual distress, loss of meaning, and existential uncertainty may increase emotional burden and weaken coping capacity, potentially influencing physiological regulation (Cilli et al., 2022; King, 2023). Conversely, spiritual resources such as connectedness, transcendence, acceptance, and meaning-making are associated with improved emotional regulation and resilience (Ghorbani et al., 2021; Southard, 2020). These findings support the holistic nursing assumption that healing involves restoration of balance across multiple dimensions of human experience rather than solely symptom reduction.
Psychospiritual interventions have emerged as integrative non-pharmacological approaches addressing psychological regulation and spiritual well-being simultaneously. These interventions include mindfulness, meditation, contemplative prayer, yoga, breathing techniques, spiritual reflection, and meaning-centered therapeutic approaches (Alkhabbaz et al., 2022; Kurniawati & Sari, 2024). In this study, psychospiritual interventions are defined as structured therapeutic strategies intentionally integrating cognitive, emotional, and spiritual processes to enhance self-awareness, promote adaptive meaning-making, regulate stress responses, and foster inner balance (Ghorbani et al., 2021; Sassen, 2023).
Evidence suggests that psychospiritual practices may influence cardiovascular regulation through modulation of autonomic nervous system activity, reduction of stress hormone secretion, improved emotional regulation, and strengthened adaptive coping responses (Alabdulgader, 2012; Chen et al., 2024; Nozdrachev et al., 2022). More recent evidence suggests that these benefits are particularly pronounced among individuals with hypertension accompanied by psychological distress (Babak et al., 2022; Loucks et al., 2019; Schneider et al., 2021). Randomized controlled trials have shown that mindfulness- and meditation-based interventions can significantly reduce systolic and diastolic blood pressure (DBP), especially in individuals with early-stage hypertension or elevated blood pressure (Chen et al., 2024). Interventions specifically designed for blood pressure regulation have reported reductions of approximately 5–7 mmHg in systolic blood pressure (SBP), largely mediated by improvements in stress regulation and attentional control (Thiyagarajan et al., 2015; Wolff et al., 2016). These mechanisms demonstrate how psychospiritual interventions influence physiological stability through interconnected biopsychosocial pathways aligned with holistic nursing principles.
Holistic nursing positions nurses as facilitators of healing through therapeutic presence, relational engagement, and interventions that respect patients’ values, beliefs, and meaning systems (Scharfman & Kubanick, 2025). Psychospiritual interventions may therefore represent practical expressions of holistic nursing competencies, including intentional presence, compassionate awareness, and support for patients’ meaning-making processes during chronic illness management (Ghorbani et al., 2021; Sassen, 2023; Scharfman & Kubanick, 2025).
However, findings from individual studies demonstrate considerable variation in the type of psychospiritual interventions employed, intervention duration, cultural context, and the magnitude of effects on blood pressure (Chen et al., 2024; Sukarmin et al., 2023). Previous systematic reviews have tended to examine these interventions separately according to specific techniques or modalities, without integrating them within a nursing practice framework (Jarelnape et al., 2024). Such fragmentation limits conceptual clarity and reduces the applicability of evidence for holistic nursing practice, which emphasizes integration rather than separation of human dimensions (Papathanasiou et al., 2013; Southard, 2020).
Within holistic nursing, individuals are understood as integrated beings in which biological, psychological, social, and spiritual dimensions interact dynamically to influence health outcomes and healing processes (Papathanasiou et al., 2013; Sassen, 2023). Nurses play a central role as facilitators of healing through therapeutic presence, mindful relationships, and interventions that honor patients’ values and beliefs (Scharfman & Kubanick, 2025). Holistic nursing, therefore emphasizes not only symptom reduction but also the restoration of harmony across dimensions of human functioning, recognizing that physiological stability may emerge from improved emotional regulation, spiritual well-being, and adaptive meaning-making processes (Helming et al., 2020). Therefore, a comprehensive synthesis of quantitative evidence is needed to clarify the magnitude and consistency of psychospiritual intervention effects on systolic and DBP while situating these findings within holistic nursing science.
This meta-analysis not only estimates pooled effect sizes of psychospiritual interventions on blood pressure outcomes but also integrates these findings within a holistic nursing theoretical framework. By examining psychospiritual interventions as multidimensional strategies influencing biopsychosocial regulation, this study strengthens the theoretical and practical foundation of holistic nursing interventions aimed at supporting whole-person healing in individuals with hypertension.
Methods
Study Design
This study was a systematic review and meta-analysis evaluating the effectiveness of psychospiritual interventions on blood pressure control in adults with hypertension or elevated blood pressure. The review was designed to synthesize quantitative evidence while conceptually situating psychospiritual interventions within a holistic nursing perspective that recognizes the interconnection of biological, psychological, and spiritual dimensions of health.
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251271811) to enhance methodological transparency and reduce the risk of selective reporting bias.
Search Strategy and Study Selection
A systematic literature search was conducted in the ProQuest, EBSCO, and Scopus databases, covering the period from 2000 to 2025. The search period was selected to capture contemporary developments in psychospiritual and integrative health interventions relevant to holistic nursing practice.
Search terms were developed using Boolean operators and combinations of controlled vocabulary and keywords, including: (“hypertension” OR “blood pressure”) AND (“psychospiritual” OR “mindfulness” OR “meditation” OR “yoga” OR “breathing exercise” OR “spiritual care” OR “spiritual intervention”). Manual searches of reference lists from eligible articles were also conducted to identify additional relevant studies.
Studies were included if they: (1) employed a randomized controlled trial design, (2) involved adults (≥18 years) with hypertension or elevated blood pressure, (3) evaluated a psychospiritual intervention and (4) reported post-intervention systolic and/or DBP outcomes.
Studies were excluded if they: (1) used non-quantitative designs, (2) lacked a comparison group, (3) did not report post-intervention blood pressure outcomes, (4) reported outcomes only as change scores without extractable post-intervention mean values, and (5) focused on outcomes unrelated to blood pressure. Study screening and eligibility assessment were conducted systematically based on predefined inclusion criteria.
Psychospiritual interventions were operationally defined as structured therapeutic approaches integrating cognitive, emotional, and spiritual processes to support stress regulation, meaning-making, and adaptive coping responses.
Data Extraction and Risk of Bias Assessment
Data were extracted systematically, including study characteristics, participant demographics, type and duration of the intervention, comparison conditions, and post-intervention mean values and standard deviations for blood pressure outcomes. Risk of bias was assessed using the Cochrane Risk of Bias Tool, covering domains of random sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting. Each domain was categorized as low risk, unclear risk, or high risk of bias. Discrepancies in assessment were resolved through discussion to ensure consistency in methodological appraisal.
Statistical Analysis
Meta-analysis was conducted using a random-effects model to account for expected clinical and methodological heterogeneity among studies, including differences in intervention type, duration, and population characteristics. The random-effects approach assumes that the true intervention effect may vary across studies due to contextual and implementation differences, which is consistent with the diversity of psychospiritual practices across cultural and clinical settings.
Effect sizes were expressed as standardized mean differences (SMDs) with 95% confidence intervals to accommodate variation in reporting formats across studies. Statistical heterogeneity was assessed using the I2 statistic, with values of 25% indicating low heterogeneity, 50% indicating moderate heterogeneity, 75% indicating high heterogeneity (Teixeira et al., 2023). Interpretation of heterogeneity considered both statistical magnitude and clinical variability across psychospiritual modalities, intervention duration, and participant characteristics.
Results
Study Selection
Study selection was conducted in accordance with the PRISMA 2020 guidelines. A total of 426 records were identified through electronic database searches (Scopus, ProQuest, and EBSCO). After removal of 28 duplicates, records were screened based on title and abstract according to publication year and topic relevance, resulting in 45 articles eligible for full-text assessment. Full-text assessment was performed for 22 articles, of which 16 were excluded for the following reasons: outcomes reported only as change scores without post-intervention values, qualitative study design, or absence of blood pressure outcomes. Ultimately, 12 randomized controlled trials were included in the qualitative synthesis, and six studies provided sufficient data for inclusion in the quantitative meta-analysis of blood pressure outcomes. The study selection process is summarized in Figure 1.
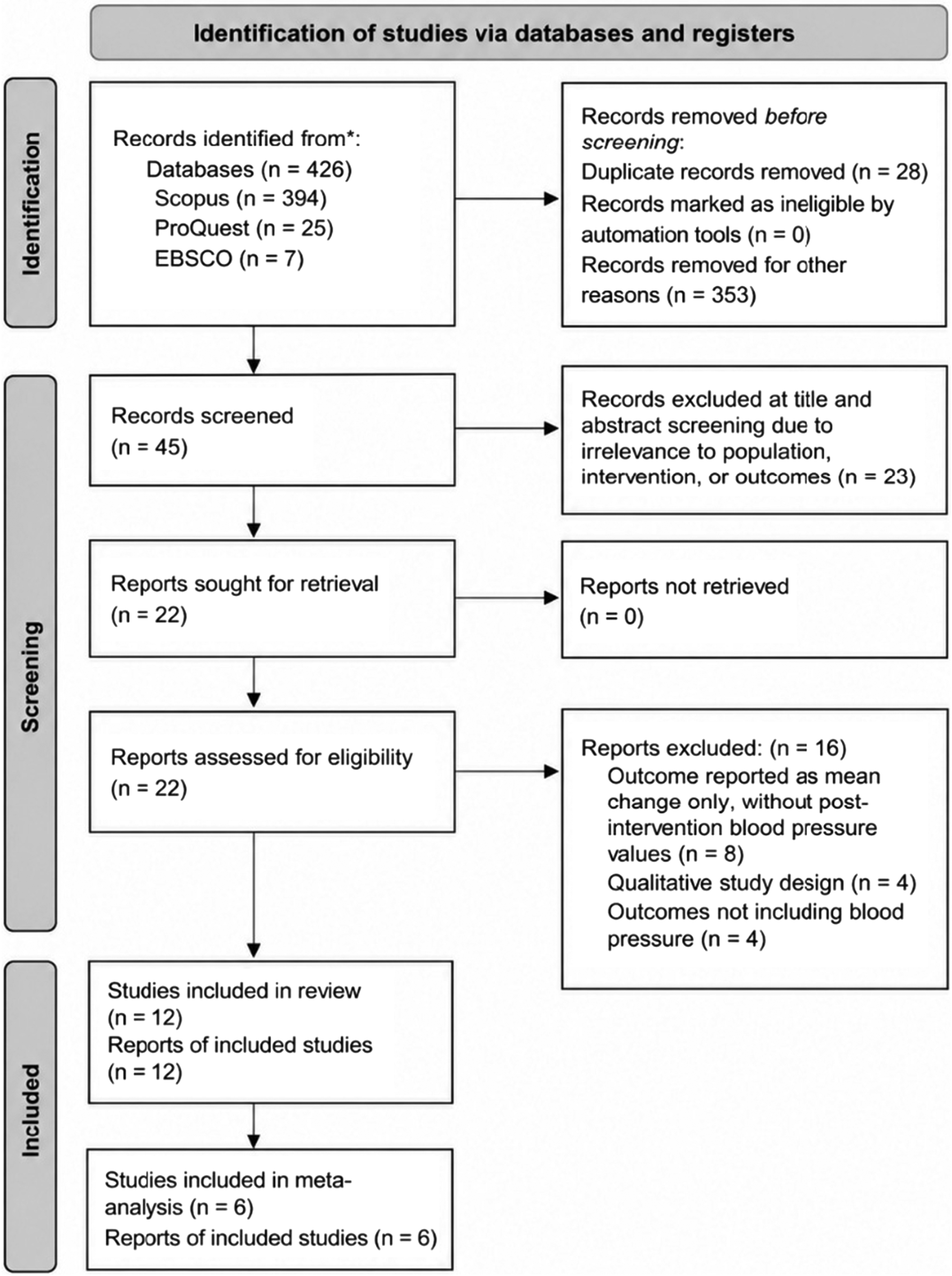
PRISMA 2020 flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of randomized controlled trials evaluating psycho spiritual interventions for blood pressure control in adults with hypertension.
Study Characteristics
A total of 12 randomized controlled trials (RCTs) examining psychospiritual interventions for blood pressure control in adults with hypertension or elevated blood pressure were included in the qualitative synthesis. Of these, six studies provided sufficient data for the meta-analysis of SBP, and five studies provided data for DBP. The studies were conducted across multiple countries and involved adult populations ranging from prehypertension to stage I‒II hypertension. Detailed characteristics of the included studies are presented in Table 1.
The psychospiritual interventions evaluated included yoga, mindfulness, meditation, mindfulness-based stress reduction (MBSR), pranayama breathing techniques, and spiritually oriented reflective practices, with intervention durations ranging from 4 to 13 weeks. Comparison groups generally consisted of usual care, health education, lifestyle modification, or waitlist control. The diversity of psychospiritual modalities reflects variation in cultural context and therapeutic approach, supporting the need for synthesis using a random-effects model to capture variability in intervention effects. Primary outcomes were systolic and DBP, measured using standard assessment procedures.
Effects on SBP
Figure 2 presents the pooled effects of psychospiritual interventions on SBP based on six randomized controlled trials.
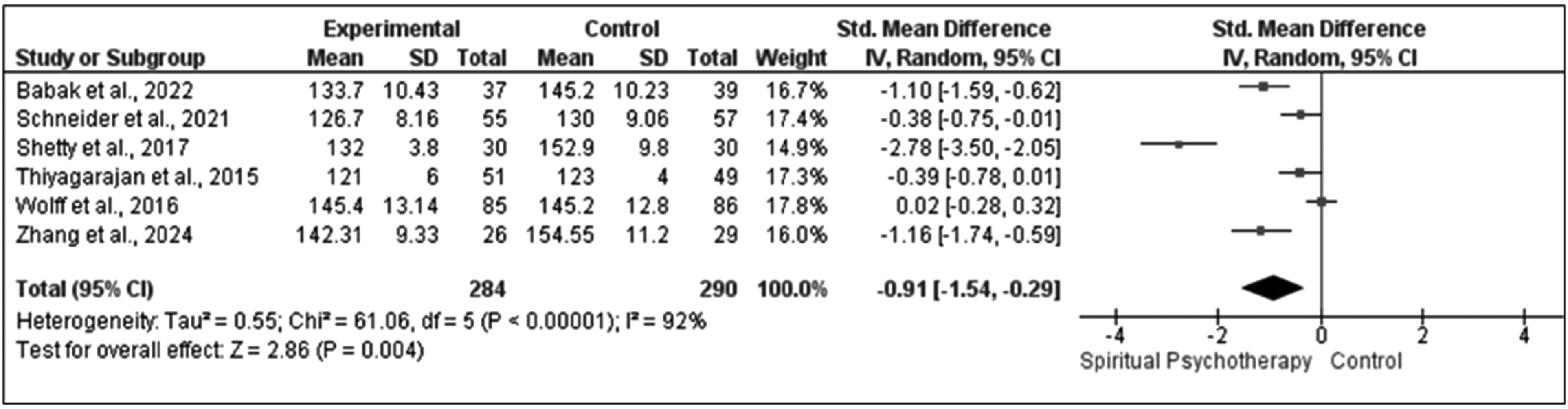
Forest plot of the effects of psychospiritual interventions compared with control conditions on systolic blood pressure in adults with hypertension.
Using a random-effects model, psychospiritual interventions were associated with a statistically significant reduction in SBP compared with control conditions (SMD = −0.91; 95% CI: −1.54 to −0.29; p = .004). The pooled effect size indicates a large intervention effect, suggesting clinically meaningful improvement in blood pressure regulation. Substantial heterogeneity was observed (I2 = 92%). The high heterogeneity reflects variability in intervention modalities (e.g., mindfulness, meditation, and yoga), duration, delivery format, and participant characteristics. Differences in cultural context and degree of spiritual integration may further contribute to variability in intervention effectiveness, consistent with the contextual nature of psychospiritual care within holistic nursing practice.
Effects on DBP
Five randomized controlled trials were included in the meta-analysis of DBP. Psychospiritual interventions were not associated with a statistically significant reduction in DBP compared with control conditions (SMD = −0.20; 95% CI: −0.77 to 0.36; p = .48), with substantial heterogeneity observed (I2 = 90%). The smaller and non-significant pooled effect suggests that DBP may respond less consistently to psychospiritual interventions across studies. Variability in intervention intensity, duration, baseline cardiovascular risk, and responsiveness of DBP to behavioral interventions may contribute to this finding.
Figures 2 and 3 demonstrate a significant pooled effect favoring psychospiritual interventions for SBP, whereas the pooled effect for DBP was not statistically significant. These findings suggest that psychospiritual interventions may influence cardiovascular regulation, particularly SBP, which is more strongly associated with stress-related autonomic activation. The observed heterogeneity highlights the importance of contextual and implementation factors when integrating psychospiritual approaches into holistic nursing care. A summary of pooled effect sizes is presented in Table 2.
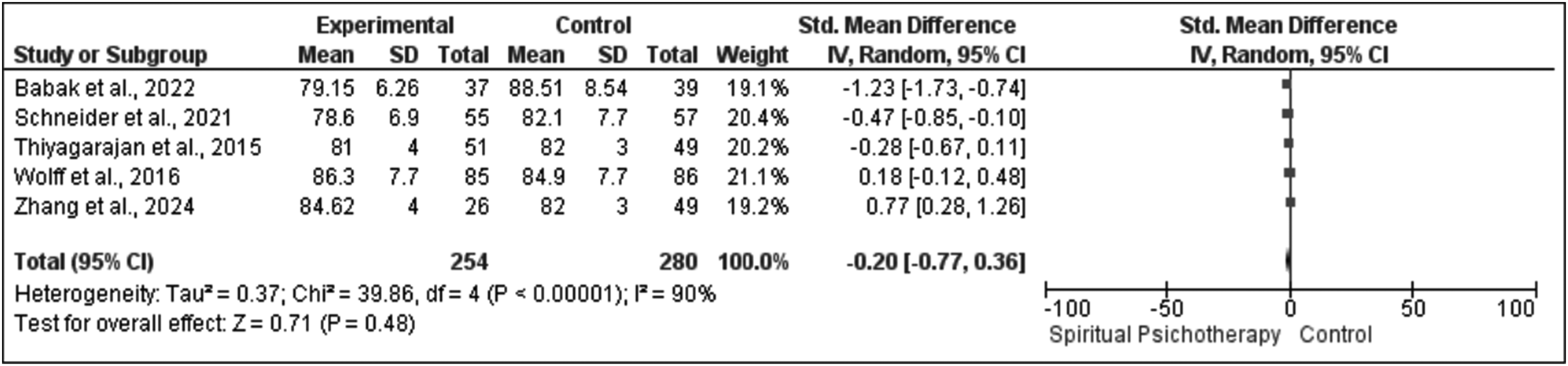
Forest plot of the effects of psychospiritual interventions on diastolic blood pressure (DBP) in adults with hypertension.
Characteristics of Included Studies (n = 12).
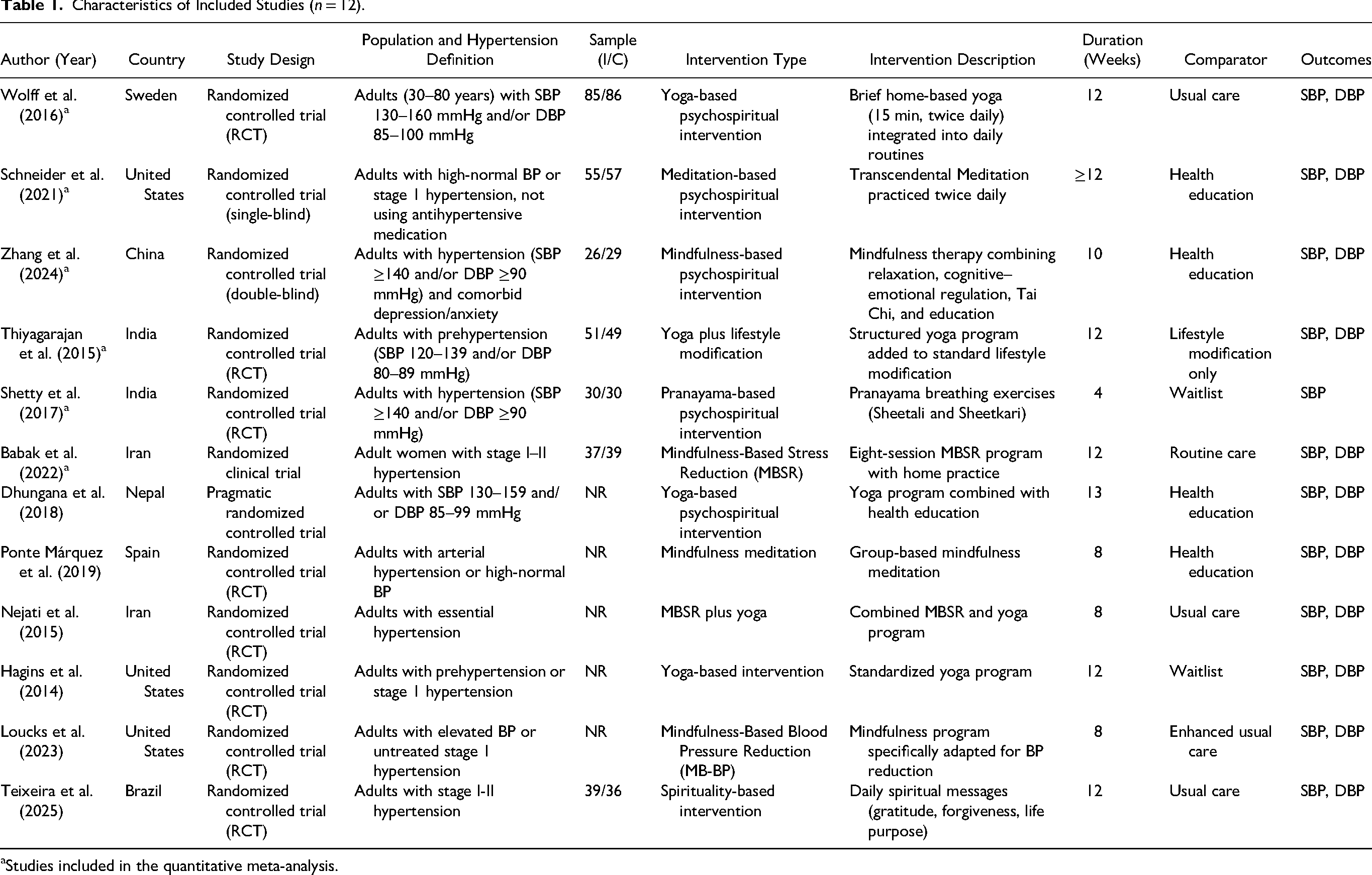
Studies included in the quantitative meta-analysis.
Summary of Meta-Analysis Results Using Standardized Mean Differences.

Studies Not Included in the Quantitative Synthesis
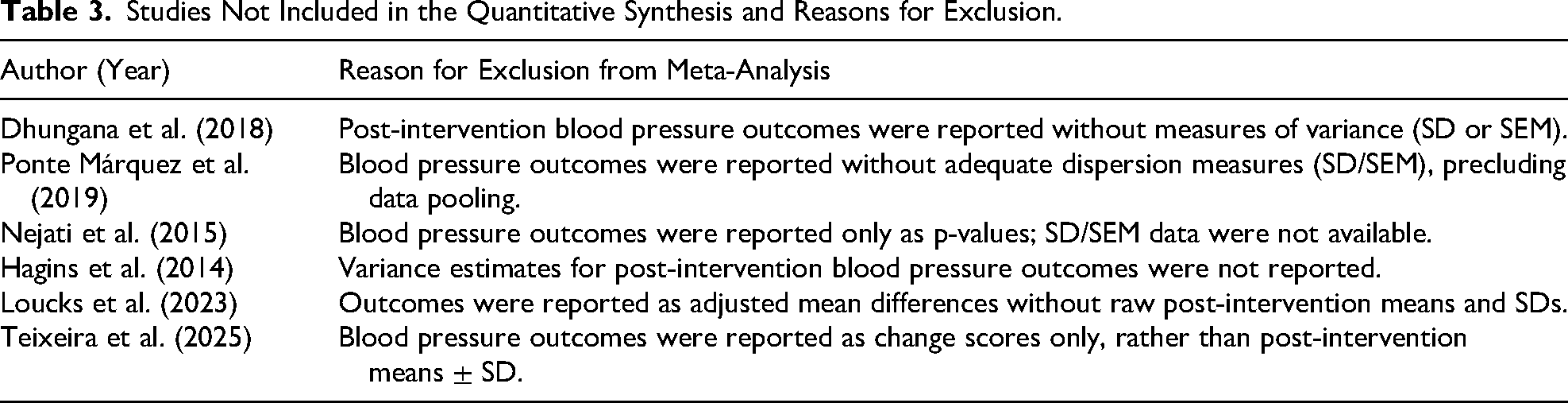
Several studies that met the inclusion criteria were not included in the meta-analysis because they did not report measures of variance (e.g., standard deviations), reported outcomes only as change scores, or employed non-quantitative study designs. Although not statistically pooled, these studies contribute contextual evidence regarding intervention characteristics and patient experiences relevant to psychospiritual care within holistic nursing practice. Table 3 summarizes the excluded studies and reasons for exclusion.
Studies Not Included in the Quantitative Synthesis and Reasons for Exclusion.
Risk of Bias
Overall, the included studies demonstrated a low risk of bias in the domain of random sequence generation. Blinding of participants and personnel was judged to be at high risk of bias due to the nature of psychospiritual interventions, which preclude blinding. Other domains, such as blinding of outcome assessors and allocation concealment, varied across studies and were, in some cases, rated as having an unclear risk of bias. The risk of selective reporting was generally low. The overall risk of bias assessment is presented in Figure 4.
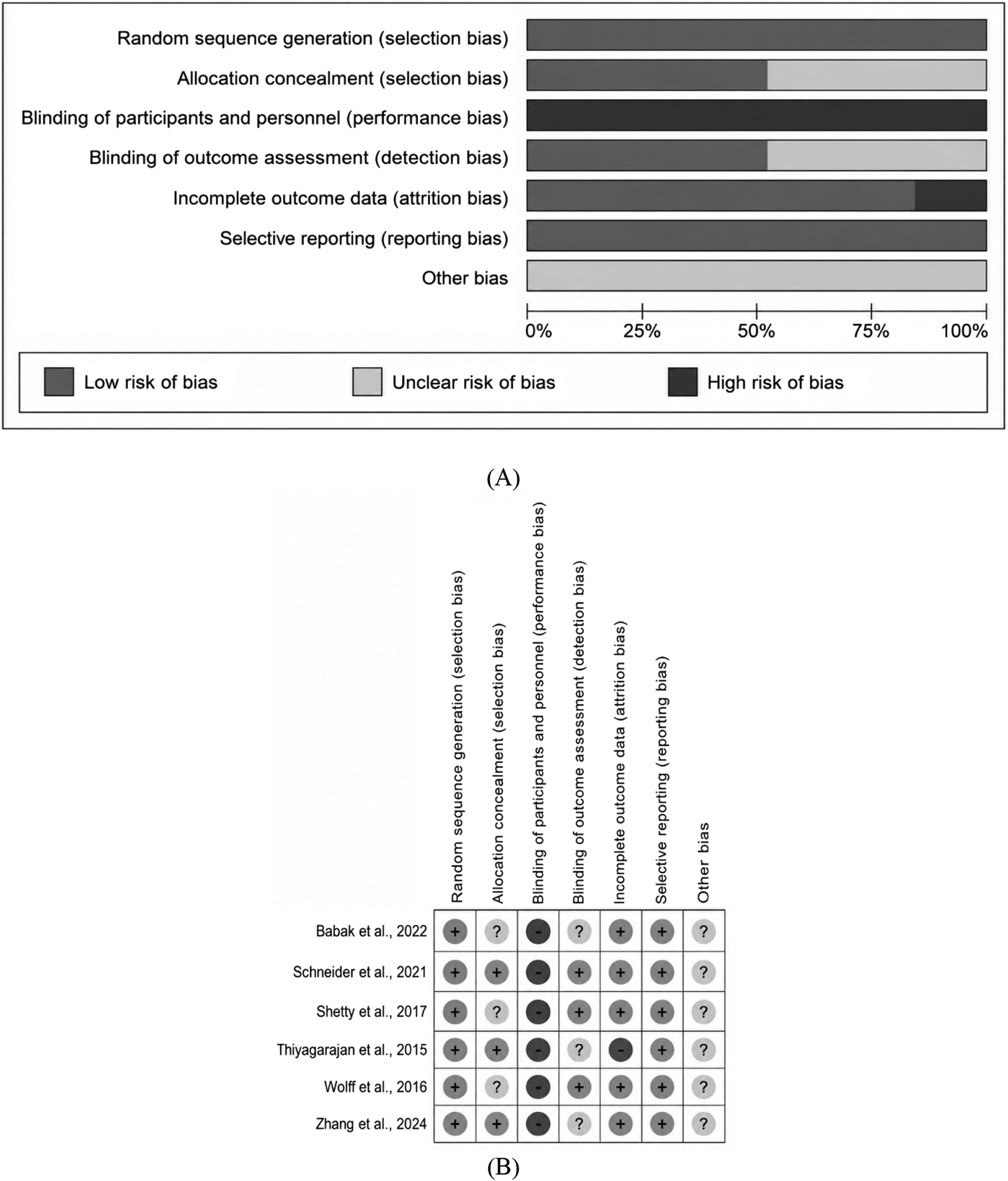
Summary of risk of bias assessment of the included studies using the cochrane risk of bias tool, presented as overall proportions (A) and study-level assessments (B).
Discussion
The findings of this meta-analysis indicate that psychospiritual interventions were associated with a significant reduction in SBP, demonstrating a clinically meaningful effect despite substantial heterogeneity across studies. While the pooled effect for DBP did not reach statistical significance, the direction of effect remained favorable, suggesting a potential physiological benefit that may vary depending on intervention characteristics and participant context.
From a holistic nursing perspective, blood pressure may be understood not only as a physiological parameter but also as a sensitive indicator of the dynamic interaction among biological, psychological, and spiritual processes. Reductions in SBP may reflect improved stress adaptation and meaning-centered coping processes across interconnected mind–body–spirit dimensions (Sassen, 2023).
Psychospiritual interventions such as mindfulness, meditation, yoga, and spiritually reflective practices appear to operate through mechanisms involving autonomic nervous system modulation, improved emotional regulation, and enhanced self-awareness (Babak et al., 2022; Chen et al., 2024). These processes support integration of emotional and spiritual experiences, which are central to holistic nursing approaches to chronic illness adaptation (Ghorbani et al., 2021).
The present meta-analysis is consistent with and supported by prior research demonstrating that psychospiritual interventions, including mindfulness, meditation, yoga, and breathing practices, reduce blood pressure through psychological and emotional regulation. Studies by Schneider et al. (2021) and Loucks et al. (2023) reported significant reductions in blood pressure following mindfulness-based interventions among individuals with early-stage hypertension, primarily mediated by reductions in psychological stress and enhanced self-awareness. Similarly, yoga- and pranayama-based interventions have been associated with improvements in blood pressure regulation through modulation of the autonomic nervous system and enhanced emotional regulation (Hagins et al., 2014; Thiyagarajan et al., 2015; Wolff et al., 2016).
The significant pooled effect observed for SBP suggests that psychospiritual interventions may primarily influence cardiovascular outcomes through stress-responsive physiological pathways, as SBP is particularly sensitive to sympathetic nervous system activation (King, 2023; Teixeira et al., 2025). In contrast, the smaller and non-significant pooled effect observed for DBP indicates greater variability in DBP responsiveness, potentially related to differences in intervention duration, intensity, and baseline cardiovascular risk.
Substantial heterogeneity was observed across studies, likely reflecting variability in intervention modality, duration, frequency, participant characteristics, and cultural context. Differences in the degree of spiritual engagement, therapeutic guidance, and integration of meaning-centered processes may also contribute to variability in outcomes (Ghorbani et al., 2021; Sassen, 2023; Scharfman & Kubanick, 2025). Despite this variability, the overall pattern suggests shared underlying mechanisms across diverse psychospiritual modalities, including improved stress adaptation and integrative coping responses during chronic illness (Ghorbani et al., 2021; King, 2023).
Chronic psychological distress has been consistently associated with dysregulation of the hypothalamic–pituitary–adrenal axis and sustained sympathetic activation, contributing to elevated blood pressure and reduced treatment adherence (King, 2023; Oei et al., 2025). Psychospiritual interventions may therefore be understood as integrative therapeutic processes that facilitate reinterpretation of illness-related stressors, strengthen adaptive regulation, and support physiological stability (Cilli et al., 2022; Ghorbani et al., 2021; King, 2023; Sassen, 2023).
By synthesizing evidence across diverse psychospiritual modalities, this meta-analysis demonstrates that beneficial effects are not limited to specific techniques but appear to reflect shared integrative mechanisms aligned with holistic nursing principles (Ghorbani et al., 2021; Sassen, 2023). This finding strengthens the conceptual linkage between psychospiritual care and measurable physiological outcomes in hypertension management.
Implications for Holistic Nursing Practice
From a holistic nursing perspective, these findings highlight the importance of understanding blood pressure regulation as influenced by psychological and spiritual well-being in addition to physiological processes. Effective hypertension management may benefit from integrating psychospiritual approaches that support stress adaptation, reflective awareness, and meaning-centered coping.
Nurses play a central role in identifying psychological distress, spiritual concerns, and meaning-related challenges that may influence patients’ ability to maintain blood pressure stability (Babak et al., 2022; Wolff et al., 2017). Through therapeutic presence and relational engagement, nurses can facilitate supportive environments that encourage reflective awareness, emotional balance, and connection with personal values and beliefs.
In clinical practice, psychospiritual care may be implemented through simple approaches such as mindful breathing, guided reflection, meditation, or culturally meaningful spiritual activities aligned with patients’ preferences. Integration of psychospiritual approaches into routine hypertension care may enhance patient engagement, promote self-regulation, and support sustainable lifestyle adaptation. Implementation of such interventions requires consideration of feasibility, cultural sensitivity, and appropriate training to ensure that psychospiritual care is delivered ethically and respectfully within diverse clinical contexts.
Overall, the findings of this meta-analysis provide empirical support for incorporating psychospiritual interventions into holistic nursing practice. By bridging physiological, psychological, and spiritual dimensions of care, nurses contribute to comprehensive hypertension management that supports whole-person healing.
These findings reinforce the role of nurses as facilitators of integrative care that promotes resilience, adaptive coping, and sustained engagement in chronic disease management.
Conclusion
This meta-analysis indicates that psychospiritual interventions are associated with a significant reduction in SBP among adults with hypertension or elevated blood pressure, while the pooled effect on DBP was not statistically significant. These findings suggest that psychospiritual approaches may influence cardiovascular regulation primarily through mechanisms related to stress adaptation, emotional regulation, and enhanced self-regulatory capacity.
The results support the role of psychological and spiritual factors as relevant components influencing blood pressure control, consistent with holistic nursing perspectives that emphasize the interconnectedness of biological, psychological, and spiritual dimensions of health. By synthesizing evidence across diverse intervention modalities, this meta-analysis supports positioning psychospiritual interventions as complementary, non-pharmacological strategies within comprehensive hypertension management.
Within holistic nursing practice, psychospiritual interventions may represent practical approaches to support patient engagement, adaptive coping, and sustainable self-management. Nurses are strategically positioned to facilitate these interventions through therapeutic presence, relational care, and culturally responsive support aligned with patients’ values and beliefs. Integration of psychospiritual care may strengthen person-centered hypertension management and promote long-term whole-person well-being.
Footnotes
Ethical Approval
Ethical approval was not required because this study used secondary data derived from previously published research and did not involve direct interaction with human participants or access to identifiable personal data.
Consent to Participate
Not applicable. This study did not involve the recruitment of participants or the collection of primary data from human subjects.
Consent for Publication
Not applicable. This manuscript does not contain any individual-level data, images, or other identifiable personal information requiring informed consent for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
Not applicable. All data analyzed in this study were obtained from previously published articles and are available within the cited literature.