
Abstract
Oral and maxillofacial surgery in veterinary medicine carries the risk of severe hemorrhage due to the great vascular supply of the head. Temporary hemostasis can be achieved with the application of pressure or hemostatic agents, but more definitive treatment may be needed to ensure bleeding will not resume once the patient is awake and normotensive. 1,2 Actively bleeding vessels encountered during maxillofacial surgery may be inaccessible, and vessels may recoil into bone, sometimes preventing definitive ligation. These scenarios may require ligation of the common carotid artery. 1 The purpose of this paper is to describe how to perform ligation of the common carotid artery in a step-by-step fashion. Both temporary and permanent ligation techniques are described.
Oral and maxillofacial surgery in veterinary medicine carries the risk of severe hemorrhage due to the great vascular supply of the head. Temporary hemostasis can be achieved with the application of pressure or hemostatic agents, but more definitive treatment may be needed to ensure bleeding will not resume once the patient is awake and normotensive. 1,2 Blood loss can be minimized and hemostasis successfully achieved if the source of bleeding is located, identified, and ligated in a timely manner. 1,2 However, a unique aspect of maxillofacial surgery is that actively bleeding vessels may be inaccessible at points in the surgery, and vessels may recoil into bone, sometimes preventing definitive ligation. These scenarios may require ligation of the common carotid artery. 1
When considering which vessel to ligate, a brief review of the vascular anatomy is necessary. The blood supply of the head and neck originates from the brachiocephalic trunk, 1 of the 2 major vessels arising from the aortic arch. 3 The brachiocephalic trunk continues cranially, giving off the left and right common carotid arteries, among other branches. The common carotid arteries course cranially within the carotid sheaths (along with the vagosympathetic nerve and internal jugular vein) and eventually terminate as the internal and external carotid arteries. The main blood supply to either half of the head is considered to be the external carotid artery, and it continues to branch into numerous smaller vessels commonly encountered in oral and maxillofacial surgery. 3 The common carotid artery is more easily located and isolated than the external carotid artery in the ventral neck of the canine and feline patient, making it a better choice for ligation or temporary occlusion. 3,4
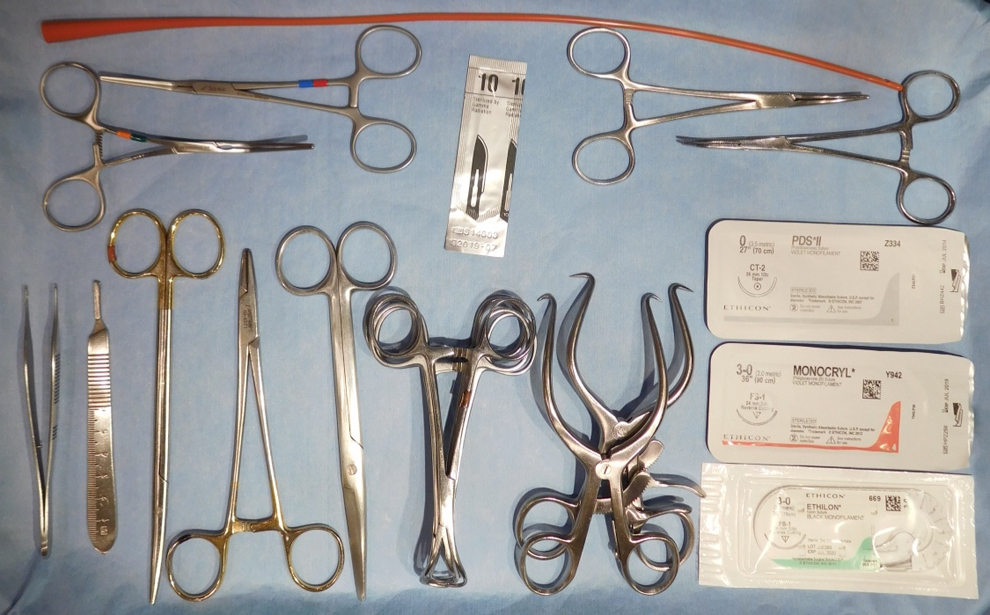
Photograph showing the surgical supplies needed to perform the procedure: size 8F or 10F red rubber catheter, a 2 to 4 mosquito hemostats, #10 scalpel blade, tissue forceps, scalpel blade handle, Metzenbaum scissors, needle holders, Mayo scissors, 4 towel clamps, 2 Gelpi retractors, 0 polydioxanone, b 3-0 poliglecaprone 25, c 3-0 nylon d .
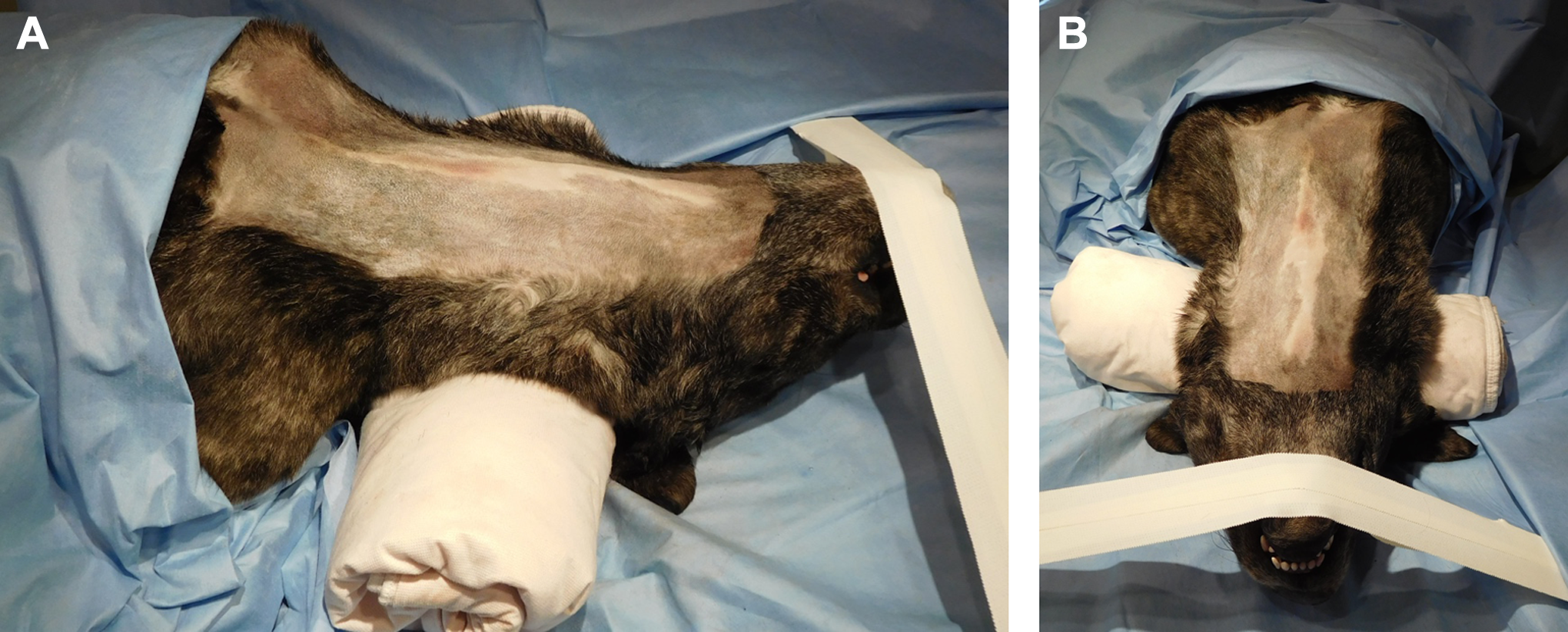
Photograph showing a canine cadaver placed in dorsal recumbency for common carotid artery ligation using a ventral approach. The head is extended and the forelimbs are pulled caudally. Lateral (A) and ventral (B) views. Note the optional towel placed to elevate the neck.
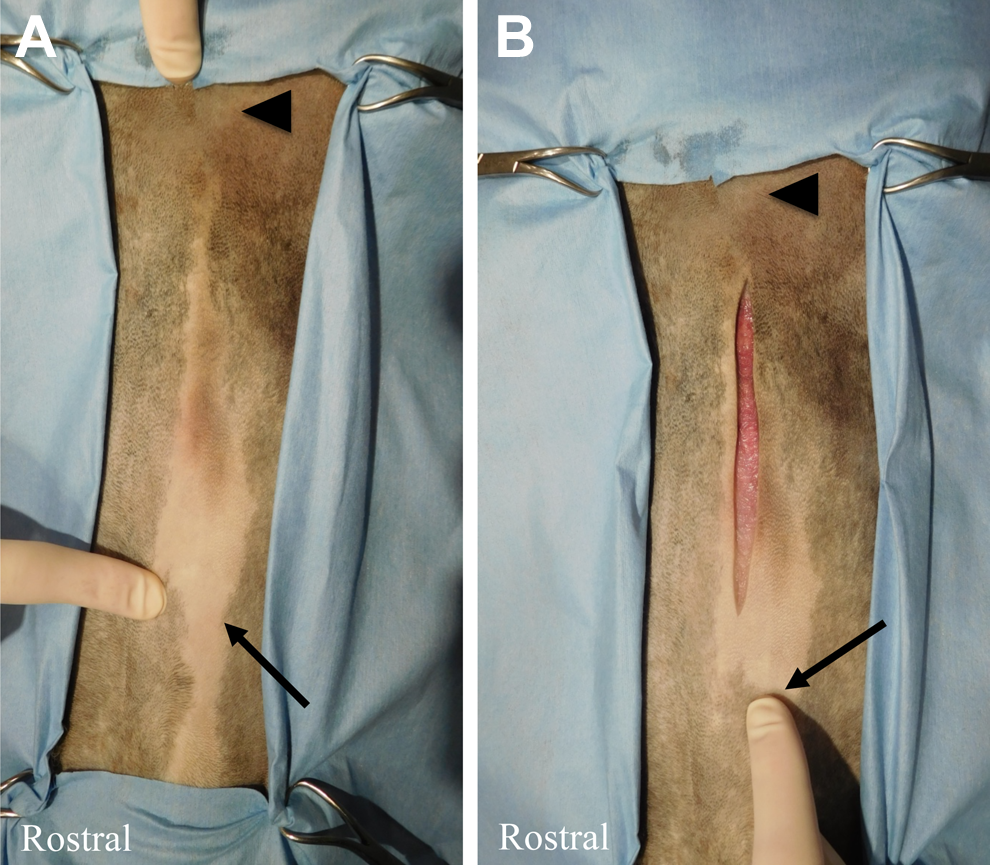
Photograph showing landmarks including the larynx (long arrow) and manubrium (short arrow). A, A 5- to 8-cm skin incision is made on ventral midline, starting 3 cm caudal to the larynx. B, Photograph showing the incision and its relation to the larynx (finger points to larynx).
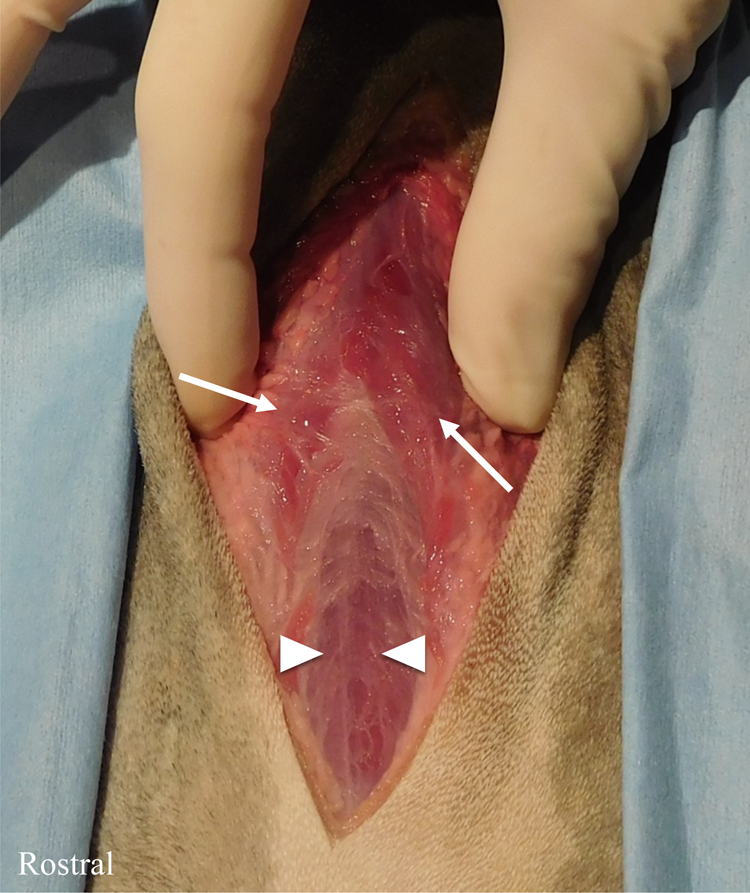
Photograph showing exposure of the muscles after incising the subcutaneous tissue. The paired sternocephalicus muscles (long arrows) are located more superficially than paired sternohyoideus muscles (short arrows).
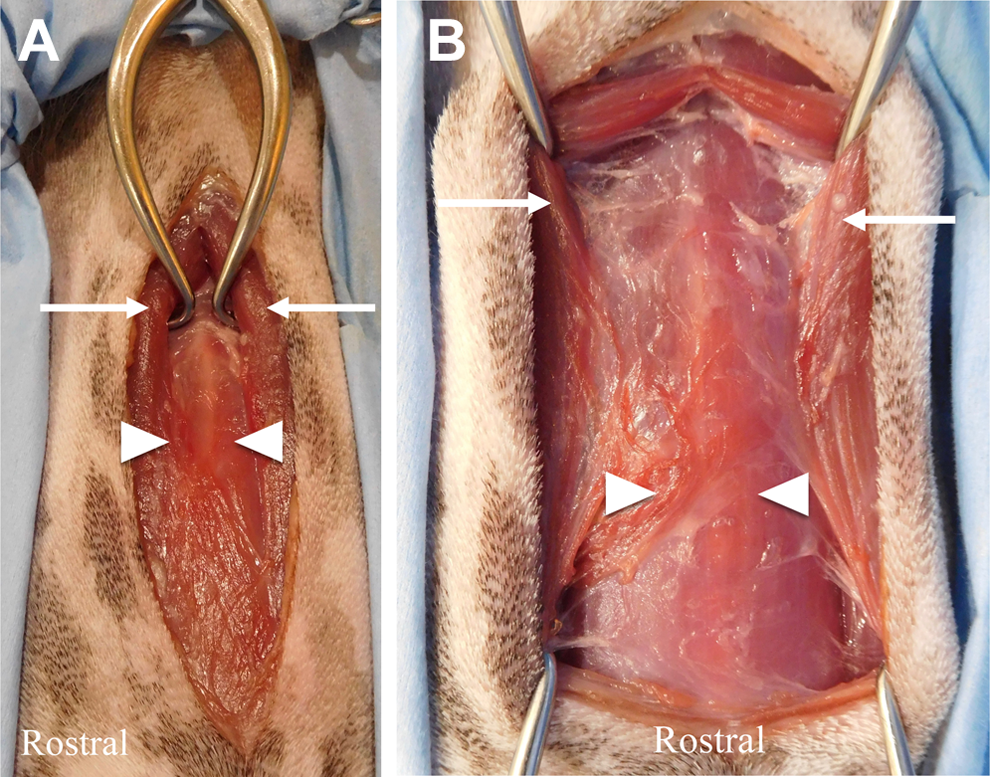
Photograph illustrating placement of the first Gelpi (A) and second Gelpi (B). The sternocephalicus muscles (long arrows) are incised and separated.
Studies have shown that temporary or permanent common carotid artery ligation can be performed to manage severe intraoperative maxillofacial hemorrhage when local measures or direct ligation of the bleeding vessel are not possible. 1,4 Unilateral and bilateral common carotid artery ligations have been proven to decrease lingual blood pressure in dogs, thereby decreasing intraoperative blood loss during maxillofacial surgery. 5,6 Furthermore, bilateral ligation of the common carotid arteries can be safely performed in dogs due to extensive collateral blood supply from the vertebral artery, allowing them to maintain adequate perfusion. 5,7 –9 Ligation of the common carotid artery should be used with caution in anemic dogs, and in all cats, due to their lack of collateral blood supply; it can be performed unilaterally with discretion in cats. 9,10 Care is taken to avoid trauma to the vagosympathetic trunk, which adheres to the dorsal surface of the common carotid artery, as well the recurrent laryngeal nerve and internal jugular vein located ventrally. 11
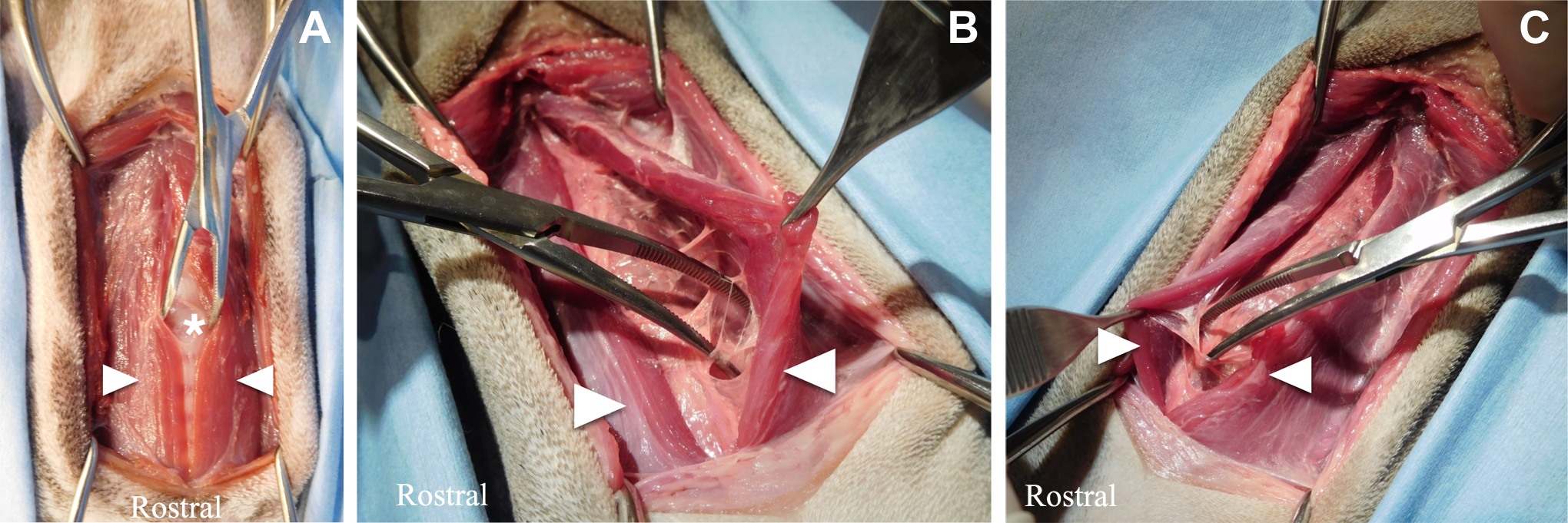
Picture illustrating blunt dissection to separate the paired sternohyoideus muscles after the fascia is incised on ventral midline (short arrows; A). Continued blunt dissection (B) and (C). *Trachea, still under fascia.
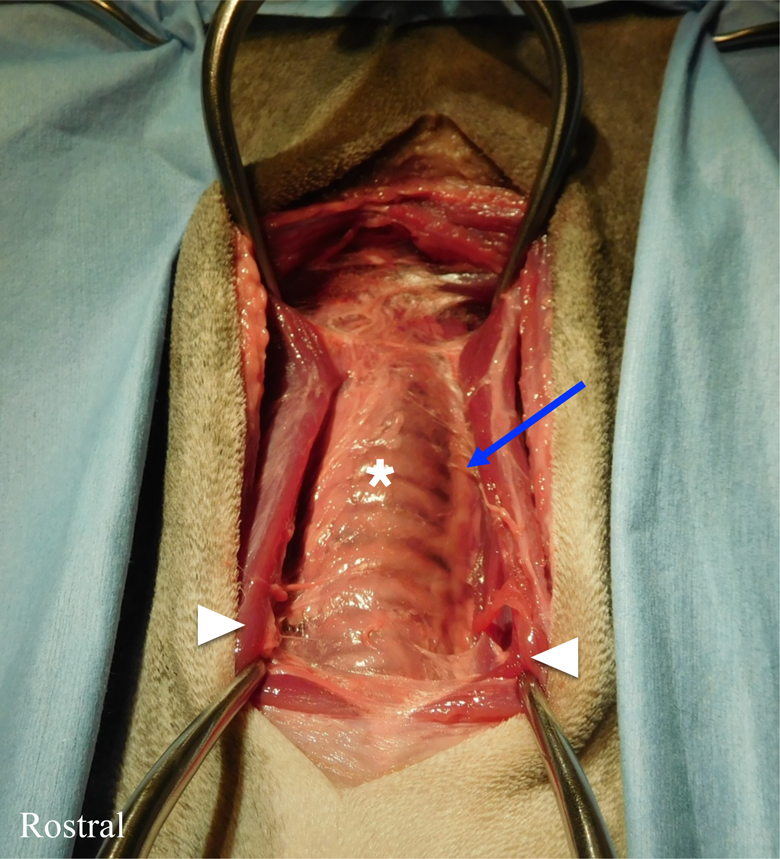
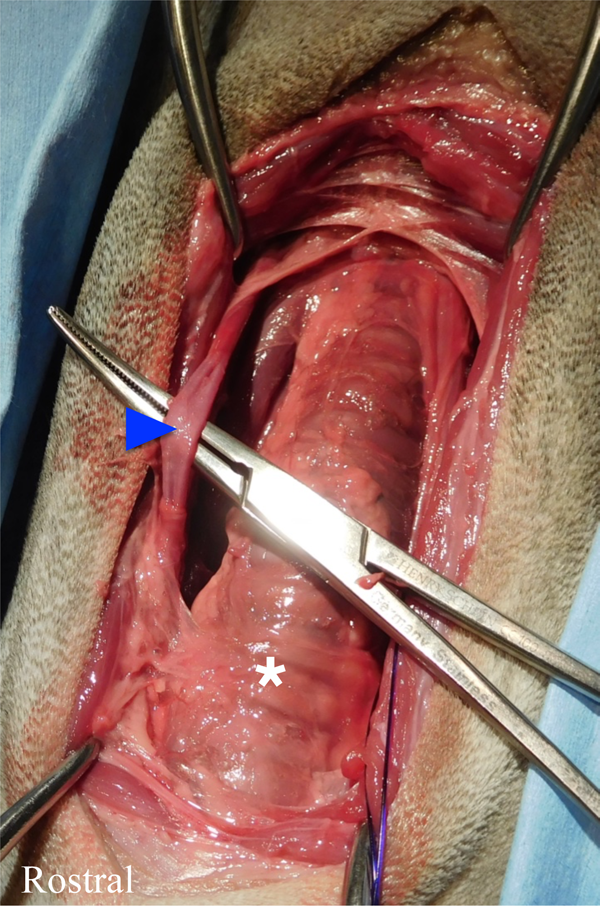
Photograph showing that after blunt dissection, the trachea (*) is more exposed and the carotid sheath can now be seen (thin blue arrow). The carotid sheath runs dorsolateral to the trachea. 11
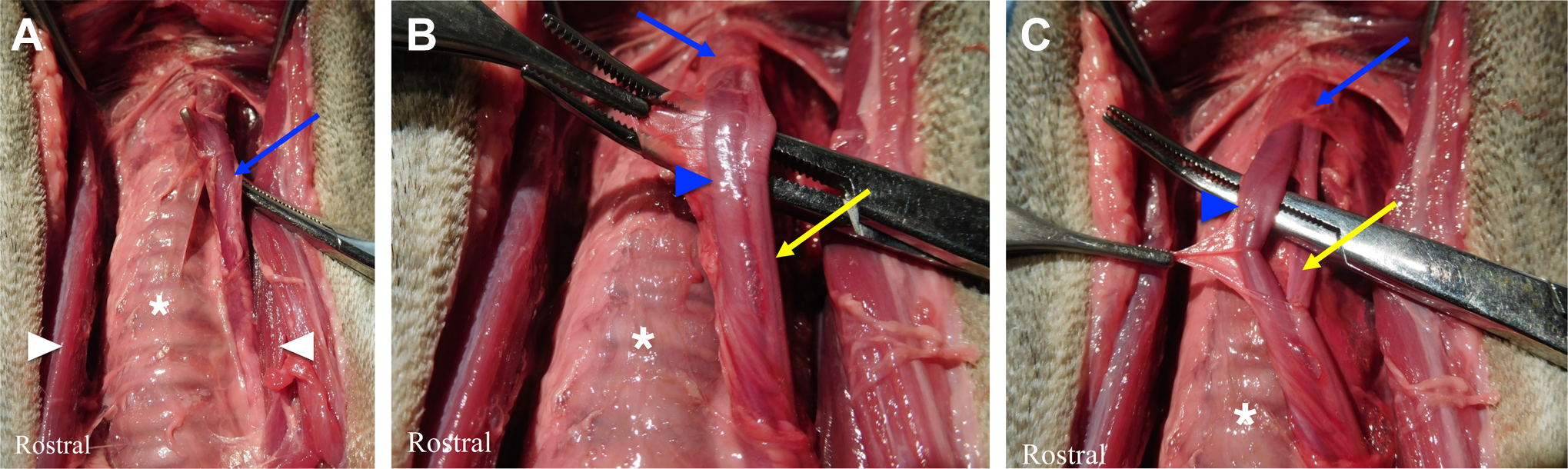
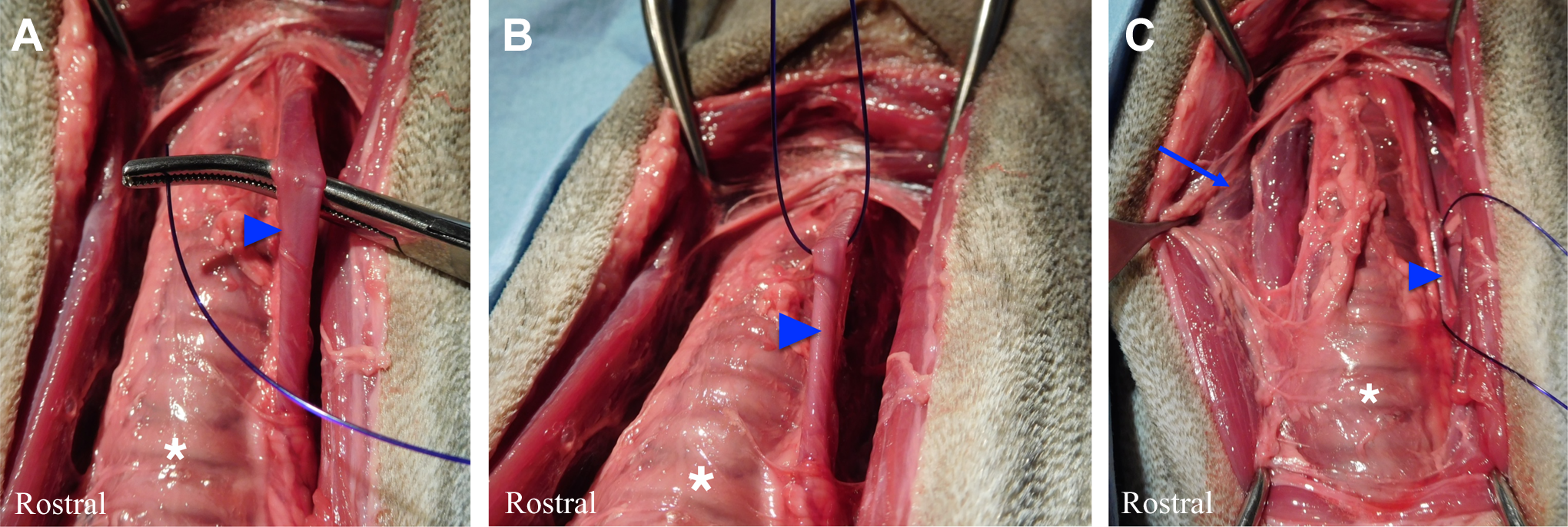
Photograph showing a curved hemostat being used to gently elevate the carotid sheath (blue arrow) from the lateral aspect to avoid trauma to the vagosympathetic trunk (also located within the carotid sheath) and the internal jugular vein (associated with the carotid sheath; A). Picture showing tissue forceps grasping the fascia of the carotid sheath (long blue arrow); now both the common carotid artery (short blue arrow) and vagosympathetic trunk (long yellow arrow) are visualized (B). The internal jugular vein is quite small in comparison to the common carotid artery and not present in this picture. Photograph showing the common carotid artery (short blue arrow) isolated from the vagosympathetic trunk (long yellow arrow) (C). It is identified by its pulse.
Photograph showing isolation of the right common carotid artery (short blue arrow). Once isolated, it can be temporarily occluded (see Figures 11 and 12) or permanently ligated (see Figure 10) with 0 polydioxanone. b The left common carotid sheath can be seen in C (long blue arrow).
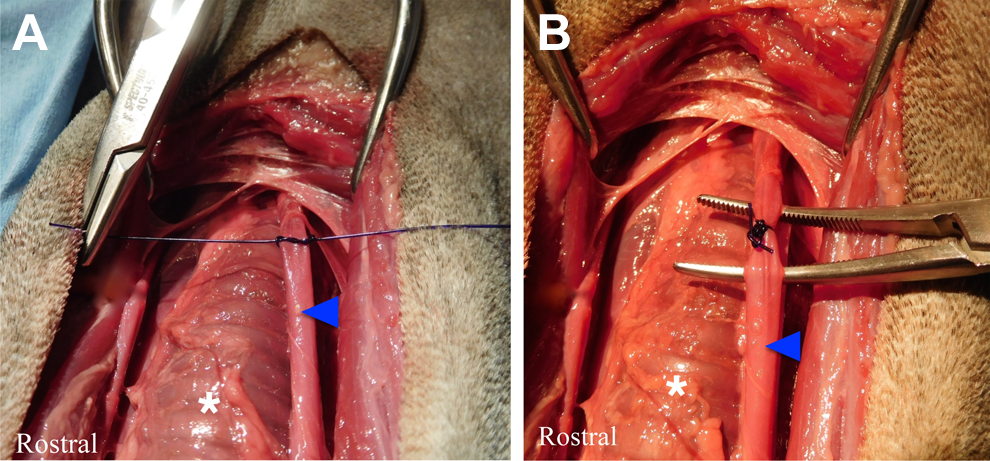
Photograph showing permanent ligation of the right common carotid artery with 0 polydioxanone (A) and (B).
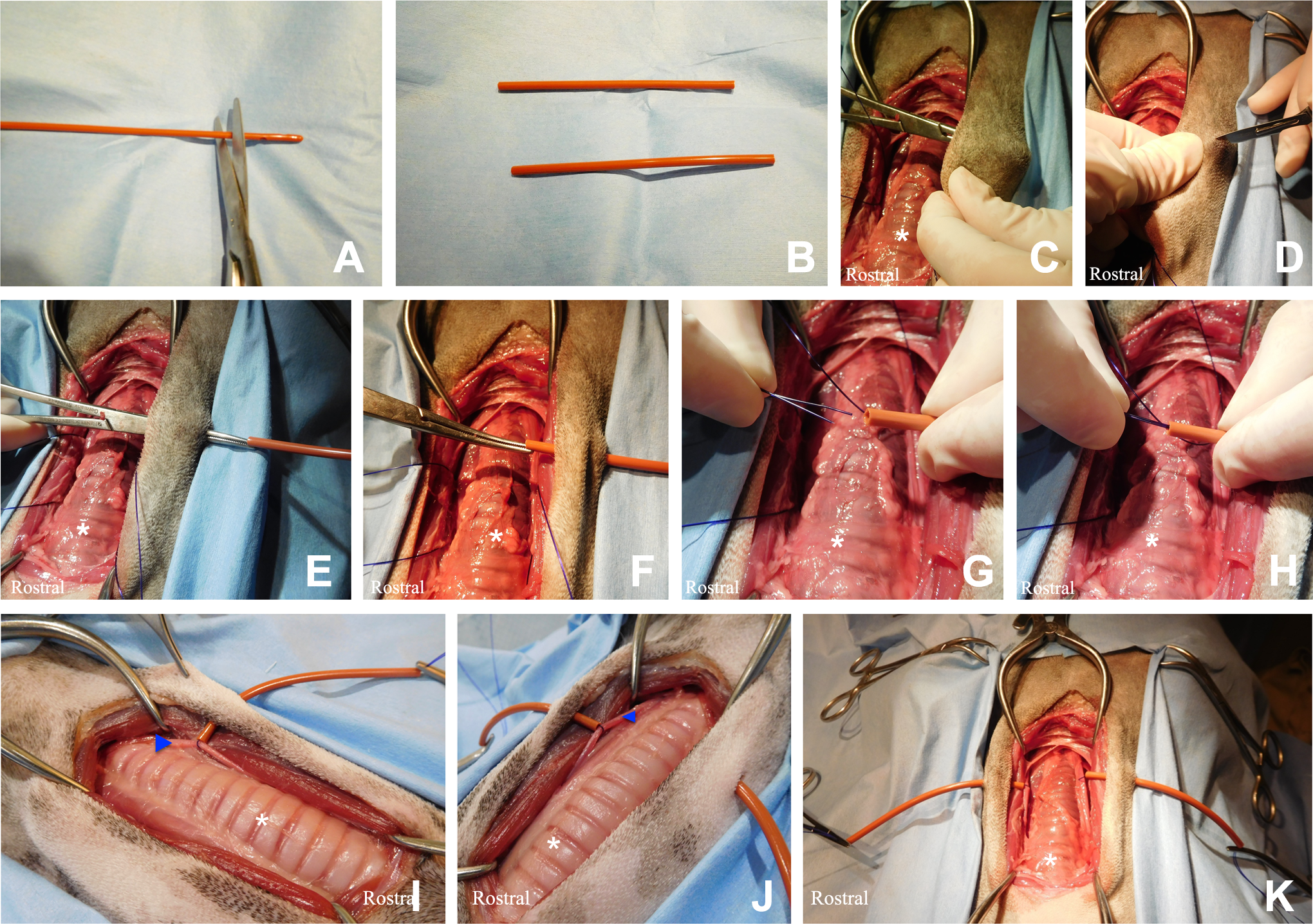
Photograph showing the steps involved for temporary carotid occlusion using a Rummel tourniquet technique. First, a size 8F or 10F red rubber catheter is cut into 2 smaller cylindrical pieces about 5 to 8 cm in length by removing both the flared and narrowed ends (A and B). A firm pressure pushes a hemostat laterally, causing a small tent in the skin about 3 cm lateral to the ventral midline incision (C). A #10 blade is used to make a 5-mm full-thickness incision through the skin and subcutaneous tissue over the tip of the hemostat with the jaws of the hemostat closed or very slightly open (D). An 8F or 10F red rubber catheter piece is next clamped with a hemostat (E) and pulled medially through the skin incision (F). Both ends of 0 polydioxanone have been looped around the right carotid artery are inserted into the catheter piece and then guided laterally until they exit the exterior end of the catheter (G and H). The red rubber catheter is held in close apposition to the common carotid artery (I). Occlusion is accomplished by pushing the catheter end against the artery while pulling the suture into the catheter, until the artery is compressed sufficiently such that no pulse can be felt. A hemostat is placed across the catheter at the skin exit site to maintain the occlusion. Alternatively, the tourniquet can be left loose and only tightened as needed during maxillofacial surgery. The procedure is repeated on the left common carotid artery (J). Bilateral Rummel tourniquets (K). The incision can be closed over the tourniquets, which are easily removed once the maxillofacial procedure is complete.
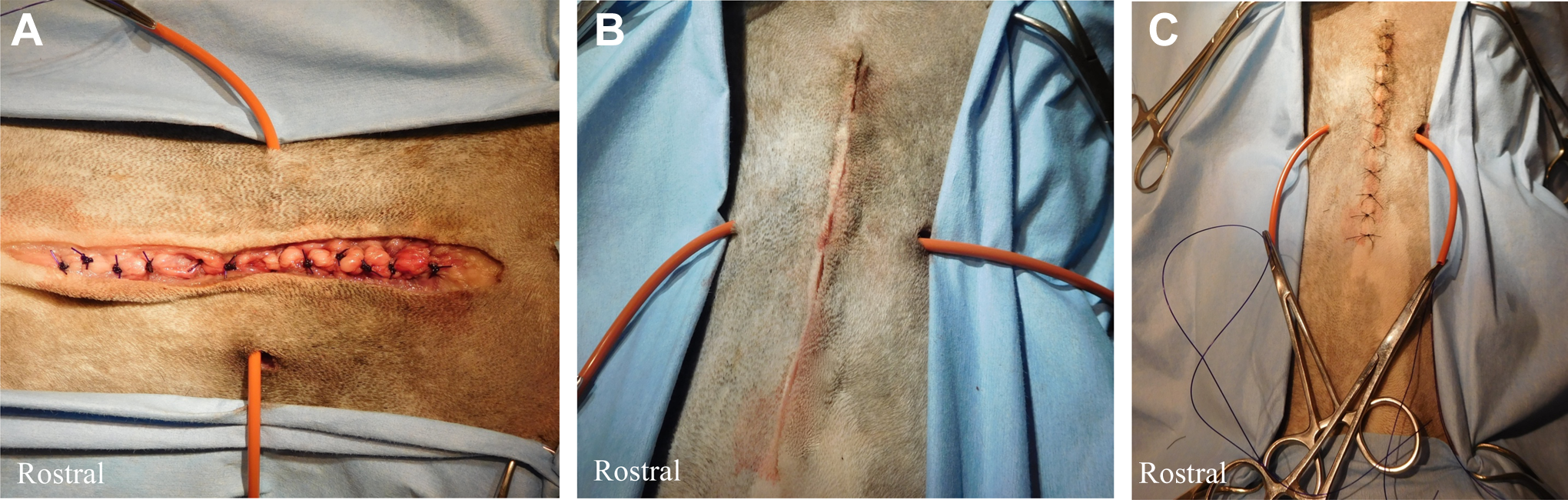
Incision closure, which is the same for both temporary ligation and permanent occlusion techniques. The muscles are closed using size 0 or 2-0 polydioxanone in a simple interrupted fashion (A). 3-0 poliglecaprone 25 c is used in a simple continuous pattern to close the intradermal layer (B). The skin is closed with 3-0 nylon d using cruciate sutures (C).

Final appearance after removing temporary ligation.
Carotid artery ligation in dogs is relatively simple and has minimal morbidity compared to humans, with several studies showing no notable adverse effects. 9 Rarely, adverse consequences of common carotid artery ligation include cerebral ischemia, retinal damage, and hematoma formation. 12,13
Preemptive temporary ligatures in the form of Rummel tourniquets can be placed around the common carotid arteries prior to major oral and maxillofacial surgery. 9,10 The tourniquets can either be tightened prior to maxillofacial surgery or tightened as needed during surgery if hemorrhage occurs. Indications for temporary occlusion of the common carotid artery include maxillectomy, mandibulectomy, glossectomy, surgery of the nasal cavity and nasopharynx, and other invasive oral and maxillofacial surgeries where significant hemorrhage is anticipated. 8 –10,14 This preventative measure provides better visualization of oral structures and reduces intraoperative blood loss.
The purpose of this article is to describe how to perform ligation of the common carotid artery in a step-by-step fashion. Both temporary and permanent ligation techniques are described.
Footnotes
Materials
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.