
Abstract
Microscopic alterations in the dental pulp of dogs have not been extensively studied. The aim of this study was to investigate microscopic alterations of the dental pulp in dogs’ teeth. One hundred and ten surgically extracted teeth (20 incisors, 23 canines, 28 premolars, and 39 molars) from 74 dogs, of different ages, with a history of chronic periodontitis (66 dogs), periapical abscesses (2 dogs), pulpitis (2 dogs), oral cavity neoplasms (2 dogs), dens invaginatus (1 dog), and dental fractures (1 dog) were included. Eight-one maxillary and 29 mandibular teeth were included. Coronal, radicular, and coronal plus radicular calculus were present in 28.2%, 17.3%, and 54.5% of the teeth, respectively. In total 78 teeth (71%) had pulp alterations, including fibrosis (26%), calcification (14%), necrosis associated with the absence of odontoblasts (14%), presence of predentin and dentin inside the cavity (8%), odontoblastic hyperplasia (3%), pigmentation (3%), pulpitis (2%), and pulp stones (1%). Forty-nine (60.5%) of the maxillary teeth and all of the mandibular teeth had pulp alterations. The premolars were most affected, and the molars least affected, by pulp alterations. Pulp fibrosis, calcification, and necrosis were observed in teeth irrespective of the distribution of dental calculus.
Introduction
Teeth are formed from dentin, enamel, and cementum, which surround and line the pulp cavity. 1 These rigid structures provide mechanical support for the dental pulp and protect it from microorganisms. Loss of the structural integrity of these tissues makes the pulp more susceptible to adverse stimuli from the oral cavity. 2
The most abundant cells in the pulp are fibroblasts, which form and maintain the extracellular matrix (ECM). The ECM consists of collagen and an intercellular fundamental substance composed of glycosaminoglycans, proteoglycans, and multi-adhesive glycoproteins. It fills the spaces between cells and connective tissue fibers and acts as a lubricant and barrier against the invasion of microorganisms.3–5 In addition to fibroblasts, pulp also contains undifferentiated ectomesenchymal cells, mesenchymal stem cells, macrophages, and other immunocompetent cells and odontoblasts. 5 The vascularization and innervation of the pulp comes from capillaries and nerve bundles that enter through the 40 to 90 foramina that make up the apical delta. 6
In a normal tooth, odontoblasts organize into a layer of tall columnar cells arranged in a palisade, with cytoplasmic extensions that form the dentinal tubules. In aged teeth, odontoblasts are present as a reduced cell layer. 7 These cells are responsible for the production of dentin throughout the life of the animal, which leads to progressive narrowing of the canal with advancing age.
Faced with an aggressive chemical, biological, or physical factor, the dental pulp responds with inflammatory or degenerative reactions, which depends on the type, frequency, and intensity of the offending agent, as well as the immune response of the individual. 8 Dental trauma and fractures are some of the processes that cause lesions in the pulp tissue by exposing the pulp cavity to the oral environment. 6 Periodontal disease can also be a predisposing factor for pulp alterations, since in addition to gingivitis, it also causes periodontitis with impairment of the supporting elements of the tooth. 9 One human study evaluated the influence of periodontitis on the pulp tissues of 67 patients with chronic periodontitis. 10 It found that all of the pulps had alterations such as inflammation, calcification, necrosis, loss of odontoblasts, and pulp fibrosis. In dogs, pulpitis and pulp necrosis can also be sequelae of periodontal disease. 11
Dental plaque is one of the main factors involved in the initiation and progression of periodontitis in dogs.12,13 An early study showed that the external dentin resorption cavities were frequent alterations in the teeth of dogs with dental calculus. 14 Given the close relationship between dentin and pulp (eg, the dentin–pulp complex), it is also pertinent to investigate changes in the pulp cavity of dogs with dental calculus.
Most studies on changes in the pulp cavity have been conducted in humans,10,15–19 and studies on dental pulp alterations in dogs are scarce. 11 Thus, the objective of this study was to investigate microscopic changes in the pulp cavities of 110 dogs’ teeth.
Materials and Methods
A total of 110 teeth were surgically extracted from 74 dogs (41 female and 33 male). Nineteen dogs had no defined breed and 55 were of different defined breeds. Of the 74 dogs, one was less than 2-years-old, 10 were between 2 and 6-years-old, and 60 were between six and 18-years-old. Three animals did not have their ages reported in their medical records. Each tooth was identified and stored individually in a 10% diluted formaldehyde solutiona and buffered with monobasicb and dibasic sodiumc solutions.
Twenty incisor teeth, 23 canines, 28 premolars, and 39 molars were included from dogs with a history of chronic periodontitis (66 dogs), periapical abscesses (2 dogs), dens invaginatus (1 dog), dental fractures (1 dog), pulpitis (2 dogs), and oral cavity neoplasms (2 dogs). The number of teeth extracted per dog ranged from one to eight, and all teeth had calculus. Eighty-one maxillary teeth and 29 mandibular teeth were included.
Dental calculus was classified as coronal (supragingival) when present on the dental crown and neck, radicular (subgingival) when present on the tooth root, and coronal plus radicular when present on the entire tooth (ie, crown, neck, and root).13,16 The frequency of coronal, radicular, and coronal plus radicular calculus in incisors, canines, premolars, and molars was evaluated. The terms coronal and radicular were used preferentially to the terms supragingival and subgingival, respectively, since the teeth were evaluated after extraction and without the presence of the gingiva.
After fixation in a 10% buffered formalin solutiond for at least 1-week, the teeth were decalcified in a 24% formic acid solutione, which was changed weekly for 2-weeks. The decalcification of the teeth occurred within a period of approximately 30-days and varied according to the size and type of tooth. After complete decalcification, the larger teeth were sectioned longitudinally. All teeth were processed using the paraffin embedding technique; dehydrated in 70%, 80%, 90%, and 100% ethyl alcoholf, cleared in xyleneg, embedded in paraffin, and sectioned using a microtomeh. Serial 0.5 μm histological sections of entire teeth were obtained and stained using the hematoxylin and eosin (H&E) technique. Histological sections of teeth with pulp cavity fibrosis were also stained with Masson's trichrome staini.
In addition to the diagnosis of pulp alterations, the frequency of these alterations in incisor, canine, premolar, and molar teeth, as well as in teeth with coronal, radicular, and coronal plus radicular calculus was evaluated.
Results
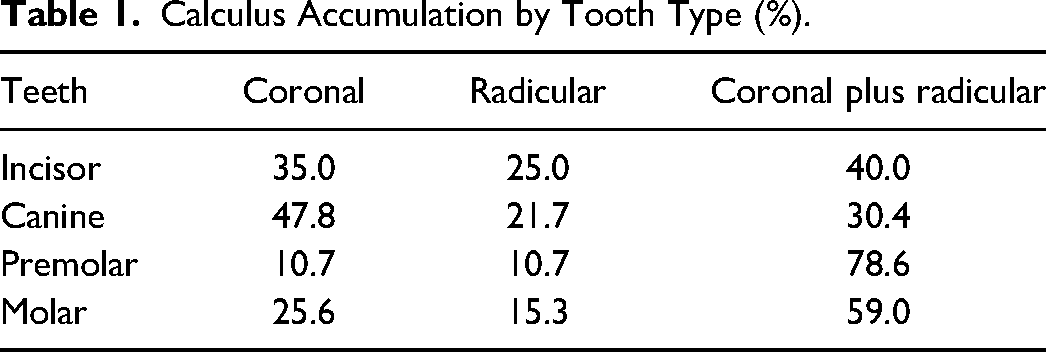
Coronal, radicular, and coronal plus radicular calculus were present on 28.2%, 17.3%, and 54.5% teeth, respectively. The types of teeth and their calculus distributions are shown in Table 1. Canine teeth had the highest percentage of coronal calculus and incisors had the highest percentage of radicular calculus. Premolars and molars had the highest percentage of teeth having both radicular plus coronal calculus.
Calculus Accumulation by Tooth Type (%).
In total 78 teeth (71%) had alterations in the pulp cavity, specifically fibrosis (26%), calcification (14%), necrosis associated with the absence of odontoblasts (14%), presence of predentin and dentin inside the cavity (8%), odontoblastic hyperplasia (3%), pigmentation (3%), pulpitis (2%), and pulp stones (1%) (Figure 1).
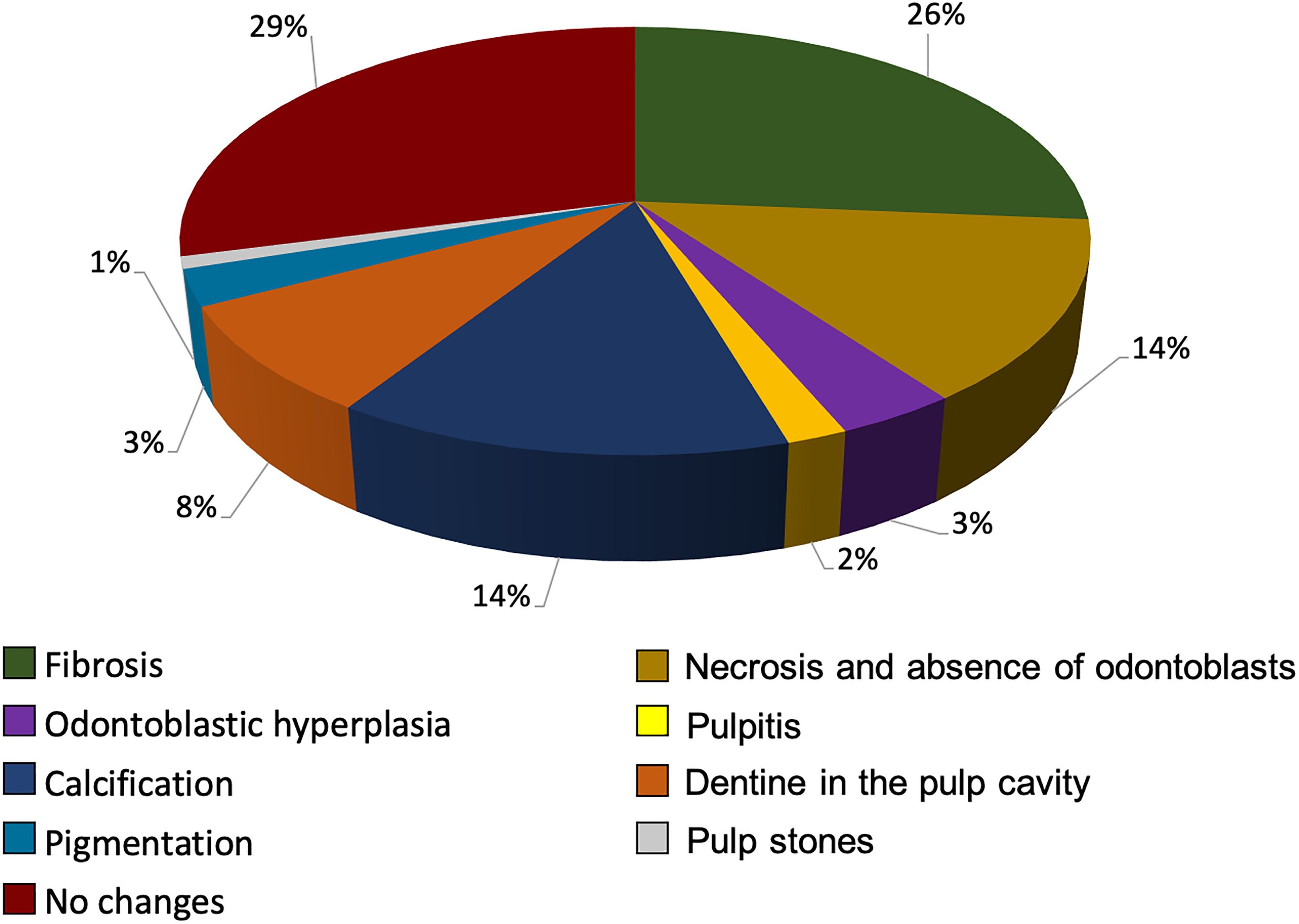
Microscopic alterations of the pulp cavities.
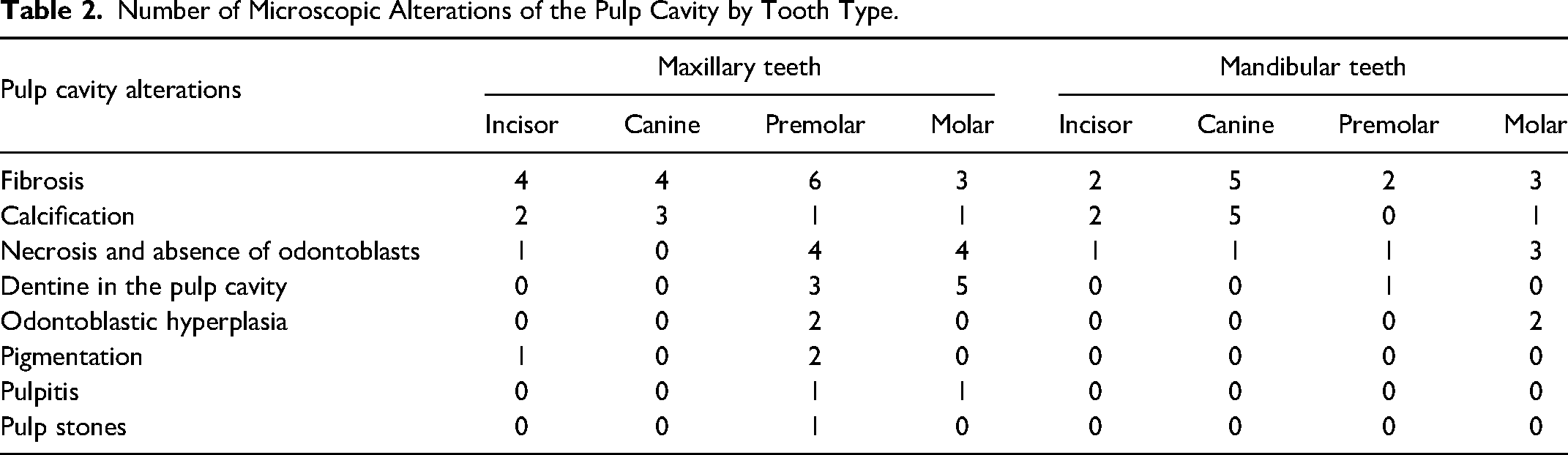
The frequency of pulp changes was also described in mandibular and maxillary teeth. Of the 81 maxillary teeth, 49 (60.5%) had pulp alterations and of the 29 mandibular teeth, all had pulp alterations (Figure 2). The number of microscopic alterations of the pulp cavity is described for each type of maxillary and mandibular tooth in Table 2. Changes in the pulp cavity were also evaluated, and their frequency described for each type of tooth. Premolar and molar teeth presented the highest and lowest frequency of pulp alterations, respectively, and together they presented the greatest variety of pulp alterations (Figure 3).
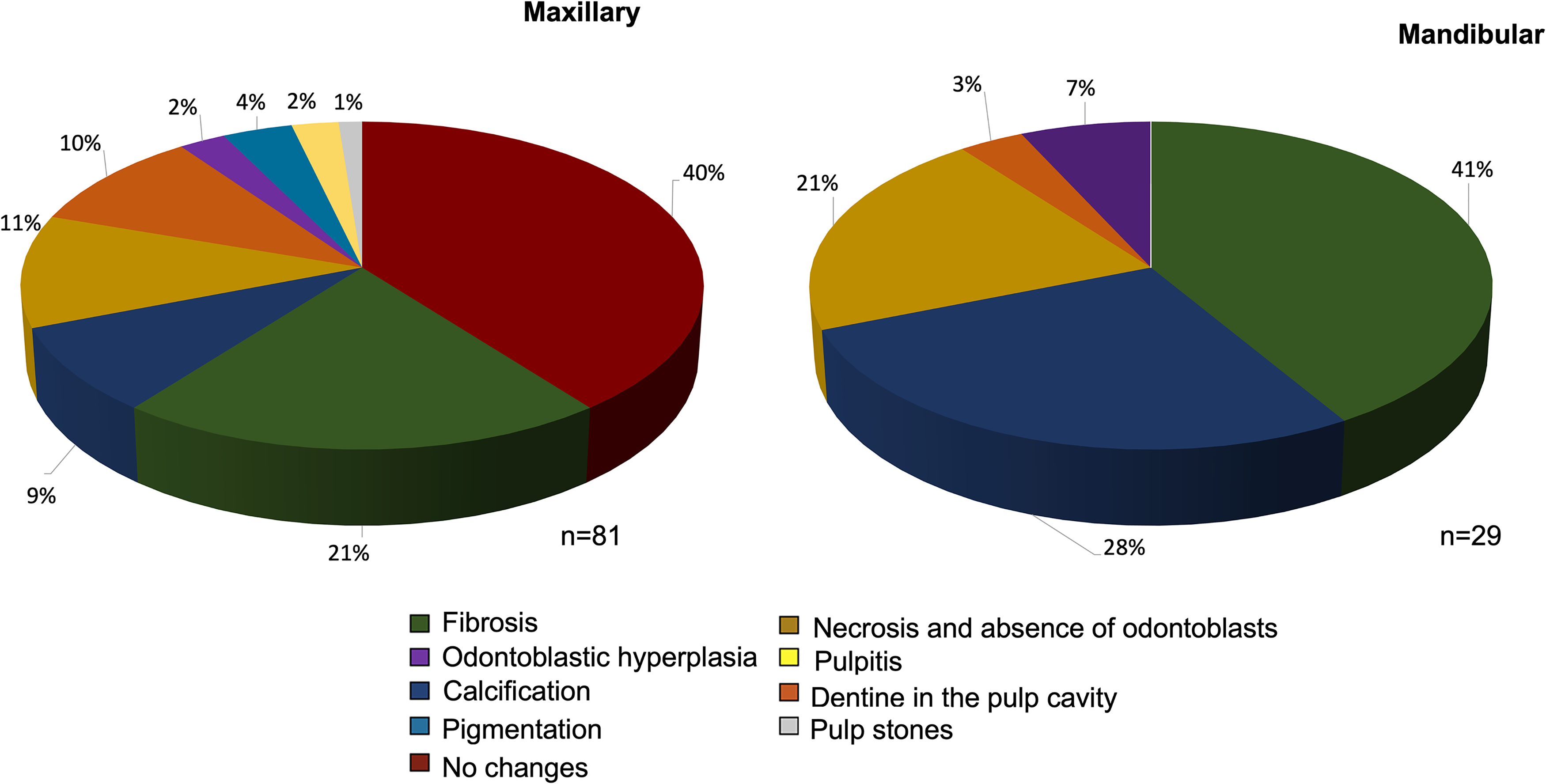
Microscopic alterations of the pulp cavity of maxillary and mandibular teeth.
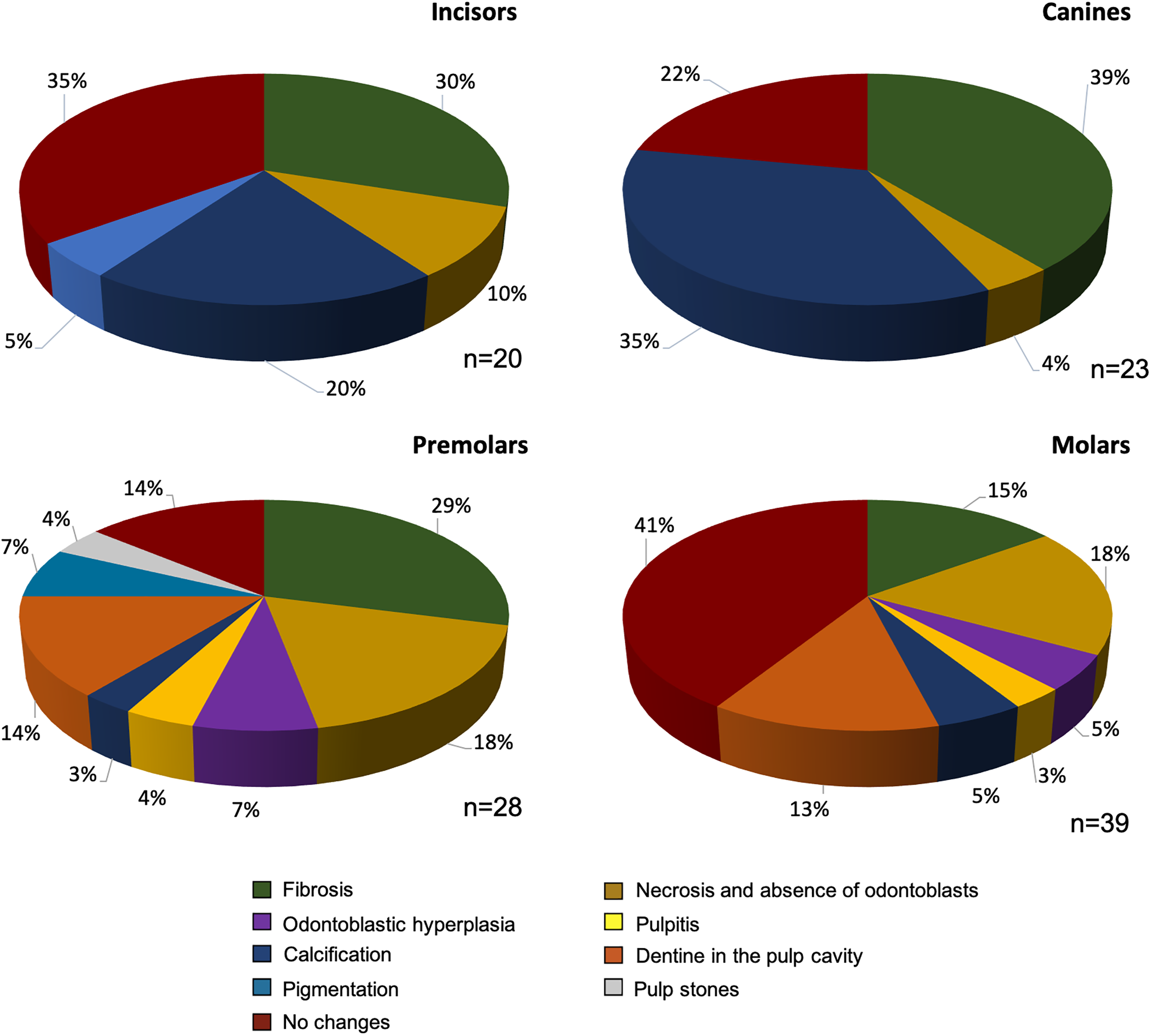
Microscopic alterations of the pulp cavity of incisor, canine, premolar, and molar teeth.
Number of Microscopic Alterations of the Pulp Cavity by Tooth Type.
Dental pulp fibrosis was the most frequently observed alteration, especially in the canine, incisor, and premolar teeth. Dental pulp fibrosis is characterized by the replacement of the entire tooth pulp or parts of the tooth pulp close to the root apex by fibrous connective tissue (Figure 4A), which stains blue with Masson's trichrome (Figure 4B and 4C).
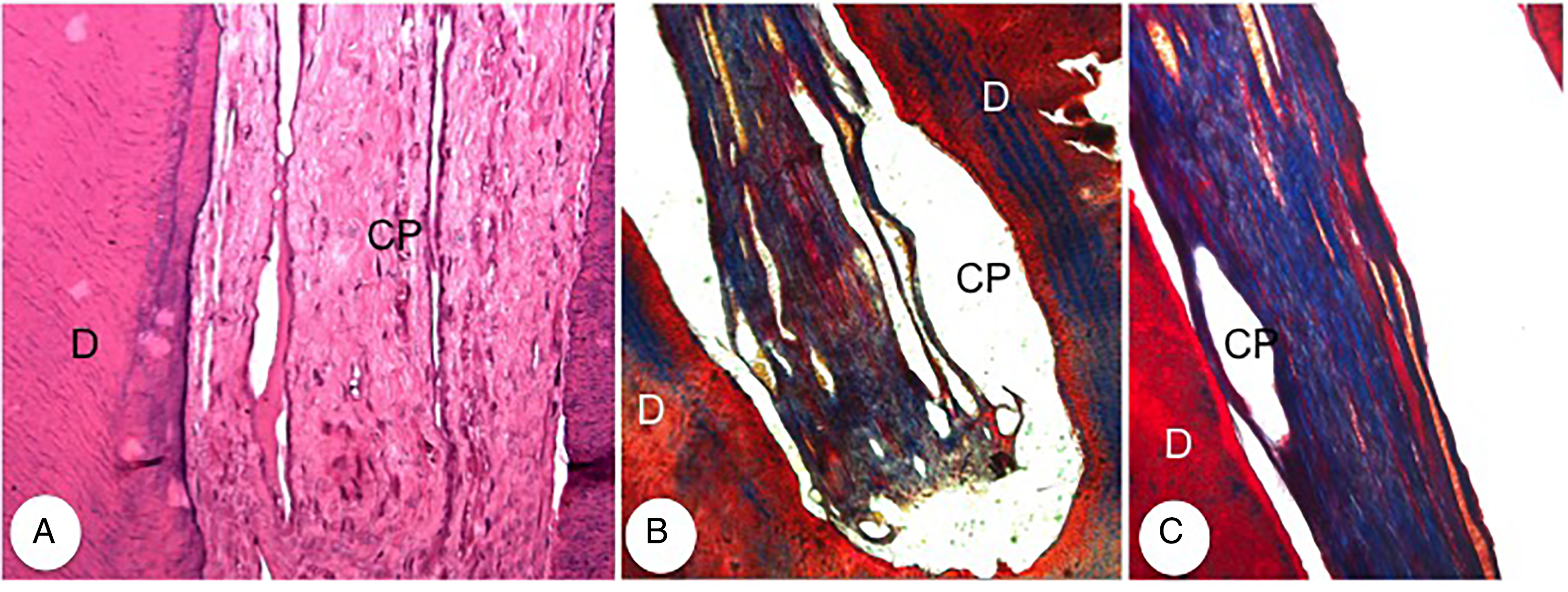
Photomicrographs of teeth with pulp fibrosis. (A) Replacement of the pulp by a large amount of fibrous connective tissue (H&E: 50x). (B) and (C) Large amount of blue collagen fibers inside the pulp cavity. Note the absence of odontoblasts (Masson's Trichrome: 12.5x and 25x, respectively). Abbreviations: CP, pulp cavity D, dentin; H&E, hematoxylin and eosin.
In several teeth, pulp fibrosis was associated with pulp calcification, the second most frequent alteration of the dental pulp (Figure 5A and 5B). This change was mainly observed in canine teeth.
Photomicrographs of teeth with calcification and pulp fibrosis. (A) Incisor tooth with multifocal to coalescing calcification of the pulp close to the root apex, which is associated with fibrosis (H&E: 50x). (B) Canine tooth with calcification and pulp fibrosis. Note the absence of odontoblasts (H&E: 50x). Abbreviations: CP, pulp cavity; D, dentin; H&E, hematoxylin and eosin.
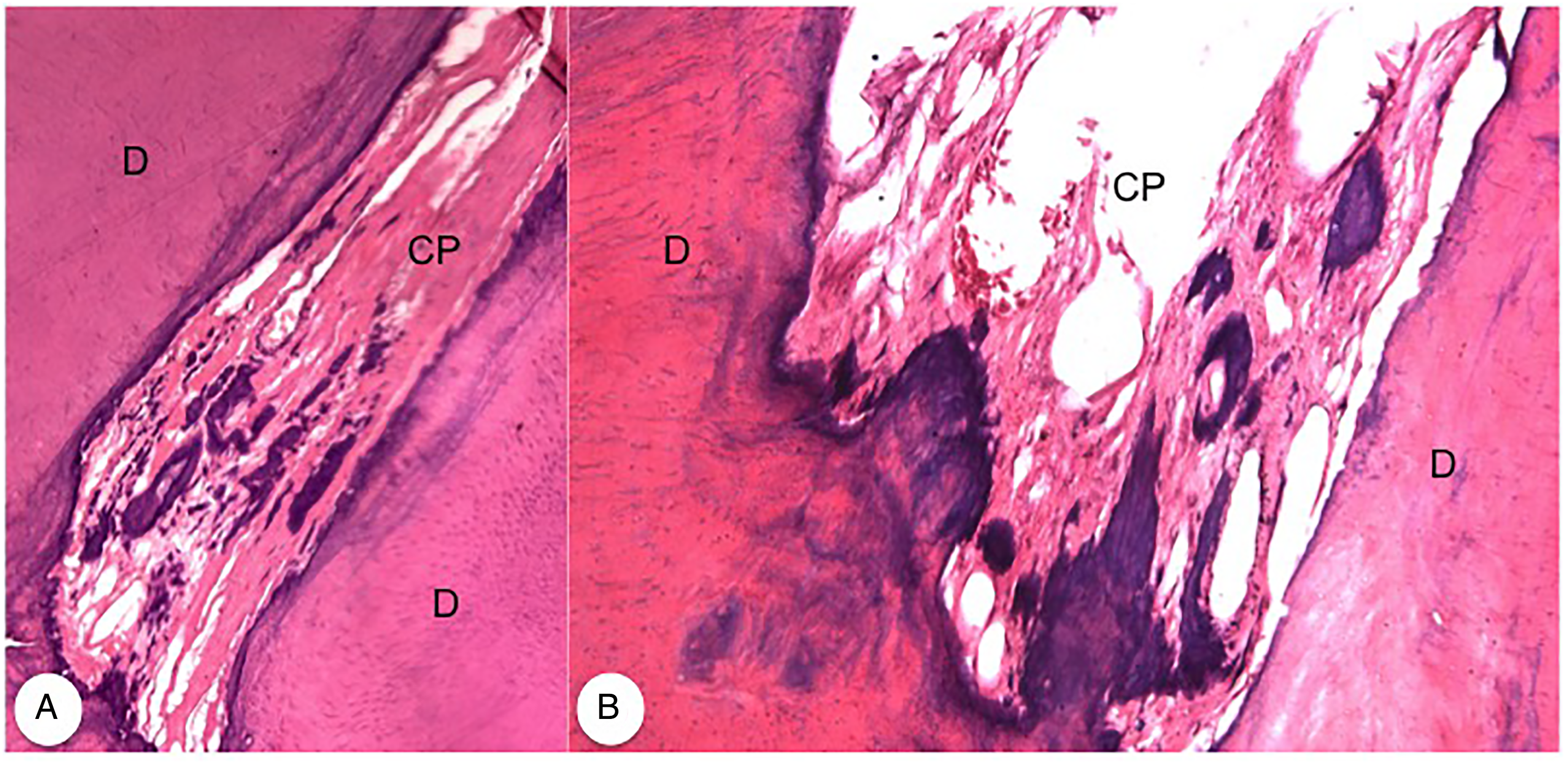
Dental pulp necrosis was more frequently observed in premolar and molar teeth. In this alteration, the pulp cavity was filled with cellular debris and/or amorphous and acellular eosinophilic material, and odontoblasts were absent (Figure 6A). In some teeth, pulp necrosis was associated with internal dentin resorption cavities (Figure 6B).
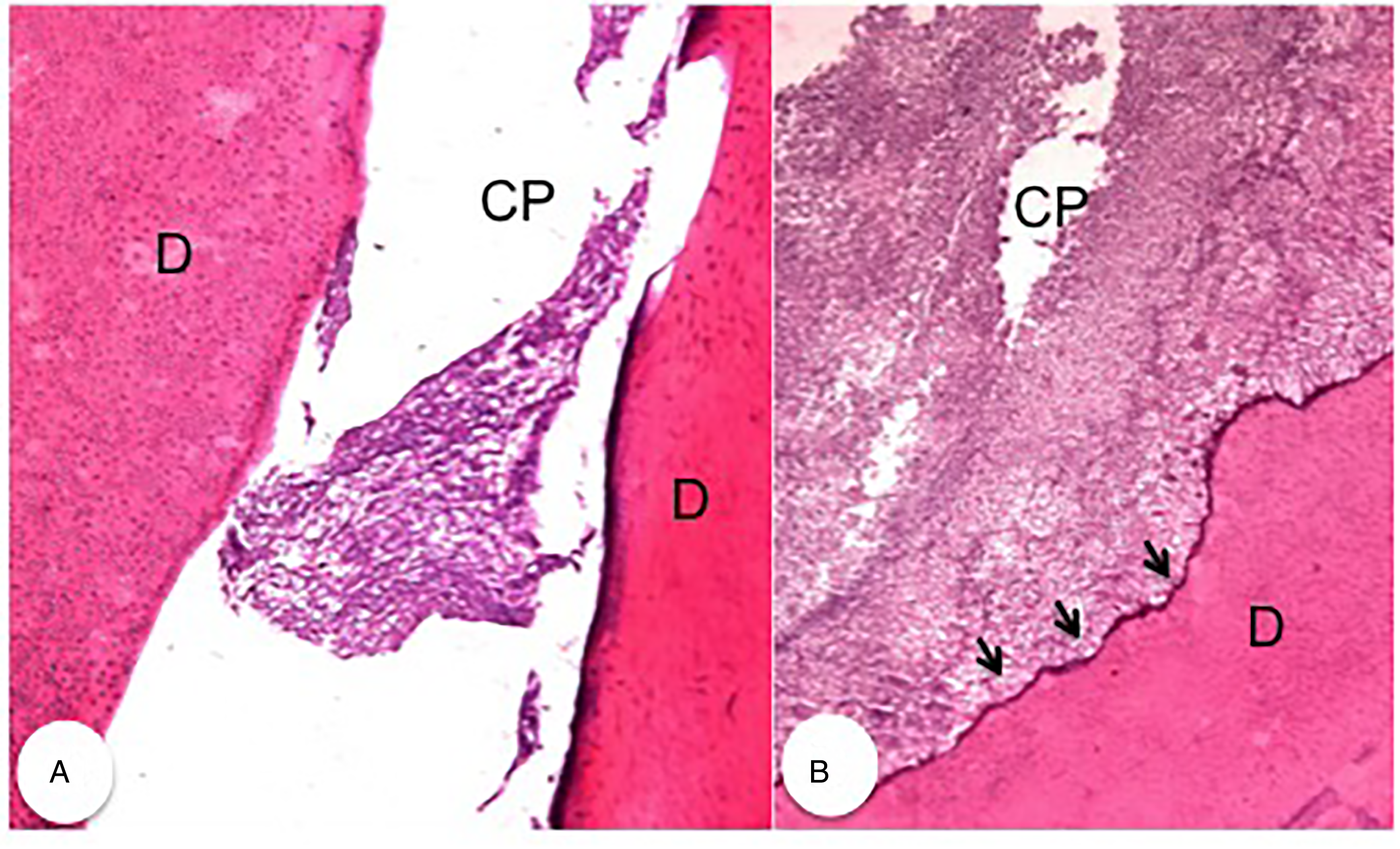
Photomicrographs of premolar teeth with pulp necrosis and internal resorption cavities. (A) Pulp cavity with cell debris (necrosis) (H&E: 50x). (B) Intense pulp necrosis and internal resorption cavity (arrows). Note the absence of odontoblasts (H&E: 100x). Abbreviations: CP, pulp cavity; D, dentin; H&E, hematoxylin and eosin.
Pulpitis was observed in only two teeth (1 premolar and 1 molar of two individual dogs). In these teeth, the inflammatory infiltrate consisted of lymphocytes, plasma cells, and some neutrophils. In one tooth, inflammation was associated with pulp fibrosis (Figure 7A). These teeth also had odontoblastic hyperplasia characterized by the presence of many odontoblasts with rounded nuclei and poorly defined cytoplasm, arranged in several layers juxtaposed to the predentin (Figure 7B). Odontoblastic hyperplasia was not only associated with pulpitis but was also observed in other teeth without inflammation.
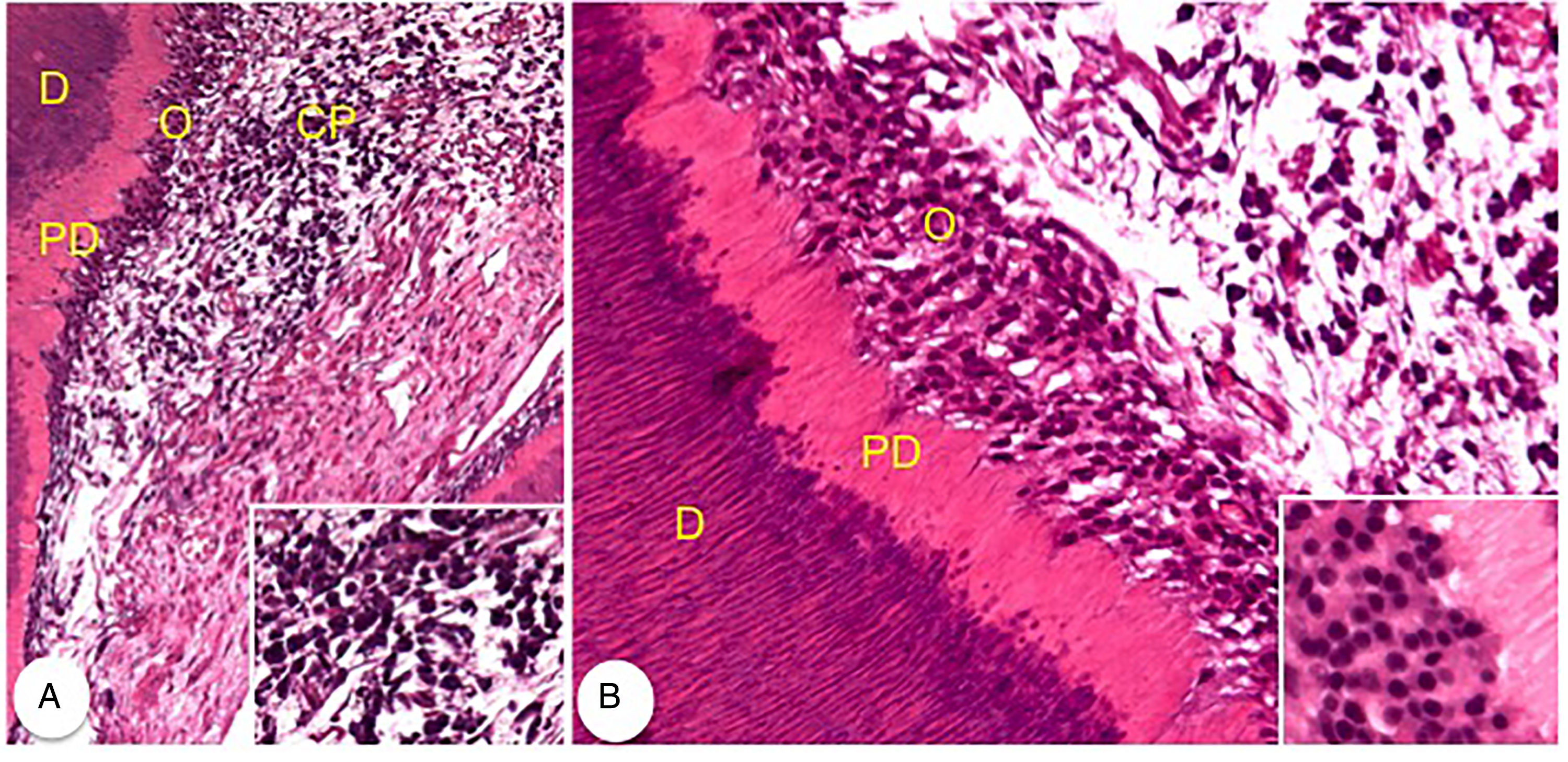
Photomicrographs of premolar teeth with pulpitis and odontoblastic hyperplasia. (A) Inflammatory infiltrate in the pulp associated with fibrosis. Inset: Note the characteristic inflammatory cells, with a predominance of lymphocytes (H&E: 50x). (B) Pulpitis and odontoblastic hyperplasia characterized by the presence of a large number of odontoblasts arranged in several layers juxtaposed to the predentin. Inset: Odontoblasts with rounded nuclei and poorly defined cytoplasm (H&E: 50x). Abbreviations: CP, pulp cavity; D, dentin; H&E, hematoxylin and eosin; PD, predentin; O, odontoblasts.
Other alterations such as pigmentation, which is characterized by the presence of a brownish pigment similar to hemosiderin inside the pulp cavity, were rarely observed. Pigmentation affected the incisor and premolar teeth. It is sometimes seen in association with necrotic debris. Pulp calculi were observed in a single premolar tooth, characterized by the presence of an eosinophilic, lamellar, and rounded material associated with fibrosis and hyperemia of the pulp (Figure 8A and 8B).

Photomicrographs of a premolar tooth. (A) and (B) Pulp calculus characterized by the presence of a rounded, eosinophilic, and lamellar material (arrow), associated with fibrosis and hyperemia of the pulp (H&E: 25x and 50x, respectively). Abbreviations: CP, pulp cavity; D, dentin; H&E, hematoxylin and eosin.
Dens invaginatus was observed in a single premolar tooth. Dens invaginatus was characterized by the presence of irregular dentin invaginations into the pulp cavity in the region of both the crown and the root (root canal), with remnants of necrotic material from the pulp and the loss of characteristic tooth morphology. Small teeth or tooth fragments could be observed inside the larger pulp cavity. Another alteration observed was the presence of predentin and dentin inside the pulp cavity. This change was mainly observed in premolar and molar teeth.
In teeth with coronal calculus (n = 21), fibrosis (1 incisor, 4 canines, 2 premolars, and 3 molars), calcification (1 incisor, 4 canines, and 2 premolars), necrosis (2 incisors), and predentin and dentin within the pulp cavity (1 premolar and 1 molar) were observed (Figure 9).
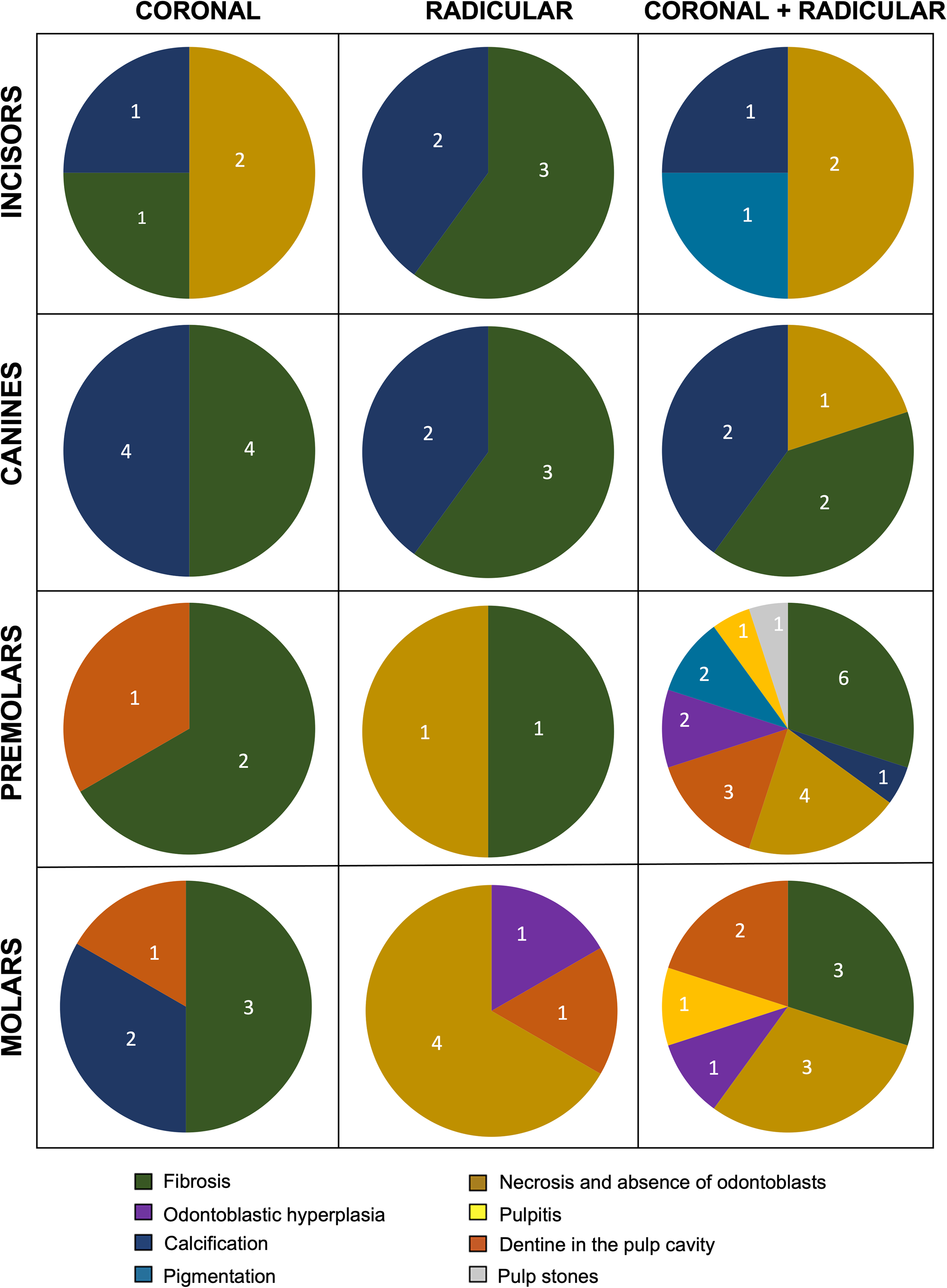
Microscopic alterations in the pulp cavity of incisor, canine, premolar, and molar teeth according to the classification of calculus (coronal, radicular, and coronal plus radicular).
In teeth with radicular calculus (n = 18), fibrosis (3 incisors, 3 canines, and 1 premolar), calcification (2 incisors and 2 canines), necrosis (1 premolar and 4 molars), presence of predentin and dentin within the pulp cavity (1 molar), and odontoblastic hyperplasia (1 molar) were observed (Figure 9).
In teeth with coronal plus radicular calculus (n = 39), a greater variety of changes in the dental pulp were observed. Pulp fibrosis was the most frequent alteration (2 incisors, 2 canines, 6 premolars, and 3 molars), followed by pulp calcification (1 incisor, 2 canines, and 1 premolar), necrosis (1 canine, 4 premolars, and 3 molars), predentin and dentin within the pulp cavity (3 premolars and 2 molars), odontoblastic hyperplasia (2 premolars and 1 molar), pigmentation (1 incisor and 2 premolars), inflammation (1 premolar and 1 molar), and pulp stones (1 premolar) (Figure 9).
Discussion
The aim of this study was to identify microscopic changes in the pulp cavity irrespective of calculus as the causal agent. Fibrosis, calcification, and necrosis were the most frequent pulp alterations, irrespective of the distribution of calculus.
Coronal plus radicular calculus was observed in more than 50% of teeth in this study. One of the reasons for this high percentage was the lack of dental cleaning, which can lead to the progression of calculus on the tooth surface and affect both the crown and the root. Tooth brushing is the most effective method of interrupting the formation of bacterial plaque, and consequently calculus.20,21 The lack of teeth cleaning, associated with an age of less than 6 years in most of the animals studied, may also be related to the increase in the extent of calculus on the teeth, and in turn periodontitis. 9 Chronic periodontitis was the reason for tooth extraction in 66 dogs in this study. Only half of the animals over 6 years of age had a history of oral prophylaxis within the past year. In addition, of the 55 animals with a defined breed in our study, 30 were small dogs. Small dogs show greater malocclusion and greater accumulation of bacterial plaque and calculus, as they often have overcrowding of teeth, with less interdental space, making it difficult to remove plaque and debris accumulation.20,21
The distribution of calculus differed among types of teeth. The canine teeth had a higher percentage of coronal calculus, and incisors had more radicular calculus. The premolars and molars had a higher percentage of teeth with coronal plus radicular calculus. Canine teeth showed a lower percentage of coronal plus radicular calculus, which can be explained by the friction that occurs during chewing.22,23 Similarly, another study demonstrated that canine teeth were more affected by coronal calculus than other locations of calculus. 24 The high frequency of coronal plus radicular calculus in premolar teeth observed in this study is similar to other study. 22
Of the 110 teeth analyzed for microscopic alterations, 78 had some type of pulp alteration. Premolar teeth were the most affected. Pulp alterations such as necrosis, fibrosis, and pulp calcification were observed in all types of teeth, but at variable frequencies.
Pulp necrosis mainly affects the molar and premolar teeth. Pulp necrosis, as well as pulpitis, may be related to periodontitis in dogs and may result from bacterial invasion of the pulp cavity through accessory canals and exposed roots. 25 Several studies in humans have demonstrated that periodontitis can cause pulpitis, necrosis, fibrosis, and calcification.16,17,19
In the present study, despite the history of periodontitis in 66 dogs, pulpitis was diagnosed in only 1 premolar and 1 molar from two dogs, and these dogs had no history of periodontitis. In one dog, the tooth with pulpitis was extracted due to an epulis, and in the second dog, the tooth with pulpitis was extracted due to a periapical abscess.
In pulpitis, in addition to inflammatory cell infiltrates, fibrosis, calcification, hemorrhage, and necrosis has be observed. 7 If the cause of the pulpitis is quickly removed, the pulp tissue may heal; otherwise, the pulpitis becomes irreversible and may progress to necrosis. 11 Therefore, the question remains whether other changes observed in this study, such as fibrosis and calcification, can also result from untreated pulpitis. However, fibrosis and calcification of the dental pulp may also be related to the ageing of teeth. 25
Another alteration found in the dental pulp of premolar and molar teeth, albeit at low frequency, was odontoblastic hyperplasia. In one of the teeth, odontoblastic hyperplasia was associated with pulpitis. It is possible that the increase in the number of odontoblasts, which characterizes the areas of hyperplasia, is a response to external or internal injuries. 26 Dentinogenesis is a dynamic process regulated by a single layer of highly differentiated postmitotic odontoblastic cells. The intrinsic capacity of the dental pulp to repair the lost or damaged dentin matrix and to increase its defense barrier depends on the vitality of the odontoblastic cell layer. 27 After an irritating stimulus, odontoblasts can undergo metabolic changes that can induce an inflammatory response in the pulp. Disturbances in odontoblasts can also affect matrix synthesis by increasing or decreasing predentin synthesis. In response to mild to moderate injuries, odontoblasts increase their metabolic activities, while in response to more severe injuries, odontoblasts may die. 28
Less frequent alterations such as pulp calculi, dens invaginatus, predentin, and dentin were also observed inside the pulp cavity. The pulp calculi were found in the premolar teeth but based on their histological characteristics (mineralized appearance with concentric formation and surrounded by fibrous connective tissue), they were “false” pulp calculi,29,30 which can be attributed to necrotic cell debris. Dens invaginatus was found in a single molar tooth of a Rottweiler. Previous studies have shown that molars are the teeth most affected by dens invaginatus, particularly in Yorkshire Terriers. Pulp necrosis is one of the main consequences of this change.7,31,32 Inside the pulp cavity of some teeth, predentin and dentin invaginations were observed between the pulp tissues. This change does not have a specific name, but similar changes have been reported in dogs’ teeth, where it characterizes irregularities in the wall of the pulp chambers. 25
Of the 110 teeth analyzed, 81 (73.64%) were maxillary and 29 (26.36%) were mandibular. Of the 81 maxillary teeth, 49 (60.49%) had pulp alterations. In addition, a greater number of different types of pulp alterations in maxillary teeth were found. In the mandible, all 29 teeth analyzed presented pulp alterations. However, it cannot be said that pulp alterations are less frequent in mandibular teeth, as the number of teeth extracted from this region was much smaller compared to the number of maxillary teeth.
It is likely that the greater number of teeth extracted from the maxilla is related to chronic periodontitis, which was the cause of surgical dental extraction in 66 dogs in this study. The location of the parotid gland duct close to the maxillary fourth premolar and neighboring teeth increases the incidence of dental plaque in these teeth, and consequently causes gingivitis and periodontitis. 10 The premolar teeth in this study represent more than 40% of the maxillary teeth with pulp alterations. However, further investigations are needed in order to analyze the relationship between pulp and dental changes in general, associated with maxillary and mandibular teeth.
Conclusion
A total of 71% of teeth showed some microscopic alteration in the pulp cavity. The maxillary premolar teeth were the most affected and the molar teeth least affected. Fibrosis, calcification, and necrosis are the main pulp alterations in dog teeth, irrespective of the distribution of calculus.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico.
Materials
Rioquímica, São José do Rio Preto, São Paulo, Brazil Vetec, Duque de Caxias, Rio de Janeiro, Brazil Vetec, Duque de Caxias, Rio de Janeiro, Brazil Rioquímica, São José do Rio Preto, São Paulo, Brazil CRQ produtos químicos Eirelli, Casa Grande, São Paulo, Brazil Sciavicco, Belo Horizonte, Minas Gerais, Brazil Dinâmica Química Contemporânea Ltda, Indaiatuba, São Paulo, Brazil Microm HM 315R microtome, Walldorf, Germany Reagen, Jardim Carvalho Colombo, Paraná, Brazil