
Abstract
In active force orthodontics in dogs, the ratio of root surface area (RSA) between the anchorage and target dentition is the primary factor when determining the expected relative movement patterns. Reinforced anchorage involves bonding of adjacent structures together (ie, 2 or more teeth) in the anchorage unit to increase the total attachment or RSAs. This methodology is commonly implemented in the movement of the maxillary canine tooth using active force orthodontics by bonding the maxillary fourth premolar and first molar teeth together. Cone beam computed tomography scans of mesaticephalic dogs were evaluated using third-party viewing software to determine the RSAs of the maxillary canine, fourth premolar, and first molar teeth. The RSA ratios were then calculated for the following comparisons: canine to fourth premolar (C:PM4), canine to first molar (C:M1), and canine to combined fourth premolar and first molar (C:PM4 + M1). Forty-eight dogs and 86 dental arcades met the inclusion parameters. 20.93% of dental arcades had a C:PM4 RSA ratio <1, none of the dental arcades had a C:M1 RSA ratio <1, and all but one arcade (98.81%) had a C:PM4 + M1 RSA ratio <1. Increased weight was significantly correlated with an increase in all RSA ratios. Based on these findings, the authors recommend continuing the practice of bonding the maxillary fourth premolar and first molar teeth together when applying active force orthodontics for the maxillary canine tooth in mesaticephalic patients.
Keywords
Introduction
The root surface area (RSA) of dentition plays a crucial role in orthodontics, particularly, in determining anchorage and the movement pattern of dentition. In the field of orthodontics, the active unit or target unit is the dentition that undergoes the majority of the movement or the desired movement.1–5 The passive or anchorage unit is used to provide resistance to allow movement of the active unit by creating a relatively fixed point of attachment.2–4 Anchorage is a tooth's resistance to movement and is largely influenced by its RSA which determines the surface area of its periodontal ligament. To increase anchorage and prevent undesired movement of the passive unit/anchorage dentition, reinforced anchorage or stationary anchorage can be employed.1,2 Reinforced anchorage involves bonding of adjacent structures together (ie, 2 or more teeth) to increase total attachment area.1,2 Stationary anchorage prevents the bodily movement of the anchorage unit, so that it requires greater force to cause it to move in response to the tipping movement of the active unit.2,4 In dogs, this method is most commonly used to facilitate maxillary canine tooth movement using active force orthodontics by bonding the maxillary fourth premolar and maxillary first molar teeth together.1,6,7
In veterinary dentistry, various conditions may necessitate active force orthodontics for maxillary canine movement. These cases include mesioversion of the maxillary canine teeth, rotation, or a class I or II malocclusion requiring movement of mandibular canine teeth. Such movements often necessitate repositioning of the maxillary canines to allow for an appropriate maxillary diastema suitable to permit atraumatic occlusion of the crown of the ipsilateral mandibular canine. 1 In veterinary dentistry, it is generally accepted that anchorage for an active force appliance used for movement of a maxillary canine tooth requires reinforced anchorage to both the maxillary fourth premolar and the maxillary first molar teeth. However, to the authors’ knowledge, there are no veterinary studies that have directly compared the RSA of these teeth, thus validating this accepted methodology. Previous studies evaluating the RSA of the dog's maxillary fourth premolar and mandibular first molar teeth have been performed using cross sections of extracted cadaver teeth.8,9 To the authors’ knowledge, no in vivo studies employing advanced imaging techniques have been conducted to assess RSA in living patients.
Numerous studies in human dentistry have employed cone beam computed tomography (CBCT) to evaluate RSA.10–14 The use of conventional computed tomography (CT) and, particularly, CBCT has been validated by human dentistry against the previous gold-standard methods of evaluating RSA, namely, 3-dimensional (3D) laser and optical scanning.10,13 Additionally, studies have demonstrated that CBCT images with 0.3 mm slice thickness were found to show no significant difference in the RSA measurement compared to a micro-CT. 3 A key advantage of CBCT over micro-CT is its practicality for use in in vivo clinical cases. Specifically, the third-party viewing softwarea utilized in this study has been extensively validated and utilized for RSA assessment in the field of human dentistry for many years.10,12–17
This study evaluates the RSA of the maxillary canine, fourth premolar, and first molar teeth of mesaticephalic dogs using CBCT. Specifically, it examines the ratios of the RSA of the maxillary canine relative to the RSA of the maxillary fourth premolar, the RSA of the first molar, and the combined RSA of the maxillary fourth premolar and first molar teeth.
Materials and Methods
A 0.3 mm slice thickness CBCT scanb was performed on all anesthetized canine patients presented to the Animal Dental Center in Annapolis, MD, Columbia, MD, Towson, MD, and York, PA in June 2024. Inclusion parameters included mesaticephalic dogs with permanent dentition with at least one maxillary quadrant with a canine tooth, fourth premolar, and first molar tooth present. Facial index (FI) was used to determine skull type regardless of the recorded breed or breed mix. FI was scored using the CBCT in a third party viewing softwarec. FI is measured by skull width multiplied by 100 divided by the facial length. 18 The skull width is measured at the widest part of the skull at the zygomatic arches and the facial length is measured from the nasion to the prosthion. The mean FI for a mesaticephalic patient, brachycephalic patient, and a dolichocephalic patient is 111, 215, and 81, respectively. 18 For this study and in accord with other veterinary studies, a patient with an FI score between 96 and 163 was classified as mesaticephalic. 19 Dogs were excluded from the study if the maxillary canine, fourth premolar, or first molar tooth had evidence of tooth resorption, root fractures, crown root fractures, hypoeruption, or open apices. Additionally, patients with a history of maxillofacial trauma were also excluded from this study. If both maxillary arcades of a patient met the inclusion parameters, both were included in the study.
The CBCT Digital Imaging and Communications in Medicine images were imported into the third-party viewing software. Within the software, each tooth was individually highlighted as an area of interest in the multiplanar reconstruction views (Figure 1). A 3D model of each tooth was then created (Figure 2). In the 3D model, the cementoenamel junction (CEJ) was identified and manually marked. The software subsequently calculated the surface area of the tooth apical to the CEJ to get the overall RSA of each tooth (Figures 3-5).
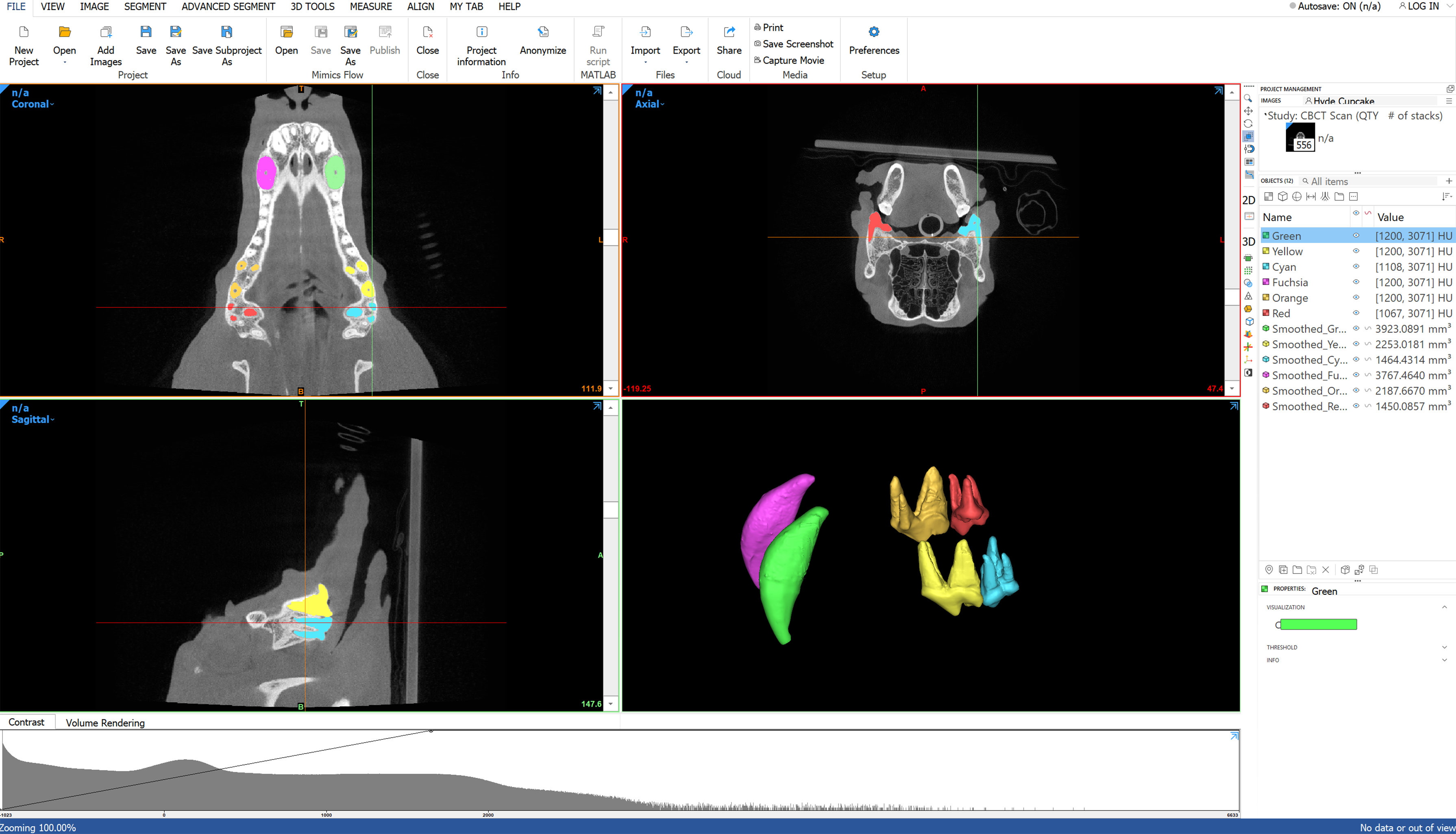
The Maxillary Canines, Fourth Premolars, and First Molar Teeth are Isolated within the Multiplanar View and a 3-Dimensional Model is Created of Each Tooth.
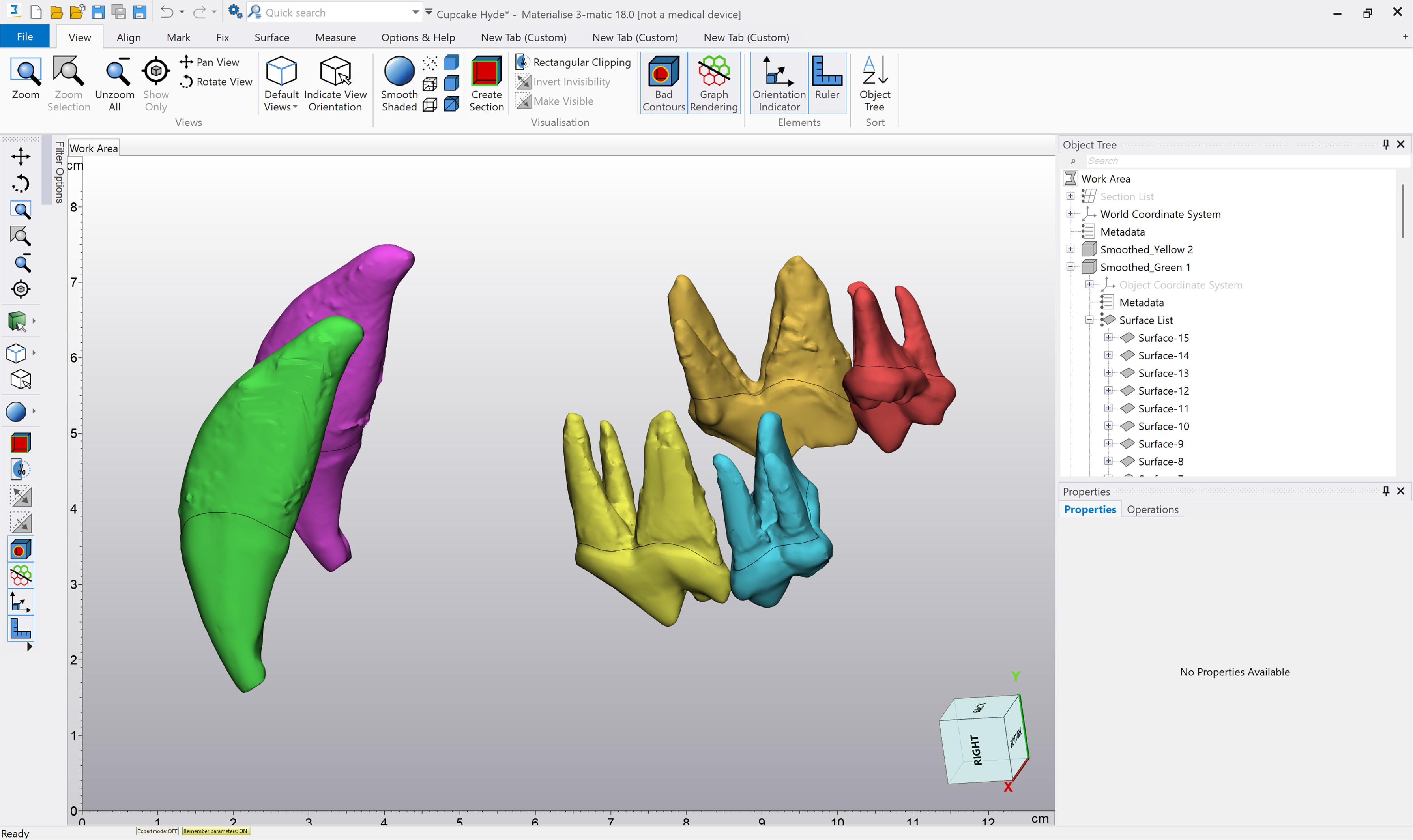
A 3-Dimensional Model of the Left and Right Maxillary Canine, Fourth Premolar, and First Molar was Created.
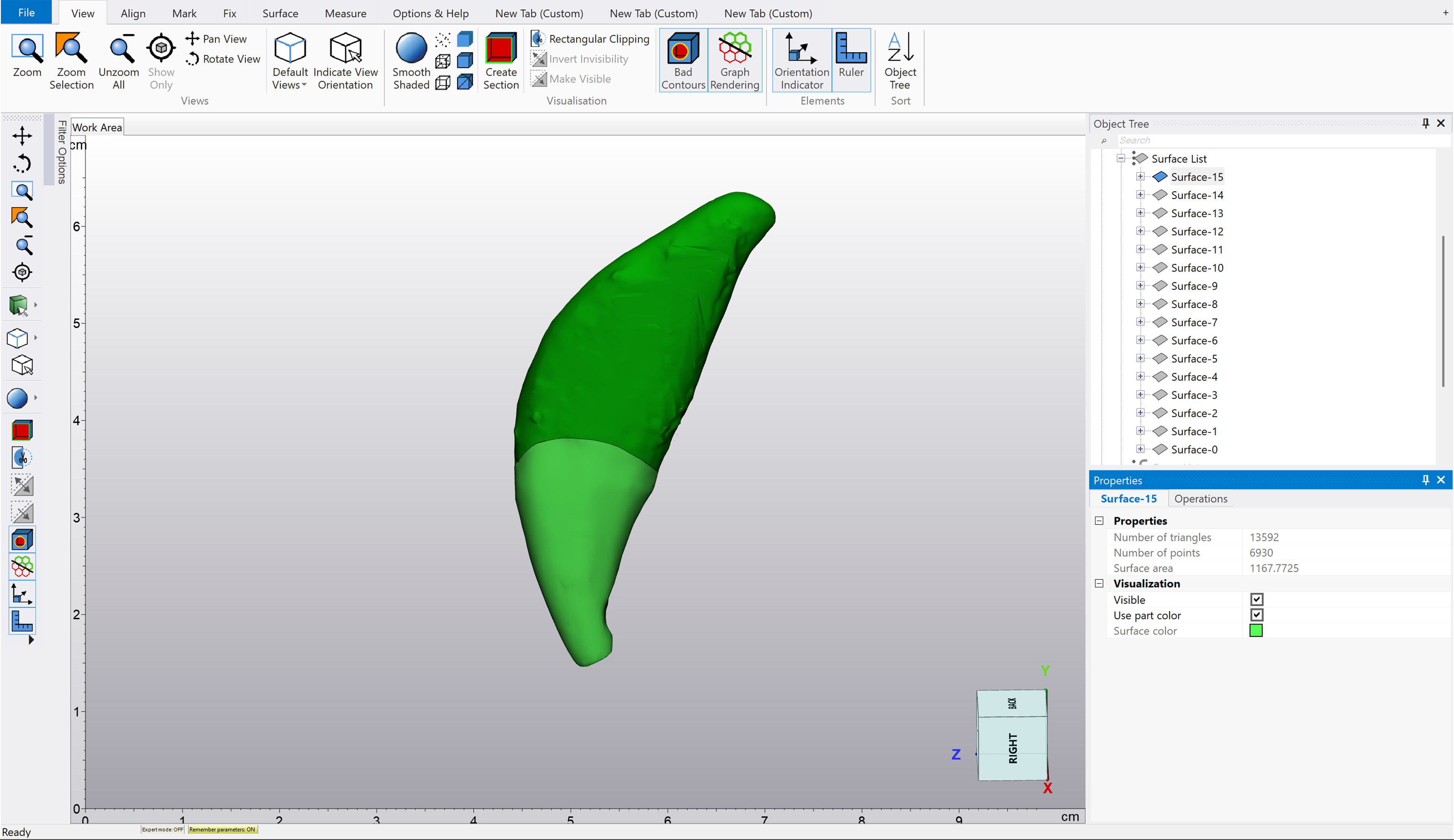
The Cementoenamel Junction of the Left Maxillary Canine (204) was Identified and Only the Radicular Surface was Isolated. The Root Surface Area was then Calculated.
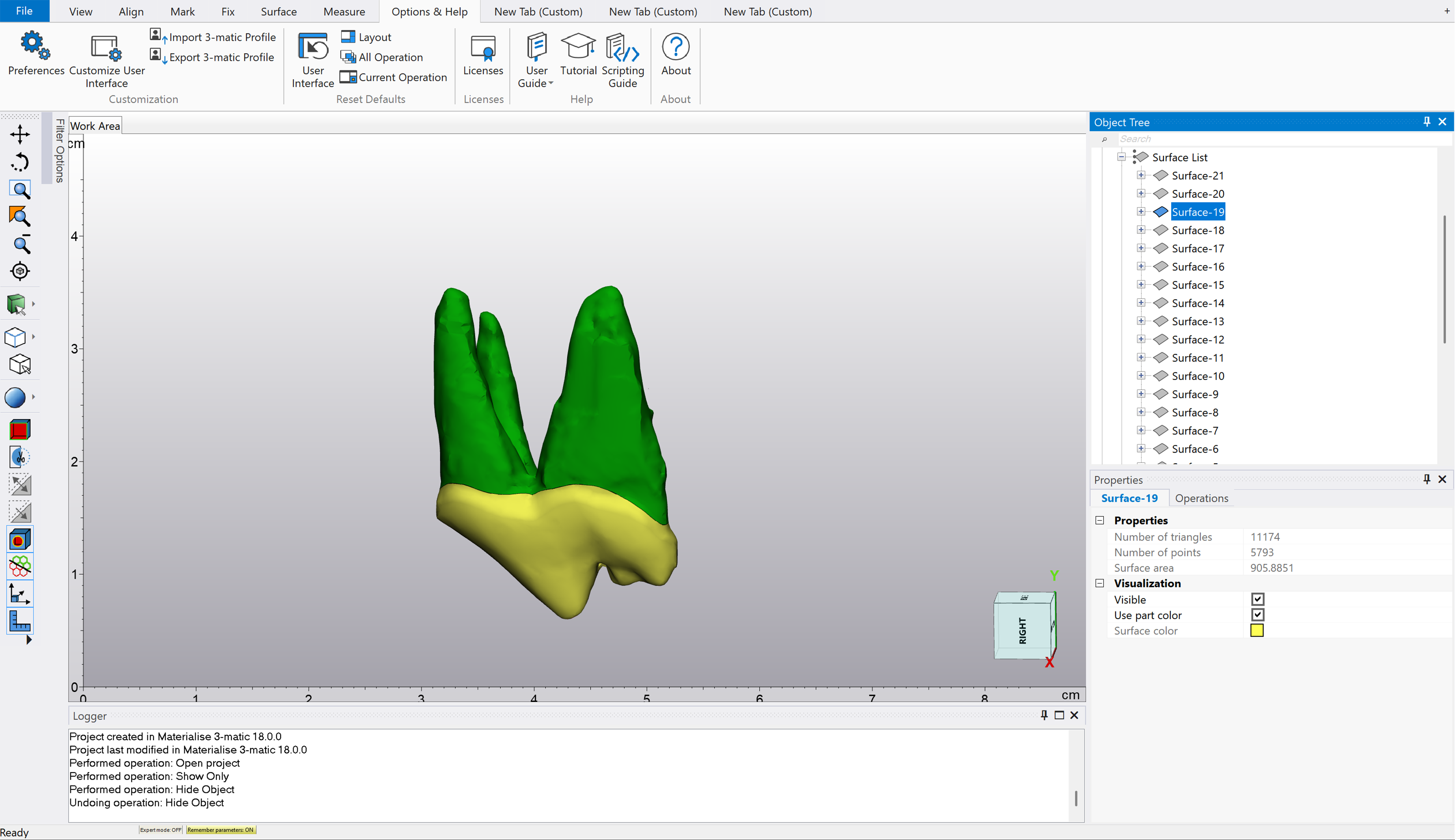
The Cementoenamel Junction of the Left Maxillary Fourth Premolar (208) was Identified and Only the Radicular Surface was Isolated. The Root Surface Area was then Calculated.
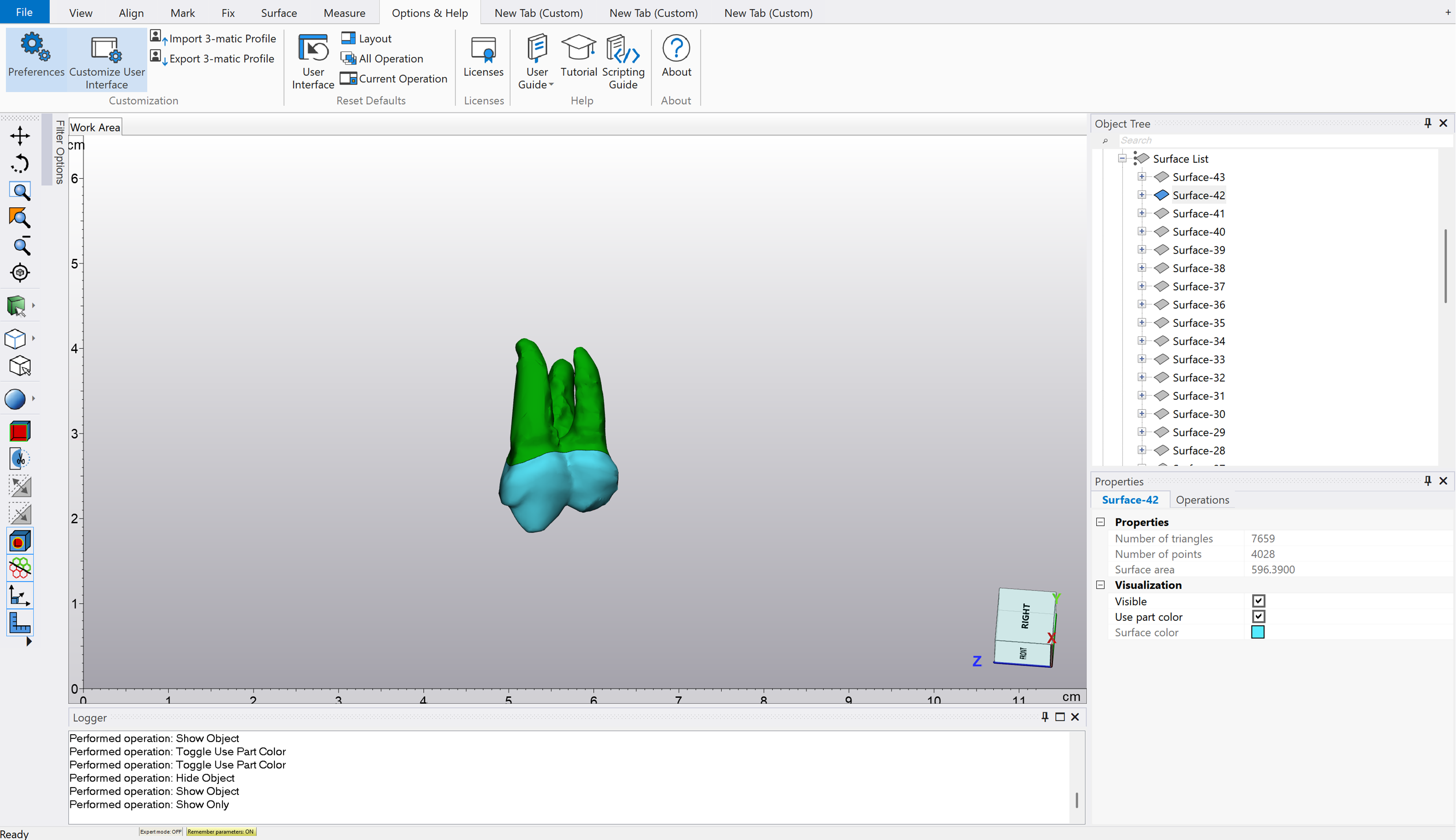
The Cementoenamel Junction of the Left Maxillary First Molar (209) was Identified and only the Radicular Surface was Isolated. The Root Surface Area was then Calculated.
The Shapiro–Wilk test was used to determine normality for weight, age, FI, canine (C) RSA, fourth premolar (PM4) RSA, first molar (M1) RSA, PM4 + M1 RSA, C:PM4, C:M1, and C:PM4 + M1. As most variables were nonparametric, results are reported as medians with corresponding 25th and 75th percentiles. The Spearman rank correlation test was employed to evaluate the correlation between body weight and surface area ratio (significance set at P < .05, −1 = strongest negative correlation, 0 = no correlation, +1 = strongest positive correlation). The Kruskal–Willis test was used to compare significance between tooth RSA for defined weight class groups of <10 kg, 10-25 kg, and >25 kg. The Dunn's multiple comparison test was applied to compare mean differences between the weight classifications (significance set at P < .05).
Results
A total of 130 dogs underwent an anesthetized CBCT scan within the study period. Of these, 48 dogs met the inclusion parameters with a total of 86 dental arcades. The median age of the group was 5 years (range 0.75-13 years). The median weight for the group was 22.5 kg (range 4.34-70.45 kg). The group included 15 dogs <10 kg, 34 dogs 10-25 kg, and 37 dogs >25 kg. Tooth RSA and ratios are summarized in Table 1.
Tooth Root Surface Areas and Ratios.
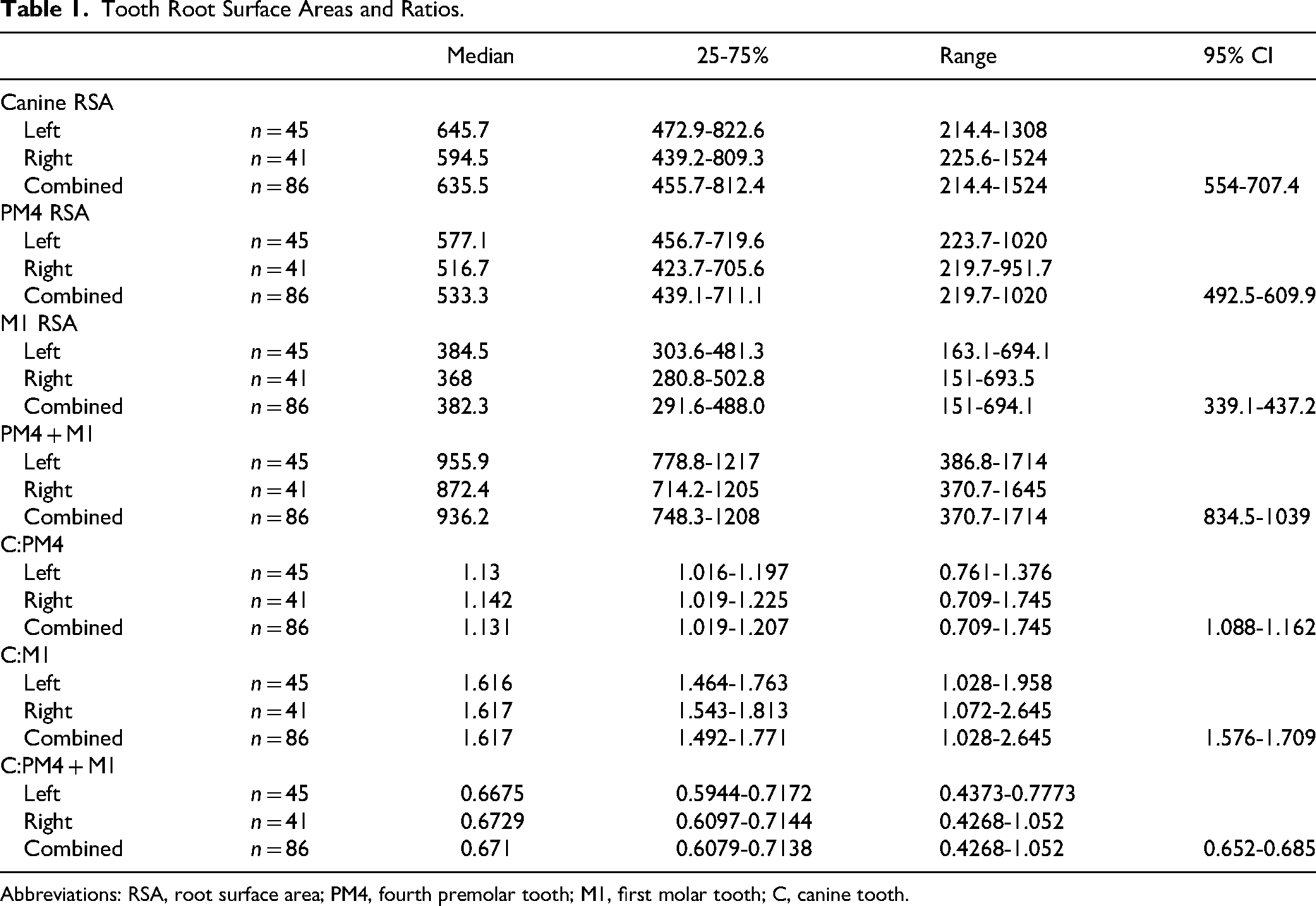
Abbreviations: RSA, root surface area; PM4, fourth premolar tooth; M1, first molar tooth; C, canine tooth.
Among the dental arcades evaluated, 18 dental arcades (20.93%) had a canine to fourth premolar RSA ratio (C:PM4) less than 1. No arcades had a canine to first molar RSA ratio (C:M1) less than 1. All but one arcade (85/86, 98.84%) had a canine to fourth premolar and first molar combined RSA ratio (C:PM4 + M1) less than 1. The single arcade with the C:PM4 + M1 RSA ratio greater than 1 (1.052) also had the contralateral arcade evaluated and the C:PM4 + M1 RSA ratio was less than 1 (0.777).
A significant positive correlation was observed between the increasing body weight and greater tooth RSA ratios for C:PM4 (r = 0.4113, 95% CI [0.2124-0.5775], P < .001), C:M1 (r = 0.4618, 95% CI [0.2712-0.6176], P < .001), and C:PM4 + M1 (r = 0.4463, 95% CI [0.2529-0.6053], P < .001) (Figure 6, Table 2).
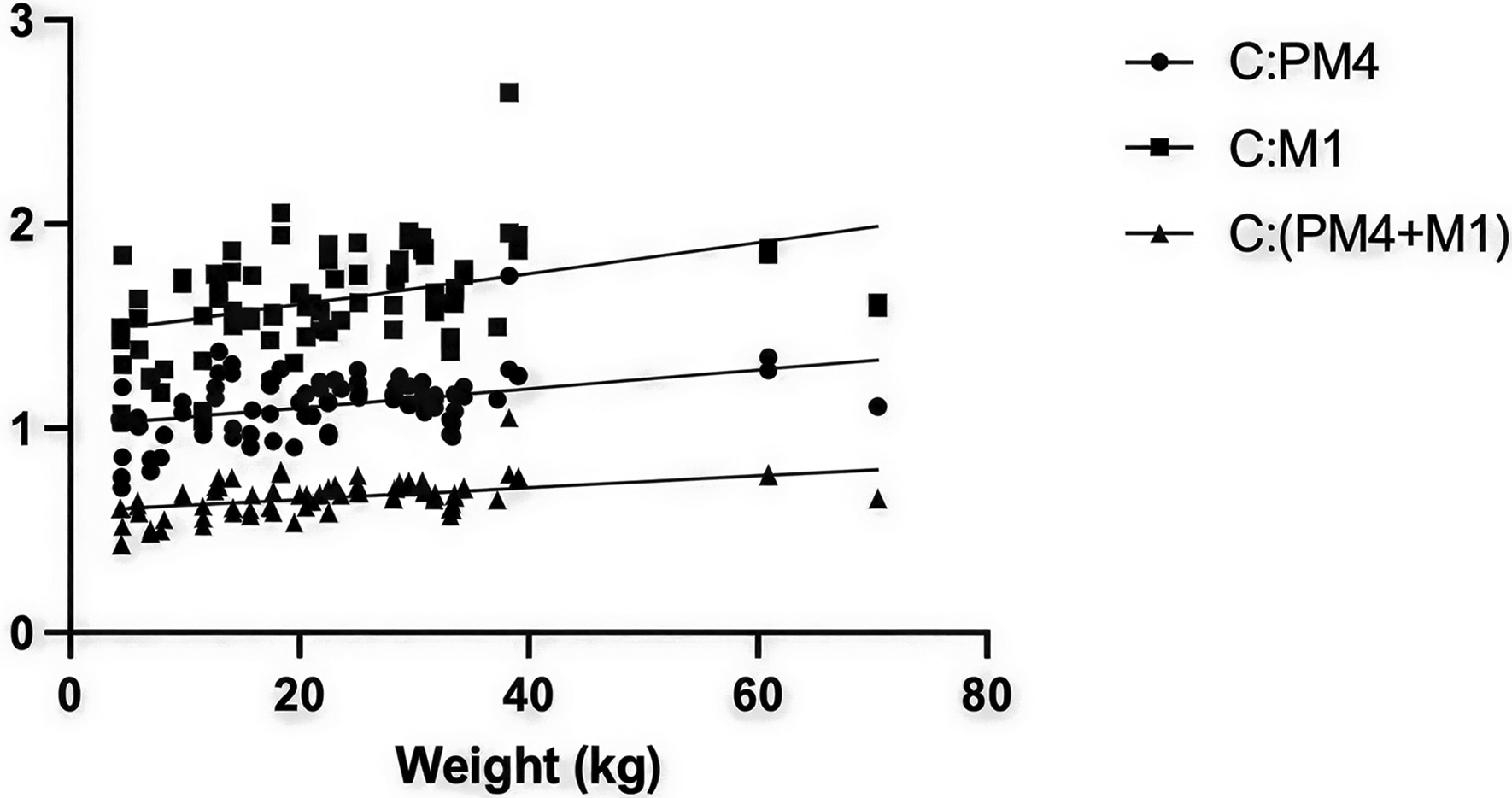
Linear Regression of the Ratios of the Canine Tooth Root Surface Area to Other Dentition by Weight.
Mean Root Surface Area Ratios by Weight Class.
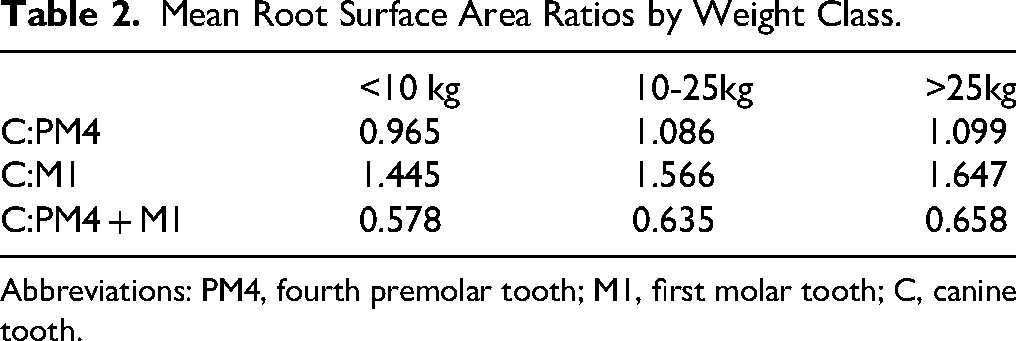
Abbreviations: PM4, fourth premolar tooth; M1, first molar tooth; C, canine tooth.
Among dental arcades from dogs weighing <10 kg, 46.67% had a C:PM4 RSA ratio of less than 1. In the 10-25 kg group, 26.47% had a C:PM4 RSA ratio of less than 1, and in the >25 kg group, 5.40% had a C:PM4 RSA ratio of less than 1.
There was a significant difference in C:PM4 ratios between dogs weighing <10 kg and those in both the 10-25 kg (P = .004) and >25 kg (P < .0001) groups. No significant difference between 10-25 kg and >25 kg groups (P = .3662) was found.
Discussion
In veterinary dentistry, one of the most frequent utilizations of active force orthodontics is in treating malocclusions involving the maxillary canine teeth in dogs. The most common desired movement of the maxillary canine teeth is distal tipping and/or bodily movement. To achieve these movements, it is standard practice to bond the maxillary fourth premolar and maxillary first molar teeth together to increase their combined RSA as an anchorage unit.1,6,7 The maxillary fourth premolar and maxillary first molar teeth can be temporarily bonded together with buttons/brackets, or with composite. This creates an anchorage unit with reinforced anchorage whose RSA is now the combination of both teeth. Anchorage is largely impacted by a tooth's periodontal ligament, and thus, the RSA of a tooth. To the author's knowledge, no previous veterinary studies have been performed comparing the RSA of dentition commonly used for active force orthodontics.
In this study, 79.07% of dental arcades had a C:PM4 RSA ratio greater than 1 indicating that, in these cases, the arcades had a canine tooth anchorage greater than the fourth premolar anchorage. Therefore, if active force orthodontics were applied to these teeth alone, it is likely that the fourth premolar would have iatrogenic orthodontic movement rather than the desired movement of the canine tooth. This undesired movement could include tipping, extrusion, or mesial luxation of the tooth. Conversely, 98.81% of dental arcades had a C:PM4 + M1 ratio less than 1. This suggests that when the fourth premolar and first molar teeth are bonded together for active force orthodontics, the canine tooth would likely exhibit the desired orthodontic movement in the majority of cases.
Significant differences were observed in the RSA ratios with respect to weight. As body weight increased, the ratio of the canine tooth RSA to the fourth premolar, first molar and combined fourth premolar and first molar RSAs increased. However, there was no weight class in which the significant difference in RSA ratios would likely have a clinical impact on treatment planning. Smaller patients, <10 kg, had a higher percentage of dental arcades that had a C:PM1 RSA ratio less than 1 compared to other weight classes. Nonetheless, only 46.67% of these arcades show indications that successful orthodontic movement of the maxillary canine would be achieved if bonded to the maxillary fourth premolar alone.
It is important to exercise caution when directly extrapolating the RSA of a tooth to its anchorage and secondarily, the movement patterns in active force orthodontics. Though the RSA of a tooth due to periodontal ligament attachment is by far the largest contributing factor to anchorage, other factors such as bone density can also play a role in tooth movement. For example, a tooth will more readily move through trabecular bone in comparison to cortical bone. 2 Additionally, tipping movement requires less force than bodily movement.1,2,4 Therefore, distal tipping of the maxillary canine tooth may still be achieved with an imperfect C:PM4 ratio if the appliance is placed near the cusp tip of the maxillary canine.
Since these studies were conducted on clinical patients, the CBCTs were performed prior to any professional scaling of the dentition. Therefore, calculus was present on some teeth. While the CEJ was readily identifiable, some small variation of the RSA may be present due to calculus accumulation on the tooth roots. This study utilized teeth with closed apices. It is important to note that in veterinary medicine, orthodontics in general, and active force orthodontics in particular, are commonly performed on actively erupting permanent teeth, ie, teeth with some degree of open apices. The developing dentition is more readily moved into appropriate, atraumatic occlusion, because the periodontal ligament and alveolar bone are constantly remodeling during the eruption process.2,3 This ensures more predictable results of the desired orthodontic movement. Therefore, some variation in the RSA and ratios from this study compared to generally younger clinical patients requiring active force orthodontics may be present.
The authors recommend continuing the common practice of bonding the maxillary fourth premolar and first molar teeth together as a passive unit with reinforced anchorage when applying active force orthodontics to create tipping movement of the maxillary canine tooth in mesaticephalic dogs.
Future studies are needed to evaluate the RSA ratios for both brachycephalic and dolicocephalic patients.
Materials
Mimics and 3-Matic Innovation Suite, Materialise, Leuven, Belgium.
VetCAT and VetCAT IQ, Xoran, Ann Arbor, MI, USA.
Invivo 7, Osteoid, Santa Clara, CA, USA.
Footnotes
Acknowledgments
The authors would like to thank Rebecca Windsor, DVM, DACVIM for her assistance with the statistical analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.