
Abstract
Canine oral lymphoma is an uncommon neoplasm that mimics inflammatory or immune-mediated oral diseases as well as other round-cell tumors, complicating diagnosis and potentially delaying treatment. The objective of this study was to describe the clinical presentation, behavior, and outcomes of canines diagnosed with oral lymphoma, including epitheliotropic and nonepitheliotropic forms of the disease. A retrospective review of 75 cases diagnosed between 2019 and 2022 was performed, evaluating histologic categorization, lesion characteristics (solitary vs multifocal, anatomic location, and descriptors), and survival data when obtainable. There were 73 cases (97.3%) of epitheliotropic T-cell lymphoma (ETCL), 1 case (1.3%) of lingual T-zone lymphoma, and 1 case (1.3%) of peripheral T cell lymphoma-not otherwise specified. The most common anatomic locations for ETCL were the mucocutaneous junction (65.3%) and buccal or labial mucosa (62.7%). Lesions affecting the mucocutaneous junction were commonly located on the mandibular labial frenulum (61.2%), and 46.7% of mandibular frenulum lesions were the only lesions present in the oral cavity. Lesions associated with ETCL were likely to be multifocal (57.3%) and ulcerated (62.8%). Patient survival was not significantly associated with lesion number (solitary vs multifocal) among epitheliotropic cases. These findings indicate that canine oral lymphoma is predominantly epitheliotropic and frequently multifocal, underscoring the importance of biopsy and histopathologic evaluation of oral tissues exhibiting subtle mucosal changes such as erythema or depigmentation. Adjunctive diagnostics, including immunohistochemistry, flow cytometry, and polymerase chain reaction for antigen receptor rearrangements, may facilitate earlier detection. Prospective studies are warranted to clarify disease progression, treatment response, and prognosis.
Keywords
Introduction
Oral cancer is responsible for approximately 6% of all canine cancers. 1 Oral lymphoma is uncommon and accounts for roughly 4% to 5% of all canine oral tumors. 2 In general, middle-aged to older dogs are more likely to develop lymphoma regardless of anatomic location.3,4 Lesions are typically multifocal and clinically characterized by erythema, hypopigmentation/depigmentation, ulcerations, and plaques,5,6 although solitary and/or solid mass lesions have been reported. 7 Oral lymphoma can occur within the oral mucosa, bones of the skull containing teeth, and lymphoid tissues of the mouth, including the tonsils. 2 Lesions within the oral cavity can represent systemic lymphoid neoplasia or local extension of lymphoma from the skin, nasal passage, philtrum, mucocutaneous junction, and lip. 2 Oral lymphoma commonly occurs as a multicentric disease, with additional sites of involvement reported in the skin, lungs, gastrointestinal tract, and lymph nodes. 2 Due to the similarities in the clinical appearance of oral lymphoma with nonneoplastic inflammatory lesions, oral lymphoma must be included as a differential for oral inflammatory lesions such as erythema multiforme, canine chronic ulcerative stomatitis, and lupus erythematosus.8,9 In its early stage, it can also look very similar to stomatitis or periodontal disease especially in older pets, 10 which can lead to a delay in diagnosis.
Lymphoma is a round cell neoplasm that comprises various lineages of lymphocytes.1–3 Classifying lymphoma is based on anatomic location, histomorphology, and immunophenotyping.2,3 T-cell lymphoma is commonly multicentric or disseminated, and it can be found in the gastrointestinal tract, mediastinum, lymphatic system, and cutaneous tissue. Histologic classification currently follows the Revised European American Lymphoma/World Health Organization (REAL/WHO) system.2,3 Immunophenotyping is conducted by identifying specific antigens expressed by lymphocytes. 2 This is commonly performed using immunocytochemistry, immunohistochemistry, or flow cytometry. Expression of CD3, which is a cell surface protein that binds the T cell receptor, supports a diagnosis of T-cell lymphoma.2,4 Other proteins are expressed by B lymphocytes including CD20 (a cell surface protein), CD79a (a transmembrane protein), and Pax-5 (a nuclear transcription factor).2–4 Expression of CD20, CD79a, or Pax-5 generally supports B-cell lymphoma, although T-cell lymphomas may express some B-cell antigens. 5 When diagnosing T-cell lymphoma in the oral cavity, it is important to consider other mucosal round cell tumors (ie, plasma cell tumor, mast cell tumor, melanoma, transmissible venereal tumor) that may present similar histologic features. 1 This emphasizes the critical role of histologic evaluation and confirmatory testing.
Epitheliotropic T-cell lymphoma (ETCL) is characterized by neoplastic lymphocytes that infiltrate epithelium including mucosal epithelium (oral cavity and other mucosal surfaces) and epithelium of the skin (epidermis, hair follicles, and other adnexal structures). Subtypes of ETCL include pagetoid reticulosis (PR), mycosis fungoides (MF), and Sézary syndrome.2,6,7 PR is characterized by striking epitheliotropism of neoplastic T lymphocytes with minimal dermal involvement. 6 In MF, neoplastic T lymphocytes exhibit epitheliotropism and infiltrate the dermis (or mucosal lamina propria) to form plaque or tumoral lesion(s). 6 Sézary syndrome is a unique leukemic form of ETCL within neoplastic T lymphocytes in peripheral blood as well as cutaneous, mucocutaneous, or mucosal lesions similar to MF. 8 MF is the most common subtype of ETCL in both humans and dogs while PR and Sézary syndrome are more obscure and potentially underdiagnosed forms of the disease.4,6 Since PR and Sézary syndrome are not routinely diagnosed in dogs, the misperception that ETCL is synonymous with MF is a common point of confusion. 9
Lingual T-zone lymphoma has been described in dogs. 10 Other types of nonepitheliotropic T-cell lymphoma in dogs include anaplastic large T-cell lymphoma (ALTCL) and peripheral T-cell lymphoma-not otherwise specified (PTCL-NOS). 7 Differentiating between ETCL and other forms of T-cell lymphoma is essential for proper diagnosis and prognostic guidance. 7 This is achieved through histopathological evaluation of cell morphology, organization of neoplastic cells, and determination of immunophenotype.6,11
Some larger studies of canine cutaneous epitheliotropic T-cell lymphoma have shown oral mucosal involvement.7,12 Lesions in the mucosa were more likely to be erythemic (53%), swollen (47%), and eroded (47%). 7 Prognostically, younger dogs, solitary lesions, and a diagnosis of nonepitheliotropic lymphoma were associated with longer median survival times.7,12 Lesion-based clinical staging of ETCL uses the following categories: premycotic, mycotic, and tumoral. According to one study, mucosal ETCL lesions were typically mycotic stage (41.4%) and solitary. 12 Additionally, though not statistically significant due to the limited number of cases, dogs with mycotic stage lesions had shorter survival times compared to dogs with premycotic lesions. 7
Canine ETCL and nonepitheliotropic cutaneous T-cell lymphoma have been described in the literature,5,6,12 but few reports have focused solely on oral manifestations.13,14 These reports are limited to only a handful of cases that highlight the difficulty in diagnosing this neoplasm due to its variation in clinical appearance. Therefore, the aim of this study was to retrospectively evaluate the records of canine oral T-cell lymphoma patients to determine clinical characteristics, histopathologic features, behavior, and outcomes of this neoplasm.
Materials and Methods
Study Population
The database of Specialty Oral Pathology for Animals (SOPA) was searched for the diagnosis of lymphoma in canine oral biopsy samples from January 2019 to December 2022. Inclusion required oral location of the lesion(s), including the mucocutaneous junction of the lips but excluding lymphoid tissue of the tonsil. The search yielded 93 cases, some of which included lymphoma as a differential diagnosis. Thirteen round cell tumors were excluded because immunohistochemistry (IHC) did not support the diagnosis of lymphoma or IHC had not been performed. Two cases of suspected epitheliotropic lymphoma were excluded because confirmatory polymerase chain reaction for antigen receptor rearrangements (PARR) testing was considered necessary for definitive diagnosis but not performed. Three cases of tonsillar lymphoma (all high-grade B cell) were excluded. A total of 75 cases of canine oral lymphoma were identified for the study.
Patient Clinical Data
Information obtained from pathology submission requests included patient signalment (breed, age, sex), number of lesions (solitary vs multifocal), oral lesion location(s), nonoral lesion location(s), and description of gross lesion(s). Diagrams and pictures submitted with the pathology request depicting the oral lesions were evaluated to ascertain/confirm lesion location(s). The oral cavity was divided into 7 areas to describe lesion location(s): mucocutaneous junction, buccal/labial mucosa, tongue, lingual mucosa (mucosa within the intermandibular space and lateral to the base of the tongue), hard palate, oropharynx, and gingiva. For solitary masses that extended across multiple locations, all affected locations were recorded. In cases involving the mucocutaneous junction, involvement of the mandibular labial frenulum was also documented if present.
Referring veterinarians were contacted to obtain medical records of the oral lymphoma patients identified. When records were provided, clinical history, metastatic regional lymph node involvement, and outcomes were recorded. When lesions outside of the oral cavity were present, the affected skin or other mucocutaneous/mucosal areas, along with the specific location, were noted. In cases where outcome information was available, cases were placed into 1 of 4 categories: alive, euthanized due to oral lymphoma sequelae, euthanized for reasons not related to lymphoma, or lost to follow-up. Time between diagnosis and data collection or euthanasia was recorded. Information regarding patient treatment(s) was not available.
Histology and Immunohistochemistry Examination
Oral biopsies were formalin-fixed and processed routinely, embedded in paraffin, sectioned, and stained with hematoxylin and eosin. Histologic sections from at least 1 lesion from each patient were evaluated. The diagnosis was established by either histomorphology alone or histomorphology with confirmation by IHC. Histomorphology alone was considered sufficient only for a subset of epitheliotropic lesions that had a monomorphic population of small to intermediate-sized lymphocytes and formation of a plaque or mass lesion. Remaining cases, including all nonepitheliotropic cases, were confirmed by IHC. Diagnosis was based on World Health Organization criteria as 1 of the following: ETCL, ALTCL, lingual T zone lymphoma (LTZL).10,11 Subtypes of ETCL (PR, MF, and Sézary syndrome) were not assigned due to limited and inconsistent clinical information.
The ETCL cases were also classified based on the histologic distribution of neoplastic T lymphocytes as epithelium only, mucosa only, or deep/tumor. Epithelium-only lesions had neoplastic T lymphocytes limited to the epithelium. Mucosa-only ETCL lesions had neoplastic cells within the mucosal epithelium and lamina propria with or without mass effect. Deep/tumor ETCL lesions had a distinct mass effect with neoplastic cells invading deep to the mucosal lamina propria, generally involving the submucosa and/or skeletal muscle. For ETCL cases with multiple lesions sampled for histopathology, the deepest lesion was used for classification based on the assumption that the depth of invasion was greater for more advanced lesions. Nuclear size was recorded relative to the diameter of erythrocytes, and mitotic count was performed by enumeration of mitotic figures within 10 contiguous high-power fields (2.37 mm2). All histopathological interpretations were performed by a board-certified veterinary pathologist.
Immunostaining for CD3 was performed on 5 µm-thick sections of paraffin-embedded tissue with the BenchMark Ultra platforma. Sections were deparaffinized, rehydrated, and antigen retrieval was performed in a prediluted Tris-based bufferb with incubation at 95°C for 36 min. Slides were incubated for 40 min with a prediluted rabbit antihuman CD3 monoclonal antibodyc. The antibodies were visualized using a prediluted goat-antimouse/rabbit secondary antibody, a horseradish peroxidase complex, and 3,3-diaminobenzidine substrated. A section of human tonsil was used as the positive control, while no primary antibody was used for the negative controls. IHC for CD3 was performed on a subset of cases, including those with equivocal histologic features and when specifically requested by the clinician. All IHC evaluations were performed by a board-certified veterinary pathologist.
Statistical Analysis
The statistical analysis of the results was performed by a statistician within the Department of Clinical Sciences at Colorado State University. The categorical data were described using counts and percentages. Patient demographics and survival data were analyzed using a chi-square test. If any of the categories had counts ≤5, it was analyzed using a Fisher's exact test. A P-value of <.05 was used as a criterion to determine statistical significance. Statistical analysis sytem (SAS) v9.4e was used to analyze all data.
Results
Study Population
Patient information can be found in Table 1. The median age at the time of diagnosis was 11 years (range 7.4-16 years). Thirty-nine dogs (52%) were neutered males, 34 dogs (45.3%) were spayed females, and 2 dogs (2.7%) were intact males. The sex ratio of males to females was 1.2:1, and it was determined that sex was not associated with disease development. There were 32 breeds identified, with mixed-breed dogs being the most common (23/75; 30%). Beagles (5/75; 6.7%) were significantly (P = .002) overrepresented among dogs with oral lymphoma when compared to the database population without oral lymphoma (184/15,803; 1.2%).
Summary Information of Patient Signalment, Lesion Distribution, and If Follow-Up Was Attained.
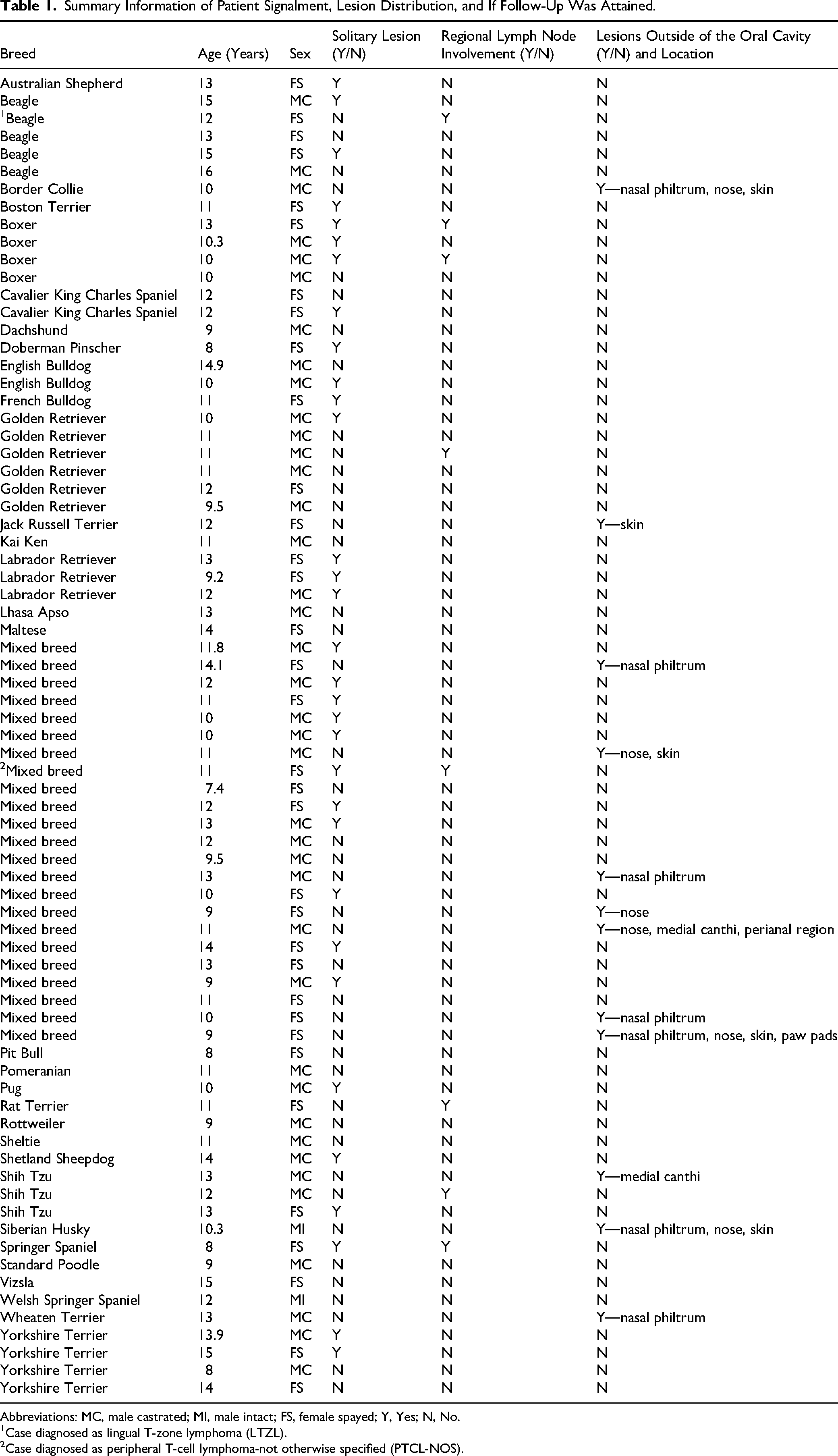
Abbreviations: MC, male castrated; MI, male intact; FS, female spayed; Y, Yes; N, No.
Case diagnosed as lingual T-zone lymphoma (LTZL).
Case diagnosed as peripheral T-cell lymphoma-not otherwise specified (PTCL-NOS).
Histologic Classification
Of the 75 cases, 73 (97.3%) were diagnosed as ETCL, 1 (1.3%) was LTZL, and 1 (1.3%) was PTCL-NOS (Table 2). The histologic category of ETCL cases was specified as deep/tumor (62/73, 84.9%), mucosa only (11/73, 15%), or epithelium only (0/73). Dogs with multifocal distribution of disease often had lesions in more than 1 category. Some cases recorded as mucosa only had epithelium only lesions, and cases recorded as deep/tumor may have also had additional mucosa-only and/or epithelium-only lesions. Figures 1 to 3 illustrate the histologic and clinical differences. Five mucosa-only lesions lacked a discernible mass effect, and neoplastic cells within the lamina propria were sparse. For these cases, IHC confirmed expression of CD3 by neoplastic cells. Additionally, Figure 3 demonstrates how epitheliotropism can be inconsistent. For mucosa-only ETCL lesions, the mitotic count ranged from 0 to 5 figures per 10 high-power fields (2.37 mm2), and the mean was 1.2 figures. For deep/tumor lesions, the mitotic count ranged from 0 to >100 figures per 10 high-power fields (2.37 mm2), and the mean was 27.6 figures. Of the ETCL cases, all had cells with small to intermediate-sized nuclei that were 1.5-2× the diameter of an erythrocyte.

Clinical And Histologic Images Of An Epithelium-Only ETCL Lesion In A 9-Year-Old Dachshund. (A, B) Arrows Depicting Lesions That Were Described As Cobblestone Mucositis And Severe Gingivitis In The Pathology Submission Request, Respectively. (C) Neoplastic Lymphocytes Are Confined To The Mucosal Epithelium (Bracket) With Rare Cells In The Lamina Propria. HE Stain, Bar = 200 μm. (D) Neoplastic Lymphocytes Have Positive Expression Of CD3, Confirming T-Cell Lineage. IHC Staining Helps To Highlight The Abundance Of Neoplastic Cells Within The Epithelium (Bracket). IHC For CD3, Bar = 200 μm.

Clinical And Histologic Images Of A Mucosa-Only ETCL Lesion In A 15-Year-Old Yorkshire Terrier. (A) The Lesion Is Characterized By Swelling And Erythema Of The Left Mandibular Frenulum. (B) Neoplastic Lymphocytes Account For Cellular Infiltrates Throughout The Mucosal Lamina Propria, While Involvement Of The Epithelium (Bracket) Is Not Obvious. HE Stain, Bar = 200 μm. (C) Positive Immunohistostaining For CD3 Confirms T-Cell Lineage Of Neoplastic Lymphocytes And Helps To Illustrate Epitheliotropism, Where CD3-Positive Neoplastic Cells Are Abundant In Basilar Layers Of The Epithelium (Bracket). IHC For CD3, Bar = 200 μm.

Clinical And Histologic Images Of ETCL In A 10-Year-Old English Bulldog. (A) Several Small Lesions (White Arrows) Are Present Within The Mucosa That Surrounds A Larger Erythemic Mass (Black Arrow). (B) Histologic Image Of A Mucosa-Only Lesion With Neoplastic Lymphocytes Throughout The Lamina Propria And Basilar Layers Of The Epithelium (Bracket). HE Stain, Bar = 200 μm. (C) The Larger Deep/Tumor Lesion Has Neoplastic Lymphocytes Infiltrating And Expanding The Deep Lamina Propria And Submucosa. However, There Is No Apparent Epitheliotropism. Bracket Indicates The Epithelial Layer. HE Stain, Bar = 200 μm. (D) In The Deep/Tumor Lesion, Neoplastic Cells Have Positive Expression Of CD3 And The CD3-Positive Cells Are Absent From The Epithelium (Bracket). IHC For CD3, Bar = 200 μm.
Subtypes of Canine T-Cell Lymphoma in the Oral Cavity.
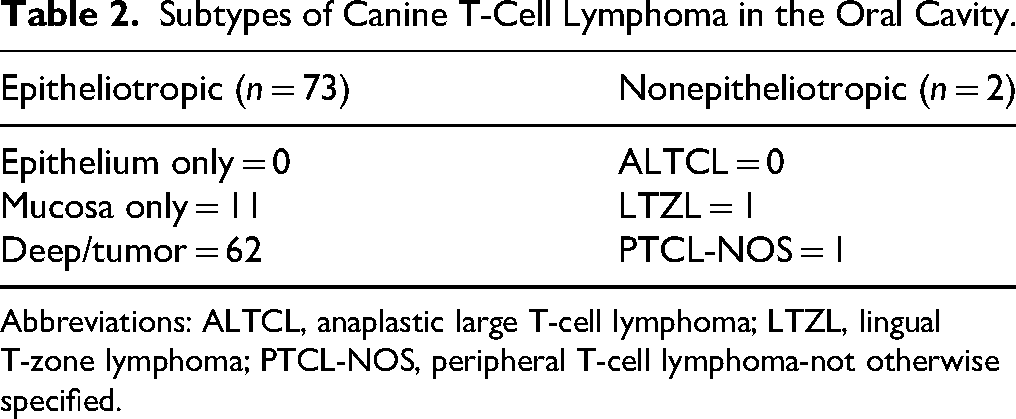
Abbreviations: ALTCL, anaplastic large T-cell lymphoma; LTZL, lingual T-zone lymphoma; PTCL-NOS, peripheral T-cell lymphoma-not otherwise specified.
The LTZL lesion was from a 12-year-old, spayed female Beagle with multifocal to coalescing, fleshy masses within the muscle of the tongue. Histologically, diffuse sheets of neoplastic round cells had nuclei that were 1.5× erythrocyte diameter and small amounts of clear cytoplasm. The mitotic count was 22 figures per 10 high-power fields (2.37 mm2). 10 Morphologically, these cells looked very much like cells of a typical ETCL lesion, although epitheliotropism was not evident. This patient had a previous diagnosis of T-zone lymphoma supported by cytopathologic evaluation and flow cytometry on an aspirate from the ipsilateral mandibular lymph node. A diagnosis of lingual T-zone lymphoma was given for the biopsy from the tongue based on the previous lymph node evaluation and striking clinical similarity to published cases of LTZL in dogs. 10
The PTCL-NOS lesion was a buccal mucosal mass in an 11-year-old, spayed female, mixed-breed Corgi dog. Histologically, diffuse sheets of small cells infiltrated the mucosa and submucosa, extending into the skeletal muscle. Grossly, the mass was 2.3 × 2.2 × 1.1 cm. The neoplastic cells had scant cytoplasm and nuclei that were approximately the same diameter as an erythrocyte. The mitotic count was 0 figures per 10 high-power fields (2.37 mm2). Immunohistochemical evaluation revealed numerous small CD3+ lymphocytes, interpreted as neoplastic T-cells, interspersed with larger CD3− cells throughout. The same population of CD3-positive small lymphocytes was partially effacing the ipsilateral mandibular lymph node.
Positive expression of CD3 was confirmed for 24 (32.9%) of the ETCL cases and for both the LTZL and PTCL-NOS cases. IHC was not pursued for 49 (67.1%) of ETCL cases for which a confident diagnosis was based on unequivocal histopathologic features and supportive clinical presentation.
Lesion Location and Characteristics
Lesion distribution within the oral cavity is portrayed by Figures 4 and 5. Overall, solitary and multifocal lesions were located within the mucocutaneous junction (49/75, 65.3%), buccal/labial mucosa (47/75, 62.7%), gingiva (30/75, 40%), hard palate (11/75, 14.6%), tongue (9/75, 12%), lingual mucosa (9/75, 12%), and the oropharynx (2/75, 2.6%). Of the 49 lesions that were affecting the mucocutaneous junction, 30 (61.2%) were located on the mandibular labial frenulum. Fourteen (46.7%) of the 30 lesions affecting the mandibular labial frenulum were the only lesions present in the oral cavity. Thirty-two dogs (32/75, 42.7%) had solitary lesions. Solitary lesions were located at the mucocutaneous junction (19/32, 59.4.%), buccal/labial mucosa (11/32,34.4%), gingiva (7/32, 21.9%), lingual mucosa (4/32, 12.5%), tongue (1/32, 3.1%), and the hard palate (1/32, 3.1%). Nine of the solitary lesions were large enough to be included in multiple location categories; therefore, the values in the previous sentence total greater than 32 lesions (100%). Four solitary lesions were large enough to affect both the mucocutaneous junction and the adjacent buccal mucosa (4/32, 12.5%). Forty-three dogs (57.3%) had multifocal lesions. Multifocal lesions were located at the buccal/labial mucosa (35/43, 81.4%), mucocutaneous junction (30/43, 69.8%), gingiva (23/43, 53.5%), hard palate (10/43, 23.3%), tongue (8/43, 18.6%), lingual mucosa (5/43, 11.6%), and the oropharynx (2/43, 4.7%).
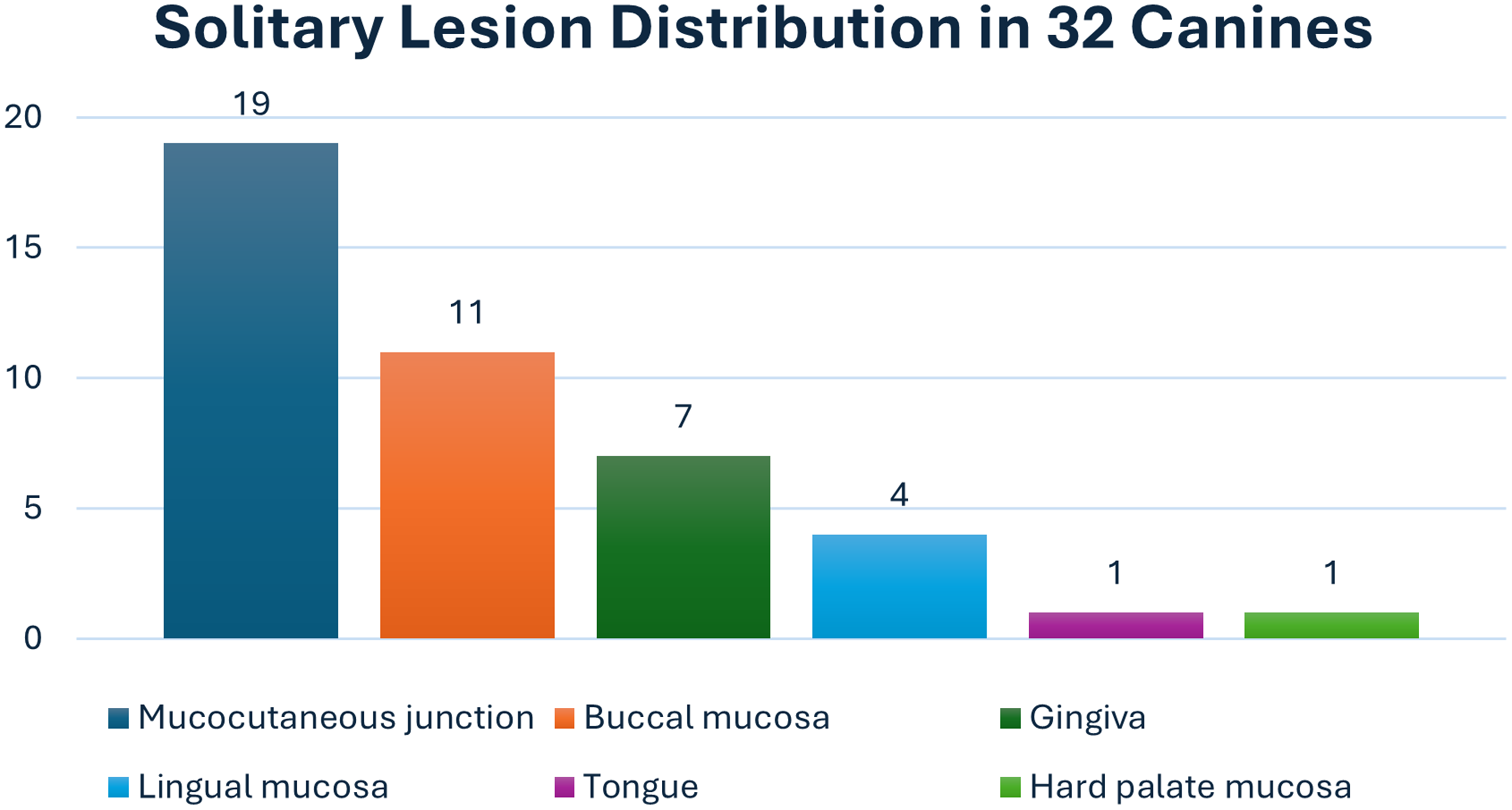
Bar Graph Showing Solitary Lesion Distribution Among Anatomical Regions Evaluated. Nine Lesions Were Large Enough To Impact More Than One Anatomical Location. No Solitary Lesions Were Present In The Oropharynx (Excluded From This Bar Graph).
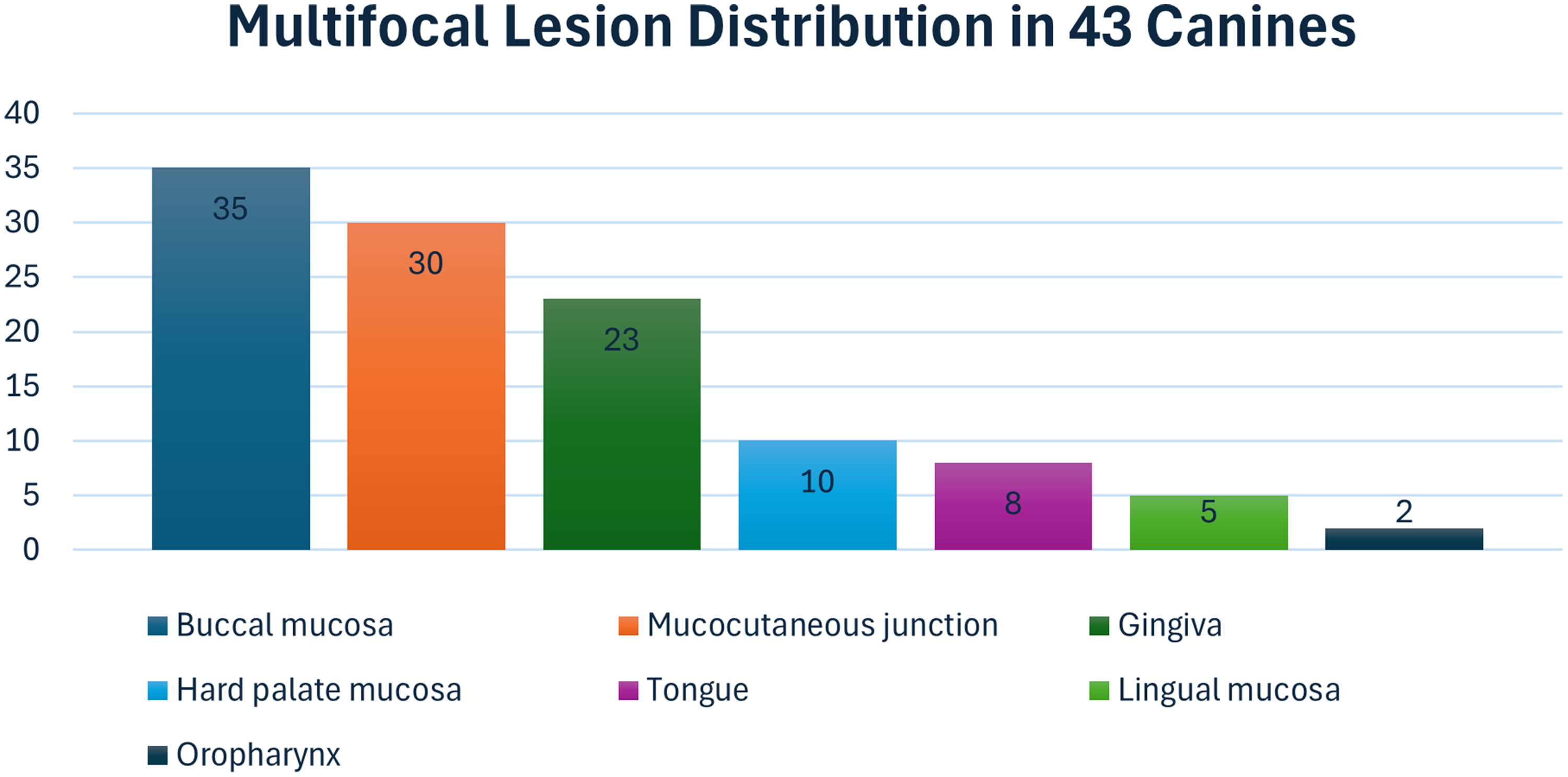
Bar Graph Showing Multifocal Lesion Distribution Among The Anatomical Regions Evaluated.
Gross lesion characteristics were based on pathology submission forms. Solitary lesions were more likely to be described as mass-like (17/32, 53.1%), erythematous/red (12/32, 37.5%), ulcerated (10/32, 31.3%), pink (6/32, 18.8%), and/or raised (6/32, 18.8%). Multifocal lesions were more likely to be described as ulcerated (27/43, 62.8%), mass-like (12/43, 27.9%), erythematous/red (11/43, 25.6%), thickened (11/43, 25.6%), swollen (6/43, 13.9%), raised (5/43, 11.6%), depigmented (4/43, 9.3%), friable (4/43, 9.3%), and/or plaque-like (3/43, 6.9%). Figure 6 depicts the wide range of clinical presentations of lymphoma in the oral cavity.

Clinical Appearance Of 4 Different Oral ETCL Lesions. (A, B) Multifocal, Erythemic Lesions Of The Gingiva And Mandibular Mucocutaneous Junction In An 11-Year-Old Golden Retriever. (C) Solitary Lesion Affecting The Right Mandibular Frenulum. The Lesion Is Large Enough That It Extends From The Mucocutaneous Junction Into The Buccal Mucosa In A 12-Year-Old Mixed-Breed Dog. (D) Diffuse Lymphoma Involving The Tongue, Characterized By A Mass Lesion On The Rostral Lateral Aspect, In A 15-Year-Old Vizsla.
Regional lymph node and distant, nonoral lesion status was not provided for every submission. In submissions where regional lymph nodes were mentioned (12), 4 reported an enlarged mandibular lymph node, 5 reported mandibular lymph node metastasis, and 3 reported metastases to a regional lymph node but did not specify the location. Metastases of these lymph nodes were either confirmed via histopathology through SOPA (6) or through flow cytometry (1) and fine needle aspirate and cytology (1) performed by the referring veterinarian. Of the 8 dogs that had regional lymph node involvement, 4 (50%) had solitary lesions, and 4 (50%) had multifocal lesions. For 12 dogs that had reported nonoral lesions, affected sites included the nasal philtrum (7), nose (6), skin (5), medial canthi (2), perianal region (1), and paw pads (1). All 12 cases with distant, nonoral lesions had multiple oral lesions. Five of the cases with nonoral lesions had multiple distant lesions. The primary site for disease development could not be determined for cases with nonoral lesions. One dog was reported to have a previous diagnosis of lymphoma, but timing, location, and treatment of the disease were not provided.
Patient Survival
Information regarding the patient's postdiagnosis status was available for 35 cases (46.7%) (Table 3). At the time of data collection, 26/35 (74.2%) dogs were alive, with a median diagnosis to data collection time interval of 669 days (range 354-1060). Two cases with regional lymph node involvement were alive (447 and 867 days) at the time of data collection. Seven of the 35 cases (20%) were euthanized due to oral lymphoma sequelae, and 2 cases (5.7%) died due to other disease processes. Both dogs that died due to unrelated disease processes had deep/tumor ETCL lesions. Euthanasia dates were available for 6 of the 7 dogs that were euthanized due to oral lymphoma sequelae; the median time to euthanasia among these dogs was 115 days (range 11-377). Of the 7 cases euthanized due to oral lymphoma sequelae, 3 had solitary lesions, and 4 had multifocal lymphoma. There was no statistically significant difference in survival between dogs with solitary lesions and those with multifocal lesions. When assessed by histologic distribution of lesions, 21/35 (60%) dogs had deep/tumor ETCL and were alive at the time of data collection with a median time of 657 days (range 354-872). The median time to euthanasia for 5 of the 6 dogs euthanized due to oral lymphoma sequelae with deep/tumor ETCL was 110 days (range 11-377). Five of the 35 cases (14.3%) had mucosa-only ETCL and were also alive at the time of data collection with a median time of 825 days (range 607-1060). One dog with mucosa-only lesions died due to oral lymphoma at 120 days. There was no statistically significant difference in survival between dogs with mucosa-only and deep/tumor lesions of ETCL.
Summary of Survival From Time of Diagnosis to Data Collection for 34 Patients.
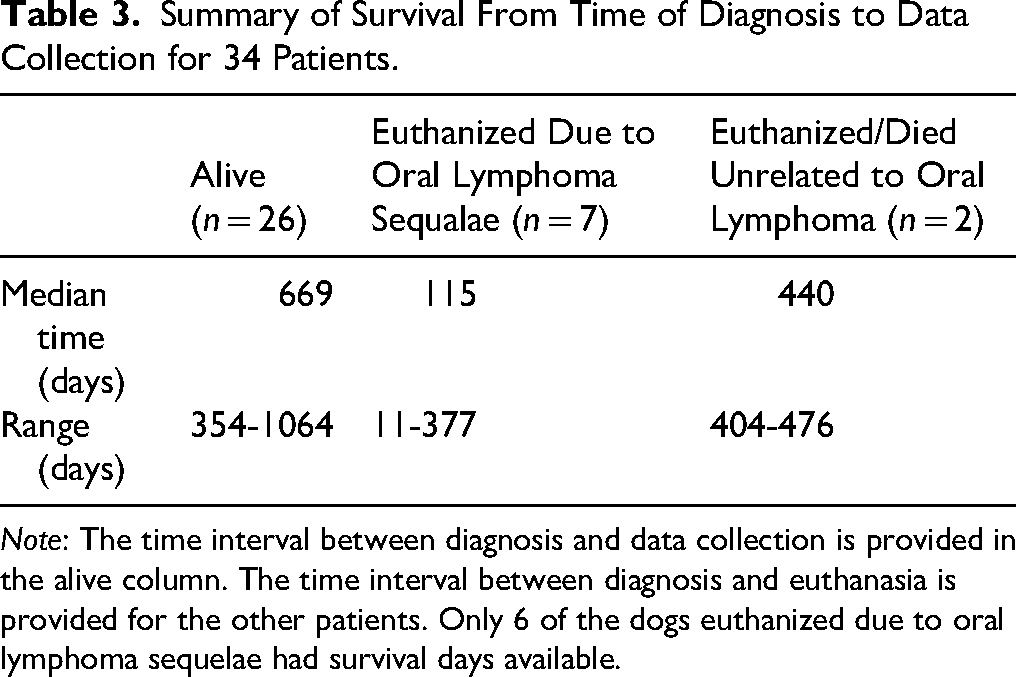
Note: The time interval between diagnosis and data collection is provided in the alive column. The time interval between diagnosis and euthanasia is provided for the other patients. Only 6 of the dogs euthanized due to oral lymphoma sequelae had survival days available.
Discussion
This study represents the largest retrospective evaluation to date of canine oral lymphoma, providing practical insights regarding clinical presentation and multiplicity of lesions. Of the 75 cases reviewed, the vast majority (97.3%) were diagnosed as ETCL. Lesions were frequently located at the mucocutaneous junction, buccal/labial mucosa, and gingiva. Mucocutaneous lesions were commonly found at the mandibular labial frenulum (61.2%), and 46.7% of mandibular frenulum lesions were the only lesions present in the oral cavity. Lesions were more likely to be multifocal (57.3%) and differed in gross appearance when compared to solitary lesions. Multifocal lesions were often ulcerated and thickened, whereas solitary lesions were often described as mass-like and erythematous. Both lesions had changes in coloration, being either erythemic or depigmented. Nonepitheliotropic subtypes of T-cell lymphoma, including LTZL and PTCL-NOS, were rare in the dogs within this study population. No cases of canine oral B-cell lymphoma were identified except for the 3 cases of tonsillar lymphoma, which were excluded from the study because of occurrence within a lymphoid organ.
The median age of dogs with oral lymphoma lesions was 11 years, which is consistent with studies that have exclusively assessed epitheliotropic lymphoma.7,12 Although Golden Retrievers were the most common purebred breed represented, they were not found to be significantly overrepresented, unlike in a previous study. 12 In contrast, Beagles were found to be significantly overrepresented, a novel finding not previously reported. No significant gender predisposition was identified in this study, similar to a study on cutaneous ETCL. 9 This contrasts with a larger retrospective study on canine epitheliotropic and nonepitheliotropic cutaneous lymphoma that found females were more likely to be affected than males. 7
Lesion Distribution and Clinical Appearance
In this study, oral lymphoma was often located at the mucocutaneous junction, buccal mucosa, and gingiva, with 62.5% of mucocutaneous lesions arising at the mandibular labial frenulum.
Most of the cases in this study (57.3%) demonstrated multifocal lesions. While dedicated research on T-cell lymphoma confined exclusively to mucosal regions (ie, oral cavity, genitalia) is limited, a previously published retrospective study evaluating dermatologic lesions reported that 1 case (1/30, 3.3%) had only mucosal lesions (oral cavity) and 3 cases (3/30, 10%) had only mucocutaneous lesions. 15 This could reflect bias in the case selection criteria since the study was primarily focused on cutaneous disease. In a larger retrospective study evaluating whole-body lesion distribution, epitheliotropic T-cell lymphoma affected solely the mucosa in 24 cases (24/148, 16.2%) and the mucocutaneous junctions in 44 cases (44/148, 29.7%). 12 The present study had only 12 (16%) cases that reported lesions that were neither oral mucosa nor oral mucocutaneous junction. These results are biased by case selection from an oral pathology service. The true distribution of lesions in canine ETCL will require studies that are not biased by the veterinary specialty. A previous study of canine ETCL showed similar T lymphocyte localization and trafficking patterns in the skin and oral mucosa. 16 It is clear that ETCL can affect cutaneous, mucocutaneous, and mucosal sites; therefore, thorough examination of the entire patient is warranted when this disease is suspected.
Previously published case reports have highlighted the diverse clinical presentation of oral lymphoma, underscoring the importance of recognizing the wide variation in lesion appearance.13,14,17 In this study, lesions frequently appeared as multifocal, eroded/ulcerated, mass-like, and erythematous, often mimicking ulcerative stomatitis, inflammatory lesions, or other oral neoplasms. Mucosal color change, such as erythema or depigmentation, should prompt biopsy and histopathologic evaluation to improve early lesion detection. In this study, 5 ETCL lesions were presumed to be early based on minimal mass effect and only low numbers of neoplastic lymphocytes within the lamina propria. For each of these, the reason for biopsy was a change in oral mucosal coloration, either depigmentation or erythema.
Multiple, deep (nonsuperficial) biopsy samples should be obtained, ideally including areas at the interface of the lesion(s) and adjacent normal tissue, to improve diagnostic yield. 18 Clinicians should be mindful to obtain biopsy samples from nonulcerated areas since preservation of the epithelial architecture is necessary to identify the epitheliotropic infiltration of lymphocytes that is characteristic of ETCL.15,18 Care should also be taken to avoid crush artifacts, and prompt fixation is essential to preserve the tissue architecture and facilitate immunophenotyping when needed. 18
Diagnosis of ETCL
Because oral lymphoma may clinically resemble an inflammatory/immune-mediated disease or another round cell neoplasm, histopathologic evaluation is imperative and additional testing is often necessary for accurate diagnosis and classification. This retrospective study included cases diagnosed as oral T-cell lymphoma, although additional confirmatory testing was applied inconsistently with approval by the patient's owner. Consequently, the approach to diagnosis was biased toward cases for which histopathology supported a definitive diagnosis that was congruent with clinical presentation. IHC is important for round cell tumors that do not have convincing epitheliotropism or have epitheliotropism but cannot be confidently differentiated from another type of round cell tumor. IHC and PARR help to differentiate between ETCL and inflammatory lesions that may have intraepithelial lymphocytes, including chronic canine ulcerative stomatitis (CCUS) and erythema multiforme.13,19 IHC can help to confirm the abundance of intraepithelial CD3-positive lymphocytes, particularly when tissue detail is distorted by cellular degeneration and nuclear pyknosis. For lesions that are equivocal, PARR testing for clonality is imperative to differentiate ETCL from CCUS, erythema multiforme, or other inflammatory lesions. 13 Because IHC and PARR testing for all cases was beyond the scope of this study, cases were biased toward advanced disease, and cases of early T-cell lymphoma were likely excluded.
Characterization of canine lymphoma continues to evolve. Genetic profiles of canine lymphoma are emerging and will help to address limitations of IHC, flow cytometry, and PARR.20,21 Rare canine lymphomas have aberrant or dual expression of T and B cell markers.21,22 Canine lymphomas that express both T and B cell markers often have clonal rearrangement of T-cell receptor, consistent with T cell lymphoma; however, some cannot be classified with PARR.21,22 Pertinent to this discussion, and meant to represent an approach to diagnosis that is both pragmatic and mindful of financial resources available to dog owners, a diagnosis of ETCL is highly probable for an epitheliotropic round cell neoplasm that has strong expression of CD3 and is too proliferative to represent an inflammatory disease. While plasma cell tumors may express CD3, they are not among the round cell tumors that may demonstrate epitheliotropism. 23 Epitheliotropism can be seen with histiocytoma and mast cell tumor, although neither of these expresses CD3. 24
Tumor Staging
Previous studies of cutaneous ETCL in dogs have inconsistently addressed tumor stage. Some studies have simply noted the presence or absence of a mass lesion 7 while another classified lesions as patch/plaque versus nodular. 9 One large canine ETCL study that included oral mucosal cases provided a lesion-based clinical stage (premycotic, mycotic, or tumoral). 12 For this study, the authors did not have sufficient information to provide a lesion-based clinical stage. Instead, a category based on histologic distribution of neoplastic cells in ETCL lesions (epithelium only, mucosa only, or deep/tumor) was provided. The present study had a high proportion of deep/tumor lesions (85.1%). This likely reflects case selection bias toward dogs with more advanced disease. It is important to note that patients who had multiple biopsies taken from multifocal ETCL lesions occasionally had lesions in different histomorphologic categories. While no ETCL cases were classified as epithelium-only, some of the mucosa-only and deep/tumor ETCL cases had epithelium-only lesions. Therefore, dogs with multifocal ETCL lesions are likely to have lesions in different clinical stages. It is not clear if histologic lesion morphology correlates with lesion-based tumor stage. There may be a benefit from developing a histologic grading system for ETCL lesions; however, future studies are needed for validation, and there is an inherent risk of grading a single lesion in dogs that have multifocal lesions.
In humans, staging of mycosis fungoides uses the TNMB (tumor, node, metastasis, blood) system. 8 By including involvement of blood (ie, leukemia), this system accommodates Sézary syndrome. Tumor staging is defined as follows: T1—flat lesions (patches, papules, plaques) covering less than 10% of the skin surface; T2—flat lesions covering 10% or more of the skin surface; T3—1 or more tumors of 1 cm or more in diameter; T4—confluence of erythema covering 80% or more of the body. 8 Future studies of canine ETCL are encouraged to use this or another clearly defined TNMB system. If coupled with robust survival data, a standardized grading system could significantly improve prognostication for dogs with ETCL.
ETCL Subtypes
ETCL, as a monoclonal proliferation of T lymphocytes that exhibit epitheliotropism, has recognized subtypes (pagetoid reticulosis, mycosis fungoides, and Sézary syndrome). Previous research suggests that MF makes up the majority of ETCL cases in dogs since PR and Sézary syndrome are reported to be rare.2,6,7 The exception is 1 study in which 20% of dogs had the diagnosis of generalized PR, 9 which might more correctly be considered MF based on other definitions. 16 Confirmation of PR would likely require PARR testing since neoplastic T lymphocytes are limited to the epithelium; therefore, there is no mass lesion. Sézary syndrome, a leukemic form of ETCL, requires confirmation of blood involvement by PARR and/or flow cytometry. To the authors’ knowledge, this testing was not performed on peripheral blood for any dogs in this study.
ETCL lesions in this study had considerable heterogeneity with respect to mitotic count, lesion number, histologic morphology, and anatomic distribution. As discussed, this data set appears to have been biased in favor of advanced disease, but it is still surprising that many deep/tumor ETCL lesions had features of high-grade T-cell lymphoma. Other studies of canine ETCL have demonstrated heterogeneity with respect to lesion morphology and biological behavior, including more favorable outcomes for patients with solitary lesions. 12 It is likely that future investigation of canine ETCL, especially characterization of solitary tumoral lesions, will provide a more refined classification system. Prospective studies are necessary to determine if patients with solitary lesions progress to having multifocal lesions and if patients with indolent ETCL can progress to high-grade T-cell lymphoma. More extensive use of molecular diagnostics, especially flow cytometry, is encouraged in both the research and diagnostic settings. Prospective studies are also needed to improve prognostication of ETCL in dogs based on lesion location, lesion number, disease stage, and treatments performed.
Nonepitheliotropic T-cell lymphoma
LTZL and PTCL-NOS represent uncommon variations of oral T-cell lymphoma in dogs. This study included 1 case of each. In a previously published case series that evaluated lingual canine T-zone lymphoma in 12 canines, lesions were found incidentally in 75% of patients that were asymptomatic. 10 The dogs with LTZL typically had multifocal to coalescing, erythemic, raised nodules on the tongue. 10 The single case of LTZL in the present study had similar multifocal lesions that were discovered incidentally during a dental procedure. Furthermore, while the mitotic count of 22 figures per 10 high-power fields in this study is greater than expected for an indolent form of lymphoma, a case series of LTZL in dogs reports mitotic counts from 2 to 75 figures per 2.37 mm2. 10 Of the 8 ETCL cases with involvement of the tongue, most had multifocal mass lesions and were clinically similar to the LTZL case except that epitheliotropism was noted histologically. While epitheliotropism is not expected for LTZL, the use of flow cytometry for cases such as this would be recommended to clearly differentiate between ETCL and LTZL.
For the singular PTCL-NOS case in this study, the patient had a smooth, nonulcerated, solitary mass. It is worth noting that there were no cases of ALTCL in this dataset. However, the pathology medical record database includes rare cases of ALTCL from the oral cavity of dogs that did not fall within the timeframe of case selection for this study.
Patient Survival
Follow-up information was limited because of the study's retrospective design. Although it was possible to gather follow-up status (ie, alive vs euthanized) on 35 patients, information regarding whether these patients pursued treatment was not available. Additionally, dogs with solitary lesions in this study did not exhibit significantly longer survival compared to those with multifocal lesions. This is contrary to a larger retrospective study where solitary lesions of epitheliotropic lymphoma had more favorable outcomes. 12 This finding may be attributable to the limited number of cases with available follow-up data. Prospective studies on oral lymphoma are warranted to gather complete survival data relating to the presence of distant, nonoral lesions, the number of oral lesions (ie, solitary lesions vs multifocal lesions), treatment performed, and response to treatment. Once this data is known, practitioners will be able to more accurately prescribe treatment plans and provide patient prognoses for owners to consider.
Limitations
This study has several limitations inherent to its retrospective design. Follow-up information was difficult to obtain, which impacted the ability to analyze meaningful data regarding survival time, clinical stage, and treatments provided, if any. Additionally, the inability to systemically evaluate the entire patient for disease beyond the oral cavity made it difficult to determine whether the patient had cutaneous or other mucocutaneous lesions. The lack of hematology results also made it impossible to identify cases of Sézary syndrome. As a final limitation, the inability to use IHC and PARR testing on a larger number of cases likely excluded early ETCL cases and possible cases of pagetoid reticulosis.
Conclusion
This retrospective study expands current knowledge of canine oral T-cell lymphoma, particularly the predominance of ETCL. The identification of rare nonepitheliotropic forms of oral T-cell lymphoma in dogs highlights the need for thorough histopathologic and immunophenotypic evaluation. Given the overlap in clinical appearance with other oral conditions, accurate diagnosis is essential. Biopsy and histologic evaluation are indicated for oral tissues with mucosal color change (erythema or depigmentation) to detect this disease early. Increased clinical awareness will support earlier recognition and enable practitioners to make more informed diagnostic and treatment decisions. This study's limitations highlight the importance of future prospective research to better understand disease progression, treatment outcomes, and prognostic factors.
Materials
VENTANA, Roche Diagnostics, Indianapolis, IN, USA ULTRA CC1, VENTANA, Roche Diagnostics, Indianapolis, IN, USA clone 2GV6, VENTANA, Roche Diagnostics, Indianapolis, IN, USA ultraView Universal DAB detection kit, VENTANA, Roche Diagnostics, Indianapolis, IN, USA SAS Institute Inc., Cary, NC, USA
Footnotes
Acknowledgments
The authors would like to thank Sangeeta Rao for their assistance with statistical analysis and data interpretation.
Ethics Statement
Ethical review and approval were not required for this retrospective, patient record-based animal study in accordance with the local legislation and institutional requirements. Written consent for the release of electronic medical record data and images was obtained.
Author Contributions
VC, CB, JR, NH: conceptualization, methodology, investigation. VC: data curation, writing—original draft. CB, NH, JR: supervision, writing—review and editing. VC completed this work while affiliated with the Department of Clinical Sciences, College of Veterinary Medicine and Biomedical Sciences, Colorado State University. The author is now affiliated with the Department of Dentistry and Oral Surgery Service, Colorado Animal Specialty and Emergency, Boulder, CO, USA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.