
Abstract
Open-mouth jaw locking in cats is an uncommon condition often associated with temporomandibular joint (TMJ) and mandibular symphysis laxity in which mechanical coronoid–zygomatic impingement occurs. This report describes a 5-year-old Persian cat with recurrent right-sided jaw locking. Clinical examination revealed persistent open-mouth posture with mandibular deviation and mild symphyseal laxity. Computed tomography (CT) confirmed ventrolateral displacement of the right coronoid process, bilateral condylar subluxation, condylar flattening and elongation of the right retroarticular process. Due to recurrence, unilateral partial coronoidectomy was performed. Immediate and 8-week postoperative CT demonstrated restoration of mandibular alignment, improved TMJ congruity and resolution of impingement without recurrence. This case highlights the key role of CT in diagnosis, surgical planning, and follow-up of open mouth jaw locking in cats and supports surgical management in recurrent cases.
Keywords
Introduction
Intermittent open-mouth jaw locking in cats is an uncommon condition described in a limited number of published cases, initially extrapolated from the canine model and later reported in individual feline case reports and small case series.1–3 The condition has been primarily attributed to dysplasia and laxity of the temporomandibular joint (TMJ) allowing lateral mandibular displacement and mechanical impingement of the coronoid process against the adjacent zygomatic arch 4 and, in some cases, has been associated with condylar and mandibular fossa flattening, elongation of the retroarticular process, articular subluxation and degenerative changes consistent with osteoarthritis documented by computed tomography (CT).1,3,5,6 Most reported cases have involved young adult cats, with a predominance of Persian cats and an apparent overrepresentation of brachycephalic breeds.1,3 Clinically, affected cats have an inability to close the mouth due to ventrolateral displacement of the mandibular ramus, with the mandible deviated and rotated toward the side of coronoid impingement.1,2 Diagnosis is based on orthopedic examination and imaging studies, including conventional radiography and CT, the latter being particularly valuable for precise anatomical assessment and identification of structural abnormalities associated with the locking mechanism.1,5,6 Treatment options described in the literature include both conservative and surgical approaches; although acute episodes may be managed by manual reduction, recurrence has frequently been reported, and definitive treatment has typically involved surgical procedures aimed at eliminating the mechanical impingement, including partial zygomatic arch resection, partial coronoidectomy or a combination of both.1–3
This report describes the clinical presentation, diagnostic evaluation—including orthopedic examination and CT —and surgical management of open-mouth jaw locking in a Persian cat.
Case Description
A 5-year-old neutered male Persian cat weighing 3.2 kg was presented with a 12-h history of persistent open mouth posture associated with mandibular deviation. The owner reported three previous episodes of similar clinical signs over the preceding three months, which were resolved by the referring veterinarian through manual repositioning of the mandible under sedation. On physical and orthopedic examination, the patient exhibited pain on manipulation of the mandible, moderate ptyalism, and repeated attempts to contact the perioral region with the forelimbs. The cat was in normal body condition, and hematologic and serum biochemical analyses were within reference intervals.
The mouth was maintained in a fixed open position, with lateral displacement of the mandible toward the right side (Figure 1). The right mandibular canine tooth was positioned more ventrally than the left. A firm bony prominence was palpated in ventrolateral position to the right zygomatic arch and mild laxity of the mandibular symphysis was detected on manual palpation.

Clinical photograph obtained at the time of presentation showing the mouth fixed in an open position. Marked right-sided deviation of the mandibular arcade is evident, with clockwise rotation of the mandible. The right mandibular canine is positioned at a lower level compared with the left, consistent with mandibular displacement.
Based on the clinical presentation, a presumptive diagnosis of right-sided open mouth jaw locking was made. To confirm the diagnosis and evaluate potential underlying anatomical abnormalities, a CT study was performed under general anesthesia. The patient was premedicated with methadonea (0.2 mg/kg) and dexmedetomidineb (4 µg/kg) intramuscularly (IM). Anesthesia was induced with propofolc intravenously (IV) to effect and maintained with isofluraned (2%) in oxygen.
CT of the head (Figure 2) was performed using a conventional fan-beam CT scannere using 1.25 mm slice thickness acquisitions with bone and soft tissue algorithms. Multiplanar reconstructions (MPR) and three-dimensional (3D) reconstructions were generated for detailed evaluation and comparison with the normal anatomy of a mesaticephalic cat (Figure 3). The right coronoid process was positioned ventrolateral to the mid-portion of the right zygomatic arch. The height of the coronoid process of the mandible relative to the length of the mandible appeared shorter than in a normal cat patient, while the zygomatic arch appeared wider and the width of the retrobulbar space in which the coronoid process moves appeared narrower than in a normal cat. Subluxation with lateral displacement of condylar processes of both TMJ was identified, more pronounced on the right side. The mouth remained open, with mandibular deviation and rotation toward the right. The right mandible was rotated to lateral more than the left and the symphyseal joint space appeared increased. Both mandibular condylar processes appeared flattened and reduced in size in relation to their corresponding mandibular fossae. Additionally, ventral elongation of the right retroarticular process was observed, with greater ventral extension compared to the left.
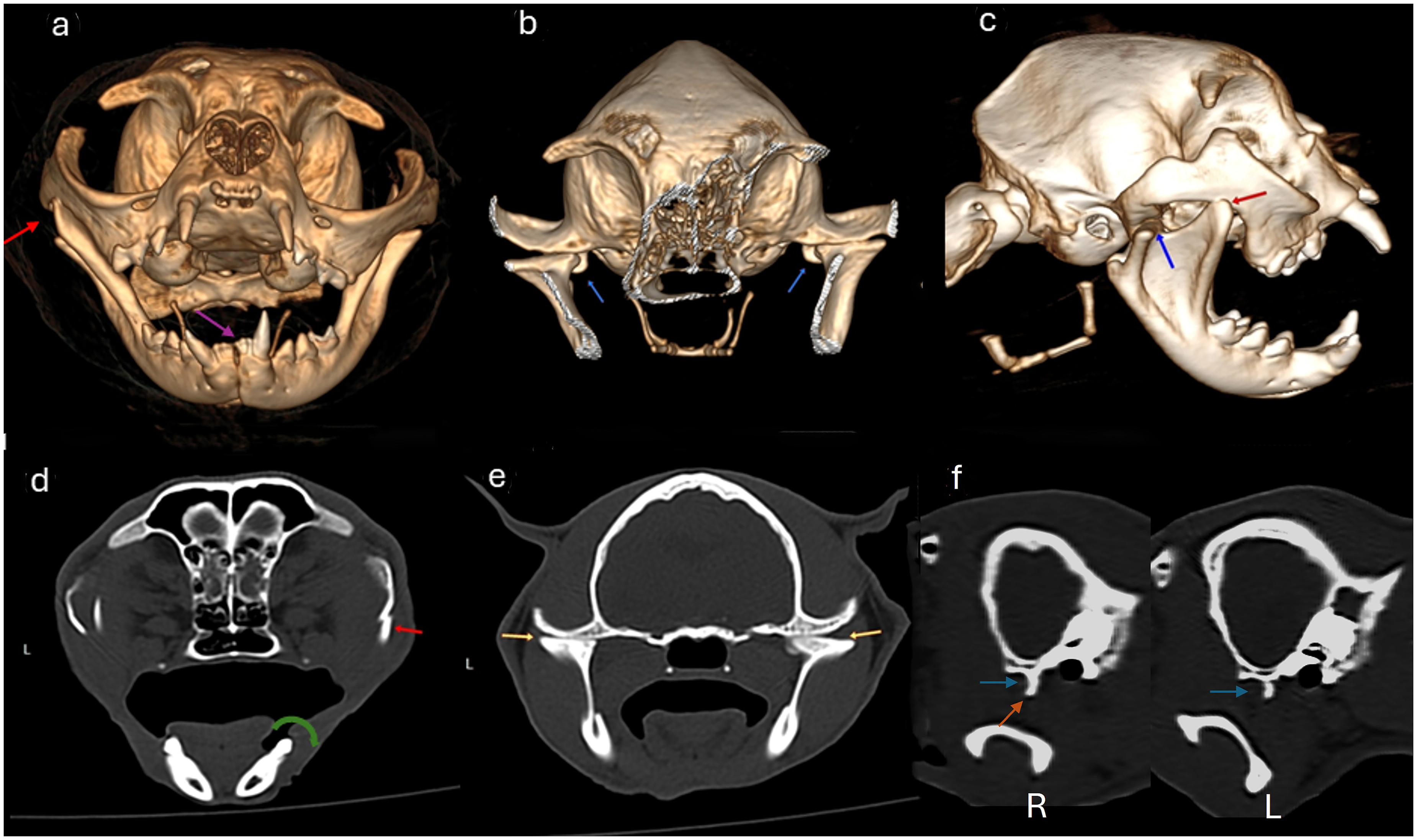
Computed tomography (CT) study of the skull at the time of presentation. The upper panel shows three-dimensional reconstructions of the skull. (a) Frontal view, (b) frontal view after partial digital removal of the mandible and nasal cavity skeleton to visualize the temporomandibular joints and (c) right lateral view. The lower panel shows multiplanar reconstructions, with transverse slices at the level of: (d) mid-zygomatic, (e) temporomandibular joints and (f) a sagittal slice at the level of the medial aspect of the right (R) and left (L) temporomandibular joints. The right coronoid process was positioned ventrolateral to the zygomatic arch (a, c, d; red arrows), resulting in mechanical open-mouth locking (a, c). Increased separation of the mandibular symphysis was observed (a; purple arrow). Bilateral lateral subluxation of the mandibular condylar processes was evident (b, c; blue arrows), leaving the medial aspect of both mandibular fossae unoccupied (f). The dorsal aspect of both mandibular condyles appeared flattened (e; yellow arrows). The right mandibular body was more laterally rotated compared with the left one (d; curved green arrow). Additionally, the right retroarticular process exhibited osseous overgrowth (f; orange arrow).
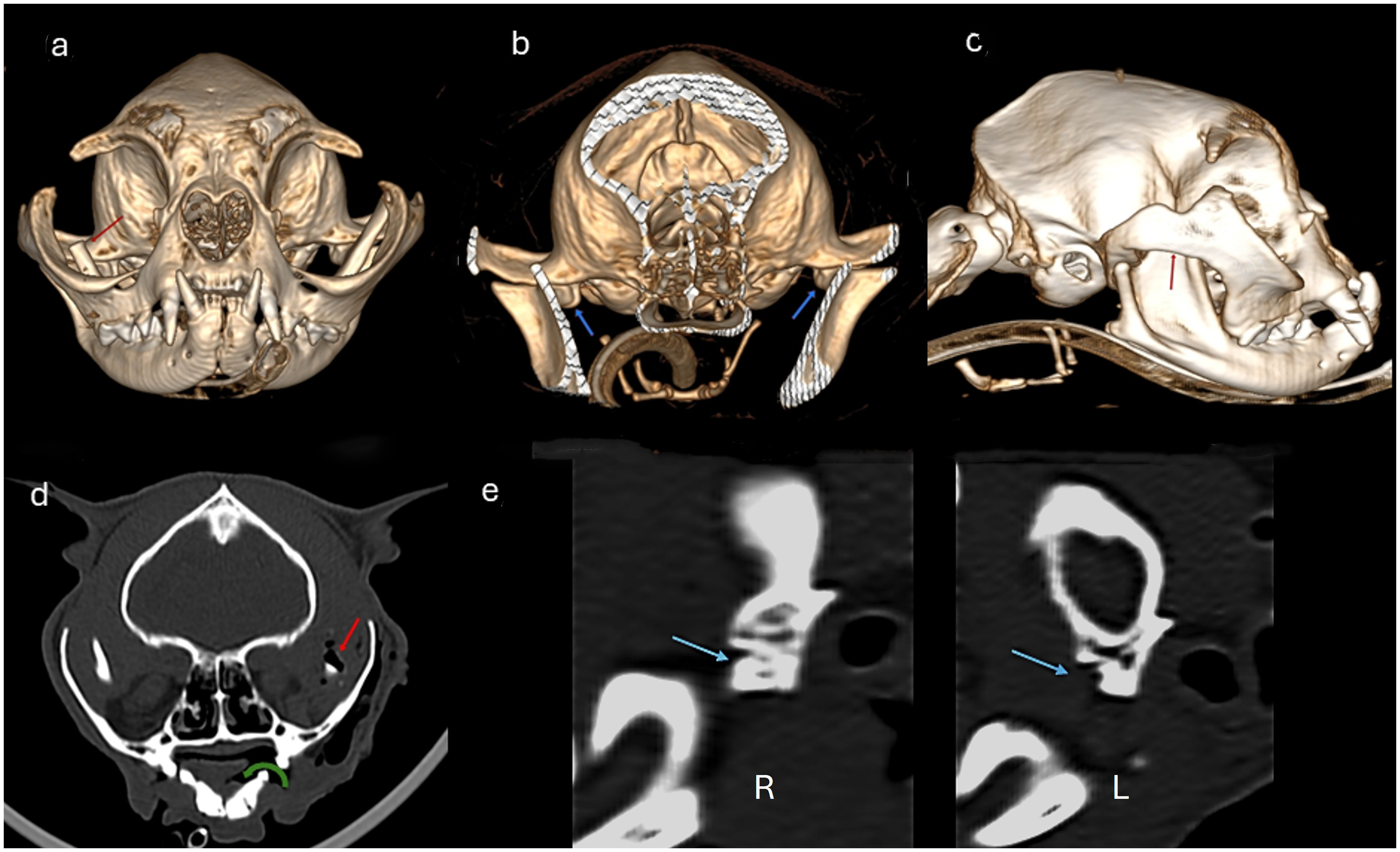
Computed tomography (CT) study of the skull of a mesaticephalic cat showing normal osseous anatomy. The upper panel shows three-dimensional reconstructions of the skull: (a) frontal view, (b) frontal view after partial digital removal of the mandible and nasal cavity skeleton to visualize the temporomandibular joints, and (c) right lateral view. The lower panel shows multiplanar reconstructions, including transverse slices at the level of the (d) mid-zygomatic arch and (e) temporomandibular joints, and a sagittal slice at the level of the (f) medial aspect of the right temporomandibular joints. The coronoid processes are positioned dorsolateral to the zygomatic arches (a, c, d; red arrows). Both mandibular bodies articulate correctly at the mandibular symphysis (a; purple arrow). The mandibular condyles fully occupy the mandibular fossae (b, c, f; blue arrows), and the retroarticular processes do not extend ventral to the condyles (f; orange arrow). The dorsal aspect of both mandibular condyles is normally shaped, maintaining the typical cylindrical morphology (e; yellow arrows).
Based on these findings, the presumptive diagnosis of open mouth jaw locking was confirmed. The imaging features were consistent with bilateral TMJ dysplasia and mild laxity of the mandibular symphysis.
After establishing the diagnosis through imaging studies, manual reduction of the mandibular locking was performed. Maximal mouth opening was achieved while applying pressure from the right lateral side toward the medial direction and simultaneously counter rotating the mandible in a clockwise direction (Video 1 in the supplementary materials). Subsequently, the locking mechanism was reproduced by applying pressure and rotation in the opposite direction (Video 2 in the supplementary materials). Finally, after unlocking the mandible again, an attempt was made to reproduce locking toward the left side by opening the mouth maximally and displacing the mandible toward the left lateral side while rotating it counterclockwise (Video 3 in the supplementary materials); however, this maneuver was unsuccessful. It was therefore concluded that the locking presumably occurred only toward the right side.
Twenty-four hours after establishing the diagnosis and obtaining informed owner consent, surgical treatment was performed consisting of a right partial coronoidectomy. The patient was anesthetized following the previously described protocol. Endotracheal intubation via pharyngostomy was used to permit intraoperative evaluation of dental occlusion and confirmation of mechanical resolution of the mandibular locking without interference from an orotracheal tube. Cephalosporinsf were administered 45 min prior to surgery. The surgical field was prepared aseptically by hair clipping, cleansing and scrubbing with chlorhexidine soap.g The patient was positioned in left lateral recumbency and the mandibular locking was manually reproduced in order to palpate the luxated coronoid process and facilitate surgical access. A semilunar skin incision was performed using monopolar electrosurgeryh, centered on the ventral border of the zygomatic arch and extending approximately 2 cm caudally and 2 cm cranially from the palpation point of the coronoid process. Bleeding control was obtained using bipolar electrocauteryi. The subcutaneous tissues were carefully separated by blunt dissection with Metzenbaum scissorsj until the masseter muscle was identified. An incision was made through the masseteric aponeurosis along the ventral margin of the zygomatic arch, allowing exposure of the displaced coronoid process. The muscular insertions were carefully released using monopolar electrosurgery, detaching the masseter muscle laterally and the temporalis muscle medially from the coronoid process. A Freer periosteal elevatork was subsequently introduced to complete isolation of the coronoid process from the adjacent zygomatic arch. A straight osteotomy was then performed with an oscillating sawl, removing approximately 5 mm from the dorsal portion of the coronoid process. After excision of the osteotomized segment, the mandibular ramus was released by withdrawing the periosteal elevator, allowing the coronoid process to reposition medially beneath the zygomatic arch and return to its normal anatomical alignment. Occlusion was reassessed intraoperatively by an assistant and confirmed to be normal prior to incision closure. The masseteric aponeurosis and subcutaneous tissues were apposed using 3-0 monofilament polyglyconatem in a simple continuous pattern and the skin was closed with 3-0 nylonn in a simple interrupted pattern.
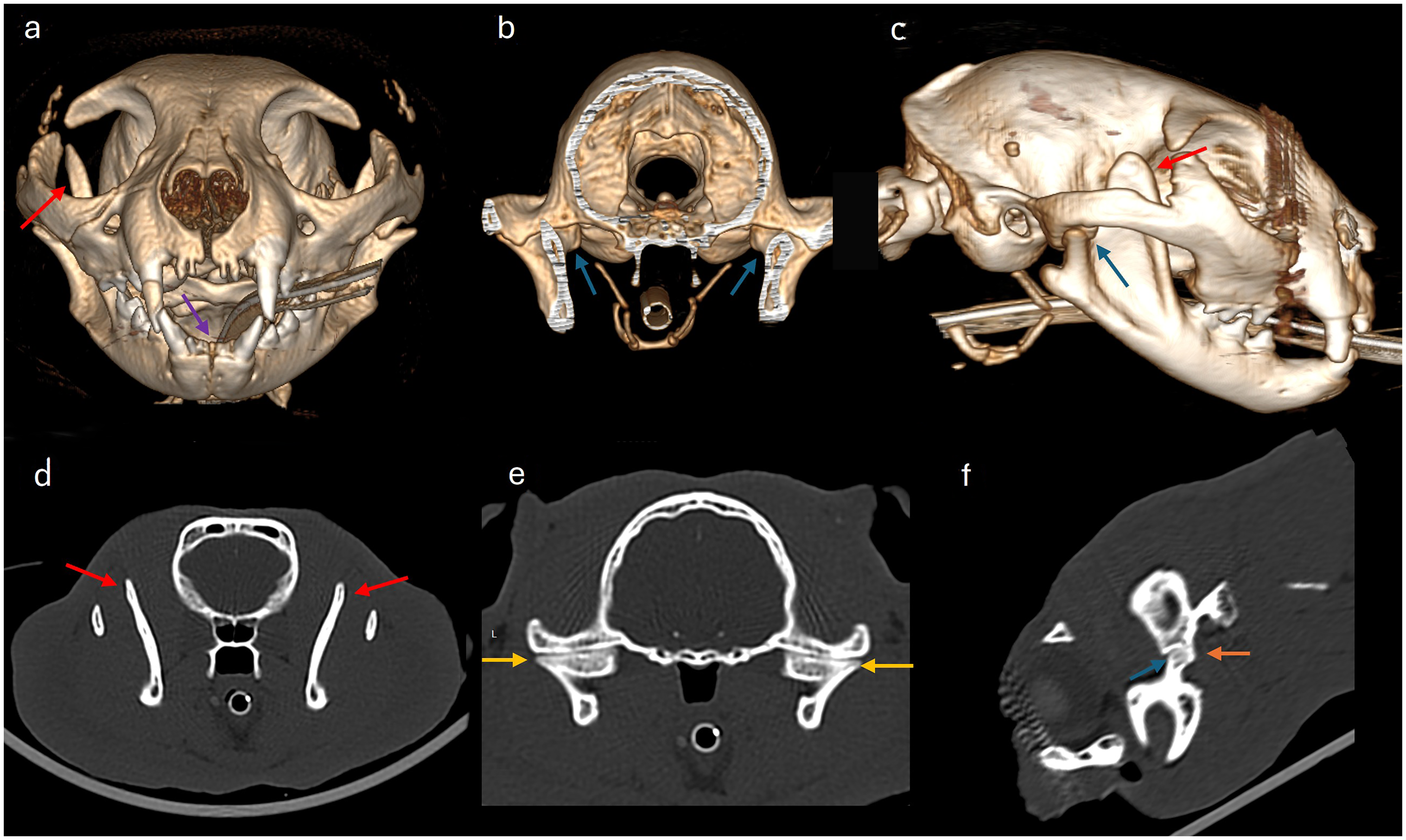
A second CT study was performed immediately after surgery while maintaining anesthesia (Figure 4). Postoperative imaging confirmed appropriate mandibular positioning, with the right mandibular ramus located medial to the zygomatic arch. Improved alignment of the mandibular condyles within the mandibular fossae was observed.
Postoperative computed tomography (CT) study. The upper panel shows three-dimensional reconstructions of the skull in the same views as Figure 3. The lower panel shows multiplanar reconstructions, with (d) transverse slice at the level of the mid-zygomatic arch and (e) sagittal slices at the level of the medial aspect of the right (R) and left (L) temporomandibular joints. Postoperative imaging demonstrates dorsal osteotomy of the right coronoid process (a, c, d; red arrows), which is now positioned medial to the zygomatic arch. Realignment of the right mandibular body is evident, with reduction of the previous lateral rotation (d; green curved arrow). The temporomandibular joints show improvement in alignment, with the left joint restored to normal positioning and the right joint demonstrating marked reduction of the previous subluxation (b; blue arrows). The medial aspect of both mandibular fossae is now occupied by the mandibular condylar processes (e; blue arrows), indicating restoration of a more physiological condylar position. Patient has recovered normocclusion (a, c).
The patient remained hospitalized for 24 h postoperatively and received intravenous fluid therapy with Lactated Ringer's solutiono administered at a maintenance rate (3 mL/kg/h). Analgesia was provided with methadonep (0.2 mg/kg) IV every 8 h and meloxicamq (0.05 mg/kg) subcutaneously (SC) every 24 h). Antimicrobial therapy consisted of cefazolinr (22 mg/kg) IV every 8 h). At discharge, oral cephalexins (20 mg/kg) per os (PO) every 12 h and meloxicamt (0.05 mg/kg) PO every 24 h were prescribed for five days. The owner was instructed to perform twice daily cleansing of the surgical site with a povidone–iodine solutionu until suture removal and to maintain an Elizabethan collarv during the recovery period. A soft dietw was recommended, and water was allowed ad libitum. Based on the owner's description of the cat's usual play behavior, activities that could promote excessive mouth opening, such as playing with toys or balls, were strictly avoided.
Suture removal was performed 14 days after surgery following confirmation of appropriate cutaneous healing. At that time, the patient exhibited normal masticatory function without signs of pain or recurrence of mandibular locking. Dietary restrictions were lifted, allowing a return to a mixed diet consisting of dry kibble and homemade food. Normal activity was also resumed.
A final clinical and CT (Figure 5) evaluation was performed 8 weeks after surgical treatment. The patient had not experienced any episodes of mandibular locking, was eating normally and showed no signs of pain upon oral manipulation. CT imaging confirmed appropriate mandibular positioning with normal occlusion and correct alignment of both TMJs. The patient was discharged from follow-up, and the case was considered resolved.
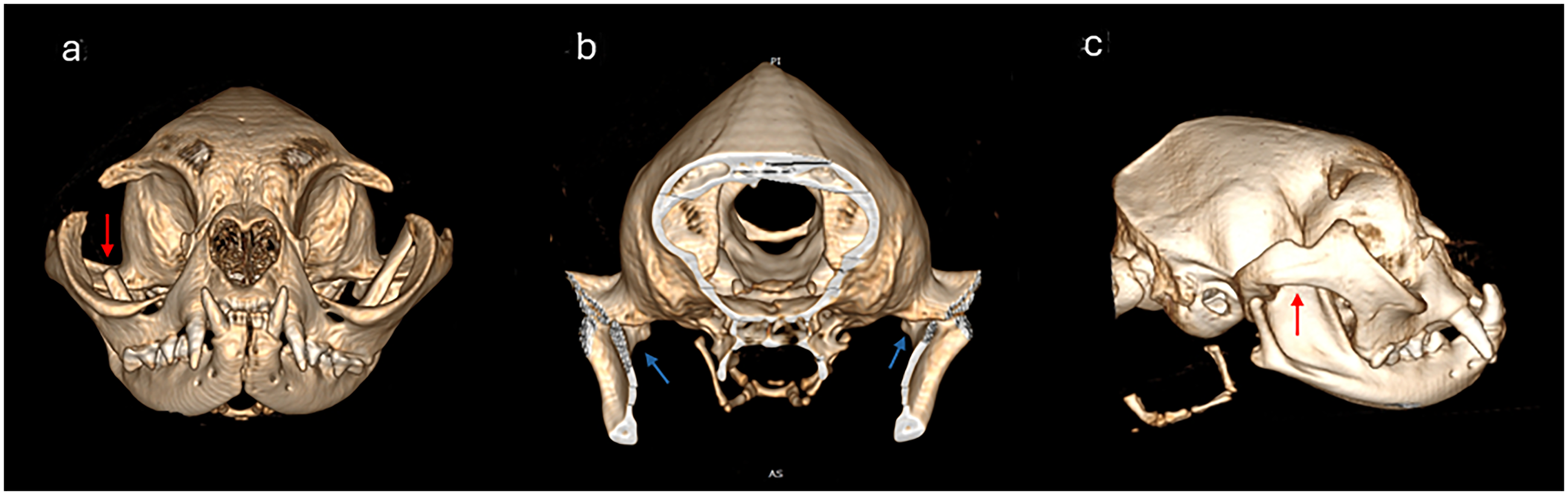
Computed tomography (CT) study performed 8 weeks after surgical treatment. Three-dimensional reconstructions are shown in the same projections as in Figures 2 and 4. Normal positioning of the right coronoid process relative to the zygomatic arch is observed (a, c; red arrows), and articular congruity has been restored in both temporomandibular joints (b; blue arrows).
Discussion
Open mouth jaw locking in cats is an uncommon condition typically associated with TMJ dysplasia, capsular laxity and secondary mechanical impingement of the coronoid process against the zygomatic arch.1–3 The mechanism by which brachycephalic cats develop open-mouth jaw locking remains incompletely understood. Brachycephalic cranial conformation in felines is characterized by mesioversion of the maxillary canine teeth, maxillary brachygnathism and dorsorotation of the jaws, 10 resulting in altered dental occlusal relationships, particularly at the level of the canine teeth. It should be noted that, in mesocephalic cats, the mandibular canine teeth occlude within the interalveolar space between the maxillary canine teeth and the third incisors. Additionally, the maxillary incisors are positioned rostral to the mandibular incisors, which occlude against the maxillary lingual surfaces near the cingulum. In contrast, in brachycephalic cats this relationship is reversed, with the maxillary incisors occluding lingually relative to the mandibular incisors. 4 This altered occlusal relationship results in an abnormal distribution of masticatory forces during occlusion. It has been hypothesized that abnormal masticatory forces generated by malocclusion may influence joint biomechanics, potentially contributing to increased laxity of both the TMJs and the mandibular symphysis. Symphyseal laxity has been suggested as a contributing factor in the development of open-mouth jaw locking, as a certain degree of intermandibular mobility may be necessary to permit sufficient lateral displacement of the mandibular ramus for coronoid impingement to occur.7–9 In the present case, mild mandibular symphyseal laxity was detected on manual palpation and supported by CT findings showing increased separation of the symphysis. Additionally, the right mandibular body exhibited increased lateral rotation compared with the left when it was locked. This combination of symphyseal and TMJ laxity may have facilitated excessive lateral displacement of the mandibular ramus, thereby contributing to the development and recurrence of the locking mechanism. Alternatively, the symphyseal laxity observed in this case may not have been a primary predisposing factor but rather a secondary consequence of increased mechanical forces acting on the intermandibular joint during prolonged periods of mandibular locking. Repeated episodes of lateral displacement and sustained abnormal mandibular positioning could have resulted in progressive stress on the symphyseal region, contributing to increased mobility over time. Several cases of mandibular symphyseal laxity associated with open-mouth jaw locking have been described in Persian cats.5,9
Although manual reduction may resolve acute episodes, recurrence is frequently reported, particularly in patients with underlying structural abnormalities.1,2 In the present case, the history of multiple previous locking episodes requiring sedation and manual repositioning supported the decision to pursue definitive surgical treatment. Given the recurrent nature of the condition and the anatomical alterations identified on imaging, surgical intervention was considered the treatment of choice to prevent further episodes.
Several surgical techniques have been described for the treatment of open mouth jaw locking, including total or partial zygomatic arch resection, coronoidectomy, symphysiotomy, symphysectomy and intermandibular symphyseal arthrodesis. Despite these variations in technique, the primary objective in all cases remains the same: elimination of the coronoid–zygomatic mechanical conflict while preserving mandibular function and joint stability. When locking occurs unilaterally, surgical intervention should be performed on the affected side; however, owners should be informed of the potential risk of future contralateral locking. 3 Reported outcomes for both partial zygomatic arch resection and partial coronoidectomy are generally favorable, with low recurrence rates when the mechanical impingement is adequately addressed.1,2,5,7–9 The choice of technique therefore appears to depend largely on surgeon preference, anatomical configuration, and the specific structural abnormalities identified in each case. In the present case, CT findings localized the impingement primarily to the dorsal aspect of the right coronoid process, supporting partial coronoidectomy as a targeted and anatomically logical approach.
CT played a central role in diagnosis and case management. Preoperative CT enabled precise characterization of the locking mechanism and associated abnormalities, including bilateral condylar subluxation, flattening of the dorsal aspect of the condyles, elongation of the right retroarticular process and increased separation of the mandibular symphysis. Similar findings have been described in previous case reports and retrospective imaging studies evaluating TMJ disorders in cats. 6 CT has been consistently shown to provide superior assessment of joint congruity, osseous remodeling and spatial relationships compared with conventional radiography.3–6,9
In addition to diagnosis, CT was instrumental in surgical planning by clearly identifying the site and extent of coronoid impingement. Immediate postoperative CT confirmed medial repositioning of the mandibular ramus relative to the zygomatic arch and improved alignment of the condylar processes within the mandibular fossae. While intraoperative occlusal assessment provides functional confirmation, postoperative CT offers objective anatomical validation and establishes a documented baseline for follow-up.
The importance of CT was further reinforced during the 8-week re-evaluation. Repeat imaging demonstrated stable mandibular alignment, normal occlusion and satisfactory positioning of both TMJs without evidence of recurrent subluxation. This imaging confirmation supports the durability of the surgical correction and highlights the value of CT, not only for diagnosis but also for postoperative monitoring.
In summary, this case reinforces two key considerations: first, that recurrent open mouth jaw locking associated with structural TMJ abnormalities is best managed surgically; and second, that CT represents an indispensable tool for diagnosis, surgical planning, objective postoperative assessment, and follow-up. Although multiple surgical techniques have been described, current evidence does not indicate clear superiority of one approach over another, and individualized treatment selection based on detailed anatomical evaluation appears most appropriate.
Materials
Semfortan, Dechra Regulatory B.V., Handelsweg 25, 5531 AE Bladel, The Netherlands.
Dexdomitor, Orion Corporation, Orionintie 1A, 02200 Espoo, Finland.
Propovet, Zoetis Spain, S.L.U., Calle Quintanavides 13, Edificio 1, Parque Empresarial Vía Norte, 28050 Madrid, Spain.
Isoflo, Zoetis Spain, S.L.U., Calle Quintanavides 13, Edificio 1, Parque Empresarial Vía Norte, 28050 Madrid, Spain.
Revolution CT, GE HealthCare, Milwaukee, WI, USA.
Rilexine, Virbac, Carros, France.
ClorhexVet, B. Braun VetCare S.A., Rubí, Spain.
MB160D Electrosurgical Uni, GIMA S.p.A., Gessate, Italy.
MB160D Electrosurgical Unit, GIMA S.p.A., Gessate, Italy.
Metzenbaum scissors, Aesculap, Tuttlingen, Germany.
periosteal elevator, Aesculap, Tuttlingen, Germany.
straight osteotome, Aesculap, Tuttlingen, Germany.
Monosyn, B. Braun, Melsungen, Germany.
Dafilon, B. Braun, Melsungen, Germany.
Lactated Ringer's solution, B. Braun, Melsungen, Germany.
Semfortan, Dechra Veterinary Products, Northwich, UK.
Metacam, Boehringer Ingelheim, Ingelheim am Rhein, Germany.
Cefazolina Normon, Laboratorios Normon, Madrid, Spain.
Rilexine, Virbac, Carros, France.
Metacam, Boehringer Ingelheim, Ingelheim am Rhein, Germany.
Betadine, Viatris, Canonsburg, PA, USA.
Click Collar; Buster, Langeskov, Denmark.
Hill's Pet Nutrition, Topeka, KS, USA.
Supplemental Material
Supplemental Material
Supplemental Material
Footnotes
Acknowledgments
The authors thank Dr Jose Roman for his assistance in the translation of the manuscript.
Ethical Approval and Informed Consent
The study describes a clinical case managed according to standard veterinary practice. Written informed owner consent was obtained for diagnostic procedures, surgical treatment and publication of the case details and images.
Author Contribution
AB conceptualized the study, performed the surgical methodology, and prepared the original draft, FSRL performed the surgical methodology, and prepared the original draft, FSR contributed to the writing, review, and editing of the manuscript, CG assisted in the surgical methodology, AC participated in the manuscript review, JL contributed to the review and editing process, MA was responsible for the anesthetic methodology and editing process, AW contributed to the review and editing process.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.