
Abstract
Linguoverted mandibular canine (LMC) teeth are a common form of malocclusion in dogs. If left untreated, contact between the mandibular canine tooth crown tips and the palatal mucosa can result in ulceration, inflammation, infection, and potentially the formation of an oronasal fistula. Various treatment modalities have been described, including both active and passive orthodontic techniques. This report describes the combined use of an active appliance (elastic power chain) and a passive appliance (inclined plane) for the correction of unilateral and bilateral LMC teeth in 2 Shiba Inu dogs. Treatment duration was approximately 60 days in both cases, and follow-up examinations confirmed stable, functional, and atraumatic occlusion. This combined approach may represent an effective and safe treatment option for achieving self-retaining occlusion in similar cases.
Keywords
Introduction
Linguoverted mandibular canine (LMC) teeth are a relatively common malocclusion in dogs. This condition may occur unilaterally or bilaterally.1,2 It may result from a dental abnormality, a skeletal abnormality and trauma, or a combination of these factors. 1 Contact between the mandibular canine tooth crown tips and the palatal mucosa frequently causes discomfort and pain, though typically the dog does not show obvious outward signs of discomfort. However, untreated LMC teeth can lead to mucosal ulceration, inflammation, infection, periodontal and endodontic disease, and even oronasal fistula formation.1–5
Several treatment methods have been described to correct the abnormality or to relieve discomfort for the animal.1–7 Orthodontic appliances may be used to achieve movement of LMC teeth and can be categorized into 2 appliance types (removable or fixed) 1 and 2 force modalities (active continuous force or passive intermittent force). 1 Removable appliances include rubber ball therapy and removable inclined planes. Fixed appliances include acrylic fixed inclined planes, sublingual omega wires, expansion wires or bars, and temporary crown extensions. Other treatment options include surgical repositioning, surgical crown reduction (amputation), 8 extraction, gingivectomy, gingivoplasty and osteoplasty. 9
The cases reported here demonstrate that a combination of active and passive orthodontic appliances was successfully used to correct LMC teeth in 2 dogs; 1 with unilateral and the other with bilateral malocclusion.
Case 1
A 7-month-old, 8.8 kg intact male Shiba Inu dog was referred for the assessment of a linguoverted right mandibular canine tooth (404) (Figure 1). At the time of presentation, the dog was otherwise healthy and, according to the owner, had not shown overt signs of oral discomfort. Clinical oral examination revealed unilateral lingual displacement of 404, with an associated palatal indentation observed on the palatal surface of the right maxillary third incisor (103), consistent with chronic crown tip contact. He was not currently on any medications, and was currently on vaccinations, heartworm, flea and tick prevention.

Case 1. Clinical photograph at presentation showing malocclusion.
Preanesthetic blood work included a complete blood count and serum biochemistry profilea, both of which were within normal limits. A 22-gauge intravenous catheter was placed, and the dog was premedicated with diazepamb (0.3 mg/kg) intravenously (IV) for sedation. General anesthesia was induced with propofolc (6.0 mg/kg) slowly IV to effect. A 6.0 mm cuffed endotracheal tube was placed, and general anesthesia was maintained with isofluraned (1.0%) and oxygen (0.6 L/min). Lactated Ringer's solution was administered IV at 5 ml/kg/hr throughout anesthesia. The right rostral mandible was rinsed with chlorhexidine solution, and full-mouth supra- and subgingival scaling was performed using an ultrasonic scalere. Full-mouth intraoral dental radiographs were taken to examine immature tooth roots using a digital dental sensorf.
A detailed oral examination and dental impressions were performed under general anesthesia. The patient underwent castration at the same time, as no contraindications were identified and since malocclusion may have a hereditary basis, the procedure was elected to prevent future breeding.6,10 The oral examination and dental procedures were not expected to result in bacteremia. The palatal trauma had caused a 4 mm deep ulcerated indentation. Tooth 404 was approximately 80% erupted and was markedly shorter than the left mandibular canine tooth (304) (Figure 2). Intraoral dental radiographs further revealed that 404 had not fully erupted at the time of examination (Figure 3).

Case 1. Photograph of rostral oral cavity showing the significant difference in crown height between the right and left mandibular canine teeth.

Case 1. Radiograph of the right and left mandibular canine teeth showing the open apex and partial eruption of the right canine tooth (arrowhead).
Treatment options for the unilateral LMC tooth 404 included: (1) orthodontic movement; (2) crown reduction with vital pulp therapy; and (3) extraction. Based on the patient's signalment, health status and temperament, orthodontic treatment was the primary treatment option. Stone models created from the dental impressions facilitated discussion of these options with the owners, who consented to orthodontic correction of 404. Crown reduction with vital pulp therapy and extraction were considered alternative treatment options in the event of treatment failure.1,8,11
In preparation for surgery, 2% lidocaineg (0.23 mg/kg) was given as a local anesthetic by performing a right caudal mandibular nerve block. The Ivy loop wiring technique 12 was used to join the right mandibular first and second molars (409 and 410) together as anchor teeth. A single 22-gauge malleable stainless steel wireh was placed interdentally using a wire twister to stabilize and provide anchorage. To ensure adequate anchorage, the loop was placed around teeth 409 and 410. A wired-hook was then fashioned at the mesiobuccal gingival margin of 409 (Figure 4).
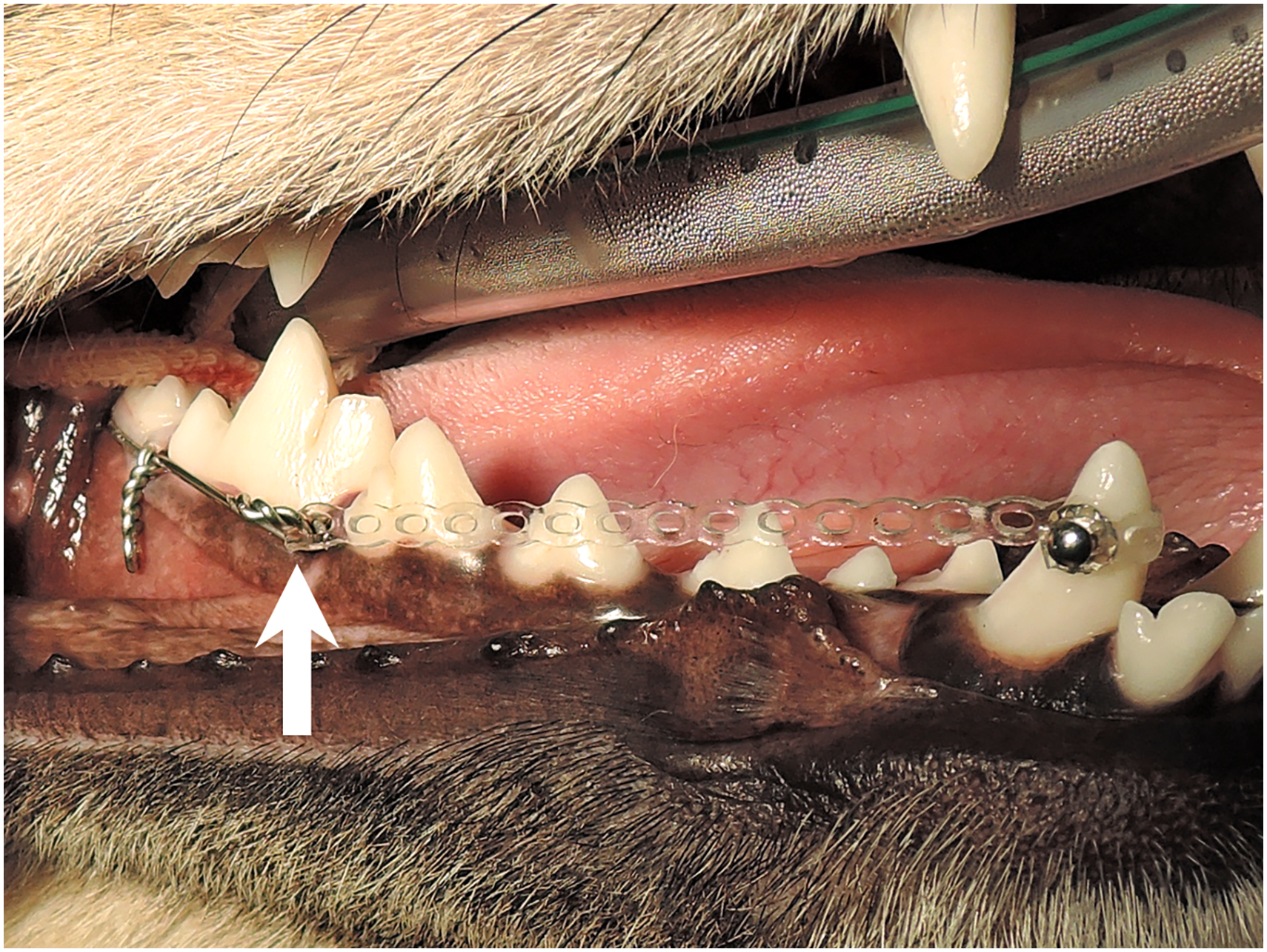
Case 1. Photograph of Ivy loop wiring technique around the right mandibular first and second molar teeth. The elastic power chain was attached to the wire hook (arrow) and routed linguo-mesially to engage the button on the buccal aspect of the mandibular canine tooth, thereby directing distobuccal movement of the tooth.
The crown surface of 404 was thoroughly cleaned using an ultrasonic scaleri and polished with a polishing brush. The mid-buccal crown surface of 404 was etched with 40% phosphoric acid gelj for 15 s, then rinsed thoroughly with water from an air-water syringe on an air-driven dental unit to remove the gel and dried with moisture-free, oil-free air to prevent contamination of the etched site. Bonding agentk was applied with an applicator brush, gently air dried, and light-cured using an LED curing lightl positioned 2 to 3 mm away from the surface of the crown, all following the manufacturer's instructions.
An orthodontic buttonm was cemented on the mid-buccal aspect of 404. An elastic power chainn,o was measured and attached to the hook on 409, routed linguo-mesially around 404, and then secured to the button. The elastic power chain was applied under tension at approximately 75% of its original length, generating a light to moderate tipping force on 404 to avoid excessive stress that could lead to periodontal ligament necrosis and undermining resorption.13,14 The routeing of the power chain would guide tooth 404 to move distobuccally.
The crown surfaces of both maxillary canines and the incisors were also thoroughly cleaned using an ultrasonic scaler and polished with polishing brush. The apical one-third of the buccal crown surfaces of the right and left maxillary canine teeth (104 and 204) were acid-etched, and bonding was carried out as previously described. A figure-of-8 wire was placed around 104 and 204 and held in place by blue-colored restorative materialp applied to buccal edges. An in situ inclined plane device was then created by placing a figure-of-8 wire around the maxillary canines and incrementally adding dental acrylicq, allowing space for 304 to remain in its normal position while directing 404 into proper alignment (Figure 5). 15
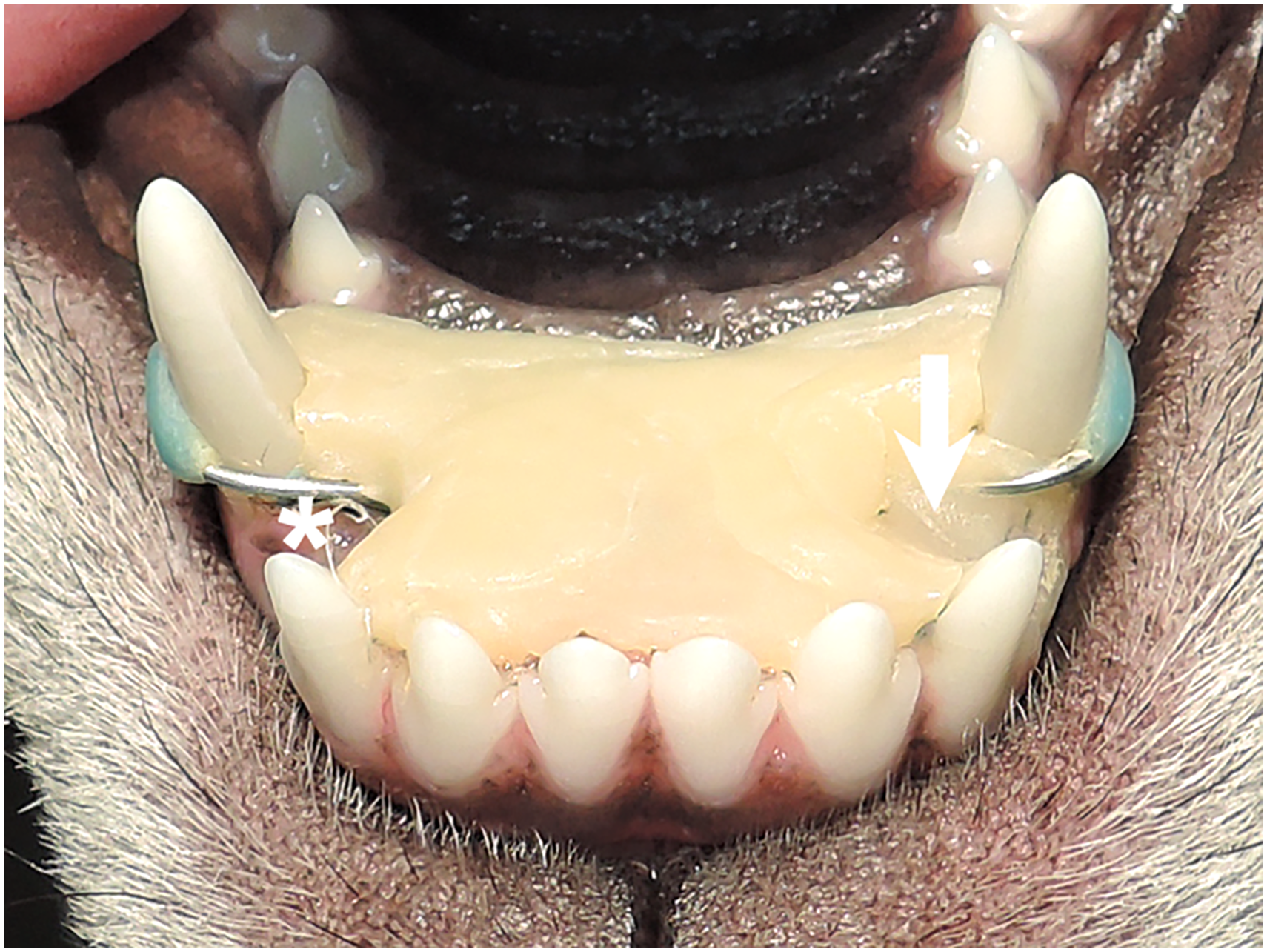
Case 1. Photograph of inclined plane. The inclined plane included a space (asterisk) to retain the normally positioned left mandibular canine, as well as a “track” (arrowhead) designed to guide the right mandibular canine into its correct position.
The owners were informed of the importance of home care for any intraoral appliance and advised to keep all toys out of reach throughout orthodontic treatment. The dog was discharged with instructions for the owner to brush the teeth and irrigate the mouth and appliance with 0.12% chlorhexidine oral rinser twice daily, and to store toys to prevent access. Reexamination was recommended after one week, with plans to replace or adjust the elastic power chain every 7 to 14 days.
The dog was rechecked on Day 17, and the elastic power chain was replaced. At that time, a mild wire-induced marginal gingival ulceration had developed, and contact gingivitis was noted at the buccal gingiva of 409 due to the elastic power chain.
The owners reported that 404 had moved to its target position by Day 19. The elastic power chain was removed at this time, but the inclined plane was intentionally left in place as a retainer because 404 remained obviously shorter than 304. General anesthesia was performed as previously described on Day 28 and the Ivy loop wire was removed. Additional acrylic was added to the palatal aspect of the inclined plane to retain 404 in its correct position.
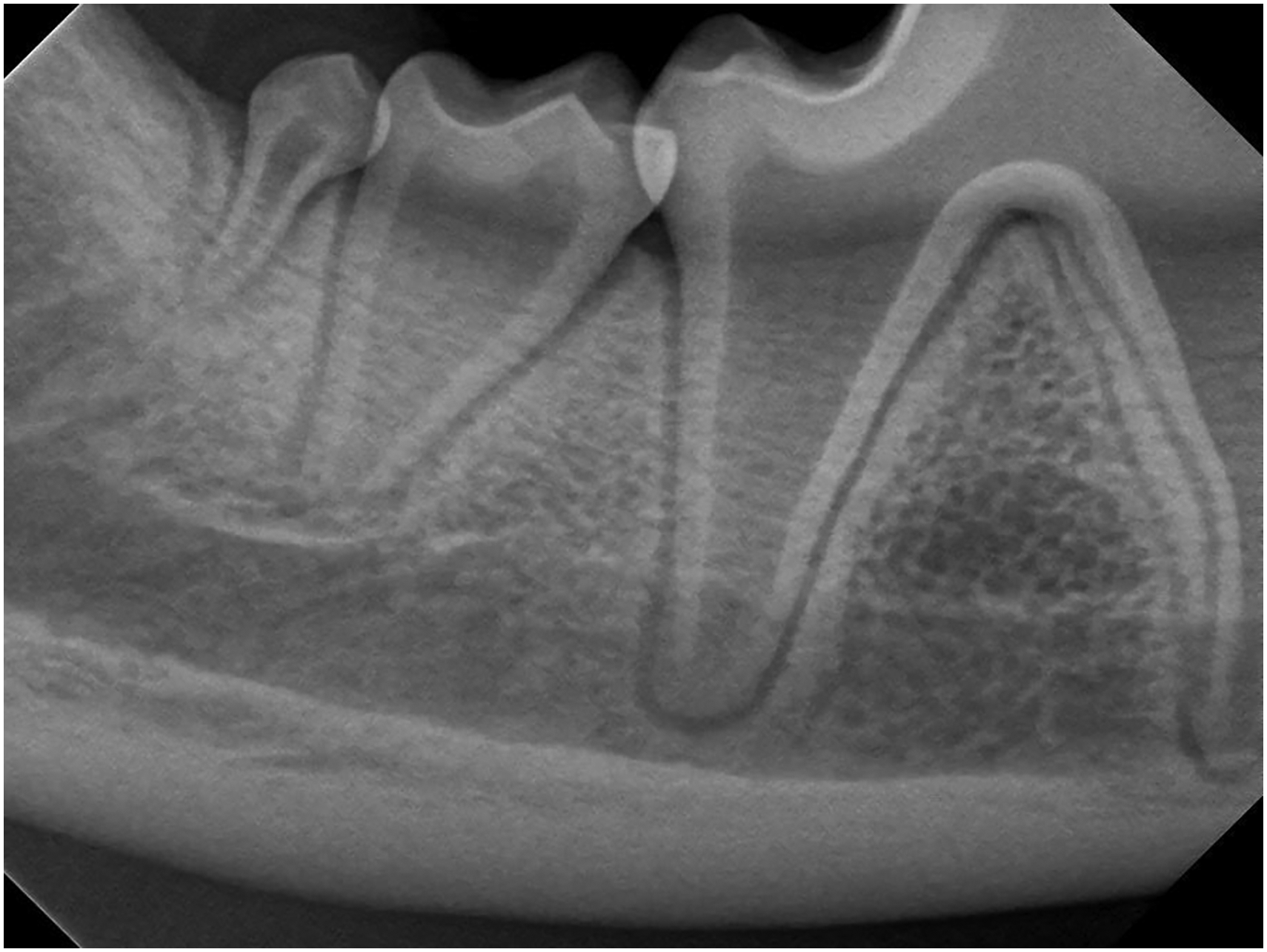
The dog was rechecked on Day 35, and the gingival tissues had healed completely. General anesthesia was again performed as previously described on Day 60 and the inclined plane device was removed. Significant mucositis of the palate was noticed immediately after inclined plane removal (Figure 6). The crown of 404 appeared slightly more exposed than at the previous examination but remained incompletely erupted. The oral cavity was evaluated and charted using a periodontal probes. Full-mouth intraoral dental radiographs were obtained, and radiographic assessment showed that partial-eruption of 404 was unchanged (Figure 7).

Case 1. Photograph of mucositis after inclined plane removal.

Case 1. Radiograph of the right mandibular canine tooth after orthodontic treatment. The apex was nearly closed and the partial-eruption remained unchanged (arrowhead).
The dog was regularly rechecked every 3 to 6 months. At the most recent 2-year follow-up examination, the dog demonstrated functional and comfortable occlusion (Figure 8). Although 404 remained slightly shorter than 304 (Figure 9), the overall occlusion was considered satisfactory.

Case 1. Sequential photographs documenting movement of the right mandibular canine tooth. (A) Before orthodontic treatment. (B) Day 1. Orthodontic appliances were placed. (C) Day 19. The tooth had moved to the maxillary canine–incisor interdental space. Hair entrapment beneath the elastic chain is noted. (D) 2-year follow-up showing normal occlusion.

Case 1. Clinical photograph at the 2-year follow-up. The crown height of the right mandibular canine tooth is slightly shorter than the left mandibular canine tooth.
Case 2
A 7-month-old, 8.4 kg intact male Shiba Inu dog was referred due to constant drooling (Figure 10). Bilateral LMC teeth (304 and 404) with class 1 and 3 malocclusions were diagnosed (Figures 11–13). Although the dog was eating and drinking normally, he exhibited continuous drooling. This was attributed to 2 factors: (1) the palatal discomfort caused by the malocclusion, and (2) difficulty closing the mouth, resulting in saliva flowing outward rather than being swallowed. Clinical oral examination revealed 2 palatal indentations near the palatal-mesial side of the right maxillary third incisor (103) and the left maxillary third incisor (203). He was not currently on any medications. He was up to date with vaccinations, heartworm, flea, and tick prevention.

Case 2. Clinical photograph at presentation. Note the saliva flow over the lower lip.

Case 2. Photograph of rostral view before orthodontic treatments. Note the labioversion of the right and left maxillary third incisor teeth.

Case 2. Photograph of the left mandibular canine tooth before orthodontic treatments.

Case 2. Photograph of right mandibular canine tooth before orthodontic treatments.
Preanesthetic preparation, anesthesia protocol, and associated procedures were performed as described for Case 1. The oral cavity was evaluated and charted using a periodontal probe. Full-mouth intraoral radiographs were obtained, and dental impressions were taken to produce stone models for treatment planning. Castration was also performed during the same anesthetic episode.
The palatal indentations were 4 mm deep and ulcerated. The right maxillary first premolar (105) was missing. The mandibular incisors were crowded, and the mandibular second incisors (302 and 402) were lingually displaced. Labioversion of 103 and 203, rotated maxillary and mandibular premolars, a persistent deciduous left mandibular second premolar (706), an impacted mandibular second molar (310) (Figure 14), and an unerupted right mandibular third molar (411) (Figure 15) were also noted. Tooth 706 was extracted during this anesthesia.

Case 2. Radiograph of the left mandibular molar teeth. Note the pyramidal tooth of second molar.
Case 2. Radiograph of the right mandibular molar teeth. Note the pyramidal tooth of second molar.
Treatment planning and owner consent followed the same approach as described in Case 1, with crown amputation or extraction reserved as alternative options if orthodontic correction was unsuccessful.
As described in Case 1, the Ivy loop wiring technique was used to join 409 and 410, and 309 and 310 as anchor teeth. Hooks were placed at the mesio-buccal line angles of 409 and 309. Orthodontic buttons were cemented on the mid-buccal aspects of the crowns of 404 and 304. The elastic power chains were attached from the hooks on 409 and 309 to the respective buttons on 404 and 304. The linguo-mesial routeing of the elastic power chains guided the mandibular canines distobuccally (Figure 16). An in situ inclined plane device with bilateral inclines was created to direct the mandibular canines into their normal positions (Figure 17).

Case 2. Photograph of Ivy loop wiring technique. Note the restorative material (arrow) applied over the twisted wire to prevent mucosal ulceration.

Case 2. Photograph of inclined plane. The inclined plane had 2 “tracks” (arrows) to direct both the mandibular canine teeth into their desired positions.
The owner was also informed of the importance of home care for any appliance in the mouth and to restrict toys during orthodontic treatment. The dog was sent home with instructions for the owner to brush the teeth and lavage the mouth and appliance with 0.12% chlorhexidine oral rinse twice daily and to ensure the Elizabethan collar was kept on if needed. Reexamination was recommended after one week, with plans to change or adjust the elastic power chain every 7 to 14 days.
The dog was rechecked on Day 9 and new elastic power chains were placed bilaterally. Mild gingival ulcerations induced by the wires and contact gingivitis at the buccal gingiva of 308/309 and 408/409 were observed.
During orthodontic treatment, the orthodontic buttons were repeatedly dislodged. This occurred on Day 13 (right), Day 29 (left), and Day 34 (both). The buttons were replaced under general anesthesia as previously described within 3 days in the first 2 instances, while the last displacement was managed 6 days later due to logistical reasons. On Day 29, the owner reported that 404 had reached its correct position, and on Day 46, that 304 had reached its correct position. The inclined plane device was removed on Day 50, and the Ivy loop wires were removed on Day 59 under general anesthesia again as described previously. By the end of treatment, drooling had ceased.
The dog was rechecked 8 months later, and the occlusion was comfortable and functional (Figures 18 and 19). A stable occlusion was achieved after 59 days of treatment, with teeth 103 and 203 returning to their normal positions (Figure 20).

Case 2. Sequential photographs documenting movement of the left mandibular canine tooth. (A) Before orthodontic treatment. (B) Day 1. Orthodontic appliances were placed, and the elastic power chain was routed lingually to eliminate interference with the maxillary canine. Note the increased mouth opening. (C) Day 59. Orthodontic treatment completed and all appliances were removed. (D) 8-month follow-up. Note the decreased Class 3 malocclusion. The patient was able to achieve greater mouth closure compared with Day 1.

Case 2. Sequential photographs documenting movement of the right mandibular canine tooth. (A) Before orthodontic treatment. (B) Day 1. Orthodontic appliances were placed. (C) Day 59. Orthodontic treatment completed and all appliances were removed. (D) 8-month follow-up. Note the relationship between the maxillary canine and third incisor, and the mandibular canine. The patient is able to close his mouth more than before treatment.

Case 2. Photograph at 8-month follow-up. Improved mouth closure is observed after orthodontic treatment, and both maxillary third incisors are in near-normal alignment.
Discussion
LMC teeth represent one of the most common malocclusions in dogs requiring intervention to achieve a comfortable, functional and atraumatic occlusion.1,2 It is common in dolichocephalic and narrow-jawed breeds such as Collies, Dachshunds, Irish Setters, Standard Poodles, and Greyhounds, but can be seen in almost any breed.1,4,6 Although Shiba Inus do not appear to be overrepresented, the 2 cases reported here both happen to be male Shiba Inus.
Orthodontic appliances used for the correction of LMC include rubber ball therapy, 16 temporary crown extension, 17 expansion devices, fixed acrylic or metal inclined planes,18–21 and removable inclined planes. Although several orthodontic and surgical treatment options (crown amputation with vital pulp therapy, surgical extraction, gingival contouring, or surgical repositioning) have been described,1,4,5,7 selection of the appropriate modality depends on patients’ age, occlusal relationships, stage of eruption, tooth position, and anticipated stability after correction.
Patient age is an important factor influencing orthodontic tooth movement, with younger animals generally demonstrating more favorable tooth movement. 4 In addition, eruption stage is critical for appliance selection, as inclined plane therapy requires sufficient eruption of the affected teeth to allow proper placement and function. Despite these favorable conditions, a fixed inclined plane alone was considered insufficient to achieve predictable correction in both cases presented here.
In both cases, the maloccluded mandibular canines were positioned excessively rostral and were unable to seat naturally within the maxillary canine–incisor interdental space. Without sufficient distal and buccal tipping, passive redirection by an inclined plane would likely have resulted in incomplete correction or relapse. For this reason, additional active force was applied using an elastic power chain to generate controlled distobuccal tipping prior to, and in conjunction with, passive guidance.
The additional orthodontic appliance consisted of Ivy loop wiring technique in conjunction with elastic power chains. The Ivy loop wiring technique is straightforward to perform and does not require specialized orthodontic equipment. It is more commonly used in maxillofacial fracture patients and has become increasingly popular when combined with intraoral acrylic or composite splinting.12,22
In addition, the twisted wire and hooks used in the Ivy loop wiring technique were covered with composite resin to reduce mucosal irritation and patient discomfort in both cases. To provide adequate anchorage, the loop is typically placed around the mandibular first molar and fourth premolar, or the mandibular first and second molar teeth. The total root surface area of the anchor teeth must exceed that of the tooth being moved; otherwise, anchorage teeth may be displaced or the loop may become dislodged.4,23
The elastic power chain was routed linguo-mesially around the mandibular canine teeth to increase buccal tipping force while avoiding interference with the maxillary canines during mouth closure. Excessive force was avoided by limiting activation to approximately 75% of the resting chain length, as excessive orthodontic force may compromise periodontal ligament perfusion and result in necrosis, ankylosis or undermining resorption.4,13,14 The biomechanical objective was to reposition the mandibular canine into a location where natural occlusal interlock could subsequently provide long-term stability.23,24
The combination of active and passive orthodontic appliances has been previously described in the veterinary literature, including temporary crown extensions combined with active force systems and inclined planes combined with power chains.6,17,25 However, reports detailing clinical decision-making, retention strategy, and staged appliance removal remain limited. The present cases illustrate how combining active tooth movement with intermittently active occlusal guidance may be advantageous in selected patients where passive therapy alone may be insufficient.
Retention following correction of LMC is often unnecessary once the mandibular canine seats appropriately within the maxillary canine–incisor interdental space and functional interlock is established.1,6 However, this assumption presumes complete eruption and adequate crown height. In partially erupted teeth, occlusal stability may not yet be sufficient to prevent relapse. 25
In Case 1, correction of the unilateral right LMC required 19 days to reach the target occlusal position. The total duration of orthodontic appliance activity, including retention was 60 days. Tooth 404 remained incompletely erupted radiographically at the completion of active movement. Because crown height was shorter, stable contact with the interdental gingiva was not fully established. Under these circumstances, premature appliance removal may increase the risk of relapse. Therefore, the inclined plane was intentionally maintained as a retainer to permit continued eruption and alveolar bone remodeling before relying on natural occlusal stability.
In contrast, in Case 2, the duration for tooth movement with bilateral LMC teeth was 28 days for 404 and 46 days for 304. The total duration of orthodontic appliance placement, including retention was 59 days. Case 2 demonstrated more complete eruption and improved seating within the interdental space, permitting staged removal of appliances. Sequential removal allowed one appliance to function passively while the other was withdrawn, minimizing the risk of relapse.
Currently, no established guidelines define retention duration in partially erupted mandibular canine teeth. Based on these cases, retention strategy should be individualized according to eruption stage, radiographic findings, occlusal stability, and width of the interdental space.
One of the key considerations in veterinary orthodontics is the total number of anesthetic episodes required over the course of treatment. Orthodontic procedures can be very challenging due to multiple confounding factors, including client compliance, appliance damage by the patient, skeletal changes of the patient during therapy, and unrealistic expectations by the client. 1 Consequently, treatment failure remains possible, and may require additional anesthetic episodes. Such circumstances emphasize the importance of effective veterinarian–client communication to ensure appropriate expectation management and informed decision-making throughout the treatment process.
In Case 1, the patient underwent 4 anesthetic episodes: (1) castration and dentition impression, (2) installation of the inclined plane and power chain, (3) power chain removal, and (4) inclined plane removal. In Case 2, 6 anesthetic episodes were performed: (1) castration and dentition impression, (2) installation of the inclined plane and power chain, (3) reapplication of the left orthodontic button, (4) reapplication of both orthodontic buttons, (5) inclined plane removal, and (6) power chain removal. Replacement of the power chain and all routine examinations during the treatment were performed while the patient was conscious.
Orthodontic treatment in veterinary patients necessitates repeated anesthetic events, which should be minimized whenever possible. Ideally, appliance placement and removal require 2 anesthetic episodes. However, additional procedures such as castration, appliance dislodgement, or staged appliance removal may increase the time and number of anesthetic episodes depending on patient-specific circumstances.
Careful case selection, secure bonding technique, and thorough owner education are critical to reducing the likelihood of appliance failure and additional anesthetic exposure. When appropriate, adjunctive procedures such as castration surgery and pretreatment dentition impression may be combined within a single anesthetic event.
In both cases, dental impressions were performed under the same general anesthesia as the castration procedures, without requiring additional anesthetic episodes. Ideally, these procedures could also be combined with orthodontic appliance placement to further minimize the number of anesthetic events.
Dental stone models facilitate communication with owners, contribute to clinical documentation, and assist in treatment planning.1,5 In clinical practice, dogs with malocclusions are often reluctant to tolerate repeated oral examinations, making visual demonstration and discussion of the condition more challenging without such models.1,5
The main challenge in Case 2 was the dislodgment of the orthodontic buttons. To prevent this, the owner must avoid any toys and maintain strict environmental control to reduce the risk of chewing and playing behaviors of the patient that could compromise the appliances. Close monitoring by the owner is essential, if continuous supervision is not possible, the use of an Elizabethan collar becomes necessary. 1 Additionally, familiarity with the dog's behavior and chewing habits is an important factor in facilitating client communication and in providing appropriate guidance to prevent damage to the orthodontic appliances. Replacement of one button 7 days after it was lost resulted in prolonged treatment duration. Fortunately, the inclined plane continued to provide an intermittent force on the target tooth, preserving treatment already achieved.
Another potential cause of orthodontic button dislodgment could be the selection of the light-cure orthodontic adhesive resint. The commercial adhesive resin used in these cases may not have provided sufficient bond strength to withstand orthodontic forces, thereby contributing to an increased number of anesthetic episodes. In contrast, in other orthodontic cases, the authors have used the same metal buttons for both anchorage units and target teeth, embedded in a blue-colored restorative composite material, with dislodgment occurring infrequently. Based on personal observation, using restorative composite material to encompass the metal button could be better than using commercial orthodontic adhesive resin. Regardless of the bonding agent selected, practitioners should ensure proper bonding technique and adhere strictly to the manufacturer's instructions. After attachment, the button should always be firmly rocked to confirm adequate bonding. 4
The disadvantages of the inclined plane include gingival and palatal mucosal irritation, fracture or loss of the appliance, and restriction of maxillary growth in younger patients if left in place for a longer time.2–4 Mucosal and gingival inflammation associated with the inclined plane is common, particularly when the appliance extends onto the palatal mucosa. 1 In both cases, the inclined plane was additionally attached to the maxillary first and second incisors to improve appliance stability and reduce the risk of displacement that might occur if the appliance were attached only to the maxillary canines and third incisors. However, this design may potentially influence the development of the incisive bone and rostral maxilla, increase the difficulty of oral hygiene maintenance, and result in more extensive palatal inflammation.1–5
Despite these concerns, both patients in the present report were older than 6 months of age, which is considered appropriate for inclined plane therapy. 1 In addition, with relatively short treatment duration and sufficient interdental space between the maxillary third incisors and canine teeth, it was considered unlikely there would be significant interference with maxillofacial growth. Daily oral home care, including the use of an oral rinse when feasible, may help reduce plaque accumulation around the appliance, and inflammatory lesions generally resolve shortly after appliance removal. Nevertheless, prolonged use of the inclined plane should be avoided, as chronic contact ulceration may lead to bone exposure and significant patient discomfort.
Dental radiographs are an essential component of orthodontic assessment that should not be overlooked.1,4,26 The primary purpose of full-mouth dental radiographs prior to orthodontic treatment is to confirm the presence, position, and integrity of the permanent dentition and tooth root, identify teeth that are malpositioned, supernumerary, unerupted, or missing, and to detect pathology of teeth intended for movement or anchorage. These evaluations are critical for risk assessment, prognosis determination, and treatment planning.1,4,26
In the present study, for example, dental radiographs revealed mesioversion and a pyramidal root of tooth 310, a pyramidal root 27 of 410 in Case 2, as well as the infra-eruption of 404 in Case 1, and these were incorporated into the treatment plan. Any teeth that may need to be moved or used as anchorage should undergo radiographic evaluation both to identify perioperative pathology and for comparison with postoperative radiographs.24,26
The major limitation of this study is the small number of cases. The limited sample size may restrict the generalizability of the combination of active and passive orthodontic appliances, and this highlights areas for improvement in future cases.
The present study demonstrated 2 cases of LMC treated using a combination of active (power chain) and passive (inclined plane) orthodontic appliances, which proved to be an effective and safe approach for correcting LMC. This treatment strategy not only achieved self-retention, comfortable and functional occlusion but also minimized trauma to the surrounding tissues, suggesting that the combined use of these orthodontic appliances may offer a practical and reliable option for managing similar malocclusions in clinical veterinary practice.
Materials
ProCyte Dx and Catalyst one, IDEXX Laboratories, Inc., Westbrook, ME, USA
Diazepam injection, Astar, Hsinchu, Taiwan
Fresofol, Fresenius Kabi, Graz, Austria
ISO, Terrell, Piramal Critical Care Inc., Bethlehem, PA, USA
Ultrasonic scaler, Cavitron Select SPS Ultrasonic Scaler, Dentsply Sirona, Charlotte, NC, USA
Dental radiographs, Midmark DR Digital Dental Sensor, Midmark, Dayton, OH, USA
Lidocaine, Tai Yu, Hsinchu, Taiwan
Stainless steel wire, Mizuho, Tokyo, Japan
iM3 Silent Hurricane Compressor, iM3, Vancouver, WA, USA
Phosphoric acid gel, Ultra-Etch™, Ultradent, South Jordan, UT, USA
Bonding agent, 3M™ Single Bond Universal Adhesive, 3M Oral Care, Saint Paul, MN, USA
Pen-Style LED Curing Light, Dentsply Sirona, Charlotte, NC, USA
Orthodontic button, Tomy Lingual Button, Tomy, Tokyo, Japan
Elastic power chain, closed type 2.8 mm Elastomeric Chain, G&H Orthodontics, Franklin, IN, USA
. Mighty-Tuff Chain Elastics, OSE, Gaithersburg, MD, USA
Blue colored restorative material, OPTIBAND™ ULTRA, Ormco, CA, USA
Dental acrylic, Tempron, GC corporation, Tokyo, Japan
Chlorhexidine oral rinse, Ligecon gargle, Washington Pharmaceutical Company, Kaohsiung, Taiwan
Periodontal probe, Hu-Friedy, Chicago, IL, USA
Light-cure orthodontic adhesive, Orthomite LC, SUN MEDICAL, Shiga, Japan
Footnotes
Acknowledgment
The authors would like to thank Tzu-Hsien Yang for assistance with manuscript preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.