
Abstract
Human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) is a multisystem disease that can involve the human eyes. Using ophthalmic examination records from January 2006 to November 2015, we retrospectively reviewed all patients who were diagnosed with HIV/AIDS in our hospital. The study was performed at a tertiary referral center in southern Taiwan. Data included age, gender, ophthalmic examinations, systemic conditions, CD4 cell counts, course, and treatment. Eleven patients were identified as having AIDS with uveitis as their presenting manifestation. All were men, with a mean age of 39.5 ± 11.4 years (range 24–56). The mean CD4+ T-cell counts were 91.7 ± 50.3 cells/μl (range 27–169). Ocular diagnoses included cytomegalovirus (CMV) retinitis in five patients, ocular syphilis in four patients, and ocular toxoplasmosis in two patients. Uveitis resolved in all patients after medical treatment. However, a retinal detachment developed in two eyes in CMV retinitis and one eye in ocular syphilis. Ocular manifestations are among the most common clinical features in patients with HIV/AIDS who have varying clinical presentations that affect almost all ocular structures. This study demonstrated that ocular findings could be an initial manifestation of an underlying disease. Awareness of ocular lesions in HIV/AIDS is important for early recognition and management.
Keywords
Introduction
Acquired immunodeficiency syndrome (AIDS) was one of the most feared infectious diseases in the late 20th century. A report from WHO/UNAIDS/UNICEF (2011) estimated that 34 million people were living with human immunodeficiency virus (HIV)/AIDS. 1 HIV infection is usually associated with a wide spectrum of diseases and is also a multisystem disorder. Ophthalmic disease affects 50–75% of patients with HIV infection at some point during the natural history of their infection,2,3 which ranges from adnexal disorders to posterior segment disorders, including the optic nerve and optic tract. Unfortunately, large proportions of patients are unaware that they have an HIV infection until severe complications develop. Hence, although rarely reported, ocular manifestations can be the presenting sign of a systemic infection in an otherwise asymptomatic individual. In this report, we will discuss 11 patients who had infectious uveitis as their initial feature and were subsequently diagnosed with an HIV infection.
Methods
This study is a retrospective review of charts including ophthalmic examination records of patients diagnosed with HIV/AIDS at a tertiary medical center in southern Taiwan between January 2006 and November 2015. The institutional review board and ethics committee approved this study (VGHKS16-CT2-05), which adhered to the tenets of the Declaration of Helsinki. All patients were serologically confirmed with HIV infection and by definition with AIDS with CD4 cell counts of <200. Clinical data obtained from case records included age, gender, duration of symptoms, ophthalmologic examinations, follow-up duration, systemic conditions, CD4 cell count, course, and treatment. The diagnosis of cytomegalovirus (CMV) retinitis in our series was based on serological results associated with the characteristic picture of large areas of retinal hemorrhage against a background of whitened, edematous, or necrotic retinas. Atypical presentation of CMV retinitis is often described as frosted branch angiitis that was also observed in the present study and is characterized by widespread retinal vasculitis with severe sheathing of the retinal vessels. As ocular syphilis can mimic numerous ocular inflammatory conditions such as iritis, chorioretinitis, vasculitis, vitritis, or papillitis, diagnosis was usually based on the following: comprehensive history taking, and physical examination, as well as high initial titers in a Treponema pallidum hemagglutination test and venereal disease research laboratory (VDRL) with subsequent response to penicillin treatment. Diagnosis of ocular toxoplasmosis was based on typical fundus pictures and serological results.
Results
Demographic and clinical features.
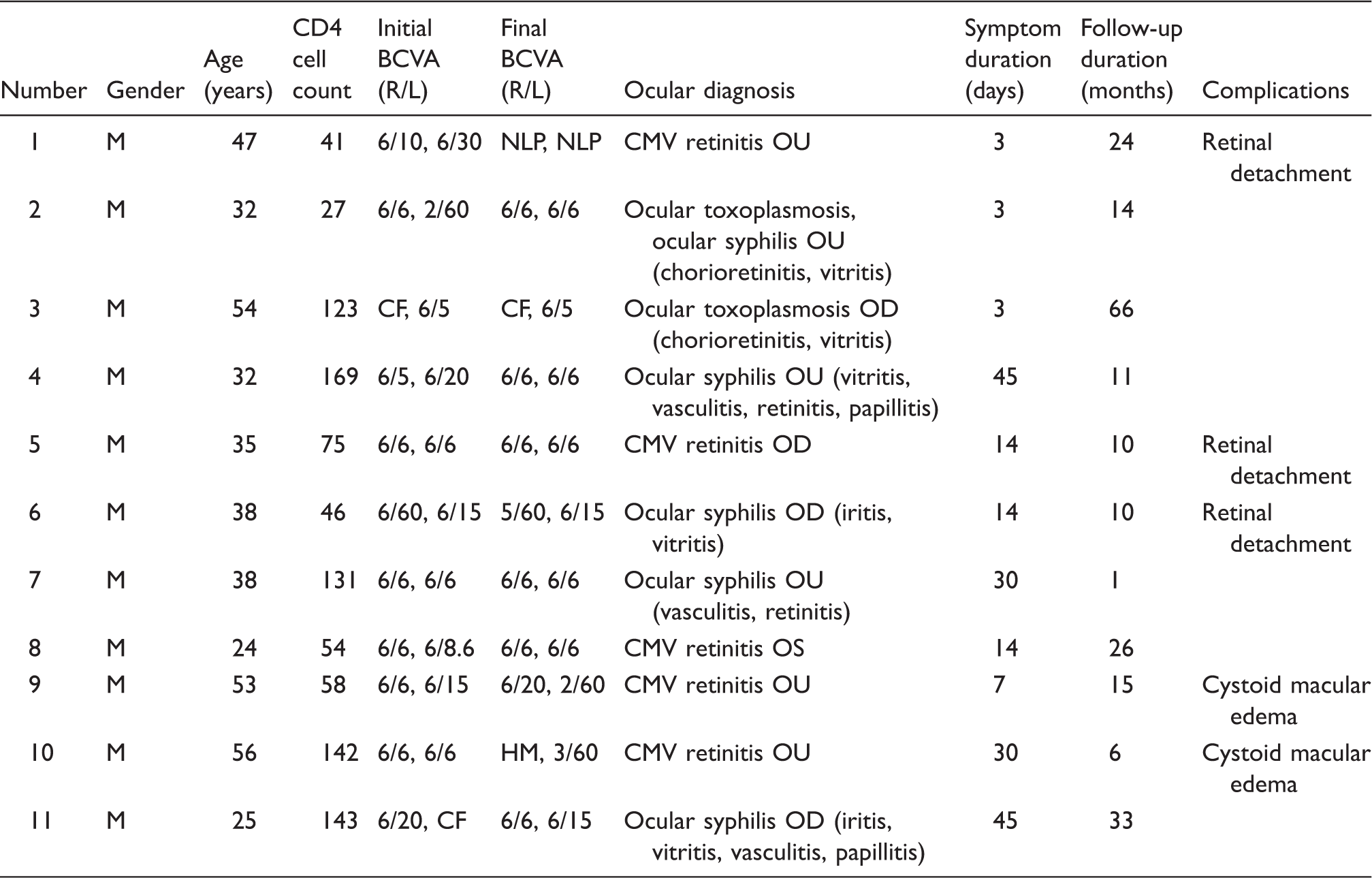
BCVA: best corrected visual acuity; CF: counting finger; CMV: cytomegalovirus; L: left; R: right; M: male; NLP: no light perception; OD; oculus dexter (right eye); OU; oculus uterque (both eyes); OS: oculus sinister (left eye).
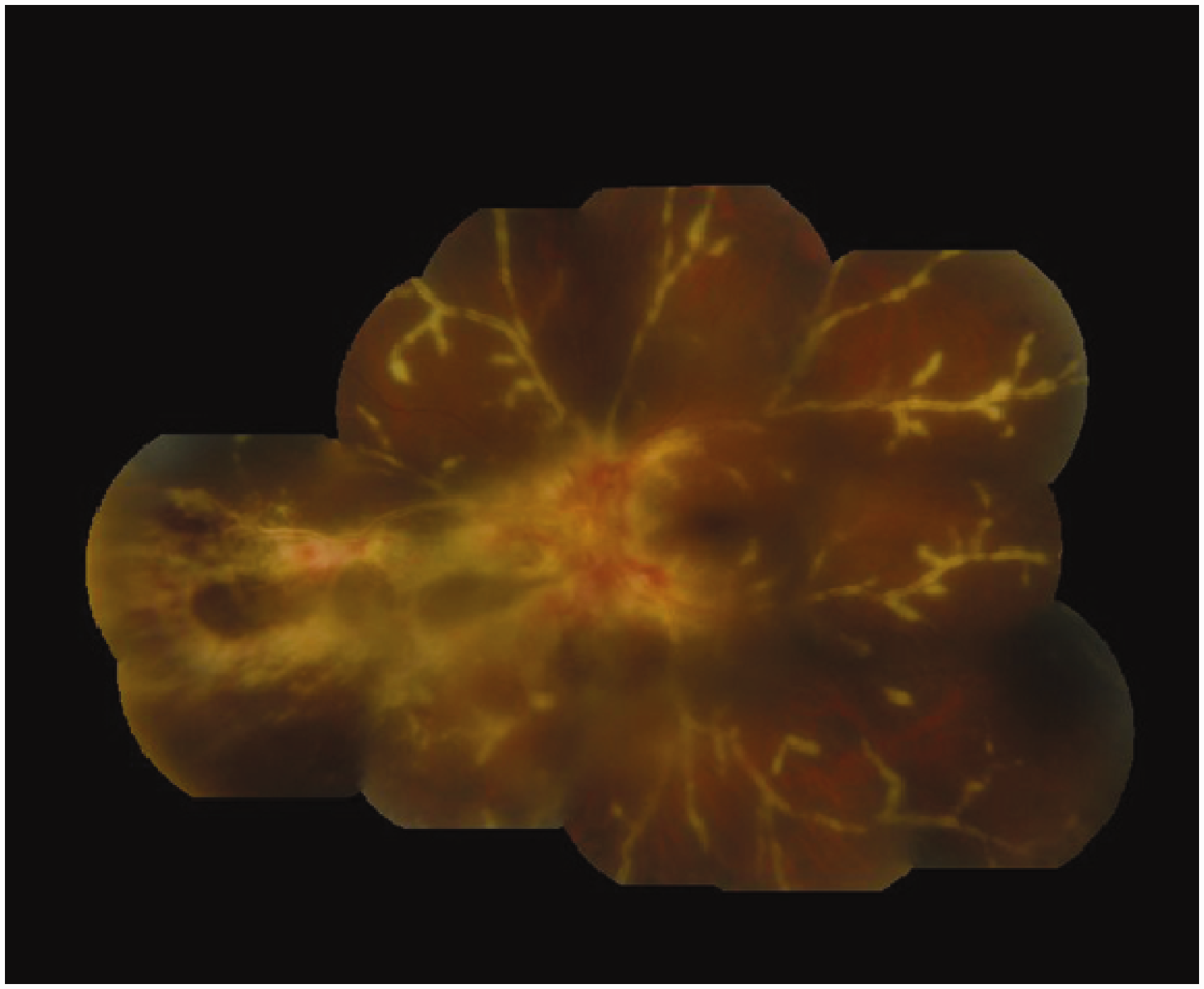
Fundus photo demonstrating fulminant CMV retinal necrosis and frosted branch angiitis in case No. 8. CMV: cytomegalovirus.
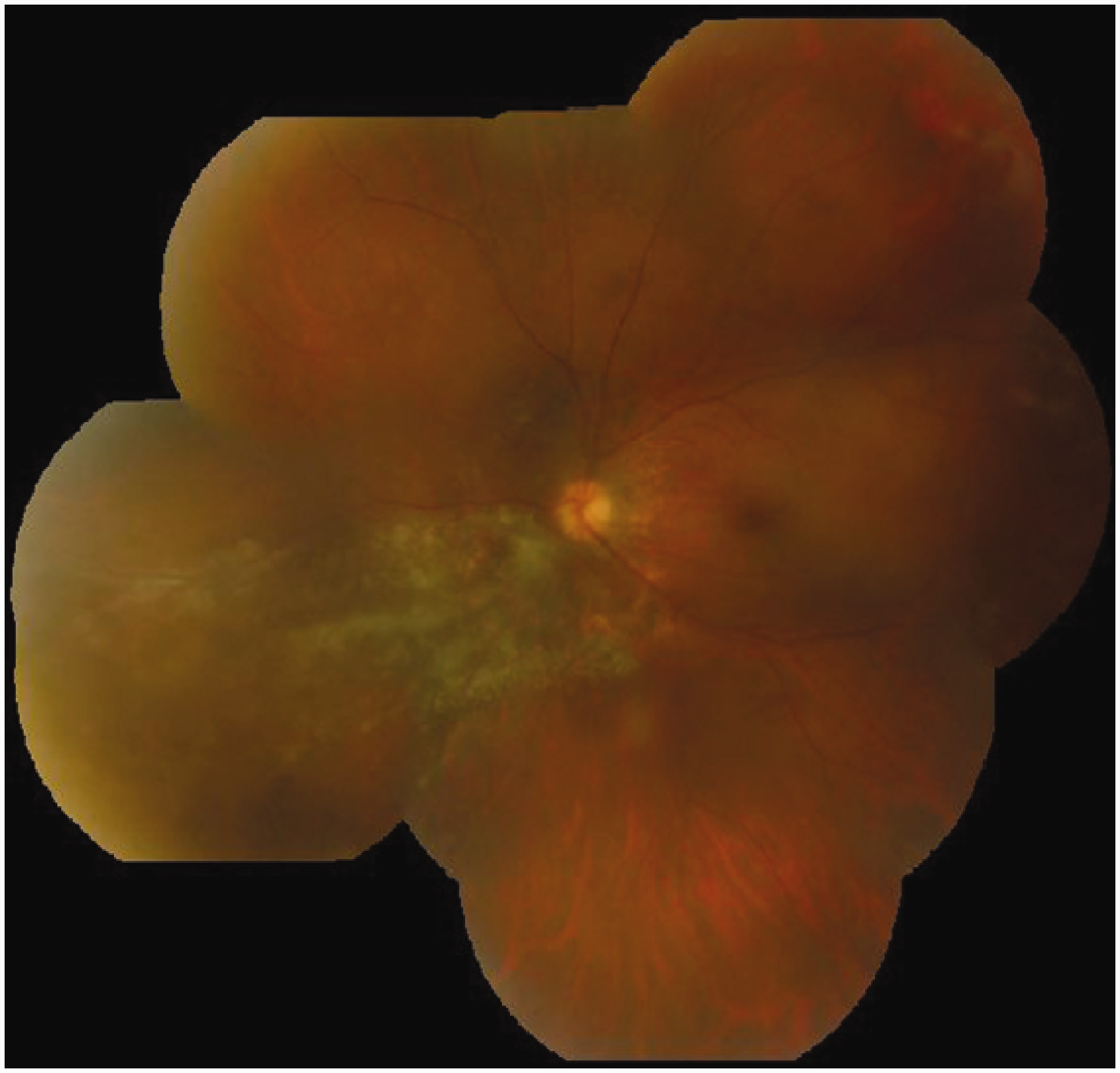
Regressed CMV retinitis with retinal atrophy and pigmentary changes was observed after HAART combined with systemic anti-CMV therapy. CMV: cytomegalovirus; HAART: highly active antiretroviral therapy.
Discussion
Ocular manifestations occur in a substantial proportion of patients with HIV/AIDS, and more than one-half of patients also have an associated infectious or noninfectious uveitis. 4
Previous studies revealed that the most prevalent initial presentations of acute HIV infection included fever, fatigue, myalgias/arthralgias, rash, headache, pharyngitis, lymphadenopathy, mucocutaneous ulcerations, or diarrhea. 5 Although ocular complications occur in up to 50–75% of untreated HIV-infected patients, ocular complications were rarely reported as the initial manifestations in patients with HIV/AIDS. 6 Most of the severe complications developed during the advanced stages of the disease, most often as CD4+ T-lymphocyte counts dropped below 50 cells/μl.7,8 In this series, we reported on 11 patients with uveitis as an initial presentation who were subsequently diagnosed with HIV infection. All patients were relatively young men who recently developed ocular symptoms. Their CD4 cell count at the time of diagnosis was all below 200 cells/μl. These data suggested that these patients have been infected with HIV for a period of time that helped us to differentiate between HIV-related and non-HIV-related ocular manifestations. All cases with uveitis were infectious, including CMV in five patients, syphilis in four patients, and toxoplasmosis in two patients (one was coinfected with syphilis). However, the distribution of the infectious etiology in this series was not compatible with the distribution of infectious uveitis in our hospital: herpes simplex virus was first, followed by CMV and syphilis. 9
CMV retinitis was the most frequent opportunistic ocular infection in HIV-infected patients, especially patients whose CD4 cell count was <50 cells/μl. 8 It also remains the most common cause of permanent visual impairment in patients with HIV/AIDS.10–13 Full-thickness retinal necrosis can lead to retinal breaks, retinal detachments, and ultimately, severe visual loss. With the introduction of HAART, HIV/AIDS-related morbidity and mortality have significantly declined. This therapy provided immune system recovery by increasing the CD4+ T-lymphocyte counts and decreasing HIV viral loads. The availability of HAART has resulted in a decline in not only mortality but also CMV retinitis and its associated complications. 12 In the current study, CMV retinitis affected five of the 11 cases (45%), but only one patient had CD4 cell count of <50 cells/μl at the time of diagnosis. The mean CD4 cell count in patients with CMV retinitis was 74 ± 40.9 cells/μl (range 41–142). The inflammation responded well to treatment, but retinal detachment developed in three eyes in two patients, with a poor outcome.
Unlike the marked decline demonstrated in CMV retinitis after the introduction of HAART, the incidence of ocular syphilis has not decreased in the HAART era. 14 Uveitis is the most common ocular manifestation in syphilis and may occur during both secondary and tertiary stages. Other possible manifestations include iritis, vitritis, retrobulbar optic neuritis, perineuritis, papillitis, neuroretinitis, retinal vasculitis, necrotizing retinitis, and exudative retinal detachment. 15 In our series, ocular syphilis was serologically confirmed in five of the 11 patients (45%). The most frequently observed ophthalmic features were retinal vasculitis (80%) and vitritis (60%). Posterior segment involvement was observed in all patients with syphilis, and anterior chamber reaction was noted in two of the five patients (40%). In addition, neurosyphilis was diagnosed in two of the five patients based on their reactive cerebrospinal fluid VDRL. Ocular syphilis does not seem to be correlated with CD4 cell count in patients with HIV/AIDS.16,17 In our study, the mean CD4 cell count was 103 ± 62.8 cells/μl (range 27–169) in patients with ocular syphilis. Restivo et al. reported on a series of 14 cases of uveitis with previously unknown luetic and HIV infection. Panuveitis is a pattern in concomitant HIV infection and posterior uveitis in HIV-negative patients. 18 This difference did not exist in our cases as all involved the posterior segment and one-half of them had panuveitis. The severity and distribution did not correlate with the CD4 cell count either. Moreover, one patient with bilateral ocular toxoplasmosis had syphilis coinfection that was confirmed with a serologic study. Our data supported evidence from other studies that syphilis is an important concomitant infection in patients with AIDS.
Toxoplasmosis is usually self-limited in immunocompetent persons but life threatening in immunocompromised patients.19,20 In Taiwan, two major risk factors associated with toxoplasmosis were raw shellfish consumption and domestic cat exposure. 21 One of our patients had eight cats at home. In patients with HIV/AIDS, atypical presentations of ocular toxoplasmosis may mimic retinal necrosis from viral infections, syphilis, or intraocular lymphoma and often inevitably progress without adequate treatment. 22 In our series, two of the 11 patients (18%) who had serologically proven toxoplasmosis infection presented with significant vitritis and typical chorioretinitis. One of our cases was coinfected with syphilis. If the patient attends late in the clinical course and the stage when IgM is positive has passed, he might be treated as syphilis only and the retinitis might progress. The inflammation responded well to systemic anti-toxoplasmosis treatment; however, the patient’s vision did not recover in one eye because a macular scar developed.
In conclusion, our results demonstrated the possibility that inflammation of the uveal tract may represent the presenting features in patients with HIV/AIDS. Although the CD4 cell count was <200 cells/μl in all cases, only three had CD4 cell counts of <50 cells/μl. All cases had opportunistic infections involving the posterior segment. Early, aggressive treatment did resolve the inflammation in all eyes, but sight-threatening RD developed in three eyes and limited the visual outcome. Therefore, comprehensive ocular examinations, thorough past medical history taking, and systemic investigation are important in uveitic patients with atypical presentations, especially in the relatively young group in our study. Awareness of ocular manifestations is crucial to early recognition and management of occult HIV/AIDS. Early diagnosis and treatment may save not only the eyes but also lives.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.