
Abstract
Background
Testosterone-associated vulvovaginitis is an under-recognised cause of genital symptoms in transmasculine patients receiving testosterone as gender-affirming hormone therapy, with 5-years prevalence 64-78%. BASHH’s Gender and Sexual Minorities Special Interest Group convened sexual health, gender, gynaecological and primary care experts and patient representatives to formulate a first-in-world best practice statement.
Method
We searched Medline, Embase, CINAHL, UpToDate, Trip Medical Database and Cochrane, to April 2025, regarding testosterone’s impact on transmasculine people’s vaginal histology and microbiomes, symptoms, and management. Papers on cis- or transgender women, editorials, and study protocols were excluded. Included studies were assessed using the Critical Appraisal Skills Programme tool. Recommendations for best practice were graded using GRADE methodology where possible, and supplemented by expert group consensus where evidence was limited.
Results
14 papers were included, of which 11 were descriptive/non-management focused. Testosterone is associated with vaginal Lactobacilli depletion, increased speciation, pH changes, atrophy, inflammation, and epithelial cell differentiation shift. The diagnosis of testosterone-associated vulvovaginitis is clinical; symptom severity does not reliably correlate with any of the above, nor other markers such as hormone levels. Two small case series and one cohort study (total n = 12) discussed treatment; topical estrogen reduced vaginal symptoms and increased Lactobacilli, with some refractory inflammatory cases requiring topical clindamycin +/− topical steroids. Presumed efficacy and safety are extrapolated from topical estrogen use in cisgender menopausal women.
Conclusion
Specific evidence for testosterone-associated vulvovaginitis management is lacking; we suggest a culturally competent approach, considering it as a differential in any transmasculine people on testosterone with genitourinary symptoms. Offer examination (if possible) to exclude infection or dermatoses; offer first-line treatment with topical vaginal estrogens. Adjunctive/alternative measures include emollients and lubricants; topical clindamycin +/− topical steroids for refractory cases or aerobic/desquamative vaginitis. Long-term maintenance therapy and review is advised. Robust trans-specific clinical trials are needed to strengthen the evidence and optimise long-term outcomes.
Objective and scope
This is the first British Association for Sexual Health and HIV (BASHH) best practice statement regarding the management of testosterone-associated vulvovaginitis in transmasculine individuals.
This statement is aimed at all clinicians managing genitourinary symptoms arising in transmasculine patients – an umbrella term referring to transgender men and non-binary patients registered female at birth. Settings may include primary care, general medicine, gynaecology, urology, sexual health and reproductive/genitourinary medicine clinics, gender identity clinics and gender-affirming surgery teams.
Stakeholder involvement
This best practice statement has been developed by a writing group including clinicians working in the fields of genitourinary medicine, obstetrics and gynaecology, general practice, and patient and public representatives. The statement has been reviewed by the BASHH Public Panel, circulated to external stakeholder groups including the British Society for the Study of Vulval Diseases, the British Menopause Society, the British Association of Dermatologists, the British Association of Gender Identity Specialists; and piloted for validation by a sample of target users, per BASHH Clinical Effectiveness Group (CEG) guidelines.
Search strategy
Searches were made according to the BASHH CEG development framework (https://www.bashh.org/_userfiles/pages/files/resources/2020_guidelines_framework.pdf).
A systematic review of literature published up to April 2025 was conducted. Databases searched included Medline, Embase, and CINAHL, alongside point-of-care resources such as UpToDate, the Trip Medical Database, and the Cochrane Library of Systematic Reviews. Inclusion criteria were: articles in English investigating the vaginal microbiota, histology, symptoms or treatments in transmasculine individuals using testosterone. Original research, reviews, and case series were included. Exclusion criteria were: studies focused on cisgender women or transgender women, editorials, and study protocols. Included studies were screened for sample size and relevance to transmasculine populations on testosterone, and assessed using the relevant Critical Appraisal Skills Programme tool, 1 where possible, according to their methodology.
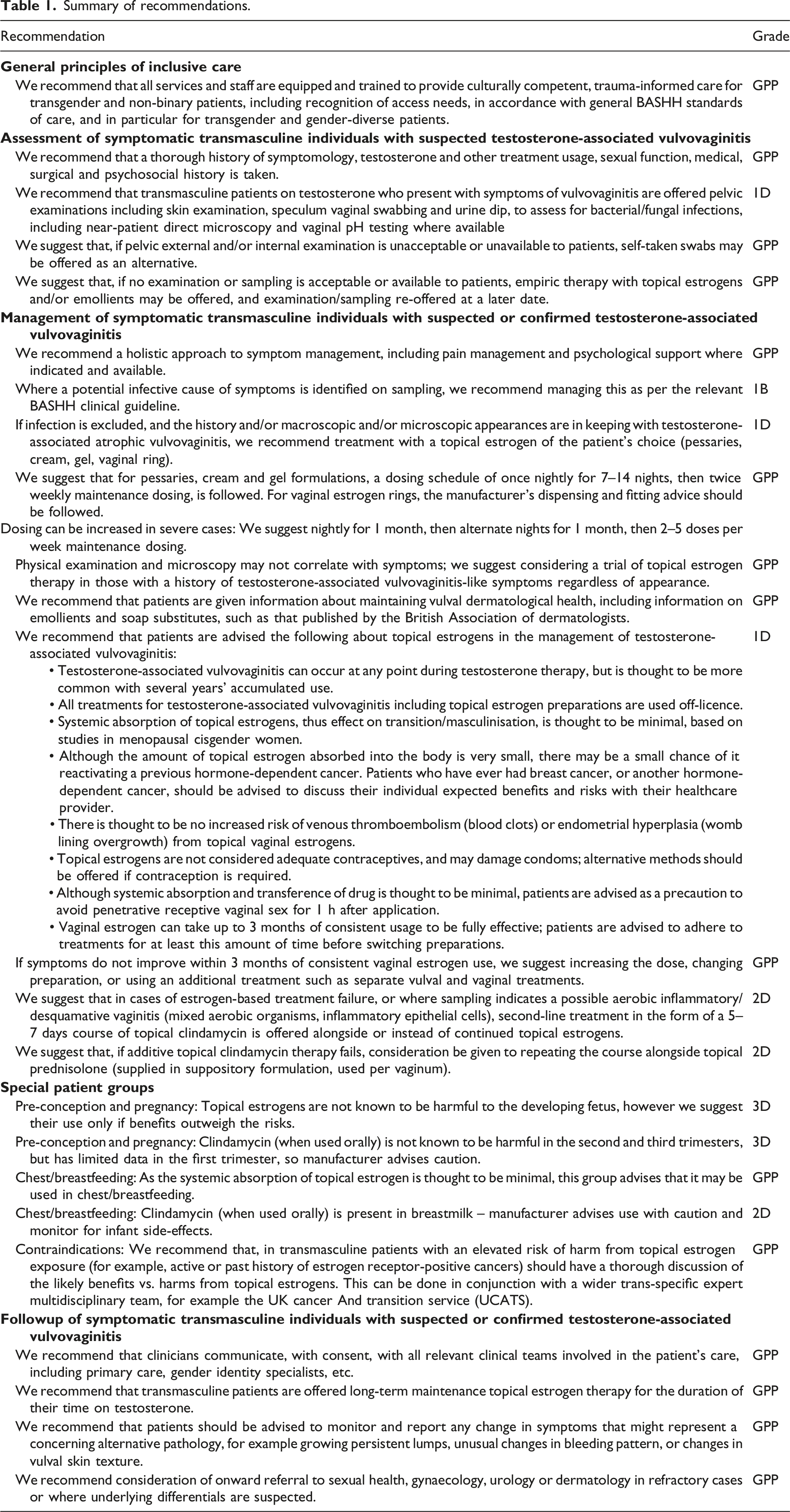
Summary of recommendations.
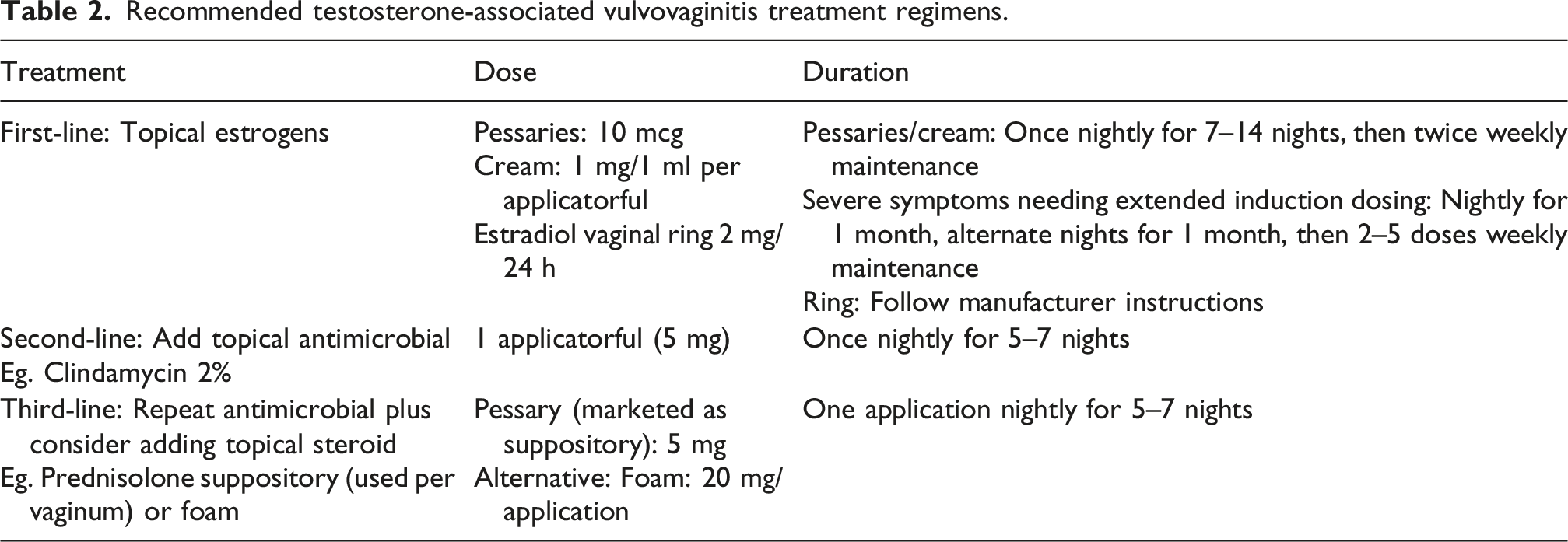
Recommended testosterone-associated vulvovaginitis treatment regimens.
Background and aetiology of testosterone-associated vulvovaginitis
There are increasing numbers of transgender and gender-diverse individuals receiving gender affirming care. 3 Transmasculine individuals on testosterone-based gender-affirming hormone therapy report high levels of symptoms of genital and pelvic pain – up to 64–78%.4–6 This is likely to be under-recognised and under-reported in non-research based clinical settings by patients and clinicians alike. In those who use testosterone as gender-affirming hormone therapy, this may trigger symptoms of vaginal atrophy and vulvovaginitis, via a variety of proposed mechanisms.
Testosterone use is associated with a vaginal microbiome depletion in Lactobacilli species.7–11 The vaginal epithelium of transmasculine individuals using testosterone shows atrophic changes and shifts in epithelial cell differentiation compared to cisgender female controls.12–14 No statistically significant correlation was found between serum estradiol or testosterone levels and vaginal microbiome, pH, or symptoms.7–9
One n = 4 case-control study 8 and two case series of n = 3 and n = 4 respectively15,16 reported on the treatment of vulvovaginal symptoms in transmasculine individuals on testosterone. The former two papers8,15 featured patients being treated with primarily topical estrogen-based therapies, with two patients also requiring topical antimicrobials; the latter case series 16 reported on treating aerobic desquamative vaginitis in transmasculine patients with antimicrobial and steroid-based therapies. All remarked that an evidence base is lacking, thus existing clinical practice in the treatment and dosing advice for testosterone-associated vulvovaginitis is based on clinical experience and protocols for vaginitis in cisgender post-menopausal women.17,18
Efficacy, tolerability and safety of all the abovementioned treatments have not been evidenced in transmasculine-specific populations.
General principles of transgender-inclusive care
The difficulties and barriers that transgender patients commonly face in seeking competent and trustworthy healthcare are well-recognised. 3
We recommend that all services and staff are equipped and trained to provide culturally competent, trauma-informed care for transgender and non-binary patients, in accordance with BASHH Standards of Care for Transgender and Gender-Diverse Patients. 19
Marginalised groups such as transgender and non-binary people often experience multiple indices of social disadvantage, which may impact on their ability to present and adhere to therapies, such as financial barriers, physical or mental comorbidities or neurodivergences, and we recommend that service access, treatment planning and recall systems are designed with this in mind.
Many individuals suffering with dysphoria around their genitals may not actively present with symptoms relating to their anatomy, and only on specific sensitive questioning may the extent of their symptoms become evident.
Clinical features and diagnosis
We recommend (GPP) that a thorough history of symptoms should be taken, including: - Bleeding patterns - Characterisation of any discharge - Symptoms of vulval pain/pelvic pain syndrome - Washing habits/douching - Urinary/bowel symptoms - Sexual history (including any effect on sexual function and quality of life) - Medical/gynaecological/surgical history, or intended plans for surgery including gender-affirming procedures, such as hysterectomy +/− salpingo-oophorectomy +/− vaginectomy, metoidioplasty, phalloplasty - Therapies used, including testosterone/hormone history/contraceptive use, plus any previous treatments tried (prescribed and self-sourced) - Cervical screening history, if applicable.
Testosterone-associated vulvovaginitis in transmasculine patients is a clinical diagnosis, and may be characterised by any of the following symptoms, in the context of current or previous testosterone usage, and particularly in long-term testosterone users (GPP): • Dryness, itching, and/or irritation of the vulvovaginal area • Vaginal bleeding/bleeding after penetrative intercourse • Pallor, friability/contact bleeding, and/or atrophy of the vulvovaginal mucosae • Dysuria • Dyspareunia (shallow and/or deep) • Vulvovaginal pain syndrome(s) including vulvodynia or vaginismus; inability to tolerate tampons, speculum examinations, or receptive penetrative sex • White or green thick purulent sloughing discharge • Raised vaginal pH > 4.5 • Often scant or absent Lactobacilli on direct microscopy; sometimes increased polymorphonuclear leucocytes (pus); sometimes higher proportions of immature parabasal vaginal squamous epithelial cells and/or mixed aerobic bacteria (features of desquamative vaginitis). • Absence of other elicitable contributing causes – see Differentials below.
Physical appearances on examination may not always correlate with the severity of symptoms. A normal examination does not exclude the diagnosis of testosterone-associated vulvovaginitis and a trial of empiric treatment may be appropriate.
Examination and investigations
Examination is recommended for all patients on first presentation (GPP); this must be tailored to patient acceptability/preference/availability of examination. Ideally, it incorporates: - Skin review (to exclude genital dermatoses including dermatitic disease, lichen planus, lichen sclerosus etc.) Consider adding photographs to patient records for later comparison. - Pelvic exam, including speculum if tolerated, to assess for pain syndromes including vulvodynia, vaginismus, and cervical lesions, and to obtain samples for nucleic acid amplification testing (NAAT) and microscopy. If near-patient direct microscopy is unavailable (eg. in primary care), laboratory samples for microscopy and culture are acceptable. - Vaginal pH testing, if available. - Urine sample to exclude urinary tract infection and assess for pregnancy. - NAAT testing for Chlamydia trachomatis, Neisseria gonorrhoeae, and trichomoniasis if available (if history suggestive of risk). - Opportunistic cervical screening may be offered if due.
We suggest offering patients options to facilitate examination where needed, including extra time during appointments, extra lubrication, self-insertion of the speculum, and using a smaller speculum or vaginally-inserted proctoscope. If pelvic external and/or internal examination is unacceptable to patients, self-taken swabs may be offered as an alternative (GPP).
We suggest that, if other causes of symptoms are excluded or not suspected, and no examination or sampling is acceptable to patients, or if examination/sampling is unavailable in the clinical setting, empiric treatment of testosterone-associated vulvovaginitis with topical estrogens and/or emollients may be offered, and examination/sampling re-offered at a later date (GPP).
Differentials
Symptoms associated with testosterone-associated vulvovaginitis may have multiple alternate underlying causes, thus differentials should be elicited per BASHH guidance and clinical judgement: • Infections of the genital tract, including urinary tract infection, vulvovaginal candidiasis, bacterial vaginosis, Chlamydia trachomatis, Neisseria gonorrhoea, trichomoniasis, pelvic inflammatory disease. • Genital dermatoses, including eczema, psoriasis, lichen planus, lichen sclerosus, vulval intraepithelial neoplasia. • Gynaecological pathologies (particularly if abnormal bleeding and/or pelvic pain are present), including cervical, ovarian or endometrial pathology. • Consideration should be given to psychosocial potentiators of symptoms, particularly around gender dysphoria relating to the genitals, interpersonal relationship stress, or history of sexual abuse.
Management
We recommend a holistic approach to symptom management, including pain management and psychological support where indicated and available (GPP).
We recommend that patients are given information about maintaining vulval dermatological health, including information on emollients and soap substitutes, such as that published by the British Association of Dermatologists. Patients may also find relief from symptoms of sexual discomfort by the use of dermatologist-approved vaginal lubricants, as well as products containing hyaluronic acid. If barrier contraception is not a concern, a ‘double-glide’ lubrication technique, using both an oil-based and water-based lubricant product, may be suggested - further information on this may be found within British Menopause Society guidelines 17 (GPP).
Where a potential infective cause of symptoms is identified or suspected, we recommend treating this as per BASHH Clinical Guidelines (1B).
If infection is excluded, and the history and/or macroscopic and/or microscopic appearances are in keeping with testosterone-associated vulvovaginitis, we recommend as first-line treatment with a topical estrogen of a format of the patient’s choice (pessaries, cream, vaginal ring, gel) – see Figure 1 below (1D). Localised vaginal estrogen treatments, information for patients: adapted from Menopause Support UK.
22
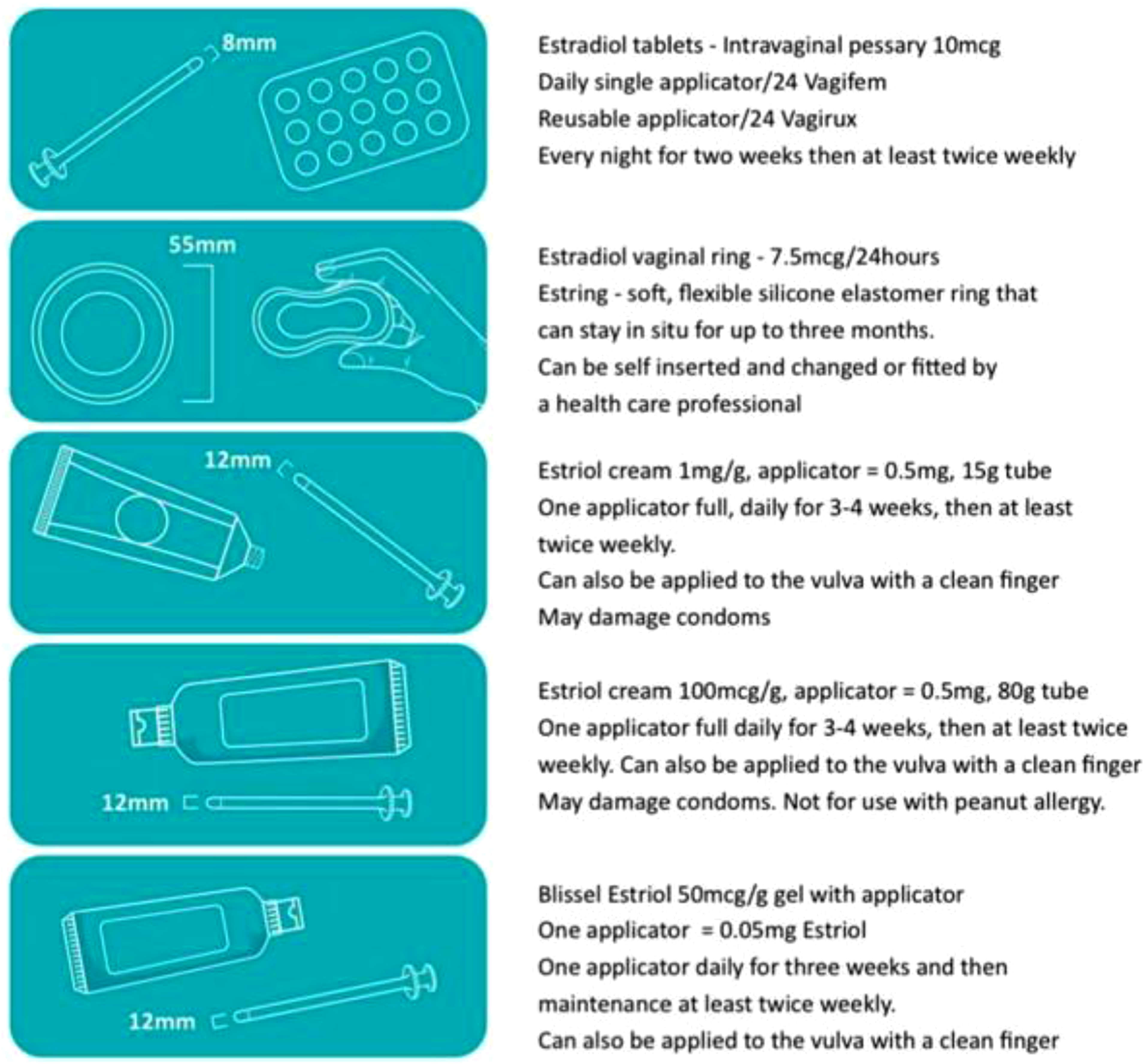
We suggest that higher-strength preparations are offered in preference to lower-strength preparations, as expert experience of this group suggests that this is a more effective strategy (GPP). Please note that currently commercially available gels in the UK are at lower strength than creams.
We recommend that for pessaries and cream/gel formulations, an induction dosing schedule of once nightly for 7–14 nights, then twice weekly maintenance dosing, is followed. For vaginal estrogen rings, the manufacturer’s dispensing and fitting advice should be followed (GPP).
We suggest that, for very severe symptoms of pain, dyspareunia or dysphoria precluding patients’ ability to insert treatments per vaginum, creams should be offered for external use initially, and adding internally-used estrogen once introital atrophy has been treated (GPP). Consideration should be given to the width of applicator supplied with each topical estrogen formulation, as this may affect patients’ ability to adhere to their treatment – see Figure 1 below (GPP). Consideration may also be given to assessment, management and/or onward referral for vaginismus/vulvodynia, using analgesia and dilator therapy techniques.
Some patients with severe testosterone-associated vulvovaginitis symptoms may require an extended induction course of topical estrogens – we suggest nightly for 1 month, then alternate nights for 1 month, then 2–5 doses per week maintenance dosing.
If symptoms do not improve within 3 months of consistent vaginal estrogen use as prescribed, we suggest increasing the dose, changing preparation, or using an additional treatment such as separate vulval and vaginal treatments (GPP).
Consideration of onward referral to related specialities such as pelvic physiotherapy, sexual health, gynaecology, urology or dermatology may be indicated in refractory cases or where underlying differentials are suspected (GPP).
Second-line and alternative regimens
We suggest that in cases of estrogen-based treatment failure, or where microscopy indicates an aerobic inflammatory/desquamative vaginitis (mixed aerobic organisms, higher proportion of immature basal epithelial cells), second-line treatment in the form of a 5–7 days course of nightly topical clindamycin may be offered alongside or instead of topical estrogens (GPP).
We suggest that, if this antimicrobial therapy fails, that compliance is checked, and consideration be given to repeating the course of antimicrobials alongside topical steroids. Prednisolone 5 mg is marketed in the UK as a suppository, and may be used per vaginum for this purpose (GPP).
Dehydroandrosterone (DHEA) pessaries are available in some formularies, and used in the management of cisgender female genitourinary syndrome of menopause where topical estrogens alone have been insufficient. DHEA is mainly converted to androstenedione and androstenediol - both androgens - which are then metabolised onward to various compounds including testosterone and estrogens. This expert group does not have experience of its use in testosterone-associated vulvovaginitis, but hypothesises that it would have limited benefit given its androgenic activity.
Ospemifine is a selective estrogen receptor modulator, acting similarly to an estrogen on the vaginal epithelium to reduce atrophic pain. It is used in the management of cisgender female genitourinary syndrome of menopause, where estrogen-based therapy is medically contraindicated or oral-only non-estrogen therapy is required. This expert group has limited experience of its use in testosterone-associated vulvovaginitis so makes no recommendation.
Targeted laser therapy is offered at some secondary care menopause clinics to cisgender women with genitourinary symptoms of menopause refractory to topical therapies. This expert group has no experience of its use in the transgender population so makes no recommendation.
Counselling of patients on treatment
We recommend that patients are advised the following about management of testosterone-associated vulvovaginitis (GPP): • Testosterone-associated vulvovaginitis can occur at any point during testosterone therapy, but is thought to be more common with several years’ accumulated use.4–6 • All treatments for testosterone-associated vulvovaginitis including topical estrogen preparations are used off-licence. • Systemic absorption of topical estrogens, thus effect on transition/masculinisation, is thought to be minimal, based on studies in menopausal cisgender women.
20
. Drug information packaged with many vaginal hormone preparations gives information relevant to systemic estrogen and side effects/complications, but the evidence base regarding localised treatment finds that topical estrogen is not systemically absorbed, thus patients may be reassured that the information included with the medication does not apply. • Although the amount of topical estrogen absorbed into the body is very small, there may be a small chance of it reactivating a previous hormone-dependent cancer. Patients who have ever had breast cancer, or another hormone-dependent cancer, should be advised to discuss their individual expected benefits and risks with their healthcare provider.21,22 • There is thought to be no increased risk of venous thromboembolism (blood clots) or endometrial hyperplasia (womb lining overgrowth) from topical estrogens.
17
• Topical estrogens are not considered adequate contraceptives, and may damage condoms; alternative methods should be offered if contraception is required.
17
• Although systemic absorption and transference of drug is thought to be minimal, patients are advised as a precaution to avoid penetrative receptive vaginal sex for 1 h after application. • Vaginal estrogen can take up to 3 months of consistent usage to be fully effective; patients are advised to adhere to treatments for at least this amount of time before switching preparations. • If vaginal estrogen is helpful, this can be added to repeat medications and used in the longer term. Vaginal estrogen can be used for as long as testosterone is continued.
Special patient groups – pregnancy, breastfeeding, contraindications
Pre-conception and pregnancy: topical estrogens are not known to be harmful to the developing fetus, however we suggest their use only if benefits outweigh the risks (3D). 23
Clindamycin (when used orally) is not known to be harmful in the second and third trimesters, but has limited data in the first trimester, so manufacturer advises caution.
Breastfeeding/chestfeeding: As the systemic absorption of topical estrogen is thought to be minimal, this group advises that it may be used in chest/breastfeeding.
Clindamycin (when used orally) is present in breastmilk – manufacturer advises use with caution and monitor for infant side-effects (2D).
Medical contraindications
We recommend that, in transmasculine patients with an elevated risk of harm from topical estrogen exposure (for example, active or past history of estrogen receptor-positive cancers) should have a thorough discussion of the likely benefits vs. harms from topical estrogens, plus available alternative strategies (GPP). This can be done in conjunction with a wider trans-specific expert multidisciplinary team, for example the UK Cancer And Transition Service (UCATS). We would recommend the ongoing use of vaginal moisturisers and lubricants in this scenario while awaiting further advice regarding topical estrogens.
There is no trans-specific evidence for contraindications for topical estrogens in those with a history of breast and other hormone-driven cancers. The British Menopause Society consensus statement 17 cite a large cohort study of 50,000 cisgender women with a breast cancer diagnosis, published in 2024, which demonstrated no evidence of an increase in early breast cancer specific mortality associated with the use of vaginal estrogen therapy, though the study did not look at breast cancer recurrence for patients taking an aromatase inhibitor. 22 However a recent observational Danish study 21 did report an increase in breast cancer recurrence rates in women using vaginal estrogen and taking an aromatase inhibitor. Whilst this does not absolutely contraindicate use of vaginal hormonal preparations in this population, the data reinforces the need for collaborative decision making, including the patient’s breast oncology team, if non-hormonal treatments are unsuccessful and vaginal estrogen therapy is being considered.
There is no evidence of increased risk of venous thromboembolism or endometrial hyperplasia from topical vaginal estrogens. Under current UK recommendations, transmasculine and non binary people on testosterone are not advised that they require progestogen-based endometrial protection, nor to have their endometrial thickness measured by ultrasound, unless there is significant ongoing unexplained bleeding or other pelvic symptoms. The use and duration of topical estrogen therapy does not alter this advice. 24
Follow-up
We recommend that clinicians communicate, with consent, with all relevant clinical teams involved in the patient’s care, including primary care, gender identity specialists, etc. (GPP).
We recommend that transmasculine patients are offered long-term maintenance topical estrogen therapy for the duration of their time on testosterone (GPP).
We recommend that patients should be advised to monitor and report any change in symptoms that might represent a concerning alternative pathology, for example growing persistent lumps, unusual changes in bleeding pattern, or changes in vulval skin texture (GPP).
We recommend consideration of onward referral to sexual health, gynaecology, urology or dermatology in refractory cases or where underlying differentials are suspected (GPP).
Auditable outcomes

Recommendations for further research
This group acknowledges the lack of robust trial data for any testosterone-associated vulvovaginitis management strategies, and suggests (ideally) that prospective randomised controlled trials of therapies, or observational cohort studies, are published.
Footnotes
Acknowledgements
The Working Group would like to thank the wider BASHH community including other members of the Gender and Sexual Minorities Special Interest Group; the British Society for the Study of Vulval Disease; the British Menopause Society; the British Association of Dermatologists; the British Association of Gender Identity Specialists; and the charity TransActual, for their editorial contributions. The patient information leaflet [provided separately] was edited for readability to a reading age of 11–12 with the NHS Document Readability tool ![]() .
.
Ethical considerations
Not primary patient research – not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this statement.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Full supporting literature review available on request (submitted for peer review to the International Journal of Transgender Health, accepted and awaiting publication).
Date of next planned review
Five-yearly: April 2031.