
Abstract
Background
Chronic dizziness is a multidimensional condition often influenced by psychological factors. Among these, personality traits such as neuroticism have been linked to heightened symptom perception and disability. However, few studies have systematically examined the relationship between neuroticism, functional burden, and diagnostic characteristics in a population with clinical dizziness.
Objective
To investigate the relationship between perceived dizziness-related handicap and neuroticism as a personality trait among patients referred to a multidisciplinary dizziness and balance clinic.
Methods
This observational study included 247 adult patients with persistent dizziness referred to a specialist clinic. Patients completed the Eysenck Personality Questionnaire (EPQ) and the Dizziness Handicap Inventory (DHI). Clinical data included diagnosis category, duration of symptoms, fall history, comorbidities, and consultation history. Statistical analyses included Spearman correlations, ANOVA, chi-square tests, cluster analysis, and multivariate linear regression.
Results
Neuroticism was significantly correlated with higher DHI scores (ρ = 0.39, p < 0.001) and a greater number of healthcare consultations (ρ = 0.19, p = 0.003). It was not associated with duration of symptoms or fall history. A chi-square test indicated a significant association between the neuroticism category and diagnosis category (χ2 = 32.02, p = 0.043), with higher neuroticism observed in functional and central disorders. Cluster analysis revealed three psychological-clinical subgroups varying in emotional burden, functional disability, and comorbidity profiles. In regression modelling, neuroticism was the only significant predictor of DHI score (p < 0.001), independent of diagnosis or symptom duration.
Conclusion
Personality domains, especially neuroticism, are strong predictors of perceived functional burden in patients with chronic dizziness. These findings underscore the importance of incorporating psychological assessment into the clinical evaluation to further facilitate tailored interventions for the management of dizziness. Personality profiling may help identify high-burden subgroups and guide individualized, multidisciplinary care strategies.
Keywords
Introduction
Dizziness ranks among the most frequent complaints in both primary care and specialist settings and has been associated with significant impairment in quality of life, work productivity, and psychological well-being. 1 Patients may use the term ‘dizziness’ to describe a spectrum of sensations – including vertigo, light-headedness, disequilibrium, or general imbalance – reflecting both peripheral and central vestibular disorders, as well as non-vestibular causes such as cardiovascular, psychiatric, or functional aetiologies. 2 This diversity complicates diagnosis, often leading to extensive investigations, fragmented referrals, and prolonged periods of uncertainty before an accurate clinical interpretation is achieved. 3
An emerging body of evidence suggests that for a subset of patients, particularly those with persistent or medically unexplained dizziness, psychological factors may play a pivotal role in symptom maintenance and perceived disability. 4 Functional vestibular disorders represent an important subgroup within this population. Persistent postural-perceptual dizziness (PPPD), for example, is a well-defined chronic functional vestibular disorder characterized by persistent non-vertiginous dizziness and hypersensitivity to motion and visual stimuli. 5 While PPPD is considered a subtype within the broader category of functional dizziness, the term ‘functional dizziness’ is often used more broadly to describe conditions in which symptoms are not fully explained by structural vestibular pathology but are influenced by central processing and psychological mechanisms. 6 Emotional vulnerability, cognitive misattribution of bodily sensations, and maladaptive coping strategies have been associated with chronic dizziness conditions, including persistent postural-perceptual dizziness (PPPD), functional dizziness, and somatoform vertigo.5,6
The Dizziness Handicap Inventory (DHI) is a widely used, patient-reported outcome measure designed to quantify the impact of dizziness on physical, emotional, and functional aspects of daily life. The DHI has demonstrated strong internal consistency and satisfactory test–retest reliability for both the total score and its subscales. Its validity is supported by findings that higher DHI scores are associated with more frequent dizziness and greater functional impairment. 7 While the DHI captures the emotional consequences of dizziness, it does not assess underlying psychological traits or personality dimensions that may influence symptom perception. Previous studies have shown that high DHI scores often correlate with comorbid anxiety and depression, regardless of vestibular test findings. 8 This suggests that psychological factors may mediate the degree to which dizziness affects patients’ lives, highlighting the need for complementary measures that specifically assess psychological traits.
Personality dimensions, particularly neuroticism, have been shown to influence how individuals interpret, respond to, and manage health-related symptoms. 9 Neuroticism, characterized by heightened emotional reactivity and a tendency toward negative affect, is associated with increased somatic symptom awareness, health anxiety, and poorer outcomes across a range of chronic conditions. 10 Emerging evidence also suggests that personality traits may play a role in chronic dizziness and PPPD, with higher levels of neuroticism linked to increased symptom persistence, distress, and disability.5,11–15 Despite this, much of the existing literature has predominantly focused on state-based measures of anxiety and depression rather than stable personality dimensions.
The Eysenck Personality Questionnaire-Revised (EPQ-R), grounded in a biologically based model of temperament, offers a structured means of assessing personality across three major dimensions: neuroticism, extraversion, and psychoticism. 16 However, relatively few studies have investigated the relationships between personality traits and dizziness -related handicap using both the EPQ and DHI. Existing work combining these measures remains limited, with most studies focusing on psychiatric comorbidity using instruments such as the Hospital Anxiety and Depression Scale (HADS), rather than trait-based personality constructs.17–19
To date, there remains a gap in understanding how stable personality traits interact with perceived disability in patients with dizziness. Addressing this gap may have important clinical implications, as individuals with certain personality profiles may benefit from early psychological screening, targeted counselling strategies, and more integrative rehabilitation approaches.
This study aimed to investigate the relationships between psychological factors (neuroticism), functional impact (dizziness-related handicap), and physical and behavioural aspects (fall history and healthcare consultation behaviour) within a biopsychosocial framework. By exploring the associations between DHI scores, EPQ findings, and clinical characteristics, this study sought to enhance the understanding of psychological contributors to dizziness severity and to support earlier identification of patients at risk for chronicity or functional disability.
Methods
Study design, setting and ethical considerations
This retrospective cross-sectional observation study was conducted at a tertiary multidisciplinary dizziness and balance clinic between January 2021 and March 2024. Ethical approval was obtained from the University’s Institutional Review Board (Protocol no.: HUM/029/1123). As this was a retrospective review of existing clinical data, a waiver of informed consent was granted by the ethics committee. However, all patients attending the clinic routinely provide consent for their anonymised information and related data to be used for research purposes. All procedures were conducted in accordance with the Declaration of Helsinki. The study analysed routinely collected clinical data from adult patients presenting with complaints of dizziness, vertigo, imbalance, or related symptoms. The clinic serves as a regional referral centre for complex vestibular and balance disorders, offering audiological, neurological, and ontological assessments as part of its integrated care model.
Sample
All adult patients (≥18 years) who completed both the DHI and the EPQ as part of their clinical evaluation were eligible for inclusion. A total of 247 patients met the inclusion criteria and their clinical data were included in the analysis.
Measures
Dizziness handicap inventory (DHI)
The DHI is a 25-item self-report instrument designed to quantify the self-perceived impact of dizziness on daily life. It includes three subdomains: physical, emotional, and functional. Scores range from 0 to 100, with higher scores indicating greater perceived handicap. The DHI was scored using the standard format (Yes = 4, Sometimes = 2, No = 0). 7 Although the original instrument does not define standardised severity cut-offs, DHI scores were categorised into four levels, namely normal (0–15), mild (16–34), moderate (35–53), and severe (≥54) to facilitate clinical interpretation. This categorisation is broadly aligned with severity groupings commonly applied in international clinical and rehabilitation settings, although no universally accepted classification system exists. 20 Higher scores indicate greater self-perceived handicap.
Eysenck personality questionnaire revised (EPQ-R)
The EPQ-R short form was administered to assess personality across three dimensions: neuroticism, extraversion, and psychoticism. The neuroticism scale (maximum score = 24) was the primary focus of this study due to its established association with chronic symptom perception and psychological distress in somatic conditions. Scores were categorised into five levels, very low (0–5), mild (6–10), moderate (11–15), high (16–20), and very high (>20) to facilitate clinical interpretation. As the EPQ-R does not provide universally established clinical cut-off values, these categories were defined for the purpose of this study based on score distribution and interpretive guidance from the EPQ-R manual. 21 The EPQ-R is a widely used measure of personality traits with established psychometric properties, demonstrating acceptable internal consistency and test–retest reliability across populations.21,22
Clinical and demographic data
In addition to DHI and EPQ-R scores, data were collected on age, sex, symptom duration, and final clinical diagnosis. Diagnoses were grouped into three categories: peripheral vestibular disorders (e.g. Meniere’s disease, benign paroxysmal positional vertigo, vestibulopathy, otolithic dysfunction, superior canal dehiscence), central vestibular disorders originating from the brain (e.g. Vestibular migraine, Mal de Débarquement Syndrome, white matter changes, degenerative dizziness, neurovascular), non-vestibular or secondary dizziness (e.g. concussion-related dizziness, orthopaedic dysfunction, ocular dysfunction, middle ear pathology), and functional dizziness disorders (e.g. PPPD, somatoform dizziness, psychosomatic presentations, anxiety or panic-related dizziness). Final diagnoses were established as part of routine clinical care within a multidisciplinary dizziness and balance clinic, based on comprehensive clinical assessment and vestibular test findings. Patients were evaluated by an experienced audiologist in collaboration with referring medical specialists, including otorhinolaryngologists (ENTs) and, where relevant, neurologists. Diagnoses were assigned according to the clinical consensus documented in the patient record.
Data analysis
The primary analysis focussed on the relationship between neuroticism and perceived dizziness-related handicap. Secondary exploratory analyses were conducted to examine associations between neuroticism and selected clinical characteristics, including consultation behaviour and fall history, to provide broader clinical context. These included group comparisons, correlation analyses, cluster identification, and regression modelling. Patients with combined central and peripheral diagnoses (n = 2) were excluded from subgroup analyses due to insufficient sample size. Subgroup analyses were therefore limited to diagnostic categories with sufficient sample sizes to ensure meaningful interpretation.
Cluster analysis
To explore potential subgroups within the study sample, a K-means clustering algorithm was applied using standardized variables: DHI score, Eysenck neuroticism score, fall history, memory problems, and anxiety treatment status. Principal Component Analysis (PCA) was used to reduce dimensionality and visualize the clustering results. While K-means clustering was selected for its interpretability and clinical applicability, it is acknowledged that this method is optimally suited for continuous variables. The inclusion of binary variables may limit the appropriateness of Euclidean distance as a similarity measure.
Regression modelling
To identify predictors of perceived functional burden, a multiple linear regression model was constructed using the DHI score as the dependent variable. Predictor variables included neuroticism score, time before diagnosis (in months), anxiety treatment status, and diagnosis category (dummy-coded). All predictors were tested for multicollinearity and regression assumptions, including normality and homoscedasticity.
Descriptive statistics were used to summarise patient characteristics and score distributions. Continuous variables were assessed for normality using visual inspection and appropriate statistical tests. Although minor deviations from normality were observed, the sample size was considered sufficient to support the use of parametric analyses, which are robust to such deviations. Means and standard deviations (SD) were reported for normally distributed data, while medians and interquartile ranges (IQR) were considered for non-normally distributed variables where applicable. Frequencies and percentages were used for categorical variables. Comparisons of DHI scores across diagnostic categories and personality dimensions were conducted using one-way analysis of variance (ANOVA) with post-hoc Bonferroni tests. Associations between neuroticism levels and DHI scores were further explored using Spearman’s rank correlation. The chi-square test was used to examine categorical relationships between diagnosis type and personality classification. Statistical significance was set at p < 0.05. All analyses were performed using Python (v3.11) and Excel.
Results
The final dataset included 247 adult patients with complete DHI and EPQ-R neuroticism scores. The mean age of patients was 52.4 years (SD = 16.8; range 18–85), with 64% being female (n = 158) and 36% (n = 89) being male. The mean DHI score was 35.8 (SD = 18.3), indicating a mild-to-moderate functional burden overall. The mean EPQ-R neuroticism score was 9.4 (SD = 4.7), reflecting mild to moderate levels of emotional reactivity in the sample. Visual inspection of the data indicated no substantial deviations from normality for the main outcome variables, supporting the use of parametric analyses.
Cluster analysis of functional handicap, personality, and comorbidity profiles
To identify latent subgroups within the study sample based on functional burden, neuroticism personality domain, and associated comorbidities, a K-means cluster analysis was conducted using standardized scores for the Dizziness Handicap Inventory (DHI), Eysenck neuroticism scores, and binary indicators for anxiety treatment, fall history, and memory complaints. Anxiety treatment was defined as current pharmacological management for anxiety (i.e., prescribed medication by a general practitioner or psychiatrist), as documented in the medical record. Data on anxiety treatment, fall history, and memory complaints were available for all patients (N = 247). Principal component analysis (PCA) was used for dimensionality reduction and visual inspection of cluster structure. Three distinct patient profiles emerged (selected based on clinical interpretability and inspection of cluster separation): • • •
DHI score by diagnostic category
To explore whether perceived handicap varied across diagnostic categories, patients were classified into four diagnostic groups: peripheral vestibular disorders (n = 110), central vestibular disorders (n = 74), functional dizziness (n = 39), and non-vestibular secondary dizziness (n = 22). Patients with combined central and peripheral diagnoses (n = 2) were excluded from subgroup analysis due to insufficient sample size. The mean DHI scores for each group were as follows: patients with functional dizziness reported the highest perceived handicap (M = 41.3, SD = 18.5), followed by those with non-vestibular secondary dizziness (M = 35.7, SD = 18.9), peripheral vestibular disorders (M = 34.8, SD = 18.0), and central vestibular disorders (M = 34.5, SD = 18.5). However, a one-way analysis of variance (ANOVA) revealed that these differences were not statistically significant, F (3, 241) = 1.10, p = 0.357, η2p = 0.014, indicating a small effect size and suggesting that functional impact as measured by the DHI was relatively consistent across diagnostic categories (Figure 1). Mean DHI score by diagnostic category.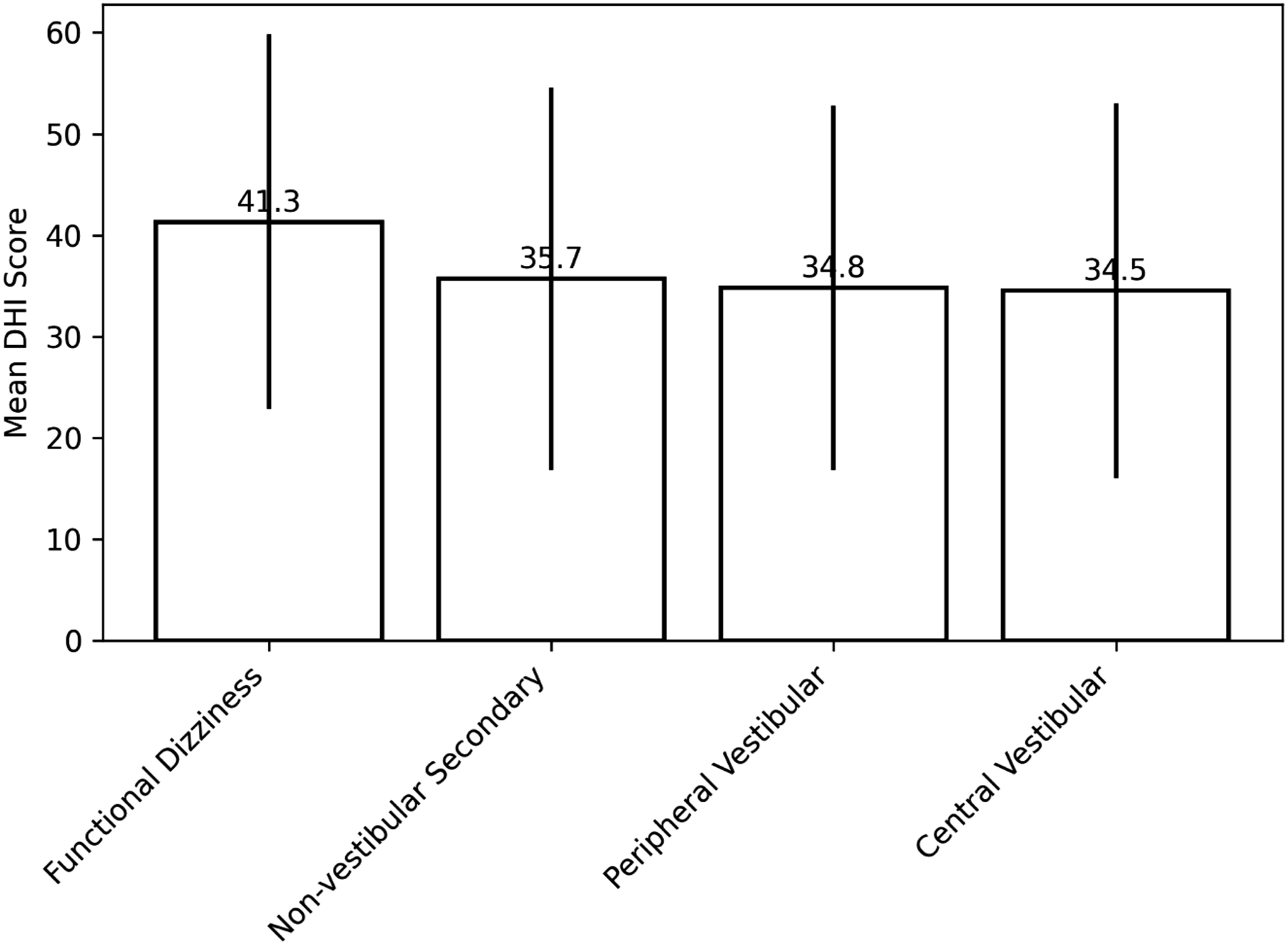
Distribution of neuroticism across diagnostic category (chi-square analysis)
This analysis examines whether neuroticism differs across diagnostic categories (i.e., distribution of personality traits across clinical conditions). A chi-square test of independence was performed to assess whether neuroticism levels differed across diagnostic categories. Neuroticism was categorized into five levels based on Eysenck scores (very low, mild, moderate, high, very high), and diagnosis was grouped into four categories: peripheral vestibular disorders, central vestibular disorders, functional dizziness, and non-vestibular secondary dizziness. Patients with combined diagnoses (n = 2) were excluded from this analysis. The analysis revealed a statistically significant association between neuroticism and diagnosis category, χ2 (12, N = 245) = 32.02, p = 0.043. Inspection of the distribution indicated that patients with functional dizziness demonstrated a higher proportion of moderate-to-high neuroticism, whereas peripheral and non-vestibular groups were more frequently represented in the mild neuroticism category. Central vestibular disorders showed a more heterogeneous distribution across neuroticism levels (Figure 2). Notably, very high neuroticism scores were relatively infrequent across all diagnostic groups. Distribution of neuroticism levels across diagnosis categories (% within diagnosis).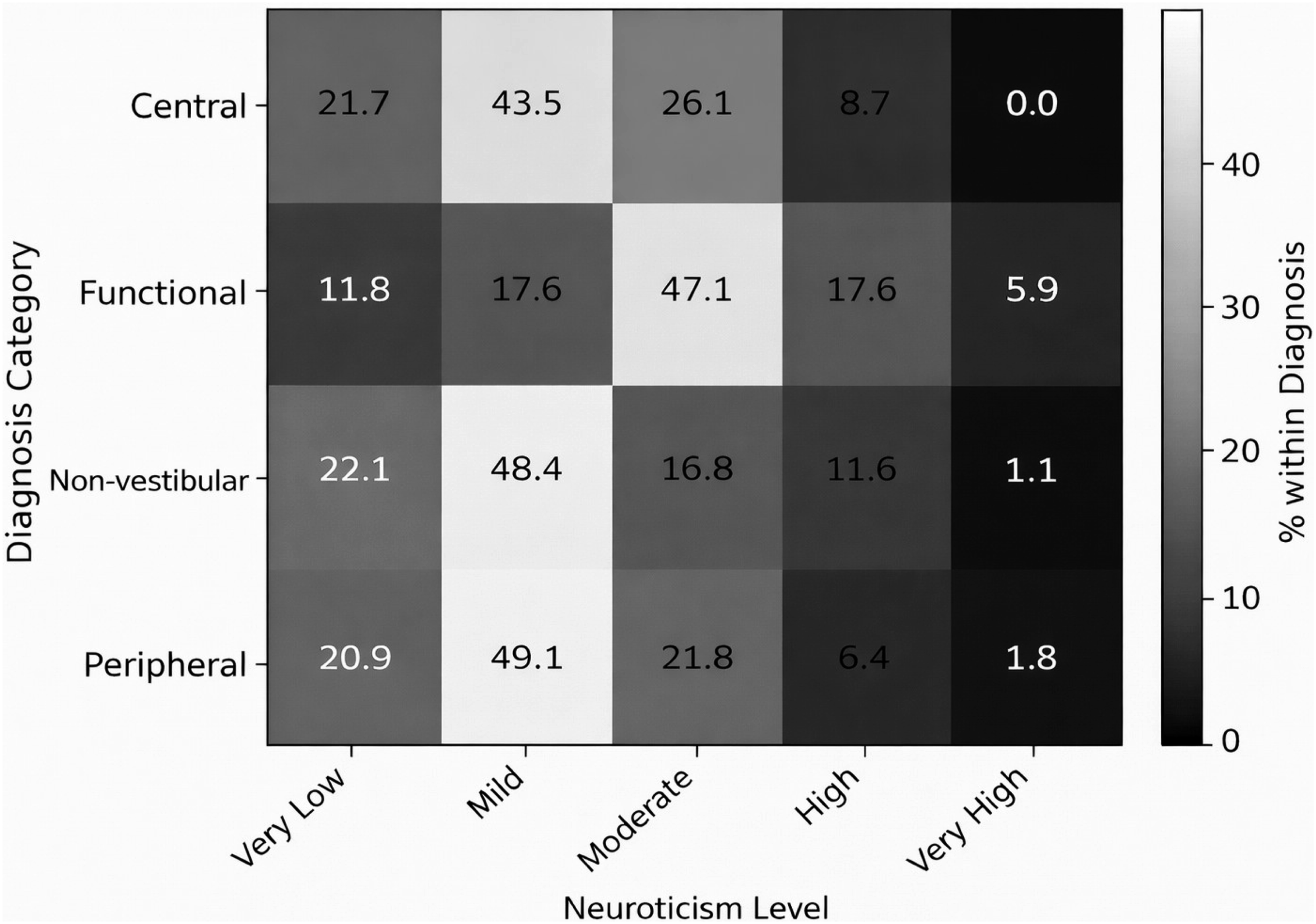
Differences in functional handicap across neuroticism levels (ANOVA)
The previous analysis examined how neuroticism is distributed across diagnostic categories, whereas this analysis evaluated whether neuroticism is associated with differences in perceived functional disability, independent of diagnostic classification. To examine this, patients were grouped into five neuroticism categories based on their Eysenck scores: very low (n = 50), mild (n = 115), moderate (n = 55), high (n = 23), and very high (n = 3). Mean DHI scores increased with neuroticism level, with patients in the high neuroticism group reporting the highest handicap (M = 48.3, SD = 20.1), followed by those with moderate (M = 42.7, SD = 18.7), mild (M = 35.1, SD = 15.8), and very low (M = 23.9, SD = 16.2) neuroticism. The very high neuroticism group had a mean DHI score of 33.0 (SD = 17.1), although this group comprised a small sample (n = 3), limiting meaningful interpretation (Figure 3). A one-way ANOVA revealed a statistically significant difference in DHI scores across neuroticism categories, F (4, 241) = 9.28, p < 0.001, η2p = 0.134, indicating a moderate-to-large effect size. This suggests that neuroticism accounts for a meaningful proportion of variance in perceived dizziness-related handicap. Post hoc comparisons (Bonferroni-adjusted) indicated that patients with moderate neuroticism had significantly higher DHI scores than those with very low neuroticism (MD = 18.8, p < 0.001, Cohen’s d = 1.05), and patients with high neuroticism also differed significantly from the very low group (MD = 24.4, p < 0.001, Cohen’s d = 1.35). Differences between adjacent categories (e.g., mild vs moderate) were smaller and did not consistently reach statistical significance. A Spearman’s rank-order correlation revealed a moderate positive relationship between DHI scores and Eysenck neuroticism scores: ρ = 0.396, p < 0.001. Mean DHI score by neuroticism category.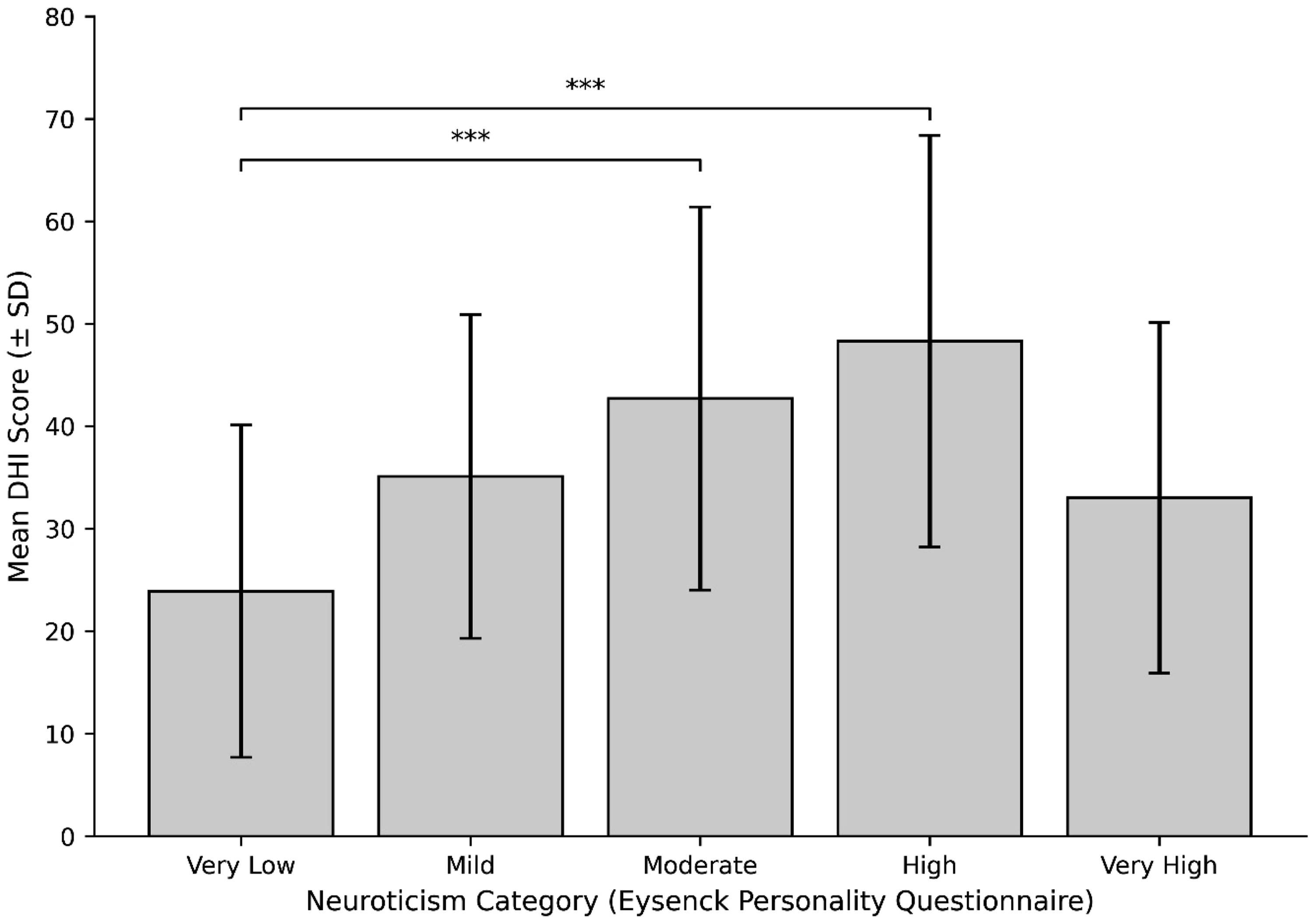
Relationship between dizziness impact and symptom duration
A Spearman’s rank-order correlation was conducted to evaluate the relationship between the duration of dizziness symptoms prior to diagnosis and the degree of perceived functional handicap, as measured by the Dizziness Handicap Inventory (DHI) (Figure 4). The analysis revealed a weak, non-significant correlation (ρ = 0.090, p = 0.16), indicating that longer symptom duration was not associated with higher reported functional burden in this sample. Relationship between symptom duration and DHI score.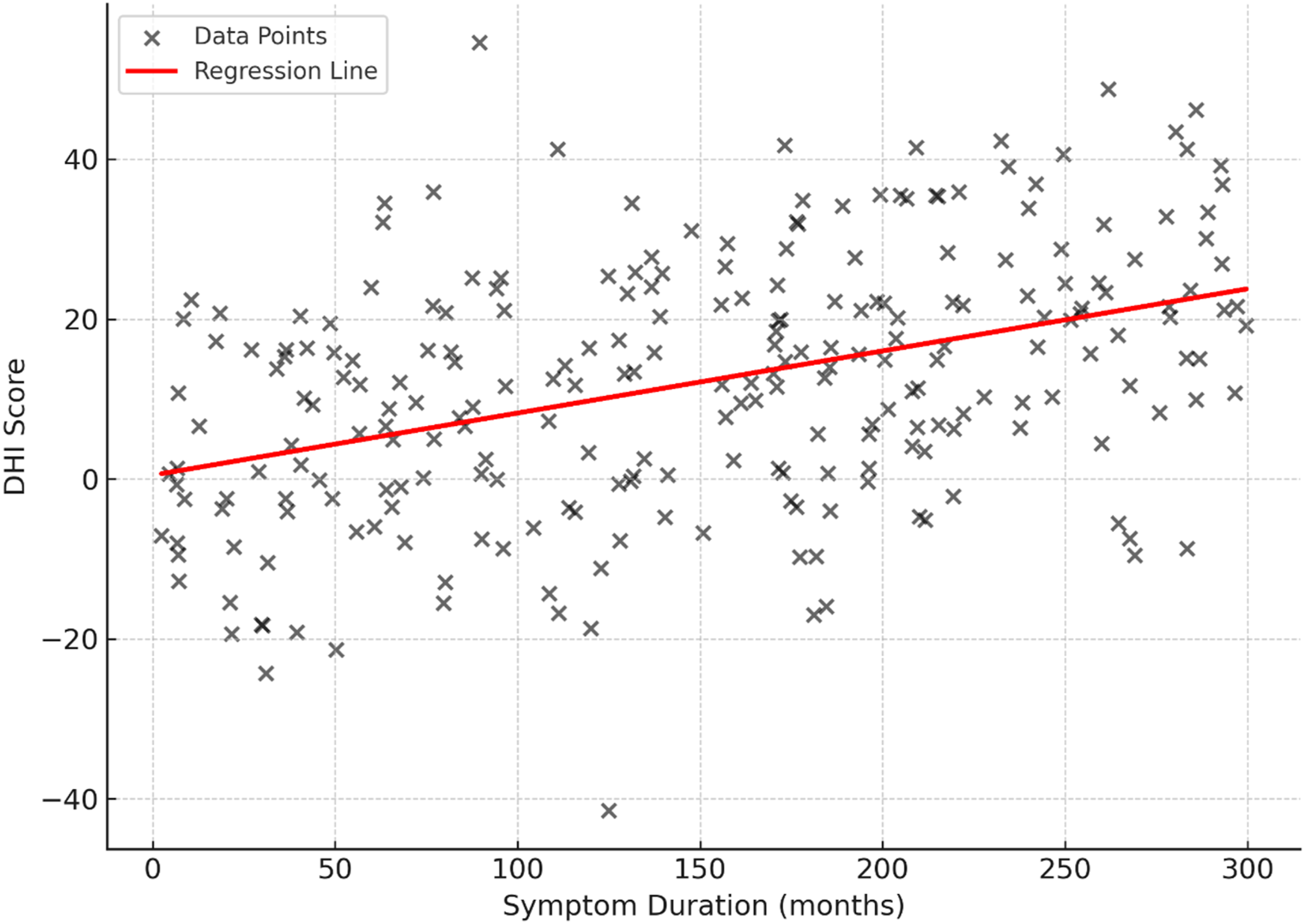
Neuroticism and healthcare consultation behaviour
A Spearman’s rank-order correlation was performed to examine the association between neuroticism and the number of healthcare professionals consulted prior to diagnosis. The total number of consultations was calculated by summing affirmative responses across nine professional categories, including general practitioners, ENTs, neurologists, psychologists, physiotherapists, and others. The analysis revealed a statistically significant positive correlation (ρ = 0.190, p = 0.003), suggesting that individuals with higher levels of emotional reactivity were more likely to consult multiple providers. This pattern may reflect underlying diagnostic uncertainty, heightened health-related anxiety, or reduced satisfaction with prior evaluations among patients scoring higher on the Eysenck neuroticism scale (Figure 5). Neuroticism versus number of healthcare consultations.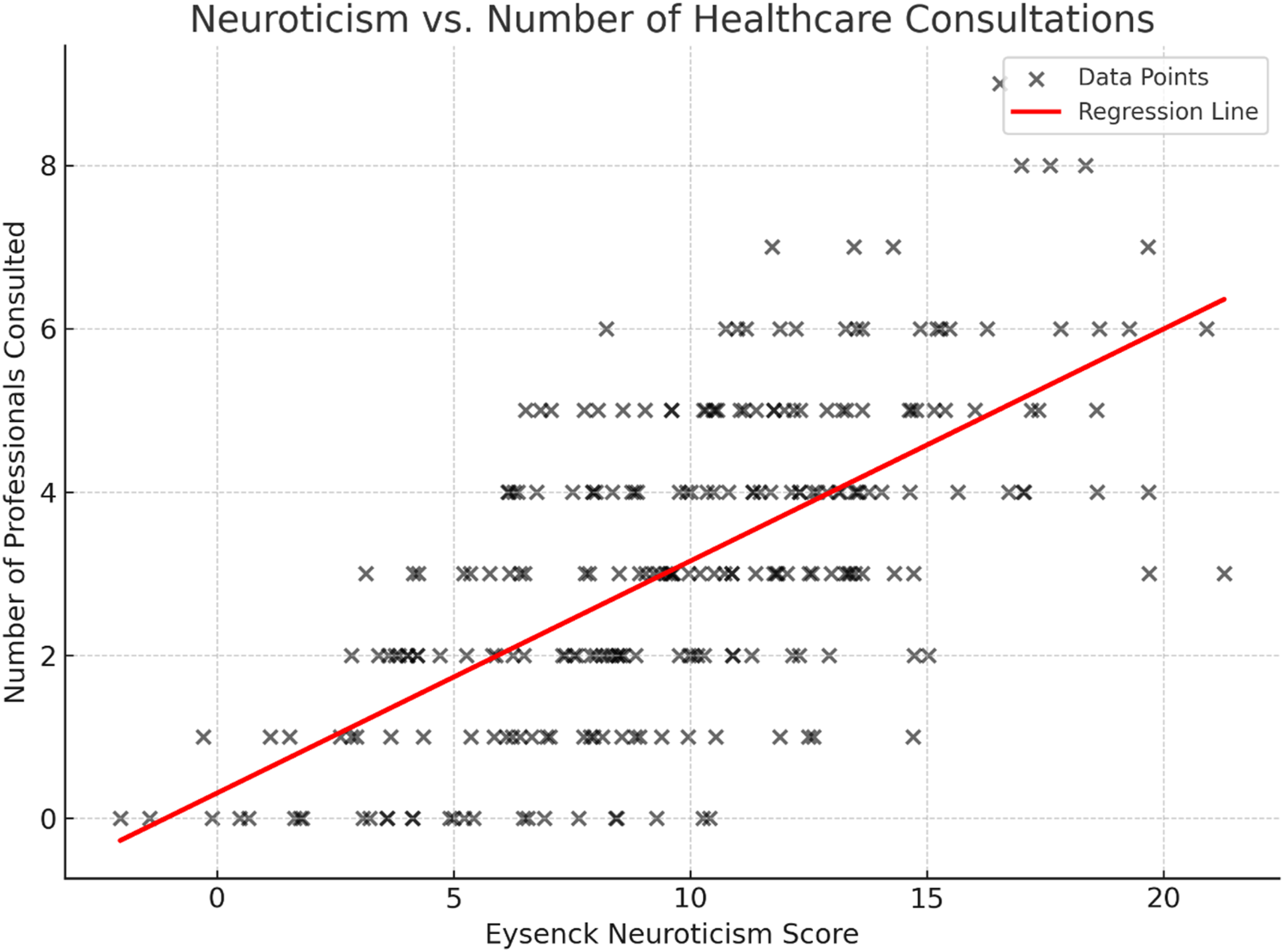
Neuroticism and fall history
A point-biserial correlation was conducted to examine the association between emotional reactivity and history of falling. Eysenck neuroticism scores were correlated with patients’ binary responses indicating whether they had experienced a fall. The analysis revealed no statistically significant relationship (rpb = −0.040, p = 0.53), suggesting that neuroticism was not associated with a higher likelihood of reported falls in this sample. While neuroticism may influence the subjective experience of dizziness and perceived handicap, these findings indicate that it does not directly relate to fall occurrence (Figure 6). Neuroticism score by fall history.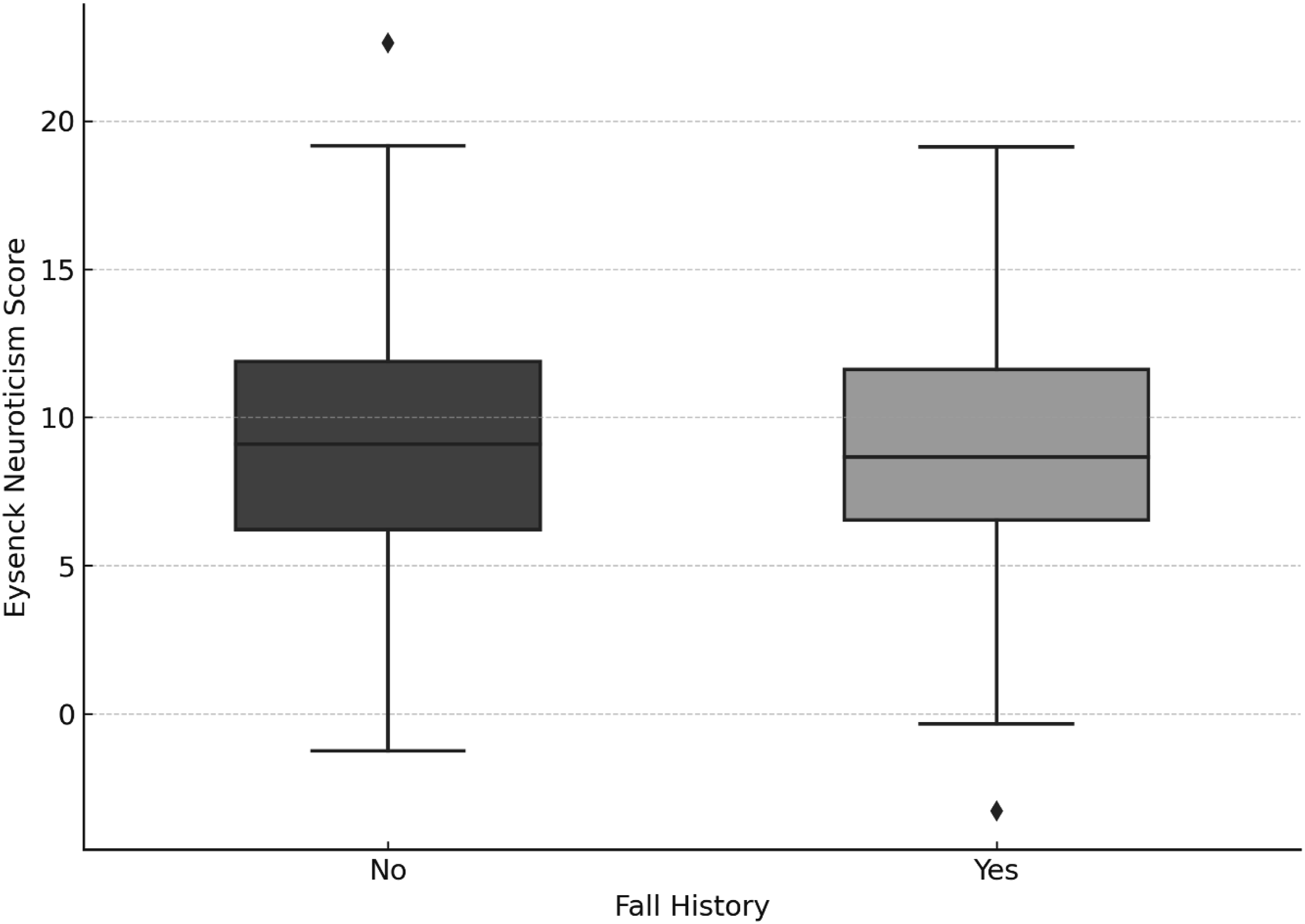
Predicting functional handicap from personality and clinical characteristics
A multiple linear regression analysis was performed to investigate whether emotional reactivity, diagnostic classification, symptom duration, and anxiety treatment status predicted dizziness-related functional handicap, as measured by the Dizziness Handicap Inventory (DHI). The overall model was statistically significant, F (7, 239) = 5.55, p < 0.001, accounting for approximately 14% of the variance in DHI scores (R 2 = 0.140).
Among all predictors, only the Eysenck neuroticism score was a statistically significant contributor to the model (β = 1.40, p < 0.001). This indicates that for every one-point increase in neuroticism, the DHI score increased by an estimated 1.4 points, suggesting a robust relationship between emotional reactivity and perceived functional burden. In contrast, symptom duration (p = 0.263), anxiety treatment status (p = 0.593), and diagnostic category (all p > 0.05) were not significant predictors of functional impairment in this model (Figure 7). Predictors of DHI scores: Linear regression coefficients.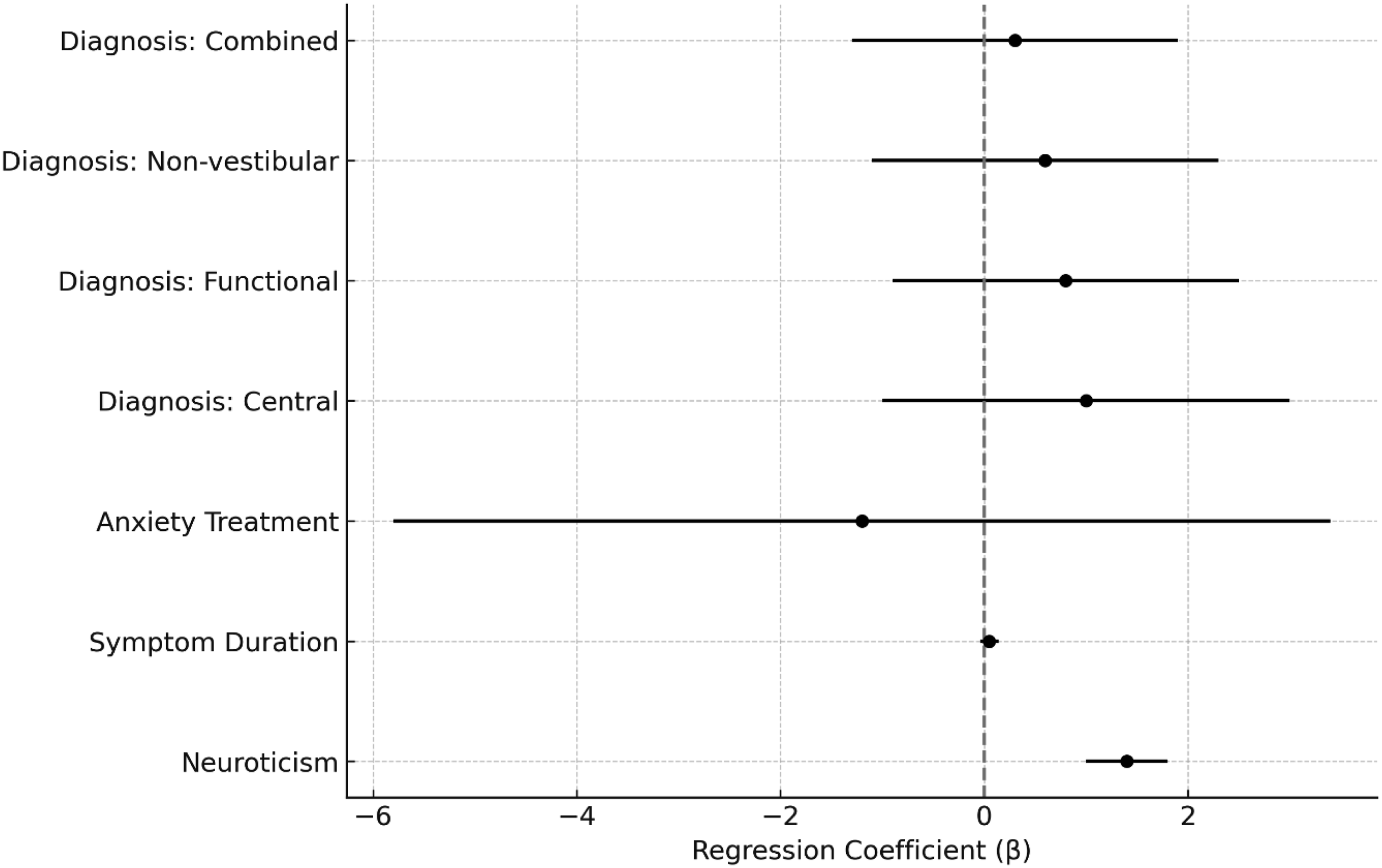
Discussion
Findings from the current study identified three clinically meaningful patient subgroups. One group, characterized by high DHI and neuroticism scores, frequently reported comorbid memory problems and anxiety treatment but had a relatively low fall history. This may reflect a subgroup experiencing high psychosomatic distress with limited objective imbalance. Conversely, another cluster with moderate DHI and low neuroticism showed a 100% fall history and frequent memory complaints, possibly indicative of physiologically driven impairment. The third, low-burden cluster reported few comorbidities and had the lowest DHI and neuroticism scores. These findings emphasize the clinical utility of multidimensional assessments in dizziness, supporting a biopsychosocial model of care. 23
Neuroticism was found to be a significant predictor of dizziness-related handicap, with meaningful association between neuroticism and DHI scores. This aligns with previous research indicating that psychological factors, particularly trait anxiety and emotional instability, play a substantial role in modulating dizziness perception and disability.14,24 This association suggests that individuals with higher neuroticism may experience increased emotional distress in response to somatic symptoms, potentially amplifying their perceived impairment even when objective vestibular findings are mild or absent.
Regression analyses confirmed that neuroticism significantly predicted DHI scores, whereas diagnostic category, symptom duration, and anxiety treatment were not significant predictors. However, the explained variance was modest (R2 = 0.140), indicating that neuroticism accounts for approximately 14% of the variability in dizziness-related handicap. Hence, although emotional reactivity is a significant contributor, the majority of variance in DHI scores remains unexplained by the variables included in the analysis. These findings suggest that additional factors, such as vestibular impairment severity, visual dependence, cognitive load, coping strategies, illness perceptions, and environmental or contextual influences, likely contribute to dizziness-related disability. Similar findings have been noted in previous literature demonstrating that chronic dizziness is influenced by a complex interaction of vestibular, psychological, and behavioural factors rather than a single determinant.5,10,14 Taken together, these findings reinforce that dizziness-related disability is multifactorial and cannot be attributed to a single psychological construct alone, supporting a biopsychosocial framework for assessment and management.
The significant association between neuroticism and diagnostic category observed in this study highlights the complex interplay between psychological traits and vestibular symptom presentation. In particular, patients with functional dizziness demonstrated a higher proportion of moderate-to-high neuroticism levels compared to other diagnostic groups. This is consistent with the conceptualization of functional vestibular disorders, including PPPD, as conditions in which persistent symptoms are shaped not only by vestibular mechanisms but also by maladaptive postural control, heightened threat appraisal, and altered sensory processing. 5
In contrast, patients with peripheral and non-vestibular conditions were more frequently represented within the mild neuroticism category, suggesting a comparatively lower contribution of enduring psychological traits to symptom perception in these groups. Patients with central vestibular disorders showed a more heterogeneous distribution across neuroticism levels, which may reflect variability in clinical presentation and individual psychological responses to neurological dysfunction. This interpretation is supported by evidence showing that psychiatric comorbidity differs across organic vertigo syndromes rather than occurring uniformly across diagnoses, and that persistent dizziness after vestibular disorders is associated with psychological strain as well as vestibular factors. 11 One possible explanation for this heterogeneity in central vestibular disorders is the variability in lesion location, symptom unpredictability, and the involvement of neural systems linked to emotional regulation and sensory integration. Although this remains speculative in the present study, the broader dizziness literature supports the view that psychosocial factors such as stress, depression, and related emotional processes are meaningfully associated with chronic dizziness. 13
Importantly, while higher neuroticism was more prevalent in functional presentations, very high neuroticism scores were relatively uncommon across all diagnostic categories. This suggests that, although emotional reactivity contributes meaningfully to perceived disability, extreme personality profiles are not characteristic of the broader dizziness population. These findings support a biopsychosocial framework in which stable psychological traits interact with vestibular and neurological factors to influence symptom severity and functional impact. 5
Fall history and duration of symptoms were not significantly associated with neuroticism, nor did symptom duration predict DHI scores. The lack of association between symptom duration and perceived handicap may reflect adaptation over time or variability in individual coping mechanisms. This finding is consistent with some previous reports suggesting that chronicity alone does not necessarily predict perceived disability, although it contrasts with other studies that have demonstrated increasing handicap with prolonged symptom duration.25,26 This discrepancy may reflect differences in patient populations, measurement approaches, or the influence of moderating psychological variables such as coping style and resilience. Notably, there was a relationship between fall history and DHI scores, suggesting that physical factors contribute to perceived disability, although this relationship appears to be modulated by psychological variables.
Overall, these findings highlight the importance of integrating psychological screening, especially for trait neuroticism, into the assessment of patients with dizziness. The results support targeting emotional processing and maladaptive coping styles in management strategies, particularly for patients with functional or centrally mediated dizziness. The limited predictive value of diagnosis category and symptom duration further underscores that psychological factors may, in some cases, supersede structural findings in determining patient outcomes. Although not central to the primary research question, exploratory analyses examining consultation behaviour and fall history were included to contextualize how personality traits may influence healthcare utilisation and symptom interpretation. These analyses should be interpreted cautiously, as hypothesis-generating rather than confirmatory findings.
Our study contributes to the growing evidence base advocating for multidisciplinary, person-centred approaches in vestibular rehabilitation. 27 The integration of psychological constructs such as neuroticism into clinical dizziness research is not only timely but necessary. Current study findings align with a growing body of literature that suggests chronic dizziness cannot be comprehensively managed using only biomedical models.4,28,29 Patients with similar objective vestibular test outcomes may report markedly different levels of disability due to variations in emotional and cognitive responses. This is particularly evident in individuals with high neuroticism, who may demonstrate increased vigilance toward bodily sensations, health-related anxiety, and catastrophizing – all of which are known to influence symptom perception and distress. Given the cross-sectional design, these findings should not be interpreted as indicating that neuroticism causes increased dizziness-related disability, but rather that these variables are significantly associated.
Implications
Current study findings offer several clinically relevant implications. Firstly, neuroticism – an easily assessed trait using short personality inventories – may serve as a useful screening tool for identifying patients at risk of elevated subjective burden. Secondly, there is growing evidence supporting the use of cognitive-behavioural therapy (CBT), and anxiety-focused interventions in patients with chronic dizziness, particularly in functional and persistent dizziness conditions, where such approaches have been shown to reduce symptom severity, improve coping, and enhance quality of life.5,30,31 Incorporating these interventions alongside vestibular rehabilitation may therefore provide more comprehensive and effective care. Thirdly, the identification of psychologically vulnerable subgroups using tools like cluster analysis provides a foundation for personalised and targeted treatment pathways.
Limitations
This study has several limitations that should be considered. Firstly, the cross-sectional design precludes any conclusions regarding causal relationships between neuroticism and dizziness-related handicap. While higher neuroticism was associated with increased perceived disability, the direction of this relationship remains unclear. It is plausible that neuroticism represents a predisposing vulnerability; however, it is equally possible that persistent or severe dizziness contributes to increased emotional distress and elevated neuroticism scores over time. Secondly, the relatively small sample sizes within certain diagnostic subgroups may have limited statistical power to detect more subtle between-group differences. Thirdly, in more recent literature, different cut-off values have been used for the DHI, with a cut-off of 30 being frequently applied.31–35 Findings from this study and other literature need to be viewed in light of these differences due to the absence of a universally accepted classification system. Fourthly, the regression model accounted for only a modest proportion of the variance in DHI scores, suggesting that additional factors – such as vestibular impairment severity, visual dependence, coping strategies, and contextual influences were not captured in the current study. Furthermore, the use of K-means clustering with mixed variable types represents a methodological limitation, as Euclidean distance may not optimally capture similarity when binary variables are included. Alternative approaches, such as Gower distance-based clustering or k-prototypes, may provide more robust modelling of mixed data. As such, the identified clusters should be interpreted as exploratory and hypothesis-generating rather than definitive classifications. Finally, the reliance on self-report measures may introduce response bias, particularly in the assessment of psychological constructs and perceived functional burden. Future research should employ longitudinal designs and incorporate a broader range of clinical and psychosocial variables to better elucidate the complex and potentially bidirectional interactions underlying dizziness-related disability.
Conclusion
This study contributes to the understanding of how personality domains, specifically neuroticism, interact with dizziness-related handicap and clinical features in chronic dizziness. Findings underscore the need to incorporate personality profiling and psychosocial support into the diagnostic and management framework for patients with chronic dizziness. Future research should investigate whether interventions targeting emotional regulation and maladaptive illness beliefs can reduce symptom persistence and improve quality of life in this population.
Footnotes
Acknowledgements
The authors would like to acknowledge the patients who provided consent for their records to be used for research.
Ethical considerations
Ethical approval was obtained from the University’s Institutional Review Board (Protocol no.: HUM/029/1123).
Consent to participate
Patients whose records were used for this study provided informed consent for the anonymised use of their data for research at the time of their consultation.
Author contributions
AN collected and analysed the data and wrote the first draft. AK critically reviewed the first draft and made necessary revisions. AN & AK collectively contributed to subsequent drafts, revisions, and the final write-up of the paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available within the article.