
Abstract
The diagnosis of autism spectrum condition (ASC) in women is increasing, prompting research into the gendered experience and presentation of female ASC. To complement this growing body of research, the current study utilised a qualitative approach informed by a feminist disability framework to explore how the intersecting dimensions of difference, gender, and ASC influence autistic women’s subjectivity and wellbeing. Drawing on the experiences of eight late-diagnosed autistic women, thematic analysis highlighted experiences of early marginalisation, challenges of living outside gendered social norms, the psychological and emotional consequences of masking, and the impact of diagnosis on subjectivity, identity, and wellbeing. Participants developed their authenticity and personhood within a performative social context that required masking of the self, a complex process with wide-ranging consequences. Findings also highlight the importance of acceptance, representation, and community for the wellbeing of autistic women. This research challenges the dominant, masculinised construction of ASC. It highlights the need for the ontological status of ASC to be reconceptualised to incorporate diverse experiences of the condition across the gender spectrum. Future research should explore how psychology can facilitate this reconceptualisation.
Autism spectrum condition (ASC) is defined and diagnosed through the presence of behaviours related to communication and repetitive and restrictive actions (APA, 2013). While ASC affects both sexes, girls and women are more likely to be diagnosed later in life (Gould & Ashton-Smith, 2011; Zener, 2019). Reasons for this gender discrepancy in early diagnosis include lack of recognition of ASC traits in girls due to the historical male-focus of research. Androcentric research findings have influenced the development of the ASC construct, diagnostic tools, and the preconceptions of health professionals, including psychologists, who report unfamiliarity with female ASC presentations and are dismissive of women who present with ASC traits (Bargiela et al., 2016; Zener, 2019). For women, the timing of diagnosis may have significant consequences. Autistic girls who do not meet the conventional construction of ASC are frequently ostracised, denied support, and labelled with other diagnoses such as learning disorders, personality disorders, depression, anxiety, and eating disorders (Cridland et al., 2014; Loomes et al., 2017).
Psychology has been complicit in this exclusionary framework by maintaining an apolitical stance towards gendered diagnostic practices despite evidence women are systematically disadvantaged, stereotyped, and pathologised by “scientific practices” within psychology (Marecek & Gavey, 2013). Current “gold standard” diagnostic tools for ASC include the ADOS-2 (Autism Diagnostic Observation Schedule, Second Edition) and ADI-R (Autism Diagnostic Interview-Revised), both of which are normed upon a predominantly male sample population (Ratto et al., 2017; Zener, 2019), reinforcing the exclusion of women from ASC diagnosis by discounting or undervaluing traits more typically observed in autistic women (Head et al., 2014; Kreiser & White, 2014).
Furthermore, gatekeepers such as parents and teachers employ different gendered expectations for girls, adding a layer of complexity when identifying ASC traits (Cheslack-Postava & Jordan-Young, 2012; Cook et al., 2017). Autistic girls report being chastised for misunderstanding social rules, committing social faux pas, or being outspoken. This negative response reinforces their need or desire to mask (Bargiela et al., 2016; Seers & Hogg, 2021). Other, more gender-conforming ASC traits such as shyness or restricted interests in books or animals are commonly overlooked by teachers and parents (Dean et al., 2017; Ratto et al., 2017).
When autistic girls believe they are to blame for their “difficult” or “abnormal” behaviours, their self-worth and efficacy are likely to be reduced and such beliefs may result in mental health issues (Bargiela et al., 2016; Cridland et al., 2014). Without appropriate diagnosis and self-understanding, experiences of relationships can be complex, confusing, and potentially abusive (Baldwin & Costley, 2015; Cridland et al., 2014).
To reduce their vulnerability and to cope with everyday life, some autistic girls develop compensatory strategies commonly referred to as “masking” or “camouflaging” (Dean et al., 2017; Gould, 2017; Hull et al., 2017; Lai & Baron-Cohen, 2015). Masking may involve social imitation and adaption, and a subconscious mimicking of social behaviour (Lai et al., 2017), where a persona is adopted to appear “neurotypical” (Bargiela et al., 2016). Masking appears to be more prevalent among autistic women than autistic men, suggesting the performance of femininity is more scrutinised and policed (McQuaid et al., 2021). Bargiela et al. (2016) demonstrated that autistic women experience pressure to play certain traditional and expected feminine roles such as wife, mother, or girlfriend, despite this being incompatible with how they wished to live. Milner et al. (2019) found autistic women feel more pressure to mask in social situations and are often more successful at doing so than autistic men.
For autistic girls and young women, the social monitoring and policing of gendered behaviour through dominant social norms, relational bullying, and shaming is a strong motivator to maintain the appearance of “normal”. However, these protective behaviours are a cause of delayed diagnosis. Autistic girls and young women are often disregarded for ASC assessment as they display some level of neuro-normative social competence (Bargiela, 2015; McQuaid et al., 2021; Zener, 2019). They may also be denied access to support due to their unconscious and conscious masking behaviours (Bargiela et al., 2016).
Autistic women describe camouflaging their autistic traits to improve employment opportunities or social connections and to avoid verbal and emotional abuse (Hull et al., 2017). However, autistic women report losing their authentic self and betraying the autistic community when masking (Bagatell, 2007; Hull et al., 2017), signifying that masking comes at a psychological cost. Masking is similar to the practice of “passing”, which has been conceptualised as the act of adopting or performing in line with normative identity roles (Kanuha, 1999) and, like masking, usually occurs within a context of social oppression.
The experience of masking ASC traits may create deep internal conflict that warrants careful consideration and exploration, particularly given the lack of clinical knowledge surrounding such experiences. While masking may uphold assumptions of neuro-normativity, concealment may occur at some cost, particularly to the psychological functioning of autistic women, in terms of both social isolation and wellbeing.
In the current study, we sought to understand the impact of cultural norms on women's construction of the self within the context of an ASC diagnosis and to gain insight into the strategies that autistic women use to navigate societal standards and develop connections with others. We consider how these strategies impact the mental wellbeing of late-diagnosed autistic women.
Methodology
Our qualitative study draws upon feminist disability theory and the social model of disability. Feminist disability theory acknowledges the similarities between the constructs of woman and disability as “other” and the intersections of gender and disability (Garland-Thomson, 2002). These critical methodologies allowed for reflection on the dominant cultural narratives of gender and the meanings imposed upon female behaviour that does not conform with gendered expectations. However, tensions exist between the apolitical stance psychology attempts to inhabit as a discipline and the explicitly political lens of feminism. These tensions shaped this research and presented challenges for us as researchers in navigating a research process primarily established around traditional frameworks of knowledge creation, which can further silence women whose experiences of autism sit outside of the heteronormative, patriarchal centre of psychology.
Deploying qualitative feminist research methods allowed us to centre the voices of autistic women (Willig, 2013), and acknowledge the intersections between power structures within psychology and societal constructions of “dysfunction” and gender. Feminist research challenges normative, hegemonic assumptions with a gendered lens and considers the perspectives of diverse groups previously rendered invisible (Bailey, 2011).
In line with a social model of disability, we do not deny biogenic causes of ASC, but also focus on the role played by societal morals and cultural norms in shaping the manifestation and experience of difference. In the context of this study, the social model of disability is used alongside feminist disability theory, which offers a means of critiquing how the medical model creates knowledge that influences dominant perceptions and experiences of ASC.
Methods
Following ethics approval from the Charles Sturt University Human Research Ethics Committee, a purposive sampling technique was employed to recruit a relatively homogenous sample. The call for participants specified that women should be aged 18 and over, residing in Australia, and have a formal diagnosis of ASC or Asperger's Syndrome. Recruitment processes were guided by sensitivity to communication and sensory needs and participants were allowed to select the interview's location and format (i.e., face-to-face online interviews or written responses) (Haas et al., 2016). No incentives were offered for participation. After written consent was obtained, a single semi-structured interview was conducted with each participant. Open-ended questions allowed participants freedom to discuss issues they felt essential to the topic. Interviews were anonymised and transcribed verbatim.
Data were analysed using reflexive thematic analysis (TA) (Braun & Clarke, 2021) informed by critical feminist theory. Our analysis attempted to honour participants’ lived experiences; however, epistemological integrity requires critical reflection, not just on the participants’ accounts, but also on researchers’ interpretations of these. It was in this subjective but conscious, critical space that the themes were created.
We familiarised ourselves with the interview data through multiple readings and transcripts were coded for similarities and differences of experiences. Through an iterative process, codes were described, refined, amalgamated, and connected to feminist theoretical frameworks. The codes were grouped, and themes were constructed that addressed the intersections of gender and ASC. Consistent with feminist research practices, power dynamics and the politics of representation were considered throughout the coding phases and analysis (Bailey, 2011). We invited participants to review their interview transcripts and provide feedback to ensure accuracy.
Participants
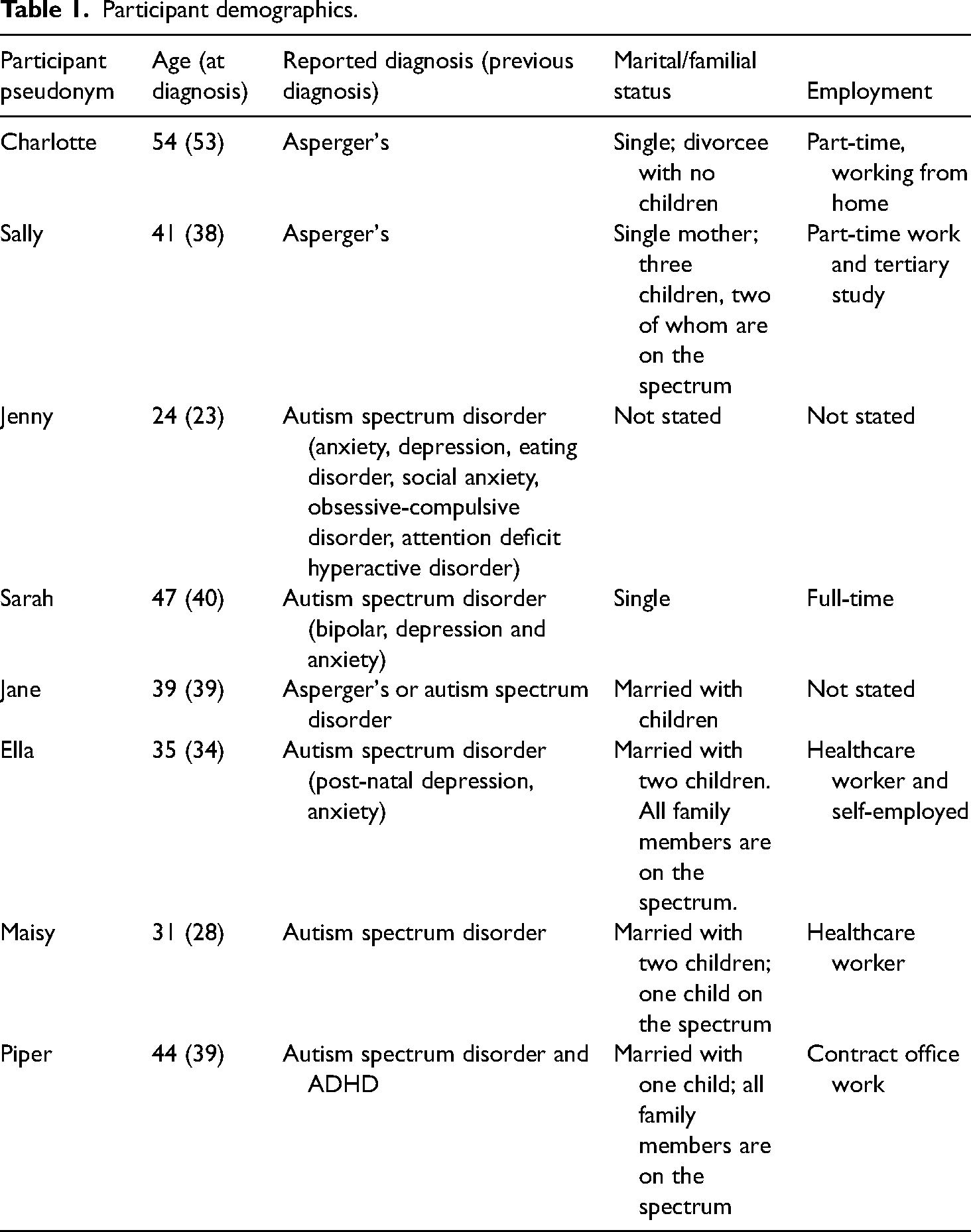
Participants reported a formal diagnosis of Asperger's Syndrome or ASC, with the average age at diagnosis of 36.75 years. Ages ranged from 24 years to 53 years (
Participant demographics.
Findings and discussion
This paper presents two core themes representing participants’ experiences of the intersection between social norms and marginalisation, managing the authentic self, and the importance of diagnosis and connection. Core to this was the notion of internalised blame for difference and the need to develop coping mechanisms to manage the social consequences of difference. This self-blame was released once a diagnosis was obtained and participants connected with other autistic women, thereby taking an active role in their identity development.
Theme 1: “Managing and masking the self”
This theme encompasses participants’ attempts to perform social norms and reduce visibility within the (neurotypical) community; the physical and psychological consequences of this performance, and the coping strategies participants used to manage these consequences. To understand an individual's use of masking, it is vital to consider the sanctioning of cultural norms as a critical motivating force for concealment. Ella positioned her masking as a choice contingent on social survival: I knew that I was different, I knew that I wasn’t like other people, and I sort of tried to blend in as much as was humanely possible. Society's not kind. If I had of stood out, then maybe I would have been bullied.
The consequences of being made visible are foregrounded here. Ella's self-construction implies a level of control over how she is perceived in social contexts. Such control may create a double bind, whereby individuals must manage not only their “difference” but also others’ perceptions of it. This strong sense of difference was often reported as having developed throughout childhood, with Jenny noting, “I always was aware of, from as young as I can remember, where I felt like I was different.”
Intensifying this sense of difference was confusion about the “arbitrarily enforced” rules and “confusing protocols” of social engagements in the neurotypical world. Such explanations were consistent across participants and reflect extant research findings about autistic girls and adolescents (Davidson, 2007; Gould & Ashton-Smith, 2011; Jones et al., 2013). Rejection by the dominant culture, combined with a lack of understanding of the mechanisms with which to engage with the dominant culture, revealed a justifiable sense of vulnerability. Jenny described feeling insecure throughout her life, and Jane provided a vivid image of a “terrified inner child” hiding within her, stating, “I rarely talk more than a simple greeting to people, except those I know well because I am afraid of feeling the rejection again and again.”
Concerns of insecurity and vulnerability are not unwarranted. Research has identified high rates of abuse of autistic girls and women (Bargiela, 2015; Cridland et al., 2014; Hurlbutt & Chalmers, 2002). Five participants disclosed instances of serious abuse during their lifetime. One woman experienced an emotionally abusive marriage, and three suffered child physical and sexual abuse, with one participant believing her autistic traits increased her vulnerability to sexual abuse. To reduce vulnerability and increase acceptance, participants modified or masked their behaviours, “because you very quickly learn, that if you behave in unacceptable ways, you’re not accepted” (Sally).
Masking behaviours included gestures, rehearsed phrases to facilitate conversation and suppression of non-normative behaviours such as flapping of arms or repetitive noises (Hull et al., 2017; Lai et al., 2017; Tierney et al., 2016), as Sally describes below: I’ve been conditioned to do it [in] non-visible ways, so I clench my toes, I press my toes into the floor or into my shoes, I mash my teeth together, [that] is one of my stims [demonstrates], clicking, socially acceptable things, like clicking my pen, or chewing.
Masking behaviour may seem problematic when enacted in a neurotypical world. However, for participants, masking was presented as a natural, subconscious performance and a deliberate, strategic behavioural tool used to manage and cope with social interactions. Participants learned phrases, prepared topics of conversation, and actively performed neurotypical, gender-conforming gestures to avoid social sanctioning: Back in school, I used to have my hand up a lot in class, and so I learnt to not put my hand up so much because I got told it was the reason I was being bullied because I knew too much and don’t put yourself out there so often and then, that is when I stopped putting myself out there. (Piper)
Jane highlights the complexity of authenticity and gender performance: “I disregard others’ opinions on how a woman should appear, but at times I do resent that others might be thinking I don’t dress or apply makeup in a suitable womanly way.” Ella purposely used masking to cope with the demands of motherhood, suggesting deliberate engagement with the mask to psychologically distance herself from emotional discomfort: At the time, I couldn’t cope, so I did what I could. I spent a lot of time out and about … I would just go out because I felt like I was so good at masking, I guess … I felt like a better parent when I was out and about … I’d crumble when I got home.
In line with the notion that masking may be enacted to avoid stigmatisation, or conversely, as an actual act of stigmatising the self, Ella's exhaustion speaks to a kind of existential depletion. This depletion is incurred through the act of rigid self-management whereby the need to manage the self, and the social expectations of others in the context of one's behaviour, may serve as a latent reminder of “defectiveness”. One might argue Ella's use of masking allows her to successfully achieve the social performance of gender and motherhood. However, the language of “success” may not be appropriate if an individual can “pass” the “test” of “concealment”, but at significant cost to their psychological welfare and wellbeing.
Descriptions of masking behaviours suggest participants are self-aware, engaged in active self-monitoring, and have a meta-representation of how the self is perceived by others, traits not usually associated with conventional constructs of ASC, suggesting current understandings of ASC may need expanding. Yet not all participants chose to mask. Piper explained she did not mask: “I suck at that, I wish I could [mask]”, adding, “I don’t do the copying thing, at least in recent years. I’ve just gone, well, bugger you if you don’t like me, and I’ll just be me, and I’ll just speak to someone else.” Nevertheless, for Piper, such openness carried consequences, with her outspoken behaviour in social settings contravening feminine gender norms, leading to ostracism: I was just never invited; I was just never invited to things. So, people look back at their photos from their late teens and early twenties of photos … of parties and weddings, and nope, nup, none of it's me. I don’t have those photos; I didn’t have any of those experiences. I got bullied out of an autistic mums’ group. Bullied. Out of an autistic mums’ group.
The desire to assimilate and the use of masking and camouflaging behaviours has been documented extensively in ASC literature (Bargiela, 2015; Davidson & Henderson, 2010; Gould, 2017; Hull et al., 2017; Müller et al., 2008; Punshon et al., 2009; Ryan & Räisänen, 2008).
Masking is a tool deployed by autistic women to enact gendered and social expectations. It reflects sophisticated social behaviour, given the self-awareness, self-discipline, and understanding of others’ evaluative responses, raising questions about the female ASC phenotype. While masking was motivated by a desire to reduce vulnerability and “otherness”, participants often failed to achieve these social goals. Participants reported ongoing marginalisation in the community, their relationships, and workplaces: [I mask] in every situation at work and in social settings with people I don’t know, so I don’t embarrass friends or look stupid to potential employers or work colleagues. I’m very aware of it, as it exhausts me, and I find it hard to concentrate on anything anyone says. I miss what people say all the time, and some think I’m stupid or uninterested and uncaring. (Sarah)
Sally masked “all the time” yet retained a strong sense of self as the outsider in relation to her hometown experiences: “people already disliked me and excluded me, I was just a bit too much to take, a bit too different, a bit too loud, a bit too, a bit too me.” Like Sally, participants relied heavily upon concealment, yet concealment was not necessarily effective in rendering their differences invisible. Where neuro-differences are concealed in social contexts over a period of time, it may be that women begin to experience a degree of identity confusion, creating further identity work for the individual.
While masking is framed as both natural and planned, it was, at times, an arduous, exhausting process for participants. They reported modifying their schedules around public encounters to meet the emotional and physical demands of masking behaviours. Surprisingly, participants did not attribute their mental health concerns to masking behaviours, but rather used masking behaviours to conceal mental health issues, as Jenny notes in context to social anxiety: “I get very anxious talking to people, but I kind of know how to cover it up and not appear nervous, whereas really, on the inside, I’m freaking out.”
The exhaustion of masking is thoroughly documented (Hull et al., 2017; Lai et al., 2017; Tierney et al., 2016; Tint & Weiss, 2017). Participants’ accounts suggest the performance of masking does not ease with time or practice, and a significant consequence of masking was loss of self. Jane identifies the permeable boundary between the self and the mask, describing confusion over time as to where the mask starts and stops: Maybe I simply am the wall. I don’t really know who I am. When I think about the mask, I don’t know which bit is the mask, which bit is myself, and which parts of the mask have fused to myself and become indistinguishable from it. It is only in the privacy of my own mind that I allow myself to express what might be the real me.
While authenticity was central to the way participants desired to approach the world, masking reflects a direct inhibition of such frankness of self, as Jane's narrative suggests: I was hidden behind a wall, a solid wall that keeps me in and hides me from the world. It was a wall of self-control that didn’t let emotions through like joy, excitement, love, hate, anger; it was blank and tended to reflect back to someone whatever they were expressing themselves … I worry that one day it will come tumbling down and completely overwhelm me.
Without authentic interactions, cognitive dissonance develops concerning how the individual sees themselves and how they see themselves presented to others (Hull et al., 2017), resulting in psychological anguish.
To recover from the emotional cost of masking, participants described using self-care strategies. They created “micro spaces” in their environment. For example, Charlotte discussed arranging extra designated breaks at work to ensure she was not overwhelmed by the environment and Piper used headphones to reduce external stimulation. Maisy described relaxing with her family, challenging the assumption autistic individuals shy away from social interaction, and suggesting the need for masking may be reduced in close, safe, and accepting familiar environments.
The need to create space as a coping mechanism is supported by previous research (Davidson, 2007; Gould, 2017; Ryan & Räisänen, 2008; Whitley & Denise Campbell, 2014). The current study demonstrated participants’ self-awareness pertaining to their psychological boundaries and capacity to implement appropriate strategies to manage their experiences of ASC, something not usually associated with ASC, wherein the individual is rarely understood as possessing self-awareness nor seen as capable of acting strategically in accordance with this awareness. This may reflect the sample obtained for this study; however, these findings raise questions around the defining features of ASC in general and the phenotype for autistic women.
Theme 2: Lost identity found: Finding the authentic self
The second theme concerns the impact of diagnosis on an individual's subjectivity and wellbeing. For participants, an ASC diagnosis allowed them to construct a coherent narrative of their past experiences and strengthen their identity. Diagnosis allowed participants to embrace their ASC traits and live authentically, reducing the need for masking and improving wellbeing. This positivity towards diagnosis is contrary to the negative portrayal of an ASC diagnosis usually seen in mainstream media. However, the long process of obtaining the diagnosis and the attitude of clinicians was not perceived positively, as expressed by Maisy, who stated: “I found the process of getting a diagnosis is [focused] on the negative. It's giving bad news, and less hope for the future.” Piper and Jenny both discuss the implications of the dominant, deficit model on clinicians’ understanding of ASC presentation in women: I had a hell of a time getting diagnosed cause I had any number of clinicians go, “Oh look, you’re a parent, and you got married, and you have a job; therefore, you can’t be autistic.” (Piper)
The GP dismissed me with, “I think if you finished university, you can’t have Asperger's”, but decided I was depressed enough to see a psychologist anyway. (Jenny)
That diagnosis was experienced and constructed positively by most participants is interesting to note, given diagnostic tools and processes relating to autism were not designed with women in mind. Participants were aware they were not the “target audience” of an ASC diagnosis, and interestingly, this created a sense of freedom in contextualising their own ASC presentation. Participants did not position themselves as feeling pressured to conform to ASC stereotypes or to present in narrow alignment with diagnostic criteria. They framed the experience of being diagnosed as a liberating moment imbued with explanatory power.
Women represent a non-normative category of ASC in terms of gender, and this allowed participants greater space to create meaning around their experiences of ASC, subverting the diagnostic process while also relying on it for validation. Participants largely rejected medical and stereotypical male constructs of ASC but nonetheless drew upon formalised diagnostic processes and understandings. Diagnosis served only to confirm to participants they were different, and this difference was beyond their control, and this may be more important than how “difference” is defined experientially or via diagnostic frameworks.
Prior to diagnosis, the lack of a framework to rationalise feelings of difference, combined with ostracisation from the dominant culture, led participants to believe they were intrinsically flawed. Women labelled themselves as “broken” (Piper), “worthless” (Jenny), “a failure” (Ella), while Maisy described herself as “the freak child”. This language reflects an internalised sense of blame and sense of personal responsibility for self-improvement that continued into adulthood, reinforced by societal and psychological discourses related to self-help, as Sally explicates: I spent the entire half, first half of my adult life trying to fix these things that were wrong with me, and, especially at the behest of my emotionally abusive, now ex-husband who thought I was lazy. I went on a crusade against myself. I read all the self-help books, the seven habits of highly effective people, and stuff, but nothing ever really stuck because it's all for neurotypical people.
These beliefs had a significant impact on participants’ emotional and psychological wellbeing as Jane voiced: “My sense of self, self-worth, confidence, and self-esteem were eroded over years of not feeling like I was good enough. I am still trying to overcome the belief in my brokenness and unworthiness to be loved.” Participants expressed feelings of depression, shame, insecurity, and a sense of not achieving their full potential or being offered the opportunity to live their authentic life.
Interestingly, two women described their past lives as relatively non-problematic in their experience of growing up with ASC traits. Charlotte, whose father displayed ASC traits, and Sarah, who was raised in a diverse community, did not identify with the negative stigma attached to their perceived difference. Identifying the self in others, experiencing acceptance, and living in a community with flexible cultural norms appeared to serve as a buffer from the sanctioning of the dominant culture, reducing identity confusion and self-blame. Charlotte and Sarah's experiences highlight the importance of representation and inclusion and support the social model of disability, whereby “the self materialises in response to its engagement with its environment” (Garland-Thomson, 2002, p. 20). When the environment is inclusive, the sense of isolation and difference reduces, and an autistic individual's sense of belonging and wellbeing is likely to improve regardless of diagnosis.
Post diagnosis, all women described a sense of relief and release. Maisy remarked, “just knowing, that is quite a relief and the other sense or feeling I got after I had processed the whole diagnosis was one of joy, and it wasn’t just your everyday happiness, it was a very heighten[ed] joyfulness.” Diagnosis was a pivotal point in participants’ negotiations of and with the self as they were able to embrace their unique traits and take control of the interpretation of their experiences. Once diagnosed, participants re-evaluated their lives and reframed past experiences with a compassionate lens. Internalised feelings of failure and shame shifted to an external arena, and participants’ self-perception and understanding improved. Diagnosis created a framework in which to process a coherent self-narrative and no longer pathologise thoughts and behaviours. With a diagnosis, participants were released from others’ expectations of them, and they did not have to try and assimilate into society. Sally stated, “So now I can work around it and stop trying to change things that I’m not going to be able to change.”
Participants spoke of creating a more authentic life post-diagnosis, revealing previously concealed personality characteristics, despite implicating themselves in significant stories of masking, suggesting that masking and authenticity are not necessarily positioned as antithetical to one another within the context of ASC. They became less protective of themselves and gained the confidence to disclose their diagnosis. Diagnosis legitimised participant requests for provisions in the workplace, and participants were able to discuss their traits and needs with close friends, reducing the need for masking. Sally demonstrates the self-acceptance and peace that follows from diagnosis: I’ve come to accept, especially since getting my diagnosis, I’m not the same as other people, and knowing it on a deep level since I was very young, and now understanding why that's the case, I’m pretty happy with the way I am, I’m not everybody's cup of tea, and that's okay.
This positive response to diagnosis is reflected in the literature (Bagatell, 2007; Punshon et al., 2009). Positive responses to late diagnosis may reflect a maturity and self-acceptance that comes with age. In this study, most participants had somewhat successfully navigated the milestones of life such as moving out of home, completing tertiary education, marriage, children, and employment, and therefore did not harbour the trepidation parents of autistic children or autistic adolescents may have about their future. This highlights the importance of visible autistic female role models in the community for clinicians, families, and autistic girls navigating the future.
Despite such positivity, the stigma of ASC was, to some degree, internalised, with participants often reframing ASC traits as those of another disorder. Piper informs people she has attention deficit hyperactivity disorder (ADHD), and Sally self-selects traits perceived as less problematic: I don’t always disclose my entire diagnosis; I use language like, I have some facial blindness, which means I often recognise your face, and I will recognise names if I see them written down, but I have a great deal of trouble putting them together.
Active reconstruction of ASC traits is consistent with research findings (Davidson & Henderson, 2010). This strategy provides participants with a sense of control and may lessen the impact of stigma and create a sense of ease for others. The desire to put others at ease aligns with socialised, gendered expectations for women and speaks to a two-fold impetus for masking. On the one hand, this may be an act of social survival for the individual; on the other, it may be a strategy enacted to cause the least amount of possible disruption to others.
Diagnosis was a complex subject. Several participants expressed sadness at not receiving an early diagnosis. They believed an earlier diagnosis would have allowed them to live better lives. Others suggested early diagnosis may not have been beneficial and could have suppressed their growth and development due to the dominant deficit model of ASC: If I was diagnosed as a child and the clinician saw me at three years of age, I was nonverbal, what would they diagnose me with? They would diagnose me with an autistic disorder, and I would just be labelled as a nonverbal child who didn’t have much hope of integrating, who didn’t have much hope of learning social skills, and you kind of … what I mean by “damage” [of labelling] is all the assumptions that came [sic] with the diagnosis. (Maisy)
Ella and Jane questioned the benefits of early diagnosis, with Jane expressing gratitude she was not subjected to historical treatments for ASC. Maisy expressed similar sentiments to Jane, explaining how the adult autistic community refers to childhood treatments, known formally as Applied Behavioural Analysis (ABA) therapy, as “torture”.
Current clinical approaches to ASC emphasise early diagnosis to ensure children receive appropriate treatment. Women in this study highlighted important, potentially deleterious implications for early diagnosis that require careful consideration. Early diagnosis can result in an understanding of challenging behaviours, access to funding, and early intervention support services and may provide the individual with a sense of belonging to an autistic community. However, labelling informs how a person is perceived and treated (Klotz, 2004). This can be troublesome for children who have little agency over their interactions with others and, as such, internalise responses and messages from others about their “disability”, potentially constructing a pathology-oriented identity. As children's characteristics are often filtered through their diagnosis, the label of ASC and the stigma of deficiency may result in parents and teachers lowering their expectations of the child, reducing opportunities, and diminishing life chances (Bumiller, 2008).
Despite negative experiences with support services that adopt the deficit model of ASC, participants identified many rewards of ASC. They indicated if they had their time again, they would want their traits supported and celebrated rather than feeling pressure to conform, as Jane describes: “I want to be valued for who I am and contribute my gifts in my own way without being asked to fit someone else's idea of who I should be and what I should do.” Most participants also reported that their diagnosis gave them “a licence to legitimately interact with the ASC community” (Maisy). Community, mentors, and friendship were important for autistic women in developing connections and exploring and cementing identity.
In particular, engagement with online communities enabled participants to meet their need for connection and belonging and provided a virtual space for attachment. Participants were able to further understand themselves, their experiences, and ASC away from the deficit-focused medical model (Haney & Cullen, 2017; Molloy & Vasil, 2002; Ryan & Räisänen, 2008). This is illustrated by Ella's report: “I’m in quite a few groups with autistic women which has helped a lot to know who I am.” Online communities also allowed the women to control the level and type of interaction with others with minimal focus required for their self-presentation, as described by Jane: “I’ve managed quite well online, as I enjoy writing, and to me, the time to order my thoughts and edit what I am saying to make sure it means what I want it to mean.”
Online communities may offer protection when the media and general population misrepresent ASC (Crabtree et al., 2010) and provide an avenue for feminist autistic advocacy and activism. Online support and protection are essential for clinicians to consider when working with autistic females interested in developing their identity and ASC understanding. Online communities challenge the normative, deficit understanding of autism, may provide mentors to adolescent autistic girls who are vulnerable to bullying and abuse, and may offer a place of safety and connection where attachment needs are met and opportunities for advocacy are provided.
Implications, limitations, and future directions
This study had a small, self-selecting sample of autistic women. It cannot be assumed their experiences are representative of every autistic female, particularly those with co-morbidities or cognitive difficulties. This study did not include self-diagnosed individuals or those just below the diagnostic threshold. The experiences of these women are pertinent to understanding the power of social and patriarchal institutions, such as gender and medicine, on the experiences of ASC, particularly as undiagnosed women do not have the validation of a label. Future research may explore the experiences of diagnosed and non-diagnosed ASC women simultaneously.
The results of this study suggest autistic women are aware of and internalise societal expectations and norms and engage in disciplinary techniques such as masking. Participants engaged in masking behaviours to meet social expectations, manage interactions, reduce discrimination, and increase assimilation. Masking was not conceptualised as a form of inauthenticity but rather a form of social survival, yet it carried psychological consequences, and the mental toll of concealment was not inconsequential.
It may be argued that a patriarchal society asks all women to internalise and meet societal expectations. This is not new or novel. However, the experiences of autistic women reflect the intersection between disability stigma and the gendered discrimination that women experience in daily life. As well as performing gender, autistic women were required to perform neurotypicality, with an added layer of concealment, self-monitoring, and ultimately, surrendering of self to the norms of the dominant class. The women did not attribute masking behaviours to poor mental health, noting the experience of subjective difference, discrimination, and isolation in their younger years led to experiences of depression and anxiety. However, masking was an effortful task requiring participants to plan and implement self-care strategies to recover from engagement with public life.
From a feminist perspective, the need to engage in self-care is akin to the need for resilience; both constructs align with neoliberal ideals around self-improvement. Rather than encouraging periods of “recovery” from daily life as an individual responsibility, psychology may be better placed in attending to societal structures that delegitimise the lives of women across the neurodiversity spectrum (Joseph, 2013).
Diagnosis provided the participants with a socially and medically accepted framework to comprehend one's experiences and consolidate one's identity. These autistic women no longer positioned themselves as failures in need of relentless self-improvement but rather expressed compassion towards themselves and their needs. Diagnosis improved wellbeing as it gave the women permission to embrace their ASC traits and choose when and how to disclose them, thereby reducing the need for masking behaviours.
Participants’ experiences highlight the importance of education and training for clinicians in recognising ASC presentation in females; in particular, the importance of clinicians’ understandings of the traumatic and emotional experiences of autistic women throughout their lifespan and the role of psychology as a discipline contributing to the subjugation and trauma of autistic women. It would be valuable for clinicians to provide support to autistic women during times of transition, such as entering employment and motherhood and forming and negotiating significant interpersonal relationships, rather than focusing on behavioural management and modification. The nature of this support must be carefully evaluated to avoid reinforcing neoliberal frameworks of self-empowerment that ultimately fail to acknowledge the social context in which an individual makes choices and acts upon their social environment. Furthermore, autistic women may be key stakeholders in developing feminist-led agendas for equality and human rights.
This study also supports research indicating the importance of autistic communities for belonging and identity formation. Communities provide another frame of meaning-making that can be interposed over traditional deficit models of ASC found in medicine and psychology. For autistic women, these communities appear to bypass the traditional, masculinised spaces of medicine and psychology, allowing space for a more nuanced understanding of the intersections of autism and gender. These spaces may allow autistic women to resist critical boundaries in mainstream feminist thought. As such, the experiences shared, and knowledge created, in these spaces have implications for the discipline of psychology and liberatory feminist movements and are worthy of further exploration.
Our study extends current research seeking to understand autistic women and how they navigate a predominantly neurotypical society. It also demonstrates the significance of the voices of autistic women in the development of the construct of ASC and underscores the importance of attending to gender in the debate as to what constitutes a disability. This is particularly salient in the context of the role of psychology as the arbiter of diagnostic categories and processes, and in pathologising and stigmatising women's experiences in insidious, far-reaching ways (Ussher, 2011). In understanding women's experiences of ASC, it is critical to reflect upon how “normality” and “diagnosis” are intractably tied to gender, social class, and power.
In this way, our findings support the social model of disability that highlights the role of the cultural context in autistic women's challenges. These findings offer support for the movement away from the medical model view of ASC and towards an understanding of neurodiversity. However, further theoretical development may be required to refine the use of this theoretical lens to understand women's experiences of power, ableism, and gender in the context of autism. To this end, our findings contribute to a growing understanding of the autistic female phenotype and provide insights that can inform the assessment, diagnosis, and support of autistic women. We, therefore, recommend reviewing and reconfiguring extant diagnostic tools to better recognise autistic women, as well as autistic-led and autistic-informed training for clinicians and other gatekeepers.
Footnotes
Acknowledgements
We would like to acknowledge the women who volunteered for this project. We are humbled by your generosity, honesty, resilience, and passion. Thank you for your courage and for sharing your experiences with us.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.