
Abstract
Introduction
Adherence to a medication regimen is ‘the extent to which a patient acts in accordance with the prescribed interval, dose and dosing regimen'. 1 Adherence is frequently reported as the percentage of prescribed doses taken by the patient over a specified period of time. An acceptable level of adherence is often set at ≥80% of the recommended treatment regimen dosages.1,2 Poor adherence to therapeutic regimens is one of the most common problems in daily practice care especially among patients with chronic conditions and can carry dire economic consequences.
Lack of adherence to medical recommendations has been proposed as an important predictor of poor outcomes in patients with SLE. 3 – 5 The adherence rate has varied from 48% to 93% according to the method used. 6 Several studies have assessed different aspects of therapeutic adherence in SLE, mostly with self-report questionnaires and pharmacy refill data but none have used electronic monitoring of therapy. 6 – 15 With the development of nanotechnology more accurate methods of adherence measurement have become available. The Medication Events Monitoring System (MEMS; AARDEX Group, Sion, Switzerland) consists of a microchip placed in the cap of the medicine bottle which records the date and time of every opening. Special software captures information and calculates multiple adherence measures.16,17
The objective of this study was to quantify adherence to medical therapy among SLE patients using MEMS, to identify the predictors of poor adherence, and its association with clinical outcomes.
Methods
This was a longitudinal cohort study of 110 SLE patients who were recruited from publicly funded outpatient rheumatology clinics in Houston, Texas, USA: two were within the Harris County Hospital District facilities and the other one at the Michael DeBakey Veteran Affairs Medical Center (VAMC). Approval for the study was obtained from our Institutional Review Boards. After permission was given by the treating rheumatologist, patients were approached during a clinic visit. A research assistant was on site to identify potentially eligible patients. All recruited participants signed informed consent forms.
Patient inclusion criteria were: (i) age 18–80 years; (ii) fulfillment of the ACR SLE diagnostic criteria; 18 (iii) disease duration one to ≤15 years; (iv) treatment with steroids, disease-modifying drugs or immunosuppressants at the time of enrollment; (v) adequate cognitive status as determined by the research assistant; and (vi) English or Spanish Language proficiency as determined by the research assistant.
The parent study examined beliefs, attitudes, and self-reported adherence. Participating in the electronic monitoring component of the study was optional. Only those patients who agreed to electronic monitoring of medication are included in this report.
Data collection
Baseline demographic data included self-reported age, sex, ethnicity, education level, employment status, health insurance status, annual household income, number of household members, and marital status. Patient self-reported outcomes and health determinant instruments were assessed at baseline and at 3, 6, 12, 18, and 24 months. These included:
a visual analogue scale (VAS) to indicate patients’ perceived disease activity (0–10 scale, in which 10 represents the highest disease activity) the Center for Epidemiologic Studies depression scale, 10-item short-form (CESD-10; 0–30 scale, in which 30 represents the greatest depression)
19
the medical outcomes study social support survey (MOS; 0–5 scale, in which 0 represents the least support)
20
the 12-item short-form health survey (SF-12; 0–100 scale, in which 0 represents the worst quality of life; mental (MCS) and physical component scores (PCS) were calculated using norm-based methods).
21
For patients who spoke only Spanish proficiently, all questionnaires, scales, and surveys were translated into Spanish using standard methods: forward/backward translation by independent translators followed by bilingual group evaluation and consensus on item translation. At each patient visit, the physician filled out the patient’s disease activity using:
Comorbidities and medications were also reviewed and documented at each visit.
Laboratory testing
Laboratory testing was performed at baseline, 12, and 24 months including: erythrocyte sedimentation rate (ESR); C-reactive protein (CRP); complete blood count, creatinine, C3, C4, urinalysis, and anti-double stranded DNA antibodies.
Assessment of adherence
All participants in our study completed the 19-item compliance-questionnaire-rheumatology (CQR) 24 self-report to record their adherence to prescribed medications at baseline, 12 months and 24 months.
Patients who agreed to undergo electronic monitoring had their medication intake for prescribed oral SLE medications tracked using MEMS®. Adherence to nonsteroidal anti-inflammatory drugs or therapy for comorbidities was not measured. MEMS® are designed to compile dosing histories of oral medications. In this system, the cap of a standard plastic vial has microcircuitry that records the time and date the bottle is opened. The system assumes that every opening of the bottle signifies the prescribed dose is taken. Specific software (Quick Read® and PowerView®, Aardex) and a MEMS® reader were used to capture and analyze data. Three measures of adherence to oral SLE prescriptions were calculated. ‘Correct dosing’ was calculated as the percentage of days that the patient took the correct number of doses as prescribed: (Total number of days with a recorded event as prescribed)/(Total number of monitored days) x 100. 25 ‘Underdosing' was calculated similarly but with fewer doses than prescribed in the numerator. Likewise, ‘overdosing' was calculated with more doses than prescribed in the numerator. For methotrexate prescriptions, the adherence measures were calculated using weeks rather than days. For each patient the average of the percent correct dosing, underdosing, or overdosing was calculated for the entire two-year monitoring period. Adherence estimates were obtained for each individual oral SLE therapy and for all SLE drugs together. Occasional openings of the medication container that were unrelated to drug taking (e.g. opening for refills) were excluded from the analysis. These openings were assessed by patient interview and direct comparison with pharmacy refills. During the initial visit, patients were informed about the characteristics of the MEMS® technology, so they were aware of the monitoring capability of the caps provided.
Statistical analysis
Categorical variables were analyzed using chi-squared or Fisher’s exact tests. Continuous variables were analyzed using Student’s t-test, Pearson’s correlation coefficients, and one-way analysis of variance with Tukey’s honestly significant difference. For the analysis, education was dichotomized into high school diploma or less, and higher educational level. Multiple regression analysis was performed to identify predictors of adherence using a stepwise procedure with entry model criteria of p value ≤ 0.15 and removal criteria of p value > 0.05. A two-sided p value of 0.05 was considered statistically significant. Analyses were carried out using SAS software version 9.2 (SAS Institute, Inc., Cary, North Carolina, USA).
Results
Baseline characteristics of patients monitored with Medication Event Monitoring System (MEMS®)
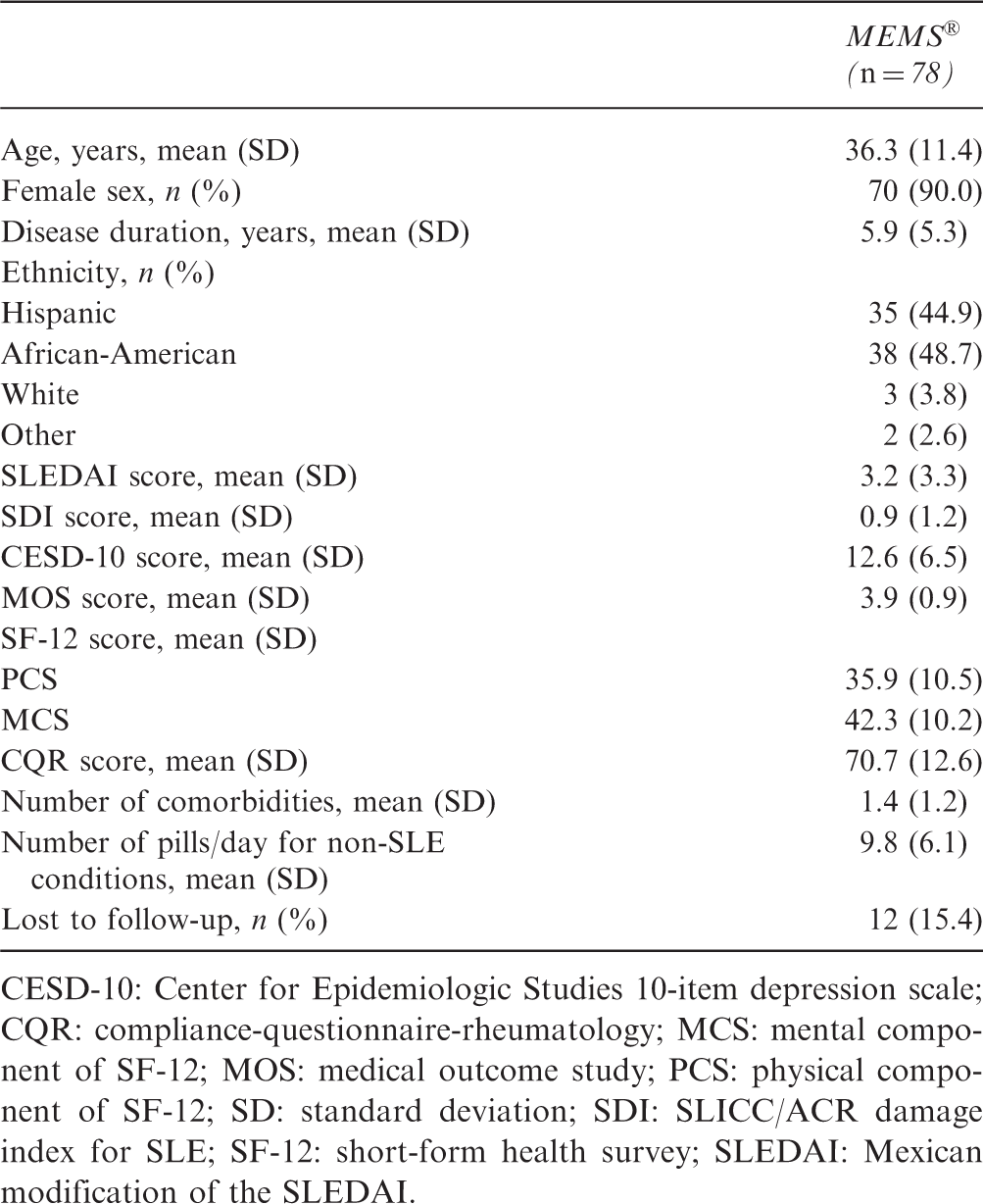
CESD-10: Center for Epidemiologic Studies 10-item depression scale; CQR: compliance-questionnaire-rheumatology; MCS: mental component of SF-12; MOS: medical outcome study; PCS: physical component of SF-12; SD: standard deviation; SDI: SLICC/ACR damage index for SLE; SF-12: short-form health survey; SLEDAI: Mexican modification of the SLEDAI.
Adherence measures using Medication Event Monitoring System (MEMS®) dosing of monitored prescriptions
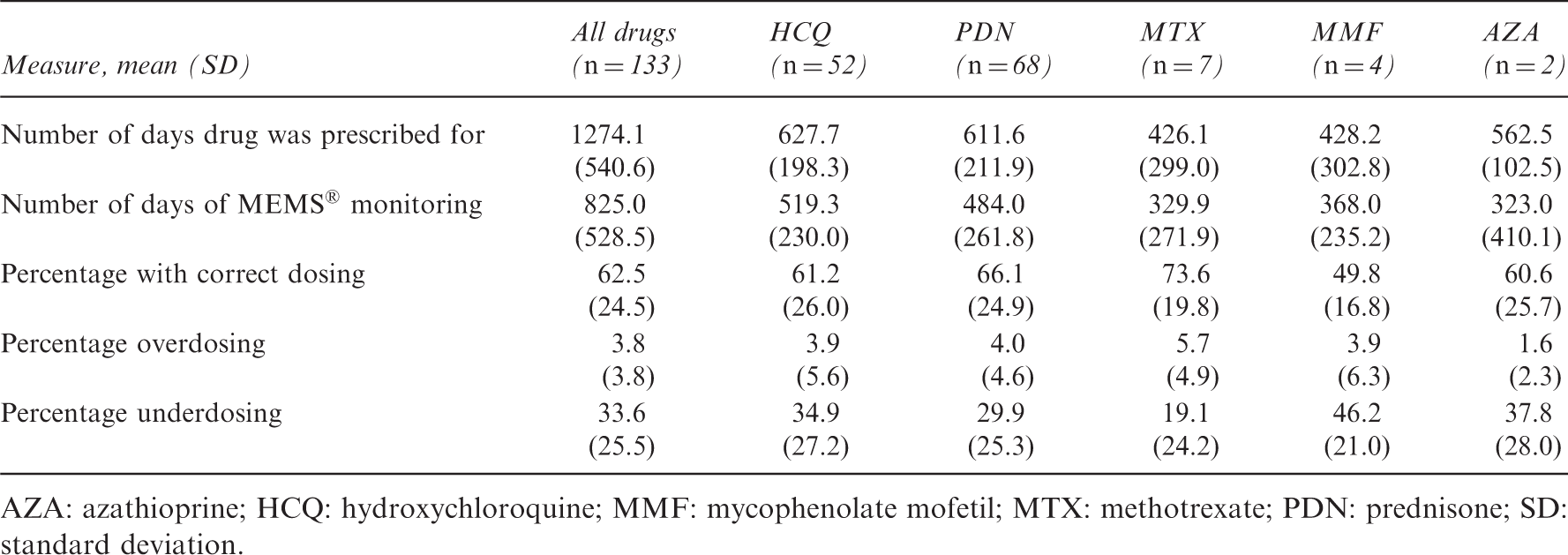
AZA: azathioprine; HCQ: hydroxychloroquine; MMF: mycophenolate mofetil; MTX: methotrexate; PDN: prednisone; SD: standard deviation.
For the analyses examining predictors of adherence, we considered all drugs together and prednisone or hydroxychloroquine independently. Lower numbers of patients received mychophenolate mofetil, methotrexate and azathioprine, and therefore these drugs were not evaluated individually but were added to the overall adherence analyses.
Bivariate analysis of baseline sociodemographic variables and clinical outcomes with percentage of correct dosing taken, for all monitored oral systemic lupus erythematosus (SLE) prescriptions, hydroxychloroquine (HCQ), and prednisone (PDN)
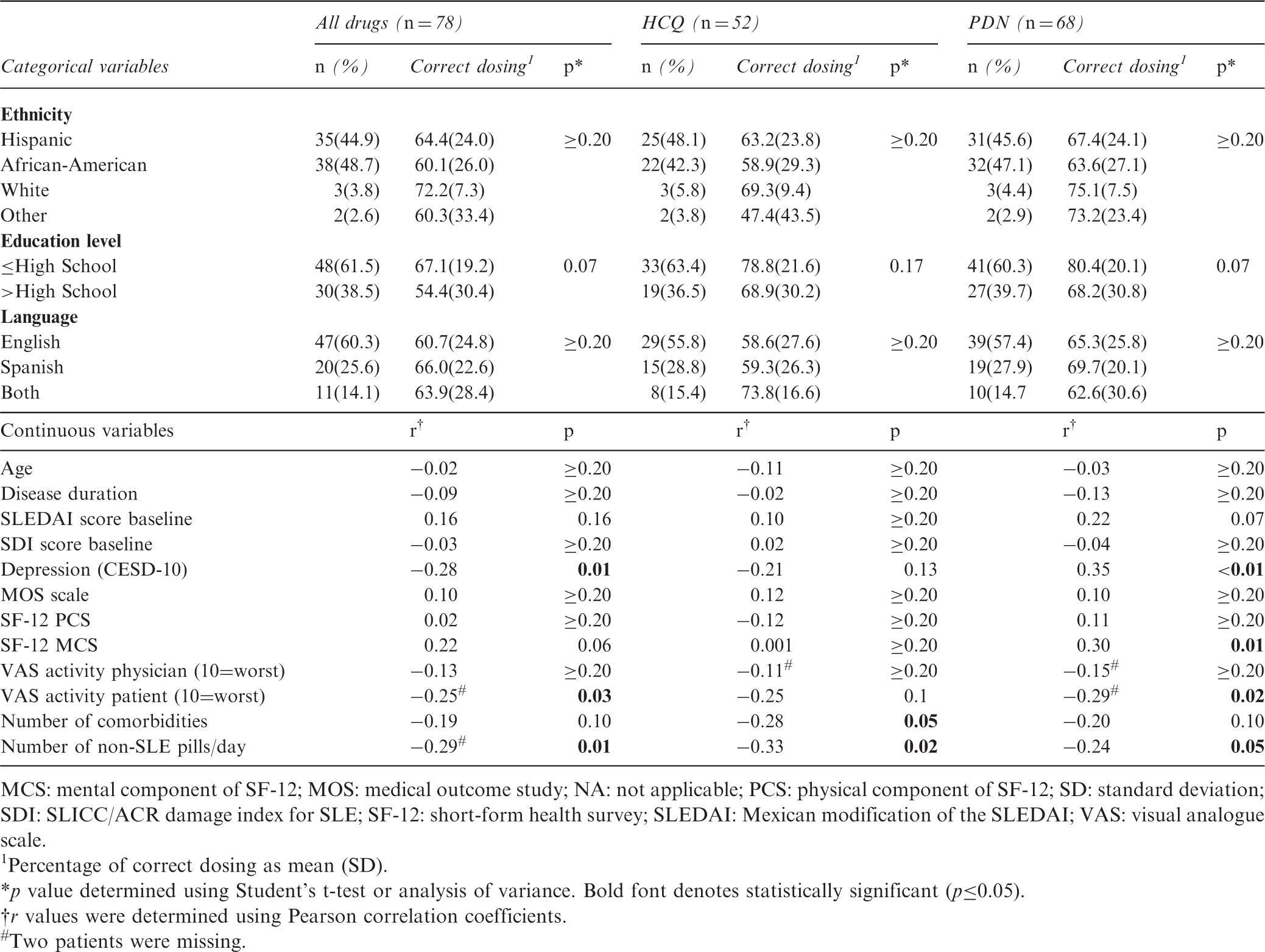
MCS: mental component of SF-12; MOS: medical outcome study; NA: not applicable; PCS: physical component of SF-12; SD: standard deviation; SDI: SLICC/ACR damage index for SLE; SF-12: short-form health survey; SLEDAI: Mexican modification of the SLEDAI; VAS: visual analogue scale.
Percentage of correct dosing as mean (SD).
p value determined using Student’s t-test or analysis of variance. Bold font denotes statistically significant (p≤0.05).
r values were determined using Pearson correlation coefficients.
Two patients were missing.
Relationship between adherence and outcomes at two years
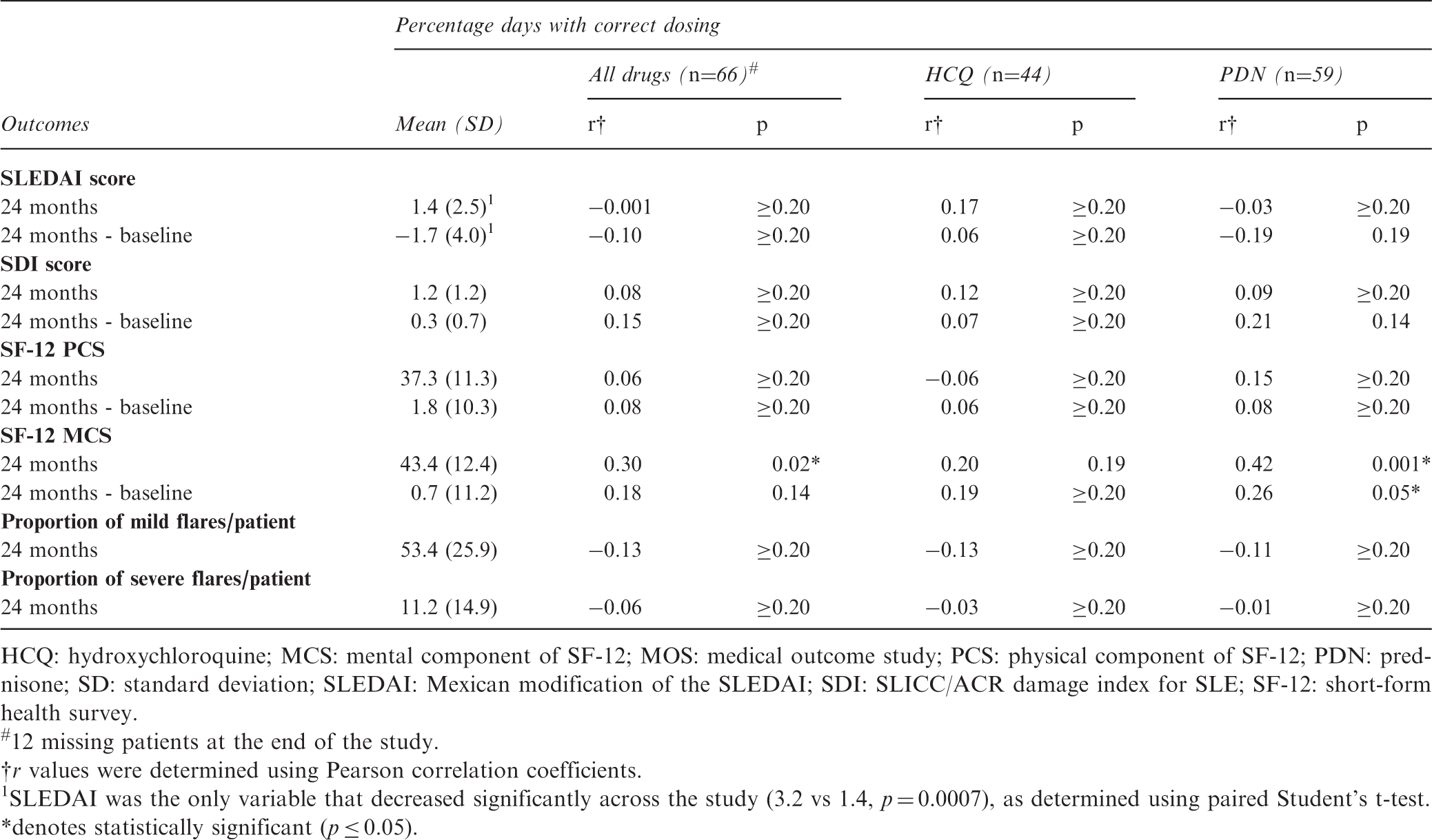
The only variable that statistically significantly changed between baseline and two years was the SLEDAI score, showing a decrease in SLE disease activity. However this change was not significantly associated with adherence. At two years the only variable significantly positively associated with adherence was a higher score for mental component of quality of life (p = 0.02) (Table 4). When considering the conventional cut-off of ≥80% for an acceptable level of adherence, we observed that only 16 patients (24%) had achieved that goal. At two years these 16 patients had a statistically significantly higher quality of life mental component score than did the 59 patients who had a compliance rate of <80% (50.4 vs 41.2; p < 0.01) (Figure 1). No significant differences were observed for SLEDAI score (1.4 vs 1.6; p = 0.15), SDI (1.0 vs 1.6; p ≥ 0.20), SF-12 physical component score (37.2 vs 37.7; p = 0.90), or proportion of visits with flares (59% vs 53%; p ≥ 0.20).
Mental component of quality of life between patients with all drugs >80% treatment adherence, as determined using Medication Event Monitoring System (MEMS®). SF-12: short-form health survey. Correlation between outcomes at 24 months and percentage of correct doses taken for all monitored oral systemic lupus erythematosus (SLE) prescriptions, hydroxychloroquine, and prednisone HCQ: hydroxychloroquine; MCS: mental component of SF-12; MOS: medical outcome study; PCS: physical component of SF-12; PDN: prednisone; SD: standard deviation; SLEDAI: Mexican modification of the SLEDAI; SDI: SLICC/ACR damage index for SLE; SF-12: short-form health survey. 12 missing patients at the end of the study. r values were determined using Pearson correlation coefficients. SLEDAI was the only variable that decreased significantly across the study (3.2 vs 1.4, p = 0.0007), as determined using paired Student’s t-test. denotes statistically significant (p ≤ 0.05).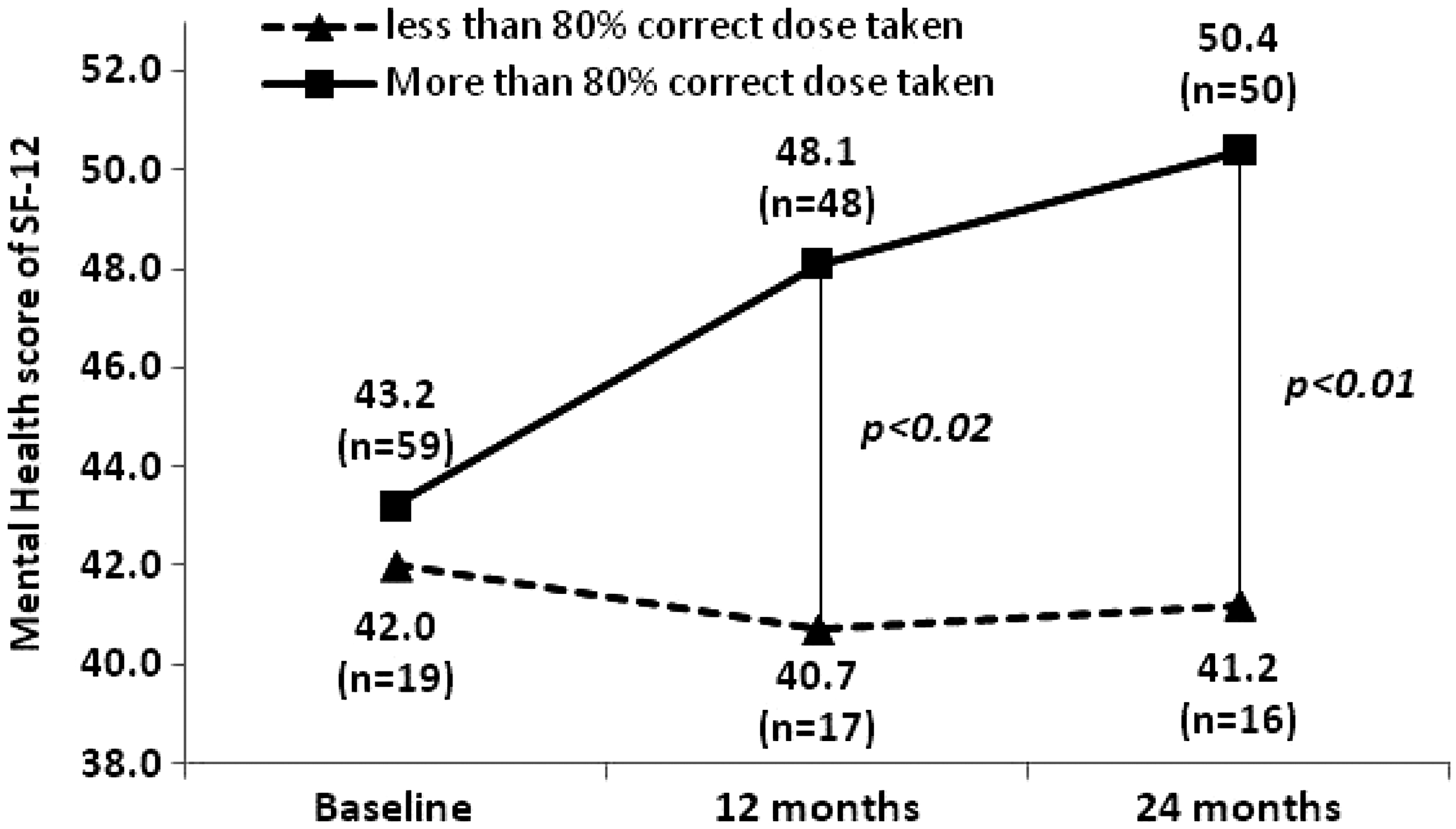
Discussion
The primary objective of this study was to quantitatively measure adherence to oral therapies in patients with SLE using electronic monitoring over a two-year period. To our knowledge, this is the first treatment adherence study of SLE patients using MEMS®. Of the available methods for measuring adherence, MEMS® is the closest to gold standard since it allows the day and precise time of every bottle opening to be obtained. 26 Our sample was comprised of mostly ethnic minority patients receiving care at publicly funded clinics. We found that only 20% of patients had an adherence rate of ≥80%. Polypharmacy and depression were associated with lower adherence.
Previous studies examining adherence with questionnaires or pharmacy refills also showed poor adherence among SLE patients, varying between 48% and 93%.6,7,9,10,13–15,27 In our study, adherence to specific drugs did not significantly differ, which is consistent with data reported by Koneru et al. 10 for prednisone, hydroxychloroquine, and other immunosuppressants.
Because SLE is a chronic disease that requires lifelong treatment, certain problems can hinder treatment adherence. In this study polypharmacy and depression were the only statistically significant characteristics associated with lower adherence rates. The association between education level and adherence in lupus patients has been studied previously.7,9,11,14 but only Koneru et al. showed that low education was related to poor adherence. 7 Treatment adherence is a complex process that results from the interaction of multiple factors. An individual’s health-related behavior depends on his/her perception of four critical areas: the severity of a potential illness, the perceived susceptibility to the effects of that illness, the benefits of taking an action, and the barriers to taking that action. 28 Beliefs and attitudes related to these domains could vary among patients and could potentially explain adherence variation.
Many patients with lupus have comorbidities such as hypertension, dyslipidemia, depression, coagulopathies, and osteoporosis, each of which may require one or more drugs for adequate control. This prescription medication burden can result in an increased incidence of adverse events and health-related costs which can also impact patient adherence. 2 In our study, the number of pills taken was a statistically significant predictor of non-adherence, pointing to the relevance of discussing the importance of each specific drug in patients receiving polypharmacy therapy.
Depression was another independent risk factor associated with non-adherence in our study. Our finding is consistent with that from a previous study, which showed that among patients with SLE, depression is associated with medication forgetfulness. 9 Evidence shows that depressed patients have poorer overall self-care and lower self-efficacy, favoring poorer treatment adherence and lower quality of life. 29 Psychological factors play an important role in patient outcomes. 30 The present findings also suggest that better treatment adherence is associated with better mental health among people with SLE. However, the direction of this effect cannot be clearly established. On the one hand patients with better mental health status might be more adherent but it is also possible that adherence leads to increased self-efficacy and better mental health status.
Our study failed to show an association between treatment adherence and traditional SLE outcomes such as disease activity and organ damage. We believe this was partially due to the fact that we included in our study both patients who had been recently diagnosed and patients with established disease. The latter may have fewer changes in disease progression over a period of time of two years. Furthermore, our sample size only had power to detect moderate to large associations and smaller effects may have been missed. A limitation of our study is that MEMS® caps only record the time the patient opens the bottle and not direct intake. Nevertheless, this is also a limitation with all other measures of adherence such as pharmacy refills or self-report, and MEMS® technology is considered the gold standard for adherence, only surpassed by direct intake observation which is impractical for daily oral therapies. While patients may open their bottles and not take their medications, such a behavior over several months would require a persistent routine and continued malfeasance, which are unlikely. 16
Adherence to treatment is crucial to the successful management of chronic diseases. Several interventions have been developed to improve adherence with long-term therapy but many are complex and only a few have been shown to improve adherence. 31 An important determinant of adherence is communication between the health provider and the patient. There is evidence that patients with SLE who participate more actively in their physician visits have better outcomes. 32 Effective communication about the nature of SLE, patient participation in decision-making, and motivating patients can conceivably improve therapeutic adherence.
Our study shows that almost 40% of SLE patients did not take their medications as prescribed. In addition, we also showed that patients with better adherence to oral SLE medications had significantly better mental health at two years. Depression and a high pill burden predicted non-adherence. Physicians and allied health care providers should attempt to identify patients at risk for non-adherence, and take the time to ask if a patient is taking the prescribed medications properly, and explore if any additional factors such as depression or other comorbidities may interfere with the adequate management of SLE.
Footnotes
Acknowledgements
We would like to thank Ms Vanessa Cox for initial data management.
Funding
This publication was made possible by Grant Number R01 AR47858 from NIAMS/NIH. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIAMS or NIH. Dr. Suarez-Almazor is a recipient of a K24 award from NIAMS.
Conflicts of interest statement
None declared.