
Abstract
Objectives
The objective of this report is to investigate the feasibility of collecting patient-reported outcomes (PROs) via e-questionnaires delivered to patients with chronic inflammatory diseases (CIDs).
Methods
Consecutive outpatients with a confirmed diagnosis of systemic lupus erythematosus, primary Sjögren’s syndrome or inflammatory bowel disease were followed at two medical departments. Patients received monthly e-mails containing the SF36, Hospital Anxiety and Depression scale and an analogue symptom scale over a six-month period. Participation rate, socio-demographic characteristics and patients’ satisfaction were analysed.
Results
A total of 128 patients were included (79% female; mean age: 42 ± 12 years). Eighty-two per cent of questionnaires were returned. The monthly participation rate ranged from 89% to 77%, with a six-month attrition rate of 13%. The mean completion rate of questionnaires was 98%. Factors significantly associated with increased answer rate were: married/couple status, greater number of children at home and previous participation in online surveys. The main reasons for non-response were: ‘too busy to participate’ (35%) and ‘away from home Internet access’ (31%). Overall, 68% of the participants found the study convenient and 96% agreed to continue at a monthly or bimonthly frequency.
Conclusion
Online home self-assessment of PROs was feasible in the setting of CIDs. Patients were satisfied and willing to continue the survey. The Internet allows immediate and sophisticated presentation of PROs to clinicians. Future studies are warranted to determine how PRO monitoring may contribute to routine care in CIDs and other diseases.
Introduction
Patients with a chronic inflammatory disease (CID), such as systemic lupus erythematosus (SLE), primary Sjögren’s syndrome (pSS) or inflammatory bowel disease (IBD), often have impaired quality of life.1–6 Measuring physical or biological parameters is not sufficient to fully assess how the disease affects their daily lives. Collection of health-related patient-reported outcomes (PROs) may be important in patients with multiple chronic conditions involving multiple care providers and complex treatments.
Recently, there has been growing interest in the use of PROs in daily clinical practice.7–12 The serial collection of PROs over time may help to detect early health or psychosocial problems, facilitate communication and shared clinical decisions, monitor changes or responses to treatment, enhance patients’ satisfaction with care, and finally may ameliorate patient management and treatment outcomes.13,14
Previous studies, in paediatric or adult oncology, or in psychiatry, have shown that periodic PRO monitoring increases discussion of emotional and psychosocial functioning and improves patients’ well-being and satisfaction with care.15–18 Some authors have postulated that this could be due to the improved memory of patients and their ability to describe their problem, which leads to the identification of problems that patients or physicians might not have raised. 19
The logistical problem of gathering questionnaire data can now be overcome by Web-based administration. Internet technology, widely available in patients’ homes and in medical institutions, allows the automatic and minimally burdensome collection of data, and makes it feasible in busy clinical practices.20–22 Moreover, the important issue concerning the equivalence of scores derived from electronic and paper-pencil questionnaires has been assessed by a meta-analysis suggesting that PROs vary little across the different modes of administration. 23
The evolution of CIDs is marked by the recurrence of flare-ups, which can be triggered by stress or anxiety, and the early recognition of changes in these emotional factors could be of value to anticipate and prevent disease flares. Accordingly, PRO evaluation and follow-up could be interesting in such a population.
To date, no study has evaluated the possibility of online PRO provision in adults with CIDs who are at particular risk of quality-of-life impairment.
Objective
The aim of this study was to investigate the feasibility of collecting PROs via a monthly e-questionnaire delivered to patients with CIDs.
Patients and methods
Study design
This was a prospective cohort study using electronic collection of PROs during a six-month follow-up period.
Study population and recruitment
Consecutive outpatients with a confirmed diagnosis of SLE, pSS or IBD, followed by our internal medicine or gastroenterology departments, were asked to participate in the study. Neither of these two departments had performed PRO collection before the study. This mono-centre study took place in a tertiary hospital over a seven-month period. Eligible individuals were identified by their regular physician, during an outpatient visit, over the one-month inclusion period. Inclusion criteria included: (i) outpatient aged 18–65 years; (ii) CID diagnosis confirmed using internationally recognized criteria;24–26 (iii) available computer, Internet access, and e-mail address; and (iv) regular use of the Internet (i.e. at least once per week, for >1 year). Exclusion criteria were: (i) patient hospitalized for >4 weeks during the 12 months prior to inclusion (to exclude patients with severe disease); (ii) patients under guardianship; and (iii) previous experience with the same online questionnaires. All patients gave their written informed consent at the time of inclusion.
Intervention and data collection
In order to evaluate ‘real’ feasibility, no specific training was given for the e-questionnaires. Every month, participants received an automatic e-mail, which contained a link to the e-questionnaire. Access to every e-questionnaire was available for a period of 10 days. An automatic e-reminder was sent after five days to participants who had not yet completed the e-questionnaire. Every e-questionnaire contained 28 questions, corresponding to a French-version of the Short Form 36 (SF36), a French-version of the Hospital Anxiety and Depression (HAD) scale and a visual analogue scale measuring patient-reported disease activity (Figure S1, supplementary material can be found online with this article, http://lup.sagepub.com). The e-questionnaires were prepared and hosted on the website www.evalandgo.com (Evalandgo©, Montpellier, France). All data except e-mail addresses were anonymized. Access to the website was protected by passwords for the participants and researchers. Data collection was performed automatically through the website facilities and finally exported to an external database for the analysis. Eval&GO© is a professional survey software and is committed to protecting privacy and confidential information (SSL protocols). It is authorized by the French Commission Nationale Informatique et Liberté (CNIL). At the end of the study, participants were sent satisfaction e-questionnaires. In addition, participants who did not reply to ≥1 e-questionnaire received a non-response questionnaire, offering them the opportunity to explain why. During the study, physicians were not informed of the results of the e-questionnaires concerning their patients.
Statistical analysis
Data are described as frequency and percentage for categorical variables and median (25th–75th percentile) or mean (standard deviation; SD) for quantitative variables. Categorical variables were compared using Fisher’s exact or Chi-square tests and continuous variables using Wilcoxon rank-sum tests when comparing two groups and analysis of variance (ANOVA) when comparing more than two groups. For this feasibility study, we planned to include ≥100 patients over a one-month inclusion period. Response rate was defined as ‘good’ when patients completed >4/6 e-questionnaires and ‘bad’ when patients answered ≤4 e-questionnaires. All tests were twosided and statistical significance was set at p < 0.05. All analyses were performed using R software version 3.02 (The R Foundation for Statistical Computing, Vienna, Austria).
Ethics and funding source
This study was conducted with the approval of the ethics committee of Limoges University Hospital, France (# 114-2013-14), the approval of the Comité consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé (CCTIRS #13.249), and the approval of the French CNIL (#913427). This study received no funding.
Results
Population, Internet use and disease descriptions
A total of 149 eligible patients were identified during the inclusion period. Sixteen patients (11%) were not included because they had no Internet access. Of the remaining 133 patients, five declined to participate for the following reasons: two did not have enough time, one did not want to hear about his illness every month and two did not give any reason for refusal. No patients were lost to follow-up, but 10 patients did not answer any e-questionnaire (Figure 1).
Flowchart of the study population.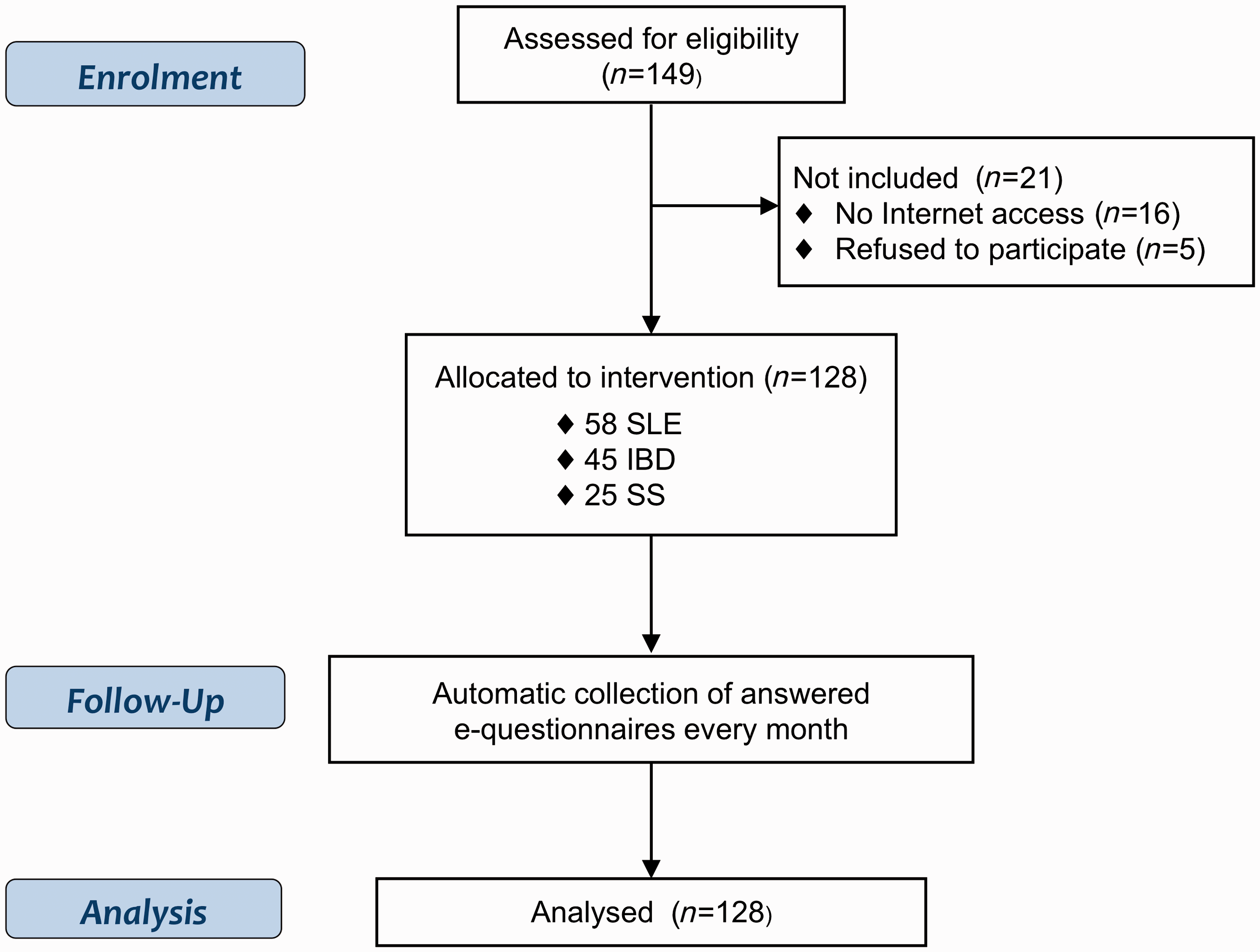
Comparison of the characteristics of the study population according to the number of e-questionnaires answered
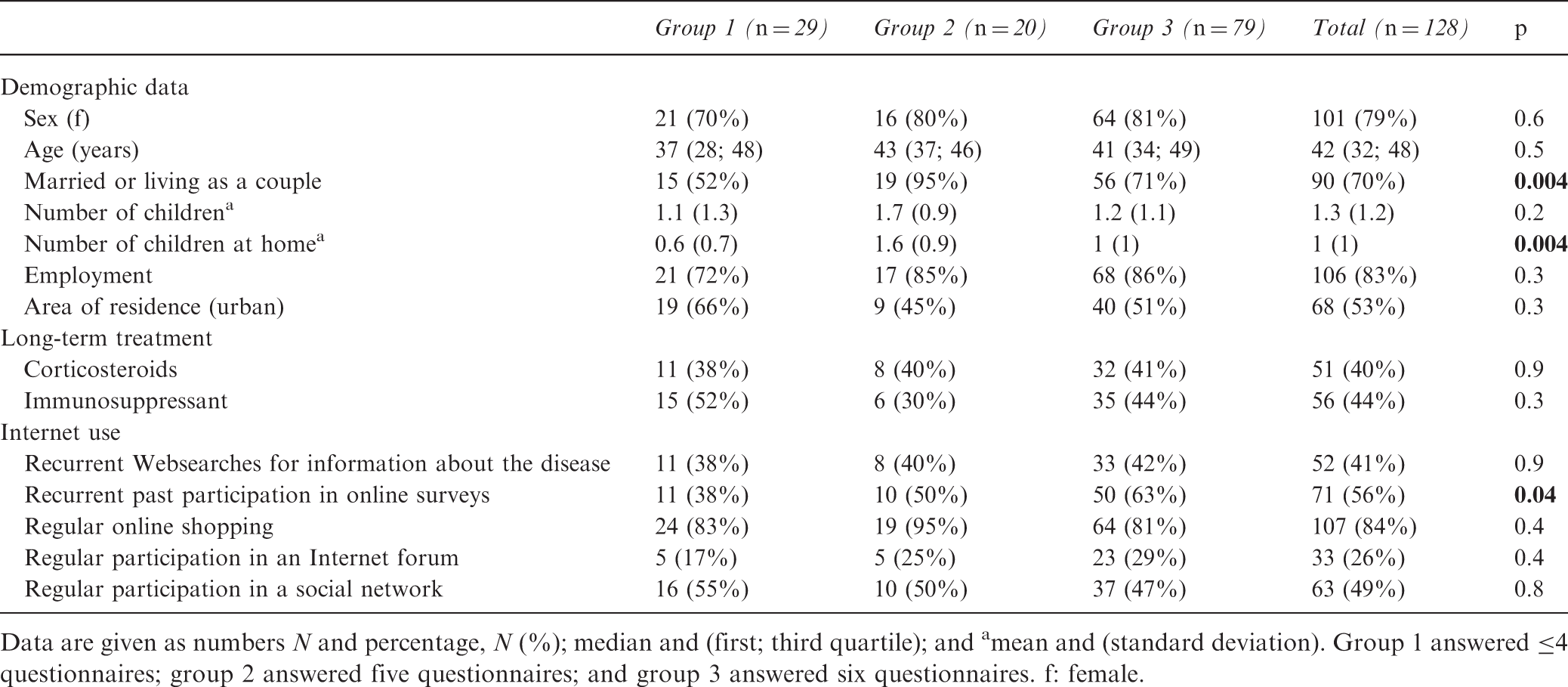
Data are given as numbers N and percentage, N (%); median and (first; third quartile); and amean and (standard deviation). Group 1 answered ≤4 questionnaires; group 2 answered five questionnaires; and group 3 answered six questionnaires. f: female.
The Internet was accessed via a desktop computer (52%), laptop (64%), tablet (14%) and/or smartphone (26%). The majority of patients (77%) reported Internet access more than once per day and 84% reported recurrent online shopping.
Among the 128 patients included, 20% (n = 25) had pSS, 35% (n = 45) had IBD and 45% (n = 58) had SLE. The disease duration was <5 years in 35% of cases, five to 10 years in 54% and >10 years in 40%. Overall, 90% of the patients were receiving long-term treatment, including corticosteroids in 40% (n = 51) and immunosuppressants in 44% (n = 56).
Participation rate
Over the six-month follow-up period, 768 e-questionnaires were sent to the participants, of which 626 (82%) were completed. The monthly rate of participation decreased over time from 89% (at month 1) to 77% (months 4, 5 and 6) (Figure S2). Thus, the six-month study attrition rate was 13%.
Overall, 77% of the patients (n = 99) responded to ≥5 e-questionnaires and 62% (n = 79) responded to all the e-questionnaires. Four patients responded to only one e-questionnaire, giving mean and median numbers of responsequestionnaires of 4.8 and 4, respectively. The mean completion rate of the e-questionnaires was 98.4% (±5.5) and the mean completion time was 12 minutes (±1.4). Completion time improved over the study period (Figure S2). Failure to complete the e-questionnaires (i.e. <50% completion) was rare as it occurred only once at months 1, 2 and 3 with three different participants. In all cases, this was the result of the early aborting of the answering process by the participant himself or herself (stopping after page n°1 or n°2).
Predictive factors
The predictive factors for good (five of six or six of six answered e-questionnaires) or bad (≤4 answered e-questionnaires) response rates were then investigated (Table 1). Married/couple status, a greater number of children at home and past recurrent participation in online surveys were significantly associated with a good response rate (p = 0.004, p = 0.004 and p = 0.04, respectively). The strength of the association between good response rate and married/couple status was odds ratio (OR) = 2.89 (95% confidence interval (CI): 1.12–7.50, p = 0.02) and that between good response rate and past recurrent participation in online surveys was OR = 2.56 (95%CI: 1.02–6.72, p = 0.02).
Low responding
After the study had ended, participants who had not responded to at least one e-questionnaire were asked by e-mail for the reason for non-response. The main reasons for low responding were: ‘too busy to participate’ (35%), ‘away from home Internet access – on vacation or in hospital’ (31%) and ‘temporarily or permanently lost Internet access’ (23%). Close examination revealed that there was no single profile of patients consistently contributing to lower response rates than their peers. Rather, individuals across the entire sample intermittently fluctuated for a variety of reasons.
Satisfaction
Patients’ satisfaction with the study
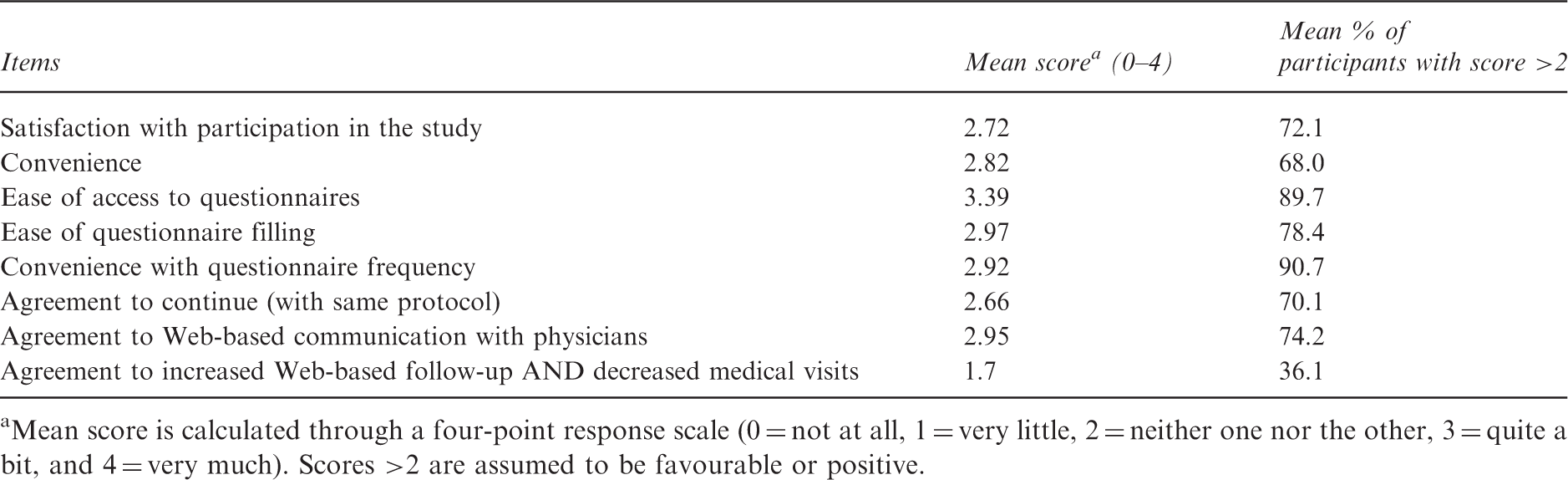
Mean score is calculated through a four-point response scale (0 = not at all, 1 = very little, 2 = neither one nor the other, 3 = quite a bit, and 4 = very much). Scores >2 are assumed to be favourable or positive.
Overall, the study was ‘convenient’ for 68% of patients and 96% agreed to continue with a monthly (56%) or bimonthly (21%) frequency. Two patients reported technical difficulties. In both cases, software compatibility problems were quickly solved by mail exchanges with the study investigator.
Discussion
The online collection of PROs by regular e-questionnaires to the patients’ homes was feasible and efficient, with a participation rate of >80%. Patients rated our system positively and found this method convenient. Moreover, the attrition rate was low despite the frequent e-questionnaire delivery. Participants also appeared willing to continue to complete self-assessments every month. Technical difficulties were extremely rare.
The analysis of patient profiles identified several predictive factors for e-questionnaire completion, such as married/couple status or a greater number of children at home. The presence of other individuals at home may increase the frequency of home Internet access and these patients may be more familiar and skilled with using the Internet. The higher response rate in the group of individuals with past recurrent participation in online surveys supports this hypothesis.
Overall, it was not possible to obtain a clear profile of patients with a better response rate. Low responding was sporadic and was distributed across the entire study population. Individual response rates fluctuated intermittently for various reasons, mostly a lack of time or a problem of access to the Internet at the required moment. As no clear profile can be distinguished, such an automated method of data collection could virtually be applied to other patients with CIDs. Further specific studies must be performed to confirm our results.
Limitations
The design of our study did not include a control group because it was a feasibility study. We could have designed a control group to compare the efficacy of online collection of PROs compared to paper-pencil standardized questionnaires. However, numerous previous studies have already compared these two modes of administration and have found no significant differences.23,27 In addition, online home collection of PROs, in real-life conditions, has been strongly suggested to reduce the Hawthorne effect, a distortion of symptom self-assessment by patients who know they are being surveyed.28,29
The attrition observed during the study may, at least partly, result from the absence of communication about the results between the patients and their regular physicians. This study was performed over a short time period, but with a high frequency of questionnaire delivery. However, after several months, patients’ enthusiasm would probably show signs of subsiding, especially if several physicians ask them to fill in different questionnaires relating to different conditions.Thus, the main obstacle to the sustained use of such a tool will be patients’ motivation after several weeks of experience. To ensure long-term routine collection of PROs, it will probably be necessary to characterize the best delivery frequency, to identify the most willing patients and to educate patients. 30
One of the main limitations of our study was the mono-centre design, which could have introduced recruitment bias. Nevertheless, although it was carried out in one centre, the inclusion of participants took place in two distinct units and was performed by different investigators. Although experienced in including patients in clinical trials, none of the investigators had previous experience in proposing online data collection to the patients. We also included patients with various CIDs, which made the sample heterogeneous. However, we did not identify any differences in response rate associated with the age of the participants, the nature of the disease, its duration or treatment. Taken together, these data suggest that online follow-up of patients may be applied to other departments involved in the management of chronically ill patients without the particular need for previous experience. This issue needs to be confirmed by further larger studies.
Another limitation arises from the selection of participants. We decided not to include people aged >65 years because of a priori lack of Internet access. Indeed, our study was a feasibility study among people who had access to the Web. Considering demographic changes, we acknowledge that Internet use will quickly spread among this population. Thus, a larger study that will include the elderly will certainly be necessary in future to assess the feasibility of such a data collection. People with a history of prior hospitalization within the year before inclusion were also excluded. As it reflects more severe disease, this was supposed to bias the results because of more frequent re-hospitalizations. Nevertheless, as they were excluded, the results of our feasibility study cannot apply to such a group of patients.
One can notice that the majority of our patients were married or living as a couple and had a job. As we included the patients consecutively, this reflects only the population that is referred to our tertiary hospital units. Larger studies are needed to assess the feasibility of PRO collection using the Internet under less-specific circumstances.
Finally, it remains to be determined how these data can be useful to the physician in daily practice. In a previous survey, we asked patients and physicians about their Internet use and expectations. 30 All physicians declared that they used the Internet during their daily practice and 54% were interested in Web-based follow-up, mostly for treatment surveillance and early recognition of disease flare-ups. Overall, 75% of the physicians wanted e-Health and e-Medicine expansion.
In the near future, we plan to study the impact of online assessment of PROs on medical decisions. To illustrate our purpose, Figure 2 shows an example of what could be automatically displayed on a physician’s computer during a routine medical consultation. PROs are pooled into several dimensions and the doctor, patient or both have filled in social or medical events.
Example of what could be displayed on the physician’s computer.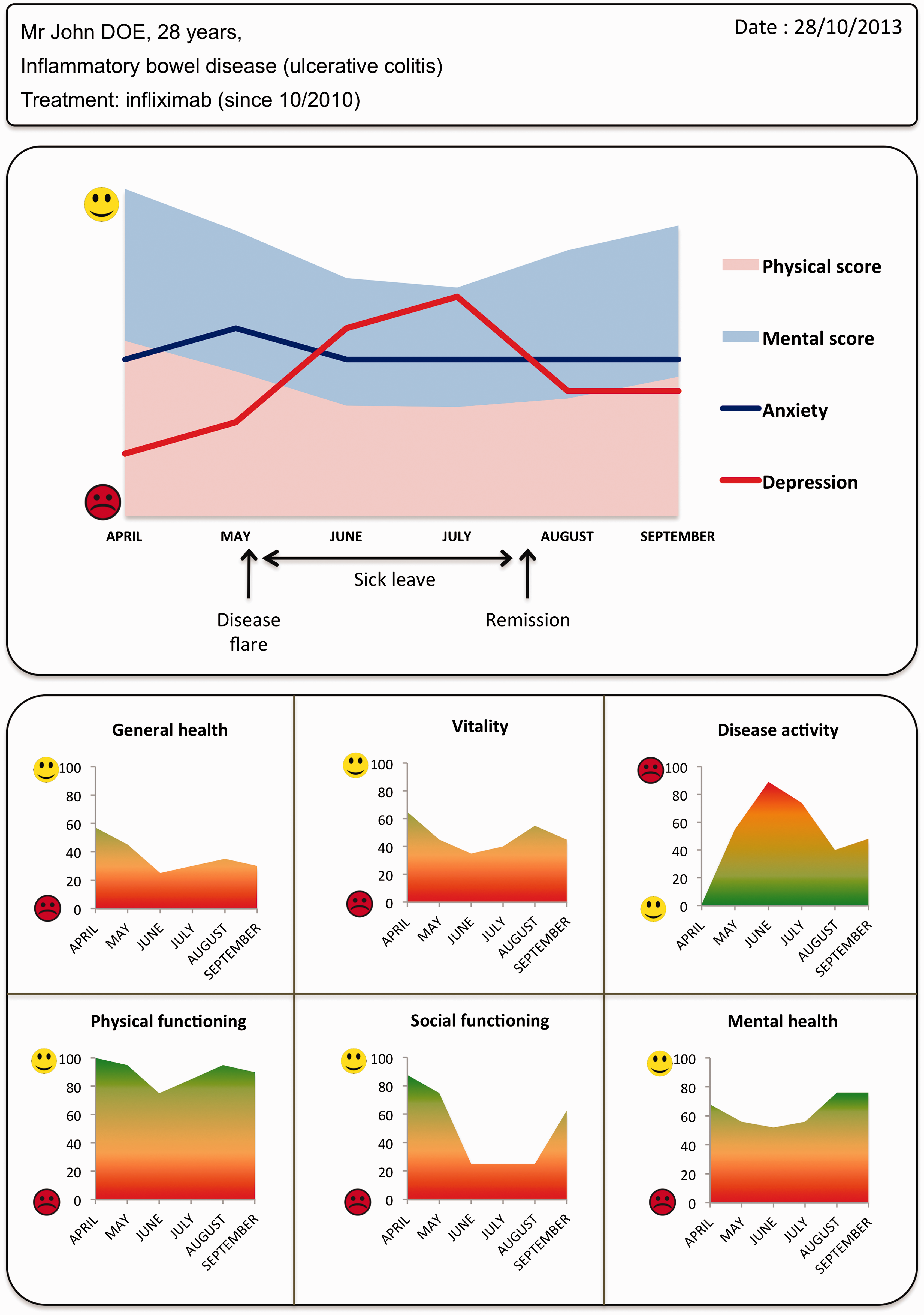
This study has shown that online home self-assessment of PROs is feasible and could be generalized to a wide range of chronic diseases. Future studies that include more patients and under less-specific circumstances are needed to confirm that this method is efficient, burden-less and useful.
Footnotes
Acknowledgements
The authors thank Dr S. Lyle for critically reviewing the manuscript and for her help with the language and editing.
All authors approved the entirety of the submitted material and contributed actively to the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.