
Abstract
Objective
The objective of this paper is to assess the role of gender on survival rate and causes of death and organ damage in systemic lupus erythematosus (SLE) patients in China from 2009 to 2015.
Methods
We conducted a multicenter cohort study to analyze the differences in outcome data between male and female SLE patients. A group of 1494 SLE patients who fulfilled the 1997 American College of Rheumatology SLE classification criteria were enrolled in the Chinese Systemic Lupus Erythematosus Treatment and Research Group (CSTAR) registry from April 2009 to February 2010. All enrolled patients were followed up at least once per year from 2009 to 2015. For patients who could not attend the outpatient clinic, follow-up was conducted by telephone interview. We collected demographic data, clinical manifestations and damage scores (System Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI)). Survival rates were evaluated using the Kaplan-Meier method.
Results
This study included 1352 women and 142 men. The five-year survival rates were 92.0% for men and 97.6% for women. The survival rates of males were significant lower than for females (p = 0.019). Male patients received methylprednisolone pulse therapy and cyclophosphamide significantly more than female patients (p = 0.010). During follow-up, 12 male patients and 66 female patients died. The most common cause of death was infection (41.7%) for men and active SLE disease (27.3%) for women. At the end of the study, the major accumulated organ damages included renal (8.5%) and musculoskeletal (7.7%), and nervous system (5.6%) for men and renal (8.8%) and musculoskeletal (6.7%) for women. There were no significant differences in SDI scores between the two groups at baseline and at the end of the study.
Conclusions
Male SLE patients had lower survival rates than female patients. Male patients received more methylprednisolone pulse and cyclophosphamide therapy. The most common causes of death were infection for male patients and active SLE disease for female patients. The major accumulated organ damages were renal, musculoskeletal, and nervous system both for male and female SLE patients in China.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease with diverse clinical and immunological features. 1 During the last few decades, SLE prognosis has significantly improved, mostly because of earlier diagnosis, better immunosuppressive therapies, and improved management of associated complications, such as infection.2–4 Studies report five-year survival rates of more than 95% in some patient cohorts. 5 Previous studies have reported that male patients often exhibit a poorer prognosis, especially involving the renal, cardiovascular, and neurologic systems. 6 Higher mortality rates in male SLE patients have also been reported.4,5 There are no multicenter cohort studies evaluating outcomes between genders in Chinese SLE patients. Therefore, we investigated survival rate, causes of death, and damage in male and female SLE patients in China.
Methods
Patient recruitment and follow-up
We analyzed preliminary data from the Chinese Systemic Lupus Erythematosus Treatment and Research Group (CSTAR) online registry, 7 which included patients from 104 high-ranking rheumatology centers, covering 30 provinces in China. The Medical Ethics Committee of the Peking Union Medical College Hospital, Chinese Academy of Medical Sciences (Approval number, S-197), the lead study site, approved this study. Written informed consent was obtained from all patients. Baseline data were collected for 1494 Chinese patients with SLE who fulfilled four or more criteria for SLE diagnosis as defined by the 1997 revised American College of Rheumatology (ACR) criteria.8,9 Patients were registered between April 2009 and February 2010. All enrolled patients were followed up at least once per year. For patients who could not attend the outpatient clinic, follow-up was conducted by telephone interview. Patients who ceased follow-up or who chose to leave the study after enrollment were defined as lost to follow-up.
Data collection
All CSTAR centers used the same protocol-directed methods to provide uniform evaluations and to record patient data. Investigators received training on diagnostic confirmation, disease activity evaluation, data input, and data quality control. The demographic data collected included gender, age at onset, age at diagnosis, age at enrollment, family history of rheumatic diseases, and reproductive history, as well as socioeconomic status, education and marital status. Systemic manifestations (e.g. neuropsychiatric SLE, vasculitis, arthritis, myositis, lupus nephritis, rash, oral ulceration, alopecia, pleuritis, pericarditis and fever) were assessed using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). All occurrences were classified according to SLEDAI definitions. Survival time was defined as the time from the date of diagnosis until death or last contact. Follow-up visits were conducted every three to four months, according to clinical practice. 10
Organ or system damage, defined as irreversible impairment, was recorded if the damage was persistent for at least six months. 11 Damage was assessed by the System Lupus International Collaborating Clinics/ACR Damage Index for Systemic Lupus Erythematosus (SDI) 12 at last visit and included medications (previous and current use). 13 According to the SDI, damage was assessed in 12 organ systems as follows: ocular (range 0–2), neuropsychiatric (0–6), renal (0–3), pulmonary (0–5), cardiovascular (0–6), peripheral vascular (0–5), gastrointestinal (0–6), musculoskeletal (0–7), skin (0–3), gonadal (0–1), endocrine (0–1) and malignancy (0–2), with a possible maximum total score of 47. 14 The follow-up period was identified as the time of disease onset to the time of death or last follow-up. Cause of death was determined by a review of case records and by discussion with the attending physicians. 15
Statistical analysis
Continuous data are expressed as mean ± SD. An independent sample t test was used to compare variables between the two groups. For non-normally distributed data, the Mann-Whitney U test was used. Categorical data are expressed as numbers or percentages. The chi-squared test or Fisher exact test was used to analyze the relationship between categorical variables. P values less than 0.05 indicated statistically significant results; values less than 0.1 were also reported. The Kaplan-Meier method was used for survival analysis. The Cox proportional hazard model was adopted to analyze predicting factors for mortality. Statistical analysis was carried out using SPSS 17.0 for Windows.
Results
Demographic and clinical characteristics of SLE patients
Demographic and clinical characteristics of SLE patients.
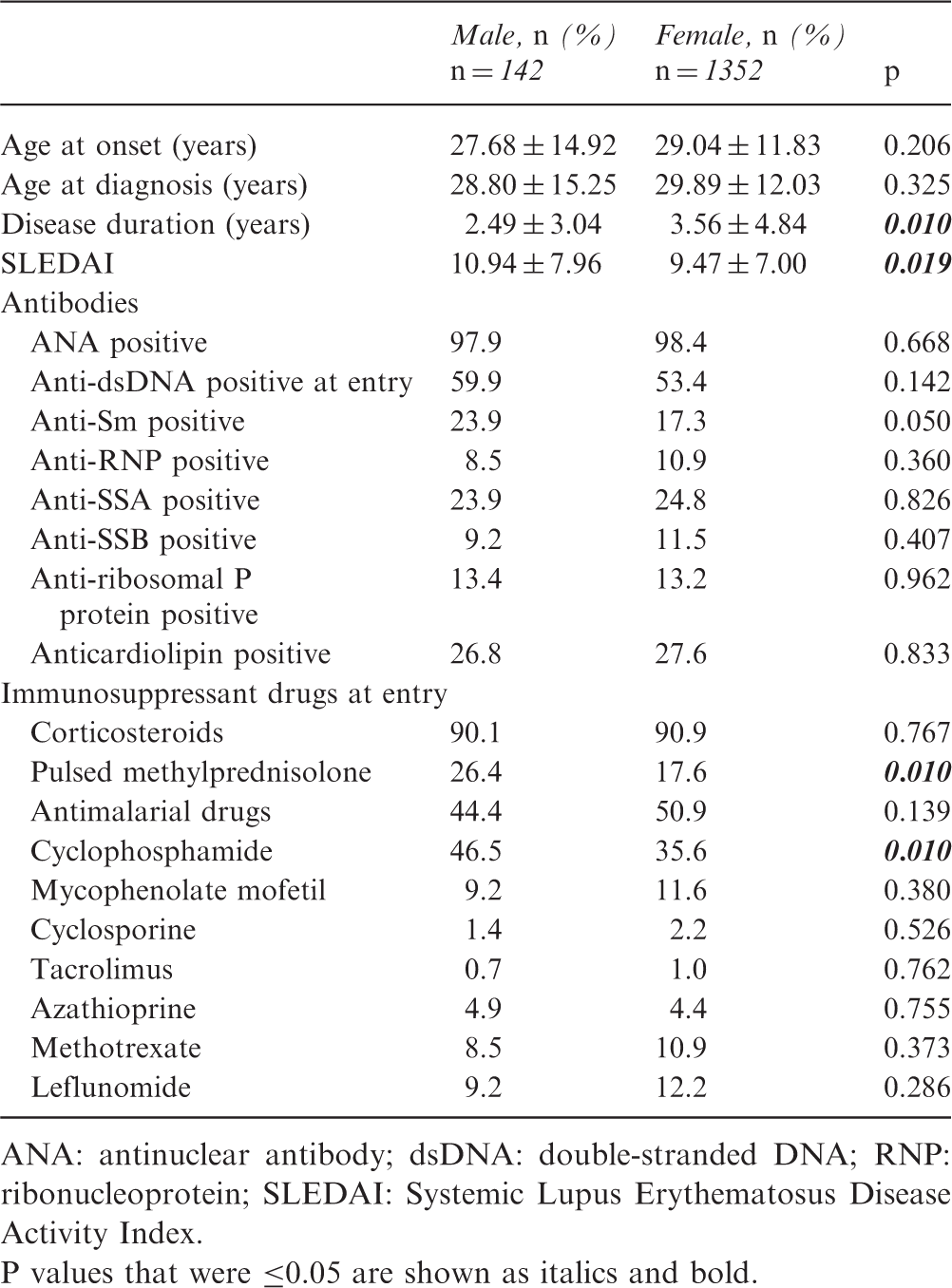
ANA: antinuclear antibody; dsDNA: double-stranded DNA; RNP: ribonucleoprotein; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index. P values that were ≤0.05 are shown as italics and bold.
P values that were ≤0.05 are shown as italics and bold.
Survival rate
Figure 1 shows the Kaplan-Meier survival plot of the cohort. The one-year survival rate was 97.8% in male patients and 99.1% in female patients, the three-year survival rate was 95.4% in male patients and 98.4% in female patients, and the five-year survival rate was 92.0% in male patients and 97.6% in female patients; these were significantly different (p = 0.019).
The survival rates of two genders in systemic lupus erythematosus patients for one, three and five years (y).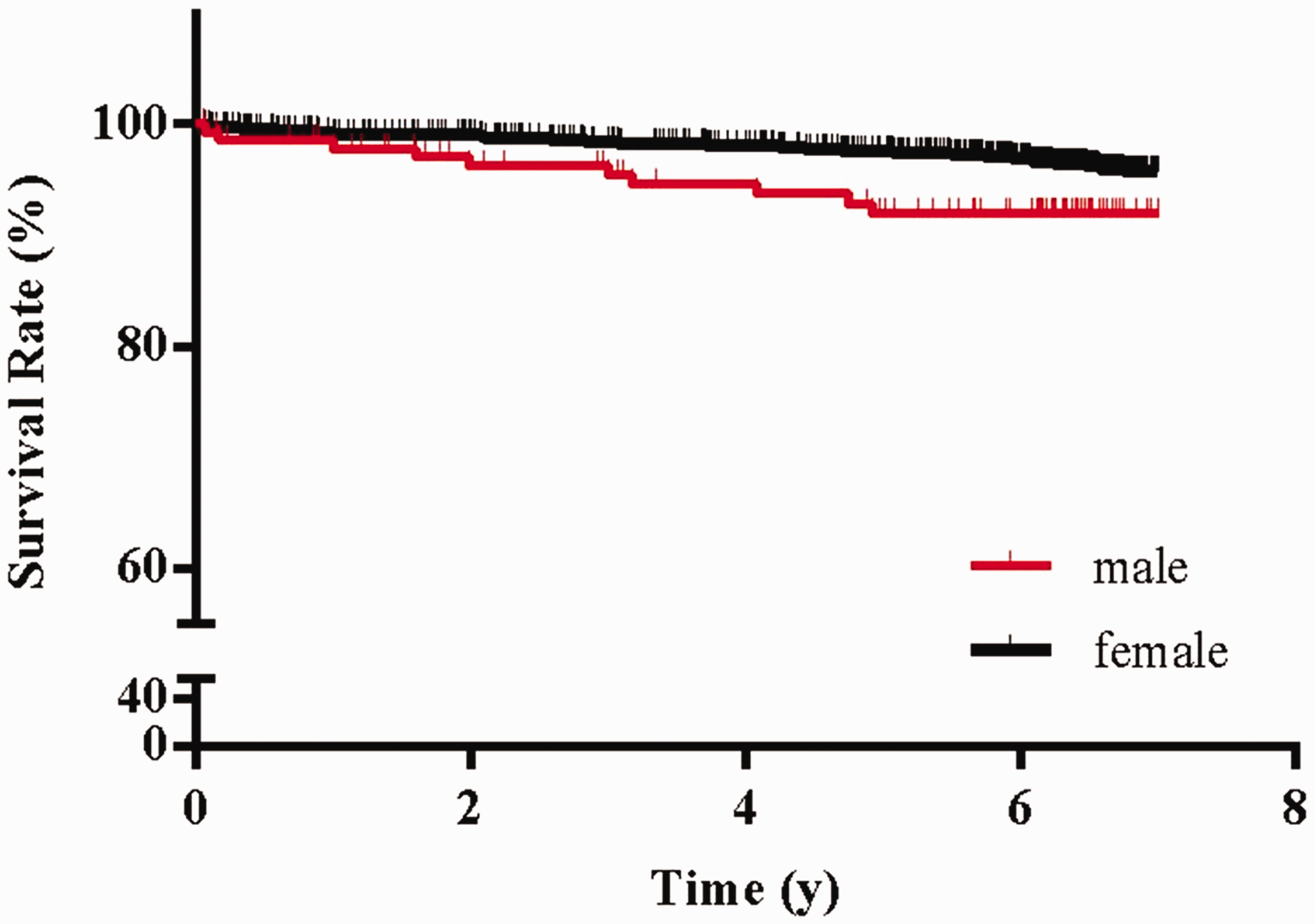
Mortality and causes of death
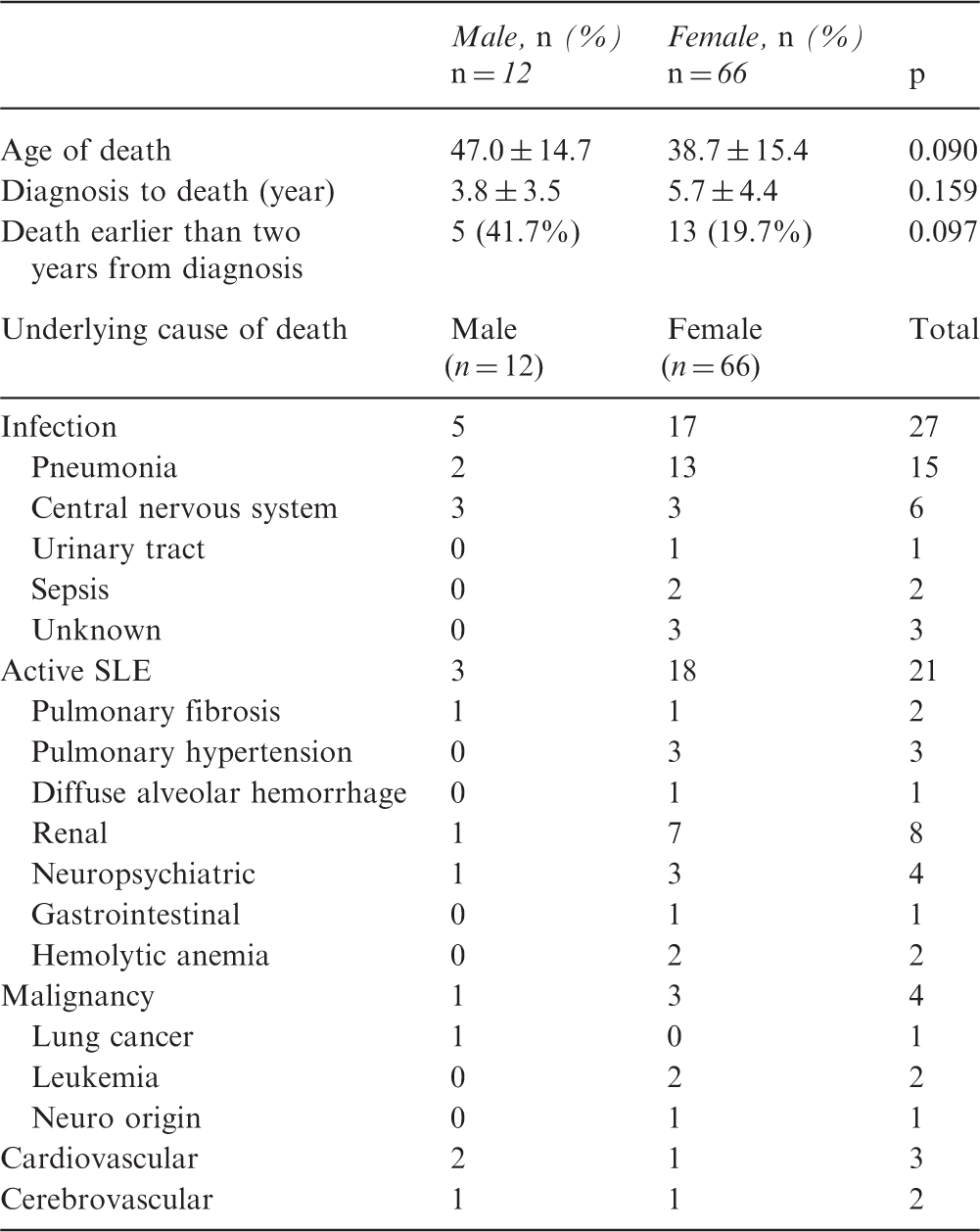
Underlying causes of death with gender distribution in patients with systemic lupus erythematosus (SLE) in China
Organ damage
SLICC/ACR Damage Index comparison between male and female patients with SLE (n = 1494)
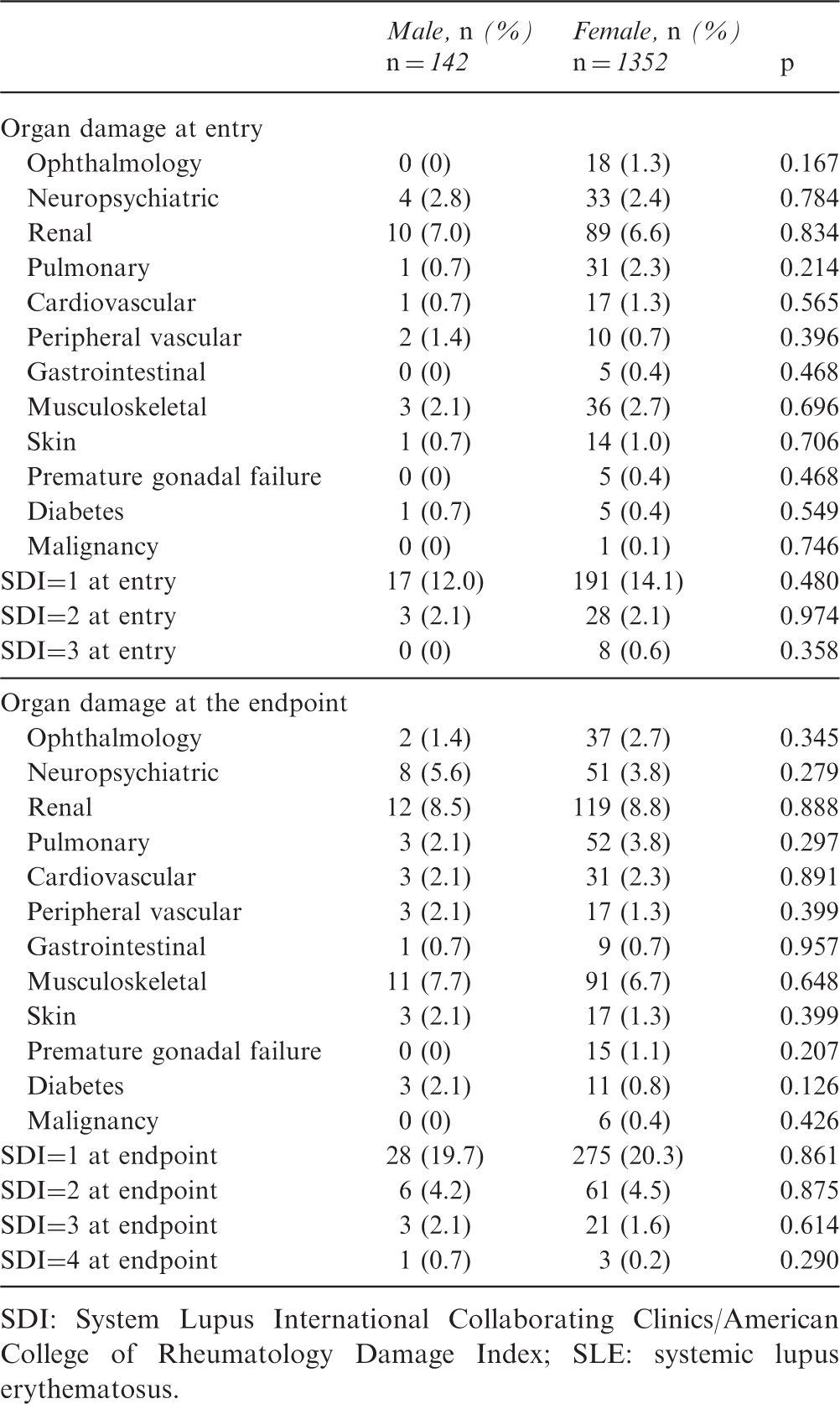
SDI: System Lupus International Collaborating Clinics/American College of Rheumatology Damage Index; SLE: systemic lupus erythematosus.
At the end of the study, 398 of 1494 (26.6%) SLE patients had chronic damage in at least one organ or system (SDI ≥ 1), including 38 male and 360 female patients, with a mean SD score of 1.32 ± 0.64 (range, 0–5). The score of female patients was 1.31 ± 0.62 and the score of male patients was 1.39 ± 0.76 (p = 0.438); 303 of 1494 patients (20.3%) had an SDI of 1, including 28 male patients (19.7%) and 275 female patients (20.3%); 67 of 1494 patients (4.6%) had an SDI of 2, including six male patients (4.2%) and 61 female patients (4.5%); 24/1494 patients (1.6%) had an SDI of 3, including three male patients (2.1%) and 21 female patients (1.6%); four of 1494 patients (0.3%) had an SDI of 4, including one male patient (0.7%) and three female patients (0.2%) (Table 3).
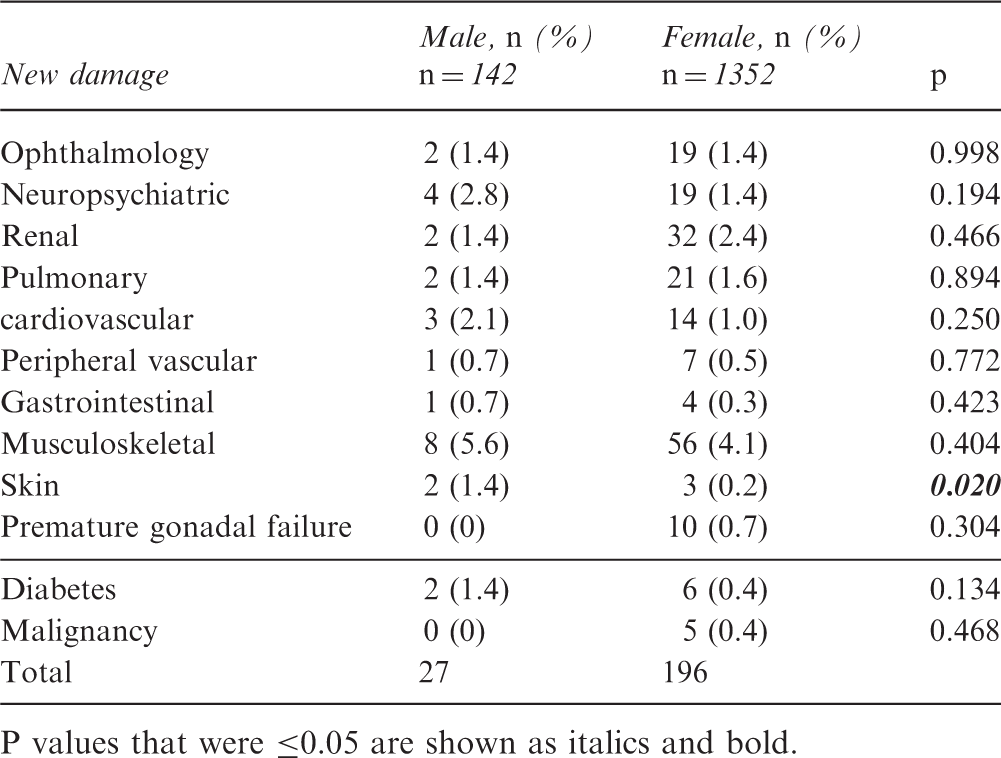
At the end of the study, the major accumulated organ damage included renal (8.5%), musculoskeletal (7.7%) and nervous system (5.6%) for men and renal (8.8%), musculoskeletal (6.7%), nervous system (3.8%) and pulmonary (3.8%) for women. Damage accrual was not significantly associated with gender. SDI item accrual during the follow-up period is summarized in Table 3. The total SDI increased from 1.19 ± 0.42 to 1.32 ± 0.64 across six years.
New damage comparison between male and female patients with SLE from entry to the endpoint
Discussion
To the best of our knowledge, this is the first Chinese study focused on the gender impact of long term-outcomes in a large cohort of SLE patients. Previous studies have reported five-year survival rates of more than 95% in some SLE patient cohorts.5,16–18 Our study showed that five-year survival rates for female patients were more than 95%; however, the rates for male patients did not reach that level, indicating that male patients have less-favorable outcomes than females. Many factors have been found to be related to the mortality of SLE, including gender, course of disease, onset of SLE after age 50 years, and the level of activity of disease.6,19
Male gender has previously been associated with a poorer prognosis,20–26 as in our study. Variables predicting early death (two years after diagnosis) include male gender, young age at diagnosis, and skin complications. 27 Our study also showed that male patients die sooner than female patients. The probable explanation for poorer prognosis and earlier death is that male patients often have more active disease with rapid progressive courses. 27 Previous studies have shown that renal disease, vasculitis, and neuropsychiatric lupus are more common in male SLE patients with higher SLEDAI scores compared with female SLE patients in China. 28 Higher mortality rates associated with worse renal outcomes are thought to occur in male patients since renal involvement in SLE is a major determinant of outcomes.24,25
Smoking is a well-known risk factor for the development of proteinuria and the progression of renal disease in the general population, especially in males.29,30 In SLE patients, studies have shown that smokers have significantly more nephropathy, microscopic hematuria, proteinuria, and higher SLEDAI scores than nonsmokers. 31 Xu et al. showed that the number of male SLE patients who smoke is nearly three times higher than female patients. 31 While the effect of gender on mortality in SLE is not entirely clear, a higher prevalence of male smokers with SLE may explain this poorer prognosis.
Our data showed that the main cause of death was infection in men and active SLE disease in women. Previous studies from China have shown that the presence of infection with disease flare was the main cause of death in lupus patients and an independent predictor for poor survival.32,33 Lu and colleagues found that the causes of death in SLE are usually similar across genders. 32 Another study found that, although the most common cause of death was cardiovascular disease in men and active SLE, infections and malignancies in female patients, there was no significant difference between groups. 33 Because our cohort had data for only six years, the cause of death can only indicate early death; thus, long-term damage from diseases, such as cardiovascular disease, requires longer-term data to evaluate. Because male patients have more organ involvements and higher SLEDAI scores than female patients, 28 rheumatologists would give them more aggressive immunosuppressive therapy. According to our study, the proportion of male patients treated with pulsed methylprednisolone and cyclophosphamide was significantly higher than that of female patients. Other research showed a similar result of more prevalent of cyclophosphamide use in men. 34 Strong immunosuppressive therapy would increase the risk of infections, so there would be a greater chance of acquiring infections; this could explain the high rates of infections in male patients.
According to SDI, our study found that renal damage was the most frequently involved system in both genders, followed by musculoskeletal and neuropsychiatric systems. The prevalence of renal damage in our result was similar to some other studies, which was approximately 8% to 14.5%. Meanwhile, one study showed the proportion of renal involvement was as high as 37.5%. 35 This difference may be due to different treatment protocols and various changes in renal histology. 36 Some investigators have reported musculoskeletal system and neuropsychiatric as the most involved systems.10,36 Damage accrual varies among ethnic groups, and damage in different systems does not follow a common pattern in SLE patients.37–40
The prevalence of eye damage was lower in our cohort of patients in contrast to other studies, which reported them to be more than 5%.10,36 In our study, ophthalmology examinations were not routine items for follow-up. It is possible that patients without obvious eye symptoms might not visit an ophthalmologist, which could explain why the rate of eye involvement is low.
The five-year survival of SLE patients has significantly improved from the 50% reported in the 1950s to currently more than 90%.4,41,42 Increased survival of SLE patients implies the accrual of cumulative organ damage, while adverse events of treatment, disease activity and comorbidities represent major risk factors.43,44 Some previous studies have indicated that men are more likely than women to experience organ damage, including neuropsychiatric, renal, cardiovascular, peripheral vascular disease and myocardial infarction. 45 However, unlike some other studies, 46 we could not conclude that male patients had much more organ damage than female patients. Some researchers obtained the same results as we did, indicating that gender is not a definite predictor of damage.47–49 One possible explanation is that certain characteristics included in damage scores appear more frequently in women. 36
This study has limitations. First, this study had a short follow-up. Longer-term studies are needed to investigate late mortality and organ damage in SLE patients. In addition, it remains to be determined whether disease relapses are risk factors for mortality.
In summary, male SLE patients had lower survival rates than female patients. Male patients received more methylprednisolone pulse and cyclophosphamide therapy. The most common causes of death were infection for male patients and active SLE disease for female patients. The major accumulated organ damages were renal, musculoskeletal, and nervous system both for male and female SLE patients in China.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Chinese National Key Technology R&D Program, Ministry of Science and Technology (2017YFC0907601, 2017YFC0907602, 2017YFC0907603), and the Chinese National High Technology Research and Development Program, Ministry of Science and Technology (2012AA02A513).