
Abstract
Objectives
Hydroxychloroquine (HCQ) is a key therapy in systemic lupus erythematosus (SLE). Medication non-adherence is reported in up to 80% of lupus patients and results in increased morbidity, mortality, and health care utilization. HCQ levels are a sensitive and reliable method to assess medication adherence. Our study evaluated the role of HCQ level measurement in routine clinical care and its association with disease activity in a predominantly Hispanic population.
Methods
SLE patients from the Columbia University Lupus cohort treated with HCQ for ≥ 6 months and reporting medication adherence were included. HCQ levels were measured by whole blood high performance liquid chromatography. Non-adherence was defined as an HCQ level <500 ng/ml. The association between HCQ levels and disease activity measured by Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) was evaluated.
Results
One hundred and eight patients were enrolled; the median age was 38 years, 91% were female, and 63% were Hispanic. The median SLEDAI-2K was 4.3 (0–20). Forty-one percent of patients had an HCQ level <500 ng/ml consistent with non-adherence, of which 19% had undetectable levels. A higher SLEDAI-2K score was associated with low HCQ levels (p = 0.003). This association remained significant after adjusting for depression (p = 0.0007).
Conclusion
HCQ levels < 500 ng/ml were associated with higher disease activity and accounted for 32% of the SLEDAI-2K variability. HCQ blood measurement is a simple and reliable method to evaluate medication adherence in SLE. Reasons for non-adherence (levels < 500 ng/ml) should be further explored and addressed.
Introduction
Hydroxychloroquine (HCQ) is the cornerstone of treatment in systemic lupus erythematosus (SLE). Its numerous benefits include prevention of flares, 1 prolonged survival,2,3 decreased incidence and severity of organ involvement, 4 lower damage accrual, 5 decreased thrombotic events,6,7 improvement in lipid profiles, 8 and decreased insulin resistance in pre-diabetics. 9 Adherence to medication is an important predictor of outcomes in chronic diseases. 10 In SLE, adherence is estimated to be as low as 20%11–14 and is associated with increased healthcare service utilization (increased outpatient and emergency department visits, as well as hospitalizations), 15 and increased renal involvement (nephrotic syndrome, renal insufficiency, or renal failure). 16
Interpreting adherence data in SLE remains challenging given the variability in the evaluation methods. Several studies utilize adherence monitoring approaches with poor feasibility in clinical practice (pharmacy calls, electronic pill bottle monitoring),13,14 or low accuracy (physician global assessment of compliance, patient report of compliance in clinic or by questionnaire).17,18 Costedoat-Chalumeau et al. suggested using blood levels to monitor HCQ adherence in SLE and described an association between low HCQ levels and higher disease activity, with lower levels predicting flares in the subsequent 6 month period. 19 Durcan et al. identified a similar inverse correlation between higher disease activity and low HCQ levels, 20 and Frances et al. demonstrated that discoid lupus patients in remission had significantly higher levels of HCQ compared with those with active disease. 21 Yet, these studies included few, if any, Hispanic subjects. Our study was undertaken to evaluate the role of monitoring HCQ levels in an urban, multiethnic, predominantly Hispanic cohort and determine its association with SLE disease activity measured by Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K). 22
Methods
Patients
One hundred and eight SLE patients treated with HCQ for ≥ 6 months, evaluated at the Columbia University Lupus Center between January 2016 and June 2017 were included. All patients were ≥18 years of age, met the 1997 revised American College of Rheumatology classification criteria, 23 and self-reported adherence to HCQ. Informed consent was obtained for all patients enrolled. The study was approved by the Columbia University Institutional Review Board (IRB-AAAQ4765).
Outcome measures
SLE disease activity was calculated using the SLEDAI-2K at the time of HCQ measurement. 22
Main predictor
HCQ testing was done by high performance liquid chromatography on whole blood by Exagen Laboratory (https://www.exagen.com/products/avise-hcq/). Adherence was defined as a HCQ level ≥500 ng/ml based on prior studies showing an acceptable precision over levels 15.7–2000 ng/ml, and the therapeutic cutoff at this level suggested by US cohorts' data. 20
Covariates
Information on demographics, socio-economic status, and smoking was collected by standardized health questionnaires and patient interviews. SLE disease duration was defined as the number of years starting from the date of physician diagnosis. Clinical symptoms, laboratory data, current medications, weight, height, SLE organ involvement, and depression diagnosis were ascertained via patient interview and examination at the time of the visit. Health literacy was assessed in English or Spanish using the validated Pfizer Health Literacy Questionnaire (HLQ), “Newest Vital Sign.” 24 Limited health literacy was defined as an HLQ score of 0–3, and adequate health literacy as a score of 4–6. Damage accrual was determined by the calculation of the Systemic Lupus International Collaborating Clinics damage index (SDI). 25
Statistical analysis
Patient characteristics
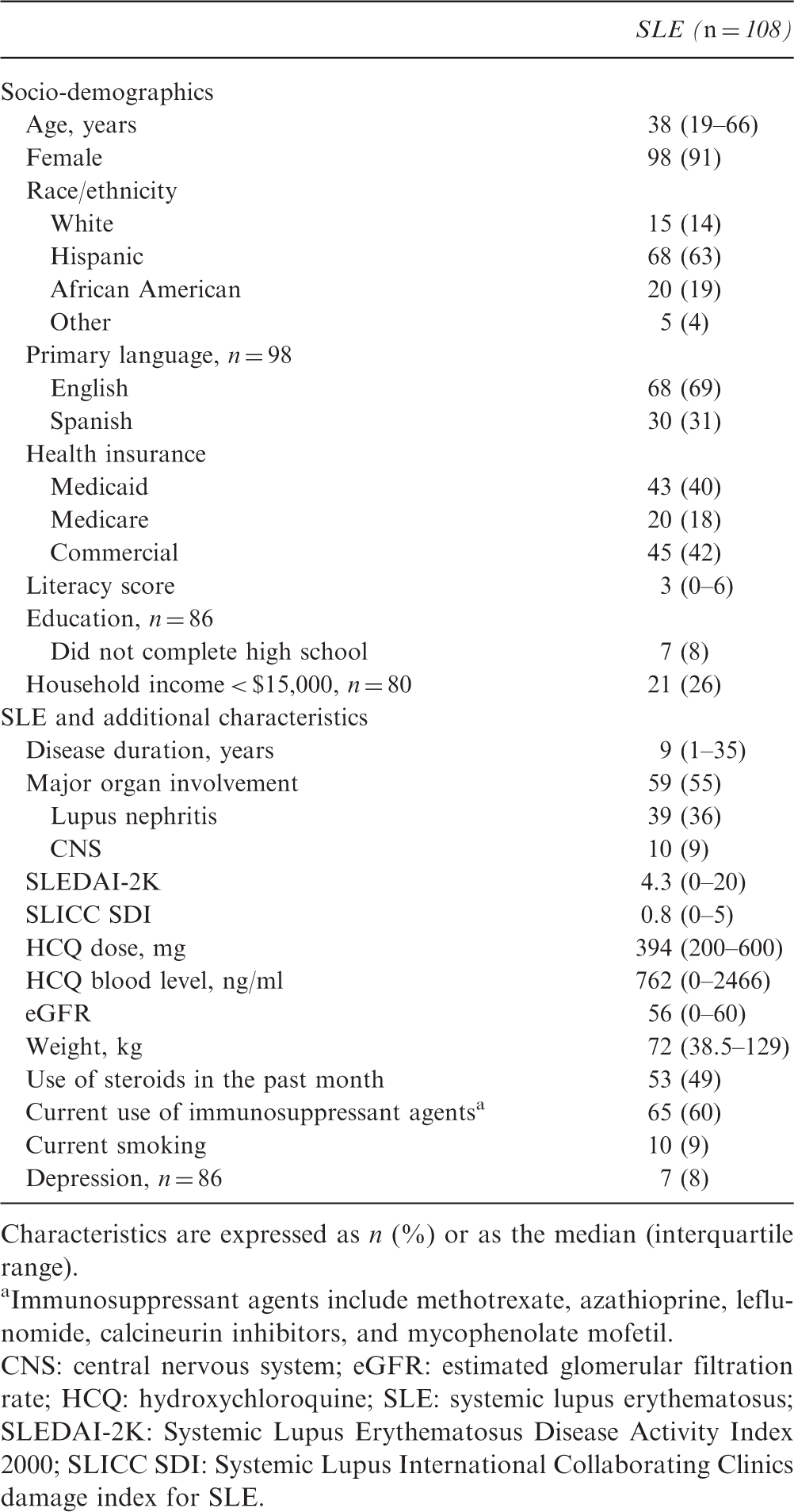
Characteristics are expressed as n (%) or as the median (interquartile range).
Immunosuppressant agents include methotrexate, azathioprine, leflunomide, calcineurin inhibitors, and mycophenolate mofetil.
CNS: central nervous system; eGFR: estimated glomerular filtration rate; HCQ: hydroxychloroquine; SLE: systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; SLICC SDI: Systemic Lupus International Collaborating Clinics damage index for SLE.
Results
Patient characteristics
The characteristics of the study participants are summarized in Table 1. Ninety-one percent of the patients were female; 63% were Hispanic, 19% African American, 14% white, and 4% from other race/ethnicity. The median age was 38 years; 69% reported English as their primary language. The median SLEDAI-2K was 4.3 and the median SDI score was 0.8. SLE had been complicated by major organ involvement in 55% of patients. Almost half of the patients had been treated with steroids in the month prior to the study and 60% were on current immunosuppression. Twenty-one patients were below the poverty level (annual household income < $15,000); 7 had not completed high school (Table 1).
Patient characteristics by HCQ status
Patient characteristics by adherence status
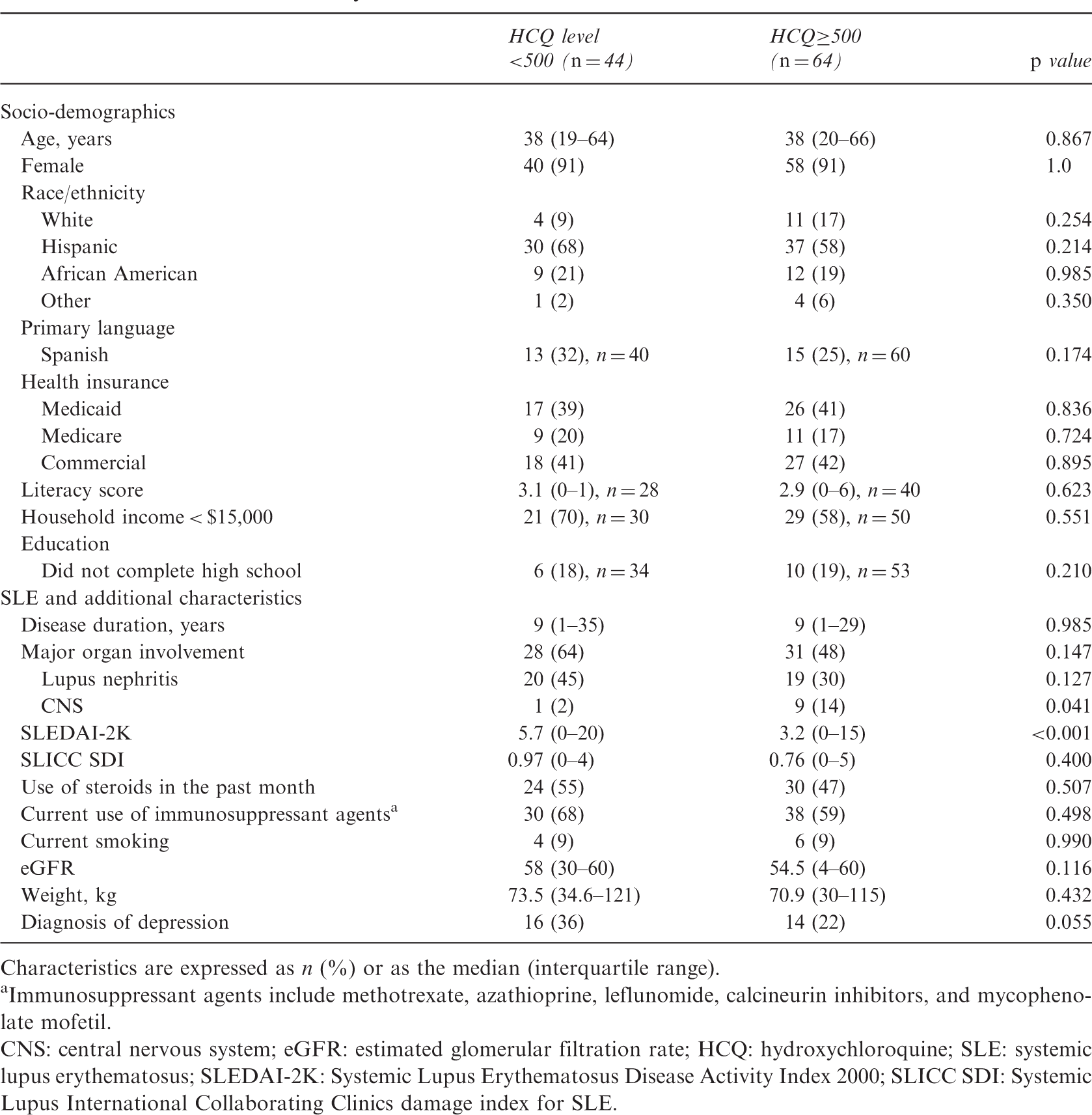
Characteristics are expressed as n (%) or as the median (interquartile range).
Immunosuppressant agents include methotrexate, azathioprine, leflunomide, calcineurin inhibitors, and mycophenolate mofetil.
CNS: central nervous system; eGFR: estimated glomerular filtration rate; HCQ: hydroxychloroquine; SLE: systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; SLICC SDI: Systemic Lupus International Collaborating Clinics damage index for SLE.
Disease activity and chronicity by HCQ status
HCQ non-adherent SLE patients had a higher SLEDAI-2K score compared with adherent patients: 5.7 versus 3.2, p < 0.001. After log transformation of the outcome, the mean was 1.62 (95% confidence interval (CI) 1.37–1.87) versus 1.13 (95% CI 0.92–1.34) respectively; p = 0.003. While no confounders were identified, a diagnosis of depression was close to meeting statistical significance in its association with HCQ adherence (p = 0.055). After adjusting for depression, the association between HCQ adherence and the SLEDAI-2K remained statistically significant: mean of 1.56 (95% CI 1.31–1.80) versus 0.99 (95% CI 0.77–1.22) respectively; p = 0.0007, with HCQ levels explaining 32% of the SLEDAI-2K variability. No interaction was identified between depression and HCQ levels (p = 0.574 for the interaction term). Among patients with depression, the mean log transformed SLEDAI-2K was 1.38 (95% CI 0.96–1.79) versus 0.68 (95% CI 0.24–1.12) in non-adherent versus adherent patients, respectively; p = 0.026. In those without depression, the mean was 1.76 (95% CI 1.46–2.07) and 1.26 (95% CI 1.3–1.49) in the non-adherent and adherent subjects, respectively; p = 0.010. The SDI was 0.97 in non-adherent patients compared with 0.76 in adherent subjects (not statistically significant) (Table 2).
Discussion
This study supports the utility of HCQ blood measurements to assess medication adherence in SLE patients. Key findings of the study are that, in this predominantly Hispanic cohort, HCQ levels <500 ng/ml were associated with higher disease activity measured by SLEDAI-2K and accounted for 32% of its variability.
Given its numerous clinical and survival benefits,1–10 HCQ remains the cornerstone of treatment in SLE. However, medication adherence has been reported to be as low as 20–30% in lupus patients,11–14 and results in increased healthcare service utilization, morbidity, and mortality.15,16 Moreover, most studies measuring medication adherence in SLE utilize less accurate methods.13,14,17,18 In recent years, HCQ blood levels were proposed as an objective and reliable tool for measuring medication adherence in clinical practices in SLE patients.
Costedoat-Chalumeau et al. described that over 6 months of follow-up, lupus patients who flared had lower baseline HCQ concentrations (703 ± 534 ng/ml versus 1128 ± 507 ng/ml). 26 Importantly, in multivariable modeling, baseline blood HCQ levels were the only independent predictor of subsequent SLE flares (this was true for two different flare definitions: SLEDAI > 6 and >4). For an increase in blood HCQ of 1 SD (≈500 ng/ml), the risk of subsequent flare decreased by 60%. Based on these data, we defined non-adherence/low HCQ levels as <500 ng/ml. However, the best cutoff HCQ level to define non-adherence remains unclear, and concentrations <200 ng/ml have been proposed by some. 27 Moreover, Durcan et al. suggested an inverse relationship between SLEDAI scores and HCQ levels but their finding did not reach statistical significance. 20 Our study now confirms this association in a predominantly Hispanic cohort.
While statistical significance was not reached, non-adherent lupus patients in our study were predominantly Hispanic and African American, and adherent patients were more likely to be white. These findings are similar to those by Feldman et al. 15 in which prescription refill data identified the increased odds of non-adherence in black people and Hispanics compared with white people. Our data provide additional evidence for the relative ease of use of HCQ blood levels.
Similar to the findings of Durcan et al., education and income did not predict differences in adherence. Interestingly, health literacy did not have a significant effect on adherence and HCQ blood levels. These findings suggest that variables other than socio-economic status and literacy contribute to adherence in lupus patients.
In our study, an underlying diagnosis of depression had a trend towards association with non-adherence, emphasizing the importance of optimizing the physician–patient relationship, screening and treating depression as potential tools to improve adherence and the overall health of lupus patients. Surprisingly, patients with a history of CNS involvement were more likely to be adherent. While the reason for this association remains unclear, it is tempting to speculate that the severity of CNS disease in SLE prompts patients to improve adherence to therapeutic regimens.
Based on the findings of the current study and the one by Durcan et al., we propose that a range of 500–2000 ng/ml should be considered as adherent and therapeutic in multiethnic and multiracial cohorts. However, Costedoat-Chalumeau et al. used a cutoff of 1000 ng/ml to determine adherence, hence differences in pharmacokinetics and pharmacodynamics of genetically different patient populations should be further investigated. 19
Strengths of our data include the use of a reliable measurement of medication adherence by calculation of blood drug levels and the evaluation of this method in a predominantly Hispanic cohort. This allowed us to study the independent contribution of HCQ blood levels to SLE disease activity in this patient population.
Limitations of our study include its cross-sectional nature, which precludes establishment of causation for our findings, and the evaluation of whether changes in the SLE disease activity score parallel changes in HCQ levels. Furthermore, a lack of longitudinal follow-up data prevents a substantial assessment of damage accrual that showed a higher numerical value in non-adherent versus adherent patients.
In conclusion, HCQ levels <500 ng/ml were independently associated with higher SLE disease activity scores in a predominantly Hispanic cohort, and accounted for 32% of the SLEDAI-2K variability. These findings support the measurement of blood HCQ levels to monitor medication adherence in lupus patients.
Supplemental Material
Supplemental material for Association between hydroxychloroquine levels and disease activity in a predominantly Hispanic systemic lupus erythematosus cohort
Supplemental Material for Association between hydroxychloroquine levels and disease activity in a predominantly Hispanic systemic lupus erythematosus cohort by L Geraldino-Pardilla, A Perel-Winkler, J Miceli, K Neville, G Danias, S Nguyen, T Dervieux, T Kapoor, J Giles and A Askanase in Lupus
Footnotes
Acknowledgements
The authors thank the patients of the Columbia University Lupus Center for their participation in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.