
Abstract
Background
Few data are available about the rate of short-term remission and its impact on the long-term outcomes of proliferative lupus nephritis in the Middle East.
Methods
An observational study was carried out involving 96 adult patients with biopsy-proven focal or diffuse proliferative lupus nephritis (PLN) from four different hospitals. Data on induction, remission and long-term outcomes were collected and analyzed.
Results
Among the 96 patients with biopsy-proven PLN (median age 27 (IQR: 21,34) years, 85% women and median duration of systemic lupus erythematosus (SLE) prior to diagnosis 27 (IQR: 11, 55) months), 67% developed remission at 6 months (proportion 0.67; 95% CI 0.57, 0.76). Mycophenolate mofetil (MMF) was used in 45/96 (47%), CYC in 41/95 (43%) and other agents in 10/96 (10%). The choice of MMF as induction agent has increased in recent years. Among baseline characteristics, only histologic activity was found to have a significant association with remission, with active lesions more likely to remit than active/chronic and chronic lesions (AOR 6.5, 95% CI 1.44–29.39, p = 0.015). Based on Kaplan–Meier analysis, the 5-year renal survival rate without doubling serum creatinine was 73.8%. Compared to patients with complete remission, lower long-term renal survival rates were observed in patients with no remission (89.7 versus 43%, p = 0.001) and partial remission (89.7 versus 77.6%, p = 0.256). The cumulative rate of doubling serum creatinine, dialysis, relapse and death was 23%, 11%, 10% and 5%, respectively, at 48-month median follow up.
Conclusion
Approximately two-thirds of patients with PLN develop remission in response to standard induction therapy. Remission was negatively associated with the presence of chronic changes in renal biopsy. Overall, MMF is the most commonly used agent to induce remission; however, with more severe disease CYC, is used more frequently. PLN is associated with significant long-term renal outcomes including a 26% cumulative rate of doubling of serum creatinine at 5 years. Initial remission predicts this long-term renal survival.
Introduction
The frequency of renal involvement in patients with systemic lupus erythematosus (SLE) varies based on differences in geographical area and ethnic background. 1 A higher frequency has been reported in blacks with an earlier presentation and a worse outcome in blacks and Hispanics.2-5 The reported rate of renal involvement is 27.9% from the European population 6 compared to a wide range of rates reported from several Asian countries (18-100%), but is mostly over 50%. 7 In Saudi Arabia, a rate of 48% to 60% is reported.8-12 Histologically, several classes of lupus nephritis (LN) with prognostic and therapeutic implications are described13-15 with class IV being the most predominant class. 16
Proliferative lupus nephritis (PLN) encompasses focal and diffuse disease and is associated with increased mortality and decreased long-term renal survival. Therefore, aggressive treatment is suggested for PLN. It tends to have a more favorable response and long-term outcomes in Caucasians as compared to more ethnically diverse US and Asian populations.1,3,17,18 Less is known about the Middle East population, particularly in the era of mycophenolate mofetil (MMF) use as induction agent. Achievement of complete remission in the short term correlates with better long-term renal outcomes.17,19-26 However, only a few studies have looked at the value of partial remission with regard to long-term outcomes.17,27,28 We aim in this study to examine the rate of short-term remission (6 months) to standard of care induction treatments, and study its predictors and effect on long-term renal outcomes in Saudi patients with PLN.
Materials and methods
Study population
Adults (age
Design and procedures
We conducted a retrospective observational study on adult patients with biopsy-proven PLN from four medical institutions in Saudi Arabia. Information was collected on clinical presentation, pathological findings, choice of induction treatment, remission and long-term clinical outcomes.
Measurements and outcomes
The primary outcome measure was the remission rate of biopsy-proven PLN at 6 months of induction therapy. The secondary outcome measures were to describe the patterns of presentation, identify predictors of remission, describe the pattern of practice with regards to the choice of induction treatment (CYC vs. MMF vs. others) and estimate the rate of long-term outcomes including doubling of serum creatinine, relapse, dialysis and mortality. The potential determinants of response to induction treatment included the baseline patient and disease characteristics and the choice of induction treatment.
We defined complete remission (CR) as normalization of renal function or 50% reduction in serum creatinine from baseline level and reduction of 24-hour protein collection to less than 0.5 g (uPCR < 0.5 g/g). Partial remission (PR) requires 50% reduction in proteinuria, and urine protein < 3 g/24 hours (uPCR < 3 g/g) and/or less than 25% reduction in serum creatinine from baseline level.29-33 No remission (NR) was defined as criteria fulfilling neither CR nor PR. Relapse was defined as an increase in urine protein by more than 2 g/day from a stable baseline, referred to throughout as proteinuric relapse. 34 For the purpose of analysis in this research, a patient is said to have received certain induction if he or she did so for a minimum of 3 consecutive months. For the purpose of this study, remission is defined at 6 months, to avoid excluding patients with no data beyond that period.
Sample size and statistical analysis
A sample of 103 patients with biopsy-proven PLN was obtained from across four tertiary hospitals. Seven patients were excluded (four due to lack of information on induction therapy, two due to lack of data on remission, and one died before initiation of induction treatment due to severe multisystem disease). We estimated the proportion (with 95% confidence limits) of patients who achieved remission. We tabulated descriptive statistics by count or percentage for categorical variables and either mean (SD) or median (IQR) for continuous data. For predictors of remission, we used univariable and multivariable analyses.
For long-term outcomes, we estimated the time to composite renal outcomes (dialysis, relapse and doubling serum creatinine) and death. Time to event analysis was performed to assess survival without doubling serum creatinine in the entire cohort and in relation to the remission status.
Throughout our analysis, we judged a p value of less than 0.05 significant. We did all statistical analyses using SPSS version 24 (IBM Corporation).
Results
Patients
Baseline clinical characteristics
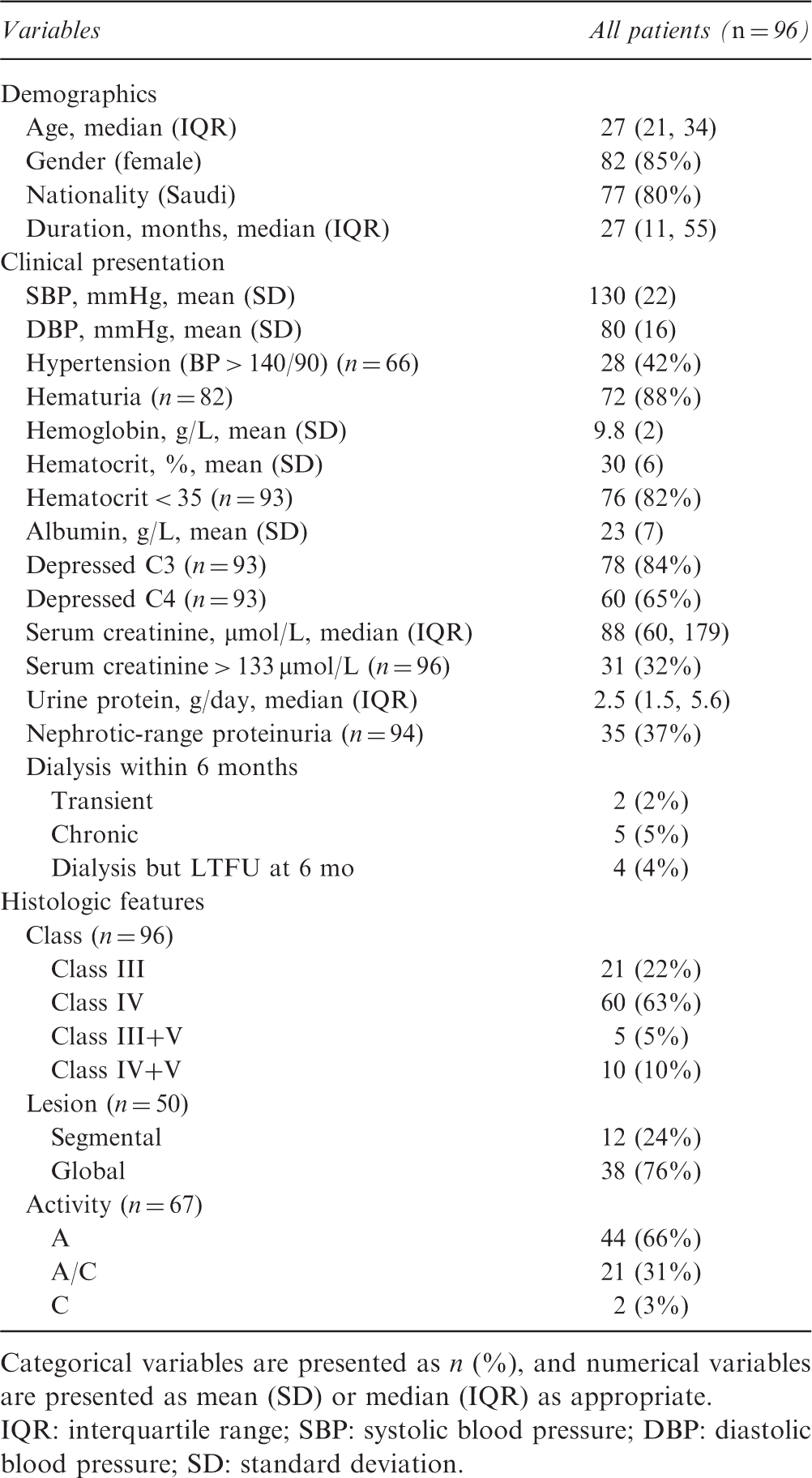
Categorical variables are presented as n (%), and numerical variables are presented as mean (SD) or median (IQR) as appropriate.
IQR: interquartile range; SBP: systolic blood pressure; DBP: diastolic blood pressure; SD: standard deviation.
At presentation of proliferative lupus nephritis (PLN), 31 patients (32%) had elevated serum creatinine > 133 µmol/L, and 35 patients (37%) had nephrotic-range proteinuria. Hypertension (blood pressure (BP) > 140/90) was evident at presentation in 28/66 patients (42%). C3 and C4 levels were depressed in 85% and 65% of patients respectively. Anemia was common with a hematocrit below 35% in 76/93 patients (82%).
The biopsy diagnoses revealed class IV as the most predominant diagnosis in 60 patients (63%). The type of proliferative lesion was reported in 50 samples, with global lesions reported more frequently (n = 38 patients; 76%). Activity was described in 76 biopsies with the majority having active (n = 44 patients; 66%) and active/chronic lesions (n = 21 patients; 31%) (see Table 1). For class IV disease, global lesions were reported more commonly (n = 28/35, 80%) than segmental lesions, and the majority were active lesions (n = 28/40, 70%).
Pattern of practice with induction treatment
Induction treatment by disease severity
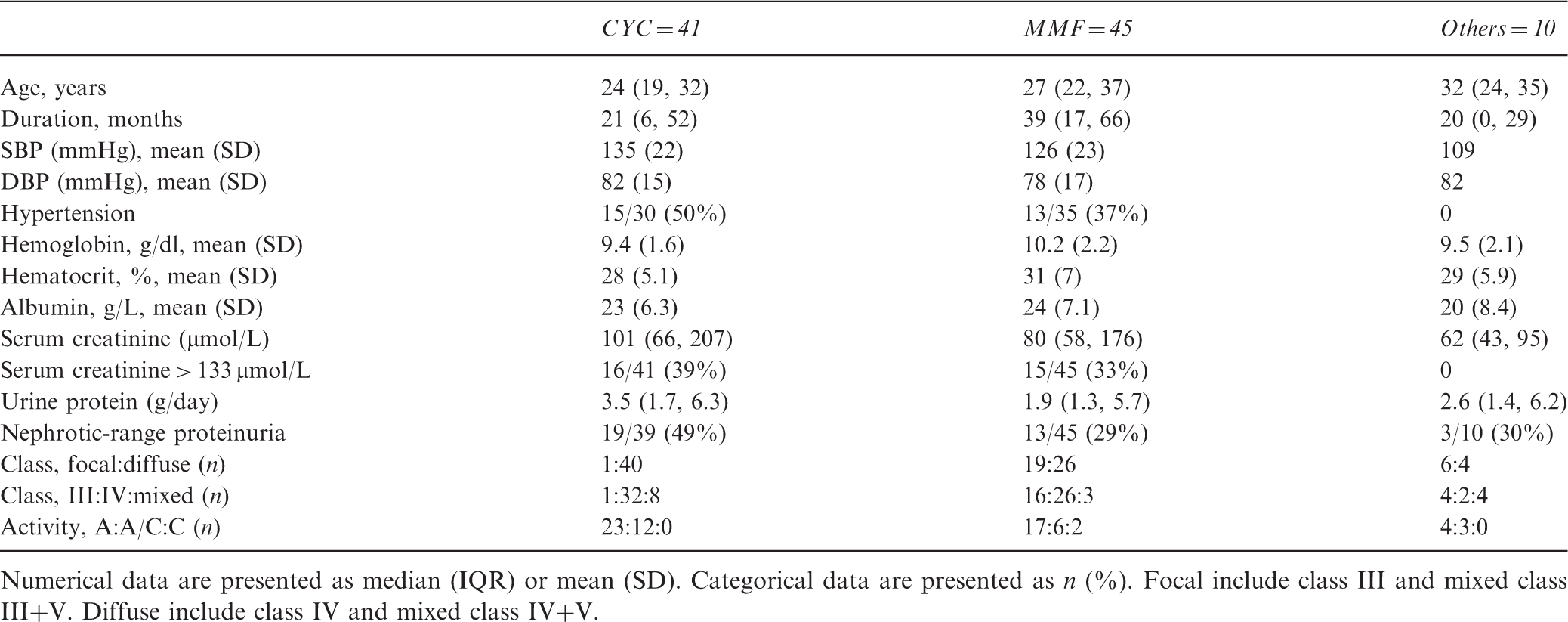
Numerical data are presented as median (IQR) or mean (SD). Categorical data are presented as n (%). Focal include class III and mixed class III+V. Diffuse include class IV and mixed class IV+V.
Regarding the temporal change in the pattern of practice for which induction treatment to choose for PLN, MMF use as first line increases over time from 42% for the period up to 2012 to 58% for the period beyond 2012; while the use of CYC had dropped from 45% to 39%; and other agents, namely azathioprine and CnI, dropped from 14% to 3%. The severity of presentation at diagnosis was different for the two time periods. Compared to the earlier period, the median urine protein level was lower in patients diagnosed beyond year 2012, being 2 g/day (IQR: 1, 3.7) versus 3 g/day (IQR: 1.7, 6.5) (p = 0.038 by Mann–Whitney U-test). The median serum creatinine level was numerically lower for patients diagnosed beyond year 2012, being 66 µmol/L (IQR: 53, 143) versus 95 µmol/L (IQR: 62, 164) (p = 0.169).
Remission rate
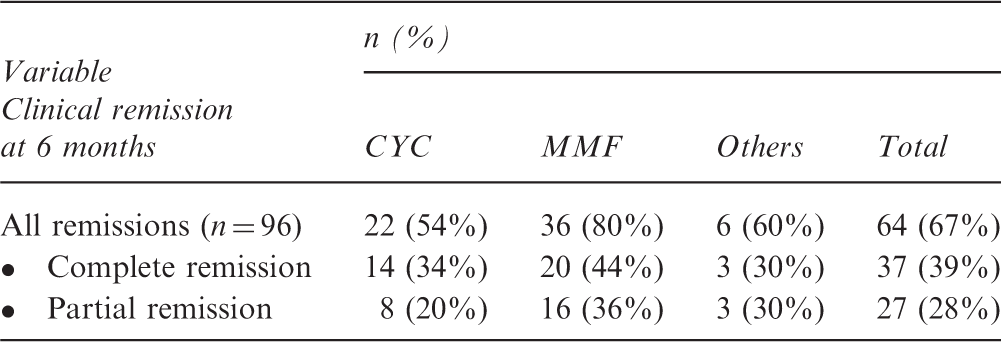
Rates of remission in patients treated for proliferative LN (n = 96)
Univariable and multivariable analyses for remission in patients treated with CYC or MMF induction for PLN (n = 86)
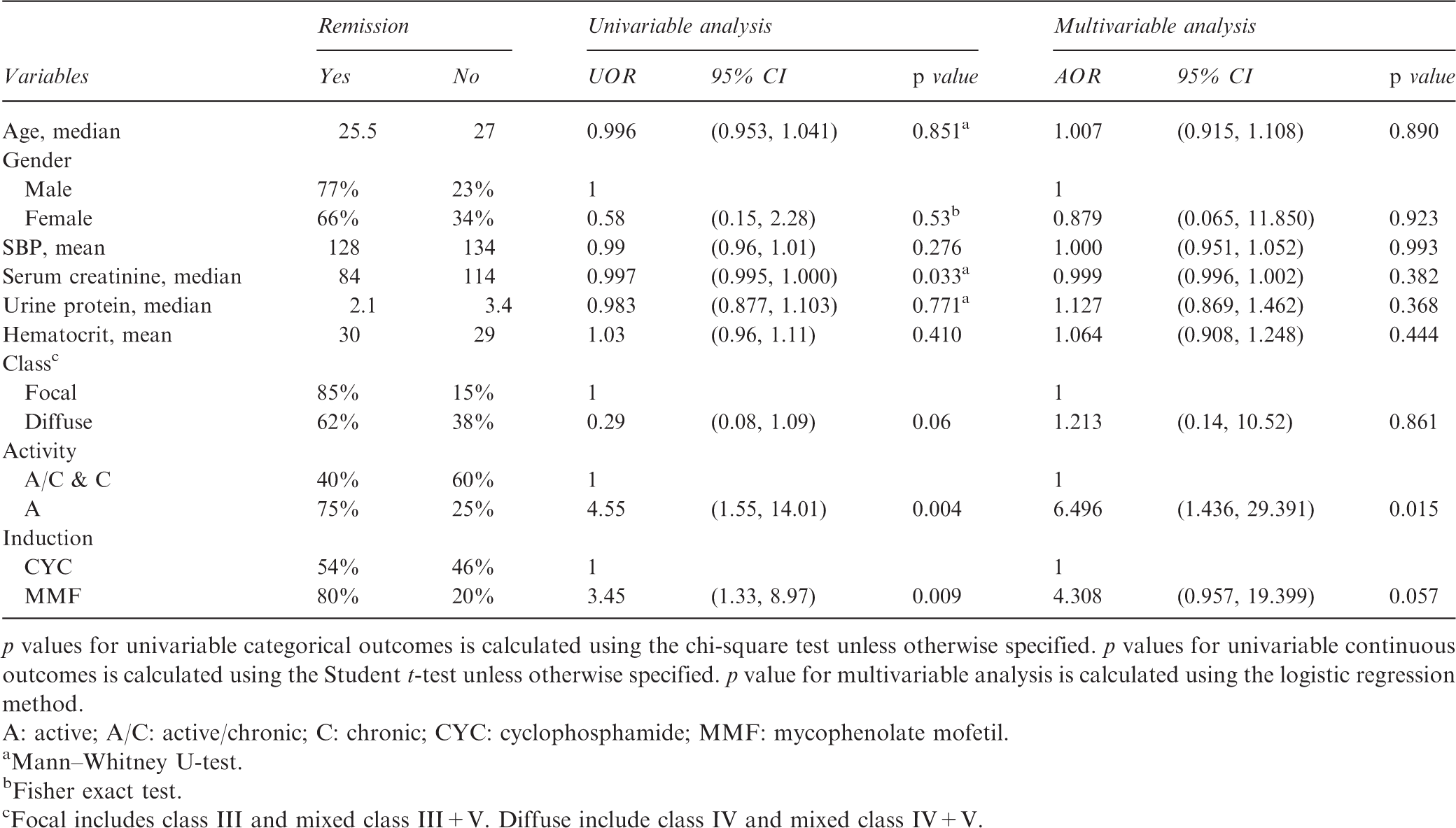
p values for univariable categorical outcomes is calculated using the chi-square test unless otherwise specified. p values for univariable continuous outcomes is calculated using the Student t-test unless otherwise specified. p value for multivariable analysis is calculated using the logistic regression method.
A: active; A/C: active/chronic; C: chronic; CYC: cyclophosphamide; MMF: mycophenolate mofetil.
aMann–Whitney U-test.
bFisher exact test.
cFocal includes class III and mixed class III+V. Diffuse include class IV and mixed class IV+V.
Long-term outcomes
At median follow up of 48 months (IQR: 24, 72) 91 patients were still alive (91/96, 95%), 77 patients with functioning kidneys (77/91, 84%). Eleven (11) patients required dialysis within 6 months, five were long-term, two were transient and four were lost to follow up by 6 months. Beyond 6 months, long-term dialysis was initiated in 10/87 (11%), proteinuric relapse developed in 9/87 (10%) and serum creatinine doubled in 20/78 (23%) of patients at median follow up of 48 months (IQR: 24, 72). The total number of patients lost to follow up was 21/96 (22%).
Comparison of long-term outcomes based on 6-month remission status
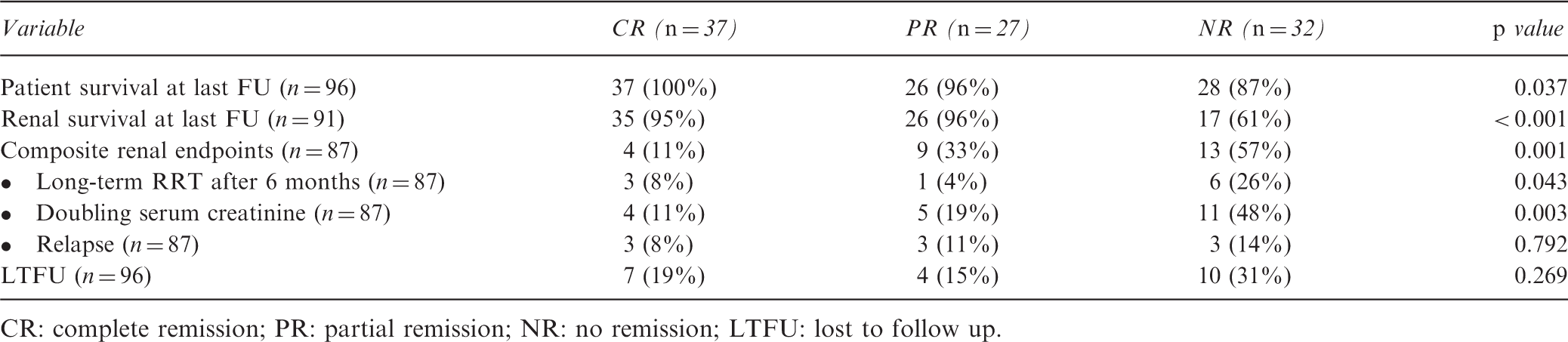
CR: complete remission; PR: partial remission; NR: no remission; LTFU: lost to follow up.
The cumulative rate of renal survival without doubling serum creatinine at 5 years is 73.8% for all PLN. Attaining remission is associated with better renal survival without doubling serum creatinine (p = 0.013; see Figure 1). There was no statistically significant difference in renal survival between patients who achieved CR and those who achieved PR (p = 0.258). However, the difference is statistically significant when patients with CR were compared to those with NR (p = 0.001). The cumulative rate of survival without doubling serum creatinine at 5 years is 89.7% for CR, 77.6% for PR and 42.5% for NR.
Survival without doubling serum creatinine according to response to induction treatment. Overall p value is 0.003. The p value for between groups difference in survival: 0.001 (CR versus NR), 0.033 (PR versus NR) and 0.284 (CR versus PR).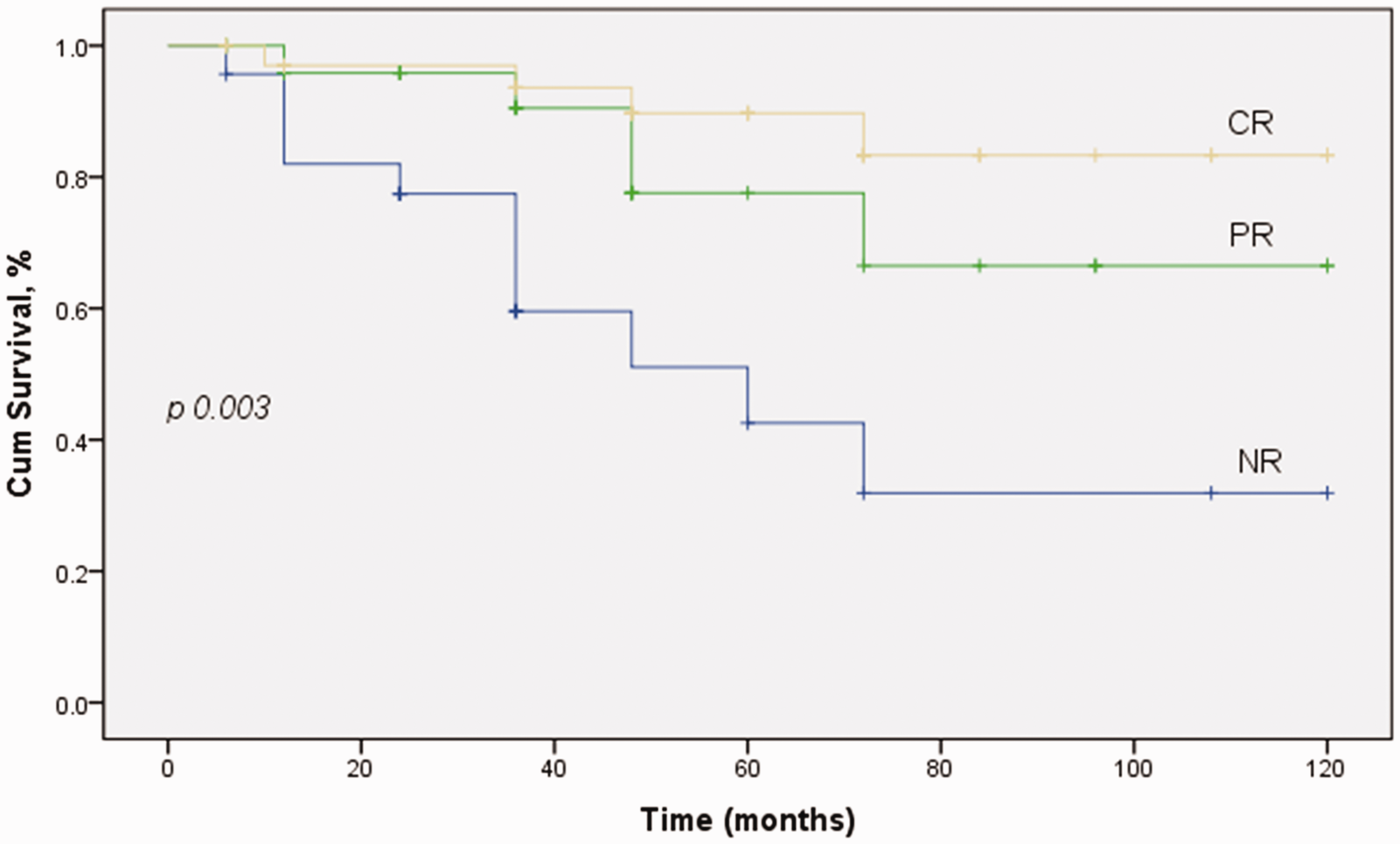
Out of the 96 patients treated for proliferative LN, 5 patients (5.2%) died over the follow up period. All were female, three of whom were Saudis, and all were diagnosed before the 2012 period. All patients had diffuse PLN (3 class IV and 2 mixed class IV+V). Regarding induction treatment; two patients received CYC, 2 MMF & 1 CnI. Only one patient achieved PR, while the remaining four achieved NR. Long-term dialysis was initiated in 4/5; one within 6 months and three beyond 6 months. The primary causes of death were sepsis (n = 3), active relapse with multisystem disease (n = 1) and hemodialysis with massive bleeding post cardiac valve surgery (n = 1).
Discussion
Our study revealed that 67% of PLN patients develop remission at 6 months of induction treatment, and remission is associated with long-term renal survival. Only histologic activity/chronicity pattern was found to be a significant predictor for remission, with patients in whom biopsies express more chronicity experiencing remission less likely. MMF is the most widely used agent for induction in our cohort; however, CYC is used more frequently with more severe disease presentation. Additionally, we noted a temporal trend of increasing use of MMF and lessening use of other agents. Furthermore, our findings revealed that, in more recent years, patients tend to be diagnosed at lower serum creatinine and lower urine protein, most likely related to changing trend in the practice to biopsy at earlier disease presentation rather than changing disease characteristics. Lastly, our data explore more on the unfavorable long-term outcomes of PLN with 11% cumulative rate of long-term dialysis, 10% rate of proteinuric relapse and 23% rate of doubling serum creatinine at median follow up period of 48 months (range 6 months to 11 years). The cumulative survival without doubling of serum creatinine is 74% at 5 years. This is better for those achieving CR (90%) and PR (78%) as compared to those achieving NR (43%).
Approximately one-third of our patients with PLN presented with severe renal disease, serum creatinine > 133 µmol/L, and 10% required dialysis at presentation, which was permanent in 5%. Anemia was present in 82%, hypertension in 42% and nephrotic-range proteinuria in 37%. Among all biopsies with PLN, Class IV LN was the most common in our cohort (63%), followed by class III (22%) and mixed V+III or IV (15%). Similar to these findings, a recent local publication on data from all renal biopsies identified PLN in 51 out of 63 biopsies with LN, of which 59% were class IV. 35 In a larger local cohort study (n = 226), among all biopsies with PLN, class IV was found in 69%, class III in 19% and mixed PLN in 12%.9,10
In our study, almost two-thirds (67%) went into remission at 6 months of standard induction treatment (39% CR, 28% PR). Histological activity was found to be a significant predictor. Remission was higher for class III (85%) than class IV LN (62%). A similar finding was observed from a smaller local study, the overall remission rate being 67.3% with a 46% CR and 21% PR. 36
Variations in the response to treatment and long-term outcomes of patients with PLN are observed in the literature, most likely related to varying disease severity and patient characteristics including ethnic background. In a study conducted by the Collaborative Study Group on a more ethnically diverse population, 86 US patients with diffuse PLN were enrolled for long-term follow up. In this study, a rate of remission similar to ours was obtained: CR in 43%, PR in 24% and NR in 32%. The researchers observed racial differences in both response to treatment and outcome of patients with severe LN. The rate of CR was higher in whites (52%) compared to blacks (29%) and others (27%). Similar to our findings, univariate analyses indicated a significant association of remission with baseline serum creatinine and chronicity index. 1 After multivariable analysis of our data, only histologic activity/chronicity pattern was found predictive of remission. Similar to these findings, prior studies have shown that chronicity index represented a significant factor,18,37,38 while other factors did not. 39
On the other hand, a higher response rate among Caucasian populations is frequently described. In an Italian study conducted by Moroni et al. in 2007 (n = 93), the remission rate among patients with PLN was high at 82% (63.4% CR and 19.3% PR); however, this was after a median follow up of 14 months. Furthermore, a more favorable long-term renal outcome was also observed with a renal survival rate of 97% at 10 years, and 90% survival without doubling serum creatinine at 10 years. 18 Overall the renal response and outcomes in this European cohort are more favorable compared to our population. One possible explanation is the difference in disease severity and difference in ethnicity.
In a more recent publication from the Hopkins Lupus Cohort study data the 24 months remission rate was 57.4% with CR of 40.9% and PR of 16.5%. 40 An association of remission status with long-term renal survival was observed as patients with CR and PR were significantly less likely to develop chronic kidney disease. Although the remission rate is similar to our findings; the long-term renal outcomes in this study were more favorable compared to our findings. This can be explained by inclusion of all classes of LN (including type V disease) and the less severe disease in this cohort. Almost one fourth (24.4%) of patients in this cohort did not require a specific induction agent. 40
We have identified a prognostic role for remission, even PR, on the long-term renal survival. The 5-year renal survival without doubling serum creatinine is 89.7% for CR, 77.6% for PR and 42.5% for NR. Similar to our observation, in a subsequent publication by the Collaborative Study Group on 86 US patients with diffuse PLN, the authors confirmed the prognostic value of CR, and even PR on the long-term renal survival. The 10-year patient survival was better for CR (96%) and PR (76%) as compared to NR (46%). Similarly, the 10-year renal survival was better for CR (94%) and PR (45%) as compared to NR (19%) (p < 0.0001 CR versus PR, p = 0.003 PR versus NR). 17 Similar findings were observed in few other studies.17,27,28
In our study, doubling of serum creatinine was seen in 20 patients (23%). We did not study predictors of long-term renal survival because we lack data on important potential predictors including data on maintenance therapy. Requirement for dialysis was reported in 15/91 patients (16%); 5 from the presentation and 10 additional patients entered ESRD beyond 6 months. A similar rate was reported in a larger local cohort that included all classes of LN including milder disease; the rate of progressing to ESRD and requiring dialysis was 12.4% and the majority of patients who died (n = 16/37) were class IV LN.9,10 Both a lower and a higher rate of developing ESRD were reported internationally: the reported rate of ESRD in the study conducted by Moroni and coworkers in Italy was 6.4%, and the rate of CKD was 15% after a median follow up of 141 months. A similar proportion (6.4%) of patients died by the end of follow up. 18 A higher rate of ESRD was reported from studies including non-Caucasian populations. 1 Among African American patients, a rate of 31% as compared to a rate of 10% in Caucasians is reported. 3
The reported rate of death in our study was five patients (5%). Mortality was not different between MMF and CYC arms. A similar rate of mortality was reported locally ranging from 6% to 8.2%,9,10,41 which is lower than that reported in the African American population of 34% 1 and more closer to the reported rate in Caucasian patients of 10%. 3
Although we included a relatively good number of patients with long-term follow up on mortality and renal outcomes, our study carries several limitations. First, there were no details on the doses of agents used for induction treatment, no details on the dose and route of steroid and CYC administration during the induction phase, and no data on the type of maintenance treatment, treatment compliance and use of other medications including antimalarial agents and renin-angiotensin system inhibitors. Second, due to the retrospective nature of the study, different centers involved and long period (up to 11 years) of data collected, there was lack of consistent reporting of important information from kidney biopsies including the number of crescents and the type of the lesion (global vs segmental). Third, the remission rate was assessed at short term (6 months) in order to maximize the number of patients included in the analysis. Perhaps more CR would have been observed if we had assessed patients’ response at or beyond 12 months of induction treatment. 42 Fourth, we did not study the risk factors for long-term outcomes due to lack of data on important predictors, especially maintenance treatment, treatment compliance and co-interventions. However, the effect of attaining remission was shown to influence the rate of doubling serum creatinine in a non-adjusted analysis.
In conclusion, renal histology with active lesions predicted the 6-month remission rate of PLN. Other baseline characteristics including age, sex, duration of SLE prior to diagnosis of PLN, BP, baseline serum creatinine, urine protein, hematocrit, histologic class and choice of induction treatment (CYC vs MMF) did not. Attainment of remission, even PR, predicts long-term renal outcomes. The response to treatment and long-term outcomes of Saudi patients with PLN is more comparable to that for non-Caucasians, including mixed-race populations, and probably less favorable compared to Caucasian patients.
Supplemental Material
Supplemental material for Remission and long-term outcomes of proliferative lupus nephritis: retrospective study of 96 patients from Saudi Arabia
Supplemental Material for Remission and long-term outcomes of proliferative lupus nephritis: retrospective study of 96 patients from Saudi Arabia by A H Almalki, F A Alrowaie, H M Alhozali, N K Almalki, A I Alsubei, M S Alturki and L F Sadagah in Lupus
Footnotes
Authors’ contributions
Research idea and study design: AH, LF, AI; data acquisition: FA, HM, NK, AI, MS; data analysis/interpretation: AH, LF; statistical analysis: AH. Each author contributed important intellectual content to the manuscript drafting or revision stages and accepts responsibility for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.